
Abstract
With excellent outcomes achievable using endovenous treatment of refluxing truncal veins, extension of ablative material and/or thrombus into adjacent deep veins is an important complication which can lead to deep venous thrombosis (DVT) or pulmonary embolism (PE). Previous work has used poorly defined terminology to identify patients with material in the deep venous system following ablation, limiting synthesis of results and the formation of treatment guidelines. We propose the term Post-ablation Deep vein Material Extension (PDME) to identify cases of ablative material and/or thrombus in the adjacent deep veins, with sub-categorisations according to mode of ablation used. PDME is a distinct entity from DVT, with often a shorter clinical course, few symptoms reported by patients, and possibility of resolution without treatment in some cases. This article explores the different forms of PDME, their classifications, and possible aetiology. A precise classification is proposed to ensure transparency in future research into this area.
Keywords
Introduction
Endovenous ablation is the first line treatment for symptomatic truncal varicose veins as recommended by European, American and British guidelines.1–3 This can take the form of thermal ablation using laser (endovenous laser ablation, EVLA) or radiofrequency (radiofrequency ablation, RFA), or non-thermal techniques utilising glue, foam or liquid sclerosant. All of these techniques have been shown to be safe, efficacious and well-tolerated by patients. 4 Both thermal and non-thermal ablation techniques rely on causing inflammation of the vein endothelium, leading to thrombosis, fibrosis and sclerosis sealing the vein and preventing reflux. However, with the adoption of these new technologies, extension of this thrombus and/or ablative material into the contiguous deep venous system is now recognised as a potential complication.5–10 Thrombus extension into the deep system raises the rare but serious risk of patients developing deep venous thrombosis (DVT) or pulmonary embolism (PE).11,12 However, current reports of these complications are plagued by misclassification, systemic underreporting, and lack of clear guidelines for recognition or treatment.
Post-ablation deep vein material extension (PDME)
A plethora of definitions and abbreviations have been suggested to define and categorise these phenomena, and with very few investigations into the underlying pathophysiology of these complications, accurate definition remains elusive. However, we recognise conflicting terminology has also hindered recognition amongst clinicians and between researchers. In this article we propose an umbrella term of ‘Post-ablation Deep vein Material Extension’ (PDME), with sub-categorisations specific to the treatment performed to improve the identification and subsequent management of these conditions (Figure 1). We propose a universal classification system for PDME applicable to all forms to standardise reporting of duplex ultrasound findings. This article explores each form of PDME in more detail and suggests a unified classification system to enable clearer reporting in future research. Classification and relationship between the different forms of PDME. EGIT = Endovenous glue induced thrombosis, TEACAC = Thrombus extension after cyanoacrylate glue closure, EFIT = endovenous foam induced thrombosis, EMIT = endovenous mechanochemical ablation induced thrombosis, ELIT = endovenous liquid sclerosant induced thrombosis, EHIT = endovenous heat induced thrombosis.
Ablation related thrombus extension - ARTE
Endovenous heat induced thrombosis - EHIT
Thrombus propagating into the deep venous system following thermal ablation was first described in the early 2000s, with authors initially reporting increased risk of DVT post ablation.6,11,13 This was later recognised as a separate entity to DVT, with the name endovenous heat induced thrombosis (EHIT), defined as propagation of thrombus up to the junction with, or into the deep vein contiguous with the ablated superficial vein. 14 Despite EHIT arising from several distinct ablation mechanisms, all resulted from thermal energy being delivered,15–18 leading to the overarching classification of EHIT, with subcategorisations for the method of ablation used. EHIT differs from DVT in that it is usually asymptomatic and therefore identified incidentally on post procedural ultrasound. The pathophysiology underlying the development of EHIT has been widely hypothesised, however no single pathogenesis has been proven. Its classification as a distinct clinical entity is reinforced by the presence of unique histological features, such as reduced collagen production, elevated hypercellular response, and surrounding oedema 19 compared to classical DVT.
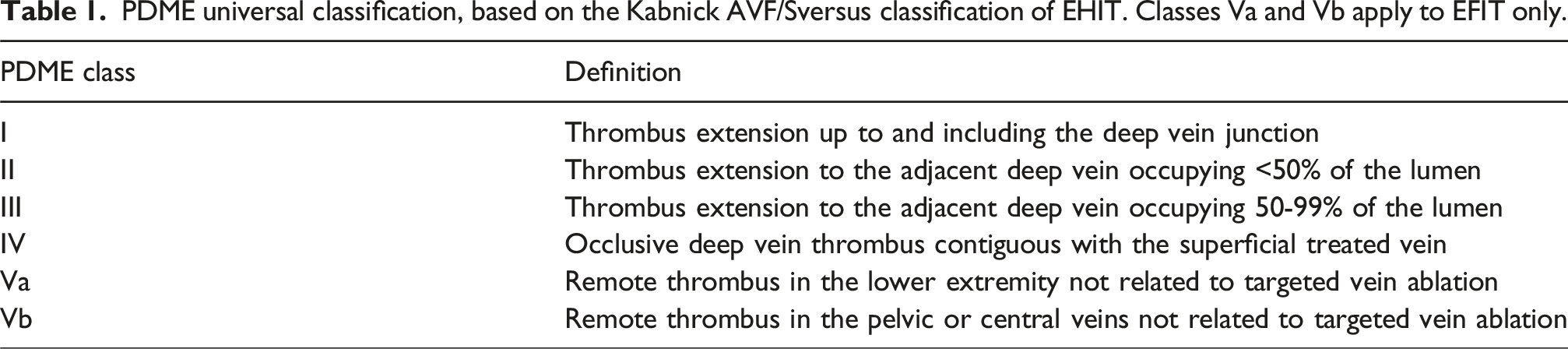
PDME universal classification, based on the Kabnick AVF/Sversus classification of EHIT. Classes Va and Vb apply to EFIT only.
EHITL – EHIT as a result of laser ablation has been well-characterised, with rates from a recent systematic review estimated at 0.85%. 26 We use the term EHITRF to delineate EHIT following radiofrequency ablation. Recent systematic reviews have estimated rates of EHIT following RFA of 1.6% 27 and 3.0%. 28 There are no documented cases in the existing literature of heat induced thrombosis following other methods of ablation such as microwave ablation, 18 HIFU, 15 and steam ablation. 29 However, their similarity in mechanism of action, involving thermal energy delivered to the endovenous endothelium, suggests that EHIT remains a possible complication.
A number of different risk factors for EHIT after endothermal ablation have been proposed, including male sex, previous history of VTE, Caprini score and increasing diameter of the GSV. 30 Some authors have compared EVLA to RFA, finding EHITL may resolve more quickly than EHITRF, 31 but that the rate of EHIT is higher post EVLA compared to RFA. 26 However, with evidence of publication bias resulting in widespread underreporting of EHIT, 30 there remains further questions regarding its incidence, pathophysiology and optimal treatment strategy.
Non thermal injuries
Endovenous glue induced thrombosis - EGIT
Cyanoacrylate glue closure (CAC) enables venous occlusion without the use of tumescent anaesthesia, with comparable closure rates to thermal techniques.32,33 CAC has also been associated with higher levels of patient satisfaction than other techniques such as RFA or surgical stripping.34,35 Cyanoacrylate glue exists as a liquid at room temperature, undergoing a polymerisation reaction to solidify and adhere to the vein wall intima on contact with liquids. The subsequent inflammatory process leads to vascular fibrosis and vessel closure. 36 In some rare cases, this can extend to the deep system, leading to deep vein thrombosis (DVT), or more worryingly pulmonary embolism (PE). 37 The exact mechanism of this is unknown, but possible theories include glue polymerisation and contraction continuing over time, or ongoing venous inflammation in response to the presence of glue. 38 Microscopic analysis of this material extending into the deep system has identified a combination of both glue and blood cells, 7 leading to the term Endovenous Glue Induced Thrombosis (EGIT). Rates of EGIT have ranged from 0 to 21%, 7 with a more recent meta-analysis estimating a pooled prevalence of 1.2% (95% CI 0.3% - 2.1%). 39 Possible risk factors increasing the likelihood of EGIT have been proposed, including longer length of treated vein, larger proximal thigh diameter, 38 and GSV diameter <5 mm7.
Cho et al. proposed a grading system for EGIT according to the percentage of deep vein occupied by thrombus and glue. Grade I described thrombus occupying <25% of the area of the deep vein, Grade II 25% – 49%, Grade III 50% - 74% and Grade IV >75%. Based on this they recommended patients with EGIT III and IV should be treated with anticoagulation due to the risk of flow limitation and deep venous occlusion. EGIT I and II are observed most frequently, and patients are usually asymptomatic and therefore safe to be managed with ultrasound surveillance only. In all patients with EGIT, this seems to resolve quickly, between 4 and 6 weeks. 38
Thrombus extension after cyanoacrylate glue closure (TEACAC) describes extension of thrombus only into the deep system, without glue. This was first described by Sermsathanaswadi in 2022, 40 who described an incidence of 4.9% in a retrospective cohort of 101 patients. TEACAC had a later onset than EGIT, occurring a week after ablation in all cases. The authors classified TEACAC based on the Kabnick EHIT classes; three patients had Grade I-II TECAC, and two had Grade III. The two patients with TECAC grade III were treated with DOAC until the thrombus resolved in 2-4 weeks. The patients with TECAC Grade I-II all spontaneously resolved within 2 weeks. TECAC represents a similar phenomenon to EGIT, but note must be made of its later presentation, different composition, and the fact TECAC has a tendency to spontaneously resolve, unlike EGIT. We propose the universal PDME classification is used for both EGIT and TEACAC (Table 1).
Endovenous liquid sclerosant induced thrombosis and endovenous foam induced thrombosis - ELIT and EFIT
Sclerotherapy is a widely used method of endovenous ablation, using detergents such as sodium tetradecyl sulphate (STS) or polidocanol (POL) to cause denaturation of proteins within the endothelium and media, and subsequent activation of apoptotic and inflammatory pathways. This results in the formation of a mixture of sclerosant and thrombus (‘sclerothrombus’) occluding the target vein, eventually leading to formation of a fibrous cord and elimination of reflux. 41 However, considering a growing body of evidence that truncal veins treated with liquid sclerotherapy tend to develop clinical and anatomical recurrence at a much higher rate than other treatments,42,43 it is now mainly recommended for the treatment of reticular veins or telangiectasias only. 44 Foam sclerotherapy is a more recent innovation where detergent sclerosant is mixed either with carbon dioxide, room air, or a mixture of carbon dioxide and oxygen (Varithena). 45 The formation of foam increases the contact of the sclerosant with the vein wall and markedly increasing its efficacy, 46 enabling use on larger diameter veins.
Due to the fact liquid sclerosant was reserved in the past for smaller reticular veins, reports of sclerosant and thrombus entering the deep venous system are sparse, but do exist. Reports as early as the 1980s describe extension of thrombus and sclerosant into the deep system, affecting 13% of 67 extremities treated with sclerotherapy. 47 A randomised controlled trial of microfoam versus surgery or sclerotherapy also reported one ‘DVT’ in the liquid sclerotherapy cohort which may well have been thrombus extension of sclerosant: unfortunately the appearance of the thrombus or further clinical details are not described by the authors. 10 In light of guidelines recommending liquid sclerosant use only on telangiectasia, sclerothrombus in the deep system should not be seen in modern clinical practice. However, we recommend the term Endovenous Liquid sclerosant Induced Thrombosis, ELIT to characterise this phenomenon if observed.
Endovenous ablation using foam was first reported in 1989 48 and is now a common treatment for both truncal and tributary reflux, as a low cost option that is well-tolerated by patients. Mixing detergent with air or carbon dioxide to produce foam enables increased contact with the venous endothelium and enhanced occlusion rates compared with liquid sclerotherapy. Propagation of this thrombus into the deep system has been reported with incidence ranging from 0% to 5.7%, 49 and has been described as Endovenous Foam Induced Thrombosis by Kulkarni et al. with similar categorisations to those used for EHIT: Type 1 describes thrombus lining <25% of the lumen of the deep vein; type 2 occupies 25-50% of the deep vein; type 3 occupies 50-99% and type 4 describes complete occlusion. 50 Kabnick further described EFIT type 5 which describes a remote thrombus, not related to thrombus extension or targeted vein ablation. EFIT type 5a describes thrombus in the lower extremity, and 5b a thrombus in the pelvic or central veins. It is worth noting the difference between this and the classifications used for EGIT which use different percentages of occlusion to describe the classes. We therefore propose the standardised PDME classification is used (Table 1), with additional classes Va and Vb.
The majority of reported cases of EFIT are asymptomatic, however in rare cases this has been associated with the development of PE.8,51 This has led to a recommendation to limit amount of foam injected to 16 mL per session by the European Society of Vascular Surgery in 2022, 44 in line with European regulations in the European Medicine Compendium. A survey of clinicians in the United Kingdom and Ireland found the majority of surgeons used 10-12 mL of foam in their clinical practice. 52
Kulkarni et al. reported a retrospective review of EFIT following foam sclerotherapy, 8 using their own classification highlighted earlier in this section. The majority of these cases affected the common femoral vein, with almost all patients remaining asymptomatic. Based on experience at their centre the authors suggest EFIT 3 (50-99% of the deep vein lumen occupied) and 4 (complete occlusion of the deep vein) be treated with anticoagulation and compression for six to 12 months, with EFIT 1 (<25% of the deep vein lumen occluded) and 2 (25-50% of the deep vein lumen occluded) treated with aspirin and/or compression, with DUS monitoring and treatment continued until resolution. The only significant risk factor found was injection of > = 10 mL of foam.
Mosher et al. performed a similar retrospective analysis for development of tibial EFIT, noting a rate of 2.7%, 53 and 55.2% of those affected reporting symptoms. Interestingly, similar proportions of EFIT spontaneously resolved irrespective of whether this was treated with anticoagulation or antiplatelet agents or simply observed.
Reporting of EFIT in the published literature remains sparse, and analysis of the deep veins affected by EFIT may allow more conclusions to be drawn regarding the pathophysiology of its development. Lack of a cohesive terminology and grading system also hinders reporting and therefore treatment guidance, with some authors also suggesting any entry of sclerosant into the deep veins is a clinical benign entity not requiring anticoagulation 54 despite other centres reporting clinically significant DVT and PE.
Endovenous mechanochemical ablation induced thrombosis - EMIT
Mechanochemical ablation (MOCA) was first described in 2010 as a novel non-thermal, non-tumescent method of endovenous ablation. 55 MOCA combines mechanical endothelial damage with the infusion of sclerosant to induce venous occlusion. Use of MOCA is associated with less pain during and post procedure than thermal techniques, 56 and the ability to treat veins in patients not eligible for thermal or cyanoacrylate ablation.
Reports of thrombus extension after MOCA are sparse. A multi-centre randomised dose-finding trial of 364 patients identified three patients who developed thrombotic complications. Two patients developed PE, one of which also had evidence of thrombus extension into the femoral vein (0.3%). 57 Systematic reviews of MOCA trials have calculated similarly low rates of thrombus extenion.58,59 This may be due to relatively low numbers of patients in trials of MOCA, and the fact that thrombus extension post MOCA has not yet been recognised as a clinical entity and classified. It is noted that one patient who developed a DVT in a randomised trial of MOCA recovered fully after a short dose of anticoagulation, similar to patients with EHIT. 48 We therefore propose the term Endovenous MOCA Induced Thrombosis, EMIT, to identify these patients. We propose the universal PDME classification is used for EMIT (Table 1), to aid future research into this field and ensure consistency in classification.
Non-thrombotic PDME
While thrombus combined with ablative material, or thrombus alone, extending into the deep veins has been described extensively, the use of foreign material to ablate veins such as glue or foam also raises the possibility of this material entering the deep system alone. We propose the term non-thrombotic PDME to describe this lesser-known phenomenon which we will now explore further.
Glue PDME
Cyanoacrylate adhesive, as described previously in this article, has been used widely for closure of vessels since 2000. While glue/thrombus extension (EGIT), or only thrombus extension (TECAC) post glue ablation has been recognised as a complication of this treatment, it is worth noting the possibility of solely glue extending into the deep system. The assumption all material extending into the deep system contains a mixture of both thrombus and glue is based on one extracted vein, where blood cells were seen interspersed with glue. 7 Novotny et al. interestingly reported a case of pulmonary embolism due to leakage of glue into the deep system, 60 but further analysis of this material was not undertaken to confirm whether this was solely glue or glue combined with thrombus. There may very well be two distinct entities that can exist after cyanoacrylate closure due to the nature of this being foreign material injected into a vein, with one form of deep venous extension containing both thrombus and glue, and another composed only of glue. We recommend further ex vivo analysis of samples from pulmonary emboli or deep venous extensions, where feasible, to further characterise these phenomena.
Foam sclerosant PDME
Since the introduction of ultrasound guided foam sclerotherapy, reports have emerged of transient neurological symptoms, including visual aura, parasthesias and speech disorders.10,61 Furthermore, echocardiography has demonstrated echogenic signals within the heart after sclerotherapy, raising concern foam can migrate into the deep veins and exert systemic effects. 62 A retrospective report by Mill et al. found echogenic phenomena to be very common in patients after foam sclerotherapy, with the signals thought to represent foam bubbles. 63 They also observed that when the SFJ was occluded and then pressure removed, a bolus of foam was released into the central venous circulation. All patients were asymptomatic while this was observed. All were also noted to have structurally normal hearts, however it has also been hypothesised presence of a right-to-left shunt may allow foam to pass into the arterial circulation and form microemboli. 64 A different potential mechanism could be air bubbles from the foam causing air embolus, which has also been seen in divers suffering similar transient neurological symptoms. 65 Another suggested cause is sclerotherapy causing endothelin 1 to be released from treated veins, which enters the systemic circulation and causes vasoconstriction in the cerebral vessels.66,67 While it is unclear whether all neurological symptoms are related to foam in the cerebral vasculature, clinicians should be aware of this as a potential complication that can cause neurological harm to patients.
Conclusions
This article is the first to highlight the concept of PDME: we propose deep material can either contain thrombus or be entirely made up of foreign material, e.g. foam sclerosant or cyanoacrylate glue. The former should be known as Ablation Related Thrombus Extension (ARTE), and the latter Non-Thrombotic PDME. ARTE and Non-Thrombotic PDME are then further sub categorised according to the ablation method precipitating the injury (Figure 1). We propose a universal classification of PDME, with fixed percentages of the deep vein occupied by each class (Table 1). This is applicable to any form of the condition and enables meaningful comparisons to be made. We hope this ensures clarity between clinicians treating patients with this complication and suggest the use of the terms PDME and ARTE in clinical practice to simplify understanding for patients and the public.
We would like to emphasise that while PDME is a subset of DVT, the natural history and aetiology are different, despite the terms often being used interchangeably in the literature. Taking the example of endovenous heat induced thrombosis (EHIT), this presents as a distinct clinical entity in contrast to DVT, with a shorter clinical course, lack of symptoms and often resolution without treatment, depending on its severity. Reported rates of PDME tend to be higher than that of DVT post endovenous ablation, 12 but it is worth noting it is often an incidental finding on postprocedural duplex ultrasound (DUS). However, the risk of transformation into DVT or PE remains, requiring vigilance amongst clinicians, and recognition that extension of material into the deep system can occur after any form of endovenous ablation, which we highlight in this article.
PDME presents a unique challenge to patients and physicians which will only become more pertinent as endovenous ablation becomes more widely adopted for the treatment of venous disease. PDME represents a spectrum of conditions with different causative agents, but all may go on to cause serious complications such as DVT and PE. Lack of unified terminology and classification limits reporting of these complications, hindering the development of effective management strategies. Particularly, the application of the term EHIT to cases of thrombus extension that are not caused by heat ablation methods is inappropriate and hinders further understanding of these unique phenomena. By proposing a framework of PDME and its sub-categorisations, this article aims to unify existing concepts, and encourage clear reporting of PDME and its sequalae. PDME has been reported in the literature for two decades: we highlight the relative lack of information about its unique pathophysiology and encourage further inquiry in this area, enabling optimal treatment and prevention strategies to be generated.
Footnotes
Author contributions
Conception and design: JB, LK, SO, AHD. Writing the article: JB, LK. Critical revision of the article: JB, LK, SO, AHD. Final approval of the article: JB, LK, SO, AHD
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Prof Alun Davies