
Abstract
Introduction
Iliofemoral deep vein thrombosis (DVT) refers to venous thrombosis that involves the iliac veins and/or common femoral veins, with or without the involvement of other veins. Patients who present with iliofemoral DVTs are at higher risk of recurrent DVTs, post-thrombotic syndrome (PTS), and greater severity of PTS than patients with less extensive DVTs.1,2
Prompt treatment of the patient with an acute iliofemoral DVT with anticoagulant therapy can reduce the risk of pulmonary embolism (PE), DVT recurrence, and possibly longer-term sequelae like PTS. Beyond anticoagulation, catheter-directed thrombolysis (CDT) and pharmaco-mechanical CDT (PCDT) are minimally invasive endovascular procedures that help obtain patency during the acute phase of illness. 3 Subgroup analysis from a large randomised clinical trial has shown that PCDT improved quality of life when used in patients with iliofemoral DVTs within 2–3 weeks after symptom onset and reduced severity of PTS. 4 However, benefits were most prominent within the first 6 months. 5 Additionally, PCDT increases risk of major bleeding, suggesting the need for careful patient selection after careful individualised assessment.
Another potential approach to treating acute iliofemoral DVT is the use of mechanical thrombectomy (MT) alone (i.e. without a thrombolytic drug) in addition to anticoagulation. Limited studies including a multicentre registry suggest that MT can often remove acute thrombus and aid in restoring venous patency, and the avoidance of thrombolytic drugs seems likely to enable a lower risk of bleeding compared with CDT or PCDT. 6 Concurrent improvement in symptoms and quality of life has been documented in MT recipients, but because these studies lacked control groups and did not employ blinded, independent outcome assessments, it remains unclear how much of the observed clinical change can be attributed to the MT procedure rather than the standard DVT therapy that was also given and natural time-dependent healing. The effects of MT, which can require large vascular sheaths to be inserted, on late venous patency, recurrent VTE, and PTS also remain unknown. Well-designed prospective trials are needed.
This article seeks to highlight the recommendations for interventional treatment of iliofemoral DVTs from the International Union of Phlebology (UIP). A one-page summary of indications, contraindications, and clinical considerations accompanies this article which can be a useful reminder to all clinicians that may encounter a patient with iliofemoral DVTs in their clinical practice (Figure 1). The one-page guideline.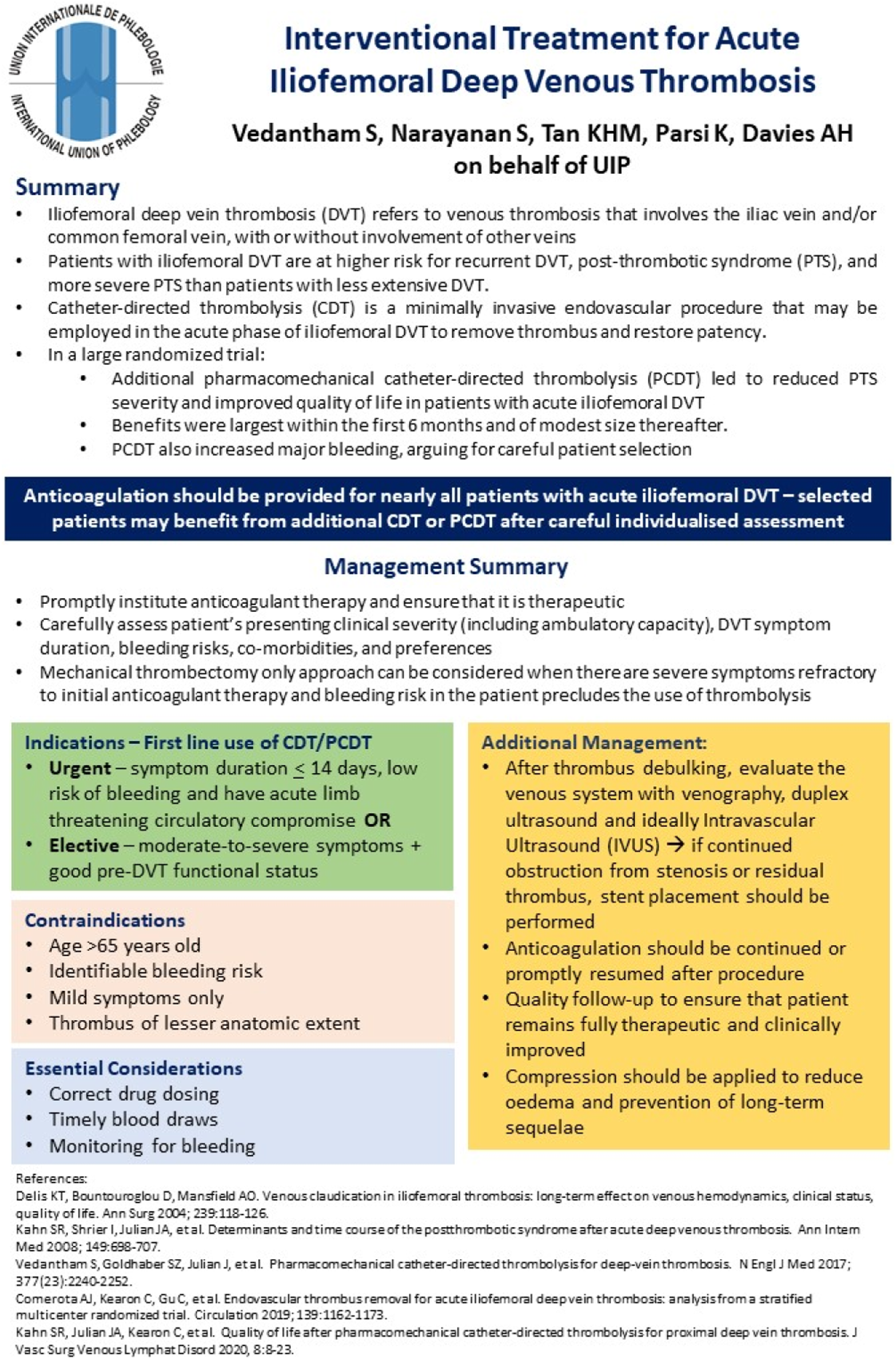
Management recommendations
It is recommended that therapeutic levels of anticoagulation therapy are promptly initiated. Selected patients with acute iliofemoral DVT and symptom onset within the preceding 2–3 weeks may also benefit from additional CDT/PCDT, which may be stratified further based on careful assessment of the patient’s clinical severity and ambulatory capacity. Clinicians should also establish their patient’s DVT symptom duration, bleeding risk, and co-morbidities. Patient preference in relation to treatment options should also be considered in the shared decision-making process. Clinicians should also consider certain contraindications to usage of CDT/PCDT, which include >65 years of age, identifiable bleeding risks, mild symptoms, and less anatomical extent of thrombus. However, an MT only procedure, if available, can be considered as an alternative to CDT/PCDT in highly selected patients with severe symptoms who present early (less than 2–3 weeks), have failed to experience symptom improvement with an initial course of anticoagulant therapy, and are judged to have a high bleeding risk or as per patient preference. The routine, first-line use of MT is not recommended since its incremental risks and benefits have not been rigorously evaluated in well-designed studies with independent outcome assessments.
The endovascular intervention may be performed urgently or as an elective procedure. An urgent intervention is recommended for patients with acute limb-threatening circulatory compromise to enable limb salvage. If patients present with non-threatened limbs, moderate-to-severe symptoms, and have good pre-DVT functional status, the intervention can be performed as an elective procedure instead. While the patient is undergoing CDT/PCDT, clinicians are advised to ensure correct drug dosing according to established protocols, timely blood draws to monitor patients’ response to treatment, and continually monitor patients to ensure that they are not bleeding.
It is recommended that after thrombus debulking with CDT/PCDT/MT, the venous system is again evaluated with duplex ultrasound, venography, and ideally intravascular ultrasound (IVUS). Should there be residual obstruction of the iliac vein from venous stenosis or thrombus, the treating clinician should consider stent insertion to ensure continued patency of the venous outflow tract. Patients should be monitored closely post-procedure to prevent, identify, and manage any complications, with particular attention to bleeding at the venous access site or at distant locations. Longer-term, patients should be continued on anticoagulation and may be given compression therapy to reduce recurrent thrombosis and limb oedema, respectively. Follow-up should be arranged to ensure that patients remain fully therapeutic and clinically improved.
Discussion
This article provides a one-page clinical practice guideline summarising the interventional treatment for acute iliofemoral DVTs. It is part of a series of publications for the International Union of Phlebology (UIP) One-Page Guidelines which are aimed at ensuring that patients with venous disease receive timely and appropriate care based on current best evidence and expert consensus.
Despite national and international society recommendations on the endovascular treatment of DVTs, management remains physician and hospital-protocol dependent. Early results from CDT trials showed favourable results when comparing CDT to anticoagulation alone. 7 However, there still exists debate on its wider application due to the continuous developments in thrombolytic techniques and the associated risks, with most physicians now reserving its use for phlegmasia cerulea dolens, massive IVC, or iliofemoral DVTs. This is supported by the CaVenT trial, which showed long-term risk reduction of PTS. 8 This selective use was further supported by the results from the ATTRACT trial, with only the subgroup analysis of iliofemoral DVT patients showing improvements in the incidence of moderate-or-severe PTS (28% vs 18%, p = .02) in the PCDT group. 4 Exploratory analyses of ATTRACT data found that patients who present with moderate–severe symptoms may be more likely to gain 24-month benefits from PCDT than patients with milder symptoms. 9
Clinicians should be reminded that the long-term management of patients also includes patient education. Patients must be reminded about the importance of strict compliance to anticoagulation as well as the red flag symptoms for bleeding related to this medication. Awareness of symptoms that may be related to a recurrence of DVT should be highlighted together with the differences in the swelling that is related to PTS. Patient education is key to help reduce rates of readmission through early identification of concerning symptoms and help improve patients’ quality of life.
For healthcare providers, this article and summary document should highlight the potential severity of iliofemoral DVTs and the indications for endovascular treatment. All vascular and other interventional specialists that may encounter patients with iliofemoral DVTs should be reminded to carefully assess individual risks and the specific likelihood of improvement with endovascular management. This is in line with multiple national and international guidelines and further reinforced by this one-page guideline. This will facilitate the urgent assessment and interventions indicated in this population of patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Professor Alun Davies on behalf of the UIP.
Contributorship
K.P. and A.H.D. conceptualised the design of the short report and one-page guideline.
S.V. and S.N. contributed to the literature review and formulation of the recommendations.
M.T. contributed to the formatting and layout of the one-page guideline (![]() ) and wrote the initial draft of the short report.
) and wrote the initial draft of the short report.
All authors reviewed the short report prior to submission.