
Abstract

Introduction
Varicose veins (VVs) are a very common presentation of chronic venous disease, with an estimated prevalence of <1-73% in women and 2-56% in men globally. 1 Associated symptoms and complications, including heaviness, pain, swelling, skin changes, and ulceration, 2 cause limitations in quality of life but are usually not life-threatening. However, bleeding, or spontaneous haemorrhage, from VVs, is a potentially life-threatening complication that is not uncommon. 3 The risk of bleeding is increased when there is atrophic skin overlying the VVs, phlebectatic blebs, or if VVs underlie an ulcer.
Should VVs rupture, the volume of bleeding can be significant, potentially life-threatening, and has been reported in the literature to lead to sudden death from circulatory collapse.4,5 Risk factors for death include anticoagulation usage and frailty: elderly patients who live alone are at high risk of death from this kind of haemorrhage. Even after resolution of the initial haemorrhage, there is a known risk of bleeding reoccurring if patients fail to receive treatment for their VVs.
Most vascular specialists agree that bleeds associated with VVs require immediate referral and management. Urgent treatment of the patient’s venous hypertension is indicated, with treatment options including endovenous ablation, sclerotherapy, and compression bandaging for ulceration. However, the potential seriousness of having had a bleed may not always be recognised by patients or non-vascular healthcare professionals. This article seeks to highlight the management recommendations from the International Union of Phlebology (UIP), with an accompanying one-page summary of steps that should be followed to manage bleeding VVs. This document is meant to be used by both general and specialist healthcare professionals, and patients.
Management recommendations
The management of bleeding VVs can be divided into two parts – first aid applied by patients themselves or by a bystander, followed by medical care provided within a healthcare facility.
The patient should be advised about the risk of bleeding and appropriate first aid measures. The first step is to lie or sit down with their leg elevated on a support or by someone else. They should apply pressure to the bleeding site with their hands, following which, a pad and compressive bandages should be used if available. The applied bandage should not be removed until medical review. Once these steps have been completed, patients should seek help via their general practitioner or an emergency ambulance.
When transferred to a medical facility, clinicians attending to the patient should recognise the urgency of the situation. Immediate management should include basic life support assessment and management if a large volume of blood has been lost, fluids to combat any signs of circulatory collapse, and reapplication of compression over the bleeding VV if the initial compression is insufficient.
Urgent referral to a vascular specialist is recommended. Duplex ultrasound imaging of the venous system should be performed urgently, with a view to early treatment of the patient’s underlying chronic venous disease. Other causes of the bleeding, including arteriovenous malformations or fistulas, vascular tumours, or arterial collaterals, should be excluded by appropriate imaging modalities.
Discussion
This article promotes a one-page clinical practice guideline summarising the clinical management of bleeding VVs. It is part of a series of publications – the UIP One-Page Guidelines – which are aimed at ensuring that patients with venous disease receive timely and appropriate care based on current best evidence and expert consensus (Figure 1). This guideline highlights the importance of appropriate first aid to slow or stem the bleeding from VVs, followed by immediate clinical management with resuscitation (if required) and definitive measures to stop the bleeding, and subsequent treatment of the varicose veins to prevent recurrence. The one-page guideline.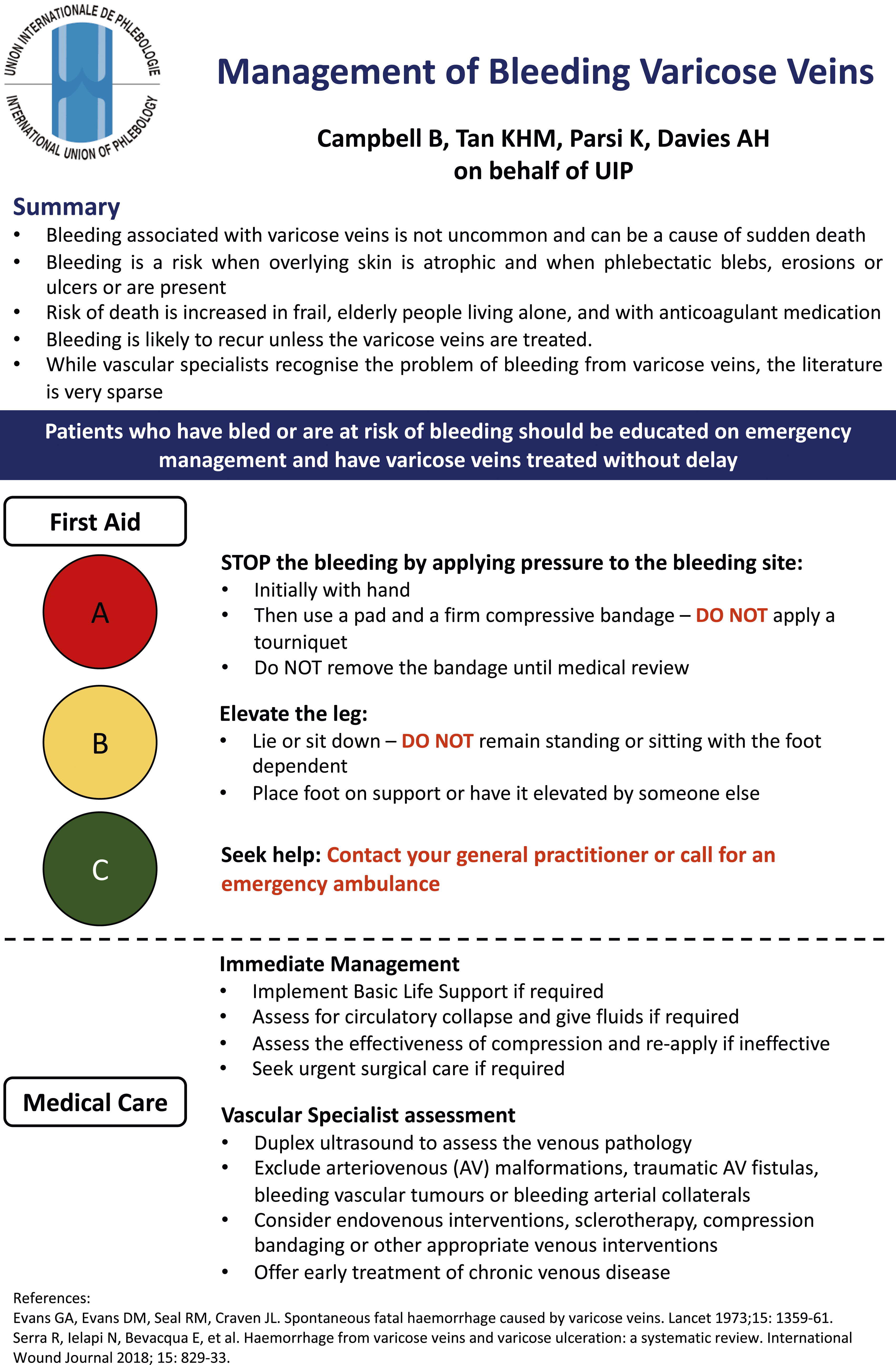
Over thirty case studies, summarised in a systematic review published in 2021, 5 have reported on significant haemorrhage related to VVs, with most cases resulting in death. The patient population most at risk of fatality from bleeding VVs is that of elderly patients who live in isolation, with nobody nearby to provide appropriate first aid. People living with VVs, especially those with risk factors for bleeding, should be counselled and educated on this potential risk. They should be taught how to perform the first aid steps for immediate management, should they experience a bleed before venous treatment. Locally, practitioners should signpost patients to the right healthcare services in case they do suffer a bleed, and they should refer patients at high risk for treatment of their veins.
For healthcare providers, this article and summary document highlight the potentially fatal consequence of bleeding VVs. Primary care physicians, emergency medicine practitioners, and other healthcare staff members who are likely to be the first point of contact for a patient with bleeding VVs need to refer the patient urgently to a vascular specialist. The urgency of referral, assessment, and treatment of patients who have bleeding VVs cannot be overemphasised.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Professor Alun Davies on behalf of the UIP.
Contributorship
K.P. and A.H.D. conceptualised the design of the short report and one-page guideline. B.C. contributed to the literature review and formulation of the recommendations. M.T. contributed to the formatting and layout of the one-page guideline (![]() ) and wrote the initial draft of the short report. All authors reviewed the short report prior to submission.
) and wrote the initial draft of the short report. All authors reviewed the short report prior to submission.