
Abstract
Objective
YouTube® has gained popularity as an unofficial educational resource for surgical trainees, but its content's quality and educational value remain to be evaluated. The aim of this study is to analyze the current content on these techniques for lower extremity DVT (LEDVT) on YouTube®.
Methods
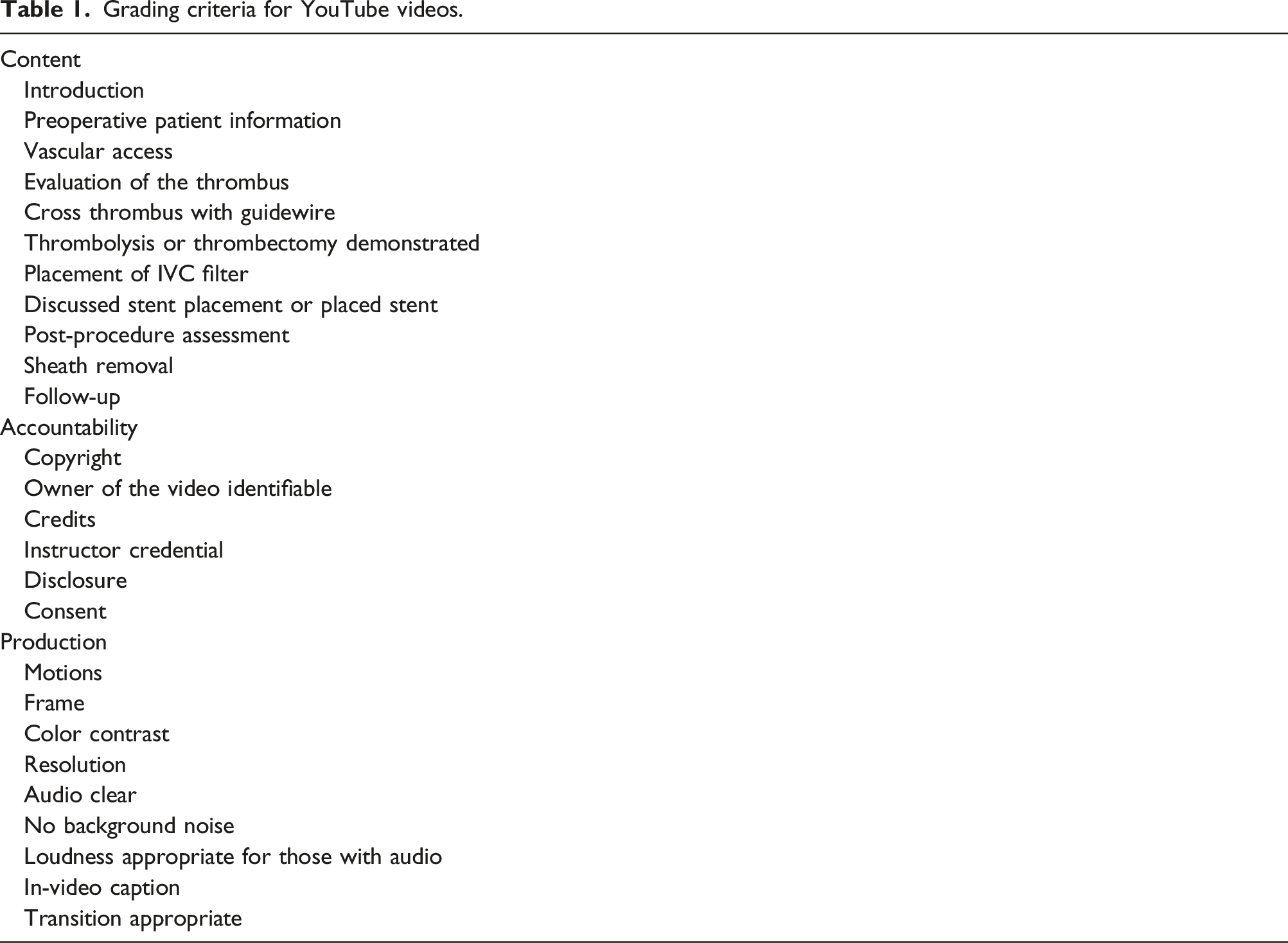
A search was performed on YouTube® using 13 search terms in August 2022 on a clear-cached browser. Open-access videos focusing on the surgical techniques of venous thrombolysis or thrombectomy for LEDVT were included. Quality and educational value were assessed and graded based on metrics for accountability (4 items), content (13 items), and production (9 items).
Results
Out of 138 videos regarding LEDVT oriented towards medical professionals, only 14 met inclusion criteria. Videos ran for a median of 3.4 min (range 0.37–35.6 min) with a median of 941 views (range 106–54624). Videos scored a median of 5.5 (range 1.0–8.0) out of 11 for content, a median of 2.0 out of 6.0 (range 0.0–2.0) for accountability, and a median of 5.5 out of 9.0 (range 3.0–9.0) for production.
Conclusion
Few YouTube® videos focus on the technical aspects of DVT thrombolysis/thrombectomy, and they vary significantly in content with overall poor accountability and production quality.
Introduction
YouTube® videos have recently become an important study resource for surgical trainees. YouTube® is an open-access platform with over 2 billion users 1 and can accrue over 14 billion views in 1 week. 2 Ninety-five percent of surgical learners and eighty-three percent of faculty have used online videos to prepare for cases with YouTube® being the most popular source. 3 Videos and multimedia-based learning have been shown to improve surgical performance in previous studies.4,5 However, data on the usefulness of YouTube® videos for surgical trainees have conflicting reports.
A recent study on carotid endarterectomy YouTube® videos found that only 17.4% of videos were high-quality videos demonstrating all key steps of the procedure and included English-language captions or narrations. 6 Another study on femoral access found that vascular specialists had fewer and older videos than interventional cardiology and radiology physicians. 7 This study also found that while 100% of videos by vascular specialists showed ultrasound-guided access, 93% of interventional cardiology and radiology videos showed landmark-guided access, which is not in keeping with current guidelines. 7
The quality of YouTube® videos on vascular procedures has not been adequately evaluated. Deep vein thrombosis (DVT) occurs in about 100 persons per 100,000 each year. 8 Catheter-directed thrombolysis (CDT) 9 and pharmaco-mechanical thrombectomy (PMT) 10 may improve vein patency and decrease the severity of the post-thrombotic syndrome and are indicated in patients with phlegmasia cerulea dolens and young patients with symptomatic DVT involving the iliac and common femoral veins. 11 CDT is a required procedure on the SCORE (Surgical Council on Resident Education) Curriculum for integrated vascular surgery residents and vascular surgery fellows. 12 The aim of this study is to evaluate the quality of YouTube® videos on endovascular thrombolysis or thrombectomy for lower extremity DVT.
Methods
Study design
This is a cross-sectional study of publicly accessible YouTube® videos on endovascular thrombolysis or thrombectomy for lower extremity DVT. This study does not involve identified patient information and is exempt from Institutional Review Board approval.
Search strategy
A search was performed on YouTube® on a clear-cached browser in August 2022. Search terms were developed with assistance from the institutional librarian and included “deep venous thrombosis lysis,” “DVT lysis,” “venous thrombolysis,” “DVT catheter-directed thrombolysis,” “deep vein thrombosis catheter-directed thrombolysis,” “DVT ultrasound accelerated thrombolysis,” “deep vein thrombosis ultrasound accelerated thrombolysis,” “DVT pharmaco-mechanical thrombectomy,” “deep vein thrombosis pharmaco-mechanical thrombectomy,” “DVT thrombectomy,” “deep vein thrombosis thrombectomy,” “DVT mechanical thrombectomy,” and “deep vein thrombosis mechanical thrombectomy.” The top 50 videos ranked as most relevant and then by most viewed were included for initial review. Internet users tend to focus on the top 10 search results and rarely go past the first page for both general and health-related information.13,14 We chose 50 videos in sequence to be more inclusive.
Inclusion and exclusion criteria
We included technical videos on endovascular lower extremity DVT thrombolysis or thrombectomy oriented towards health professionals. Videos excluded were (1) videos for patients; (2) videos on upper extremity DVT; and (3) videos showing open surgical techniques.
Assessment
Grading criteria for YouTube videos.
Video viewing, rater training, and correlation
Videos were assessed offline following download to prevent streaming issues, where video content is modulated for specific device and download capability. Video evaluators (QY and AR) were trained with example videos of good and poor video production quality. Accountability and content were evaluated as either present or absent and did not require rater judgment. Two raters scored all three domains of the videos independently with disagreements resolved by consensus and persisting disagreements resolved with senior author input.
Statistical analysis
Categorical data were presented as numbers (percentages). Continuous data were presented as median (interquartile range, [IQR]). Statistical analysis was performed using R version 1.2.5001 (RStudio, Inc., Boston, MA).
Results
Video selection
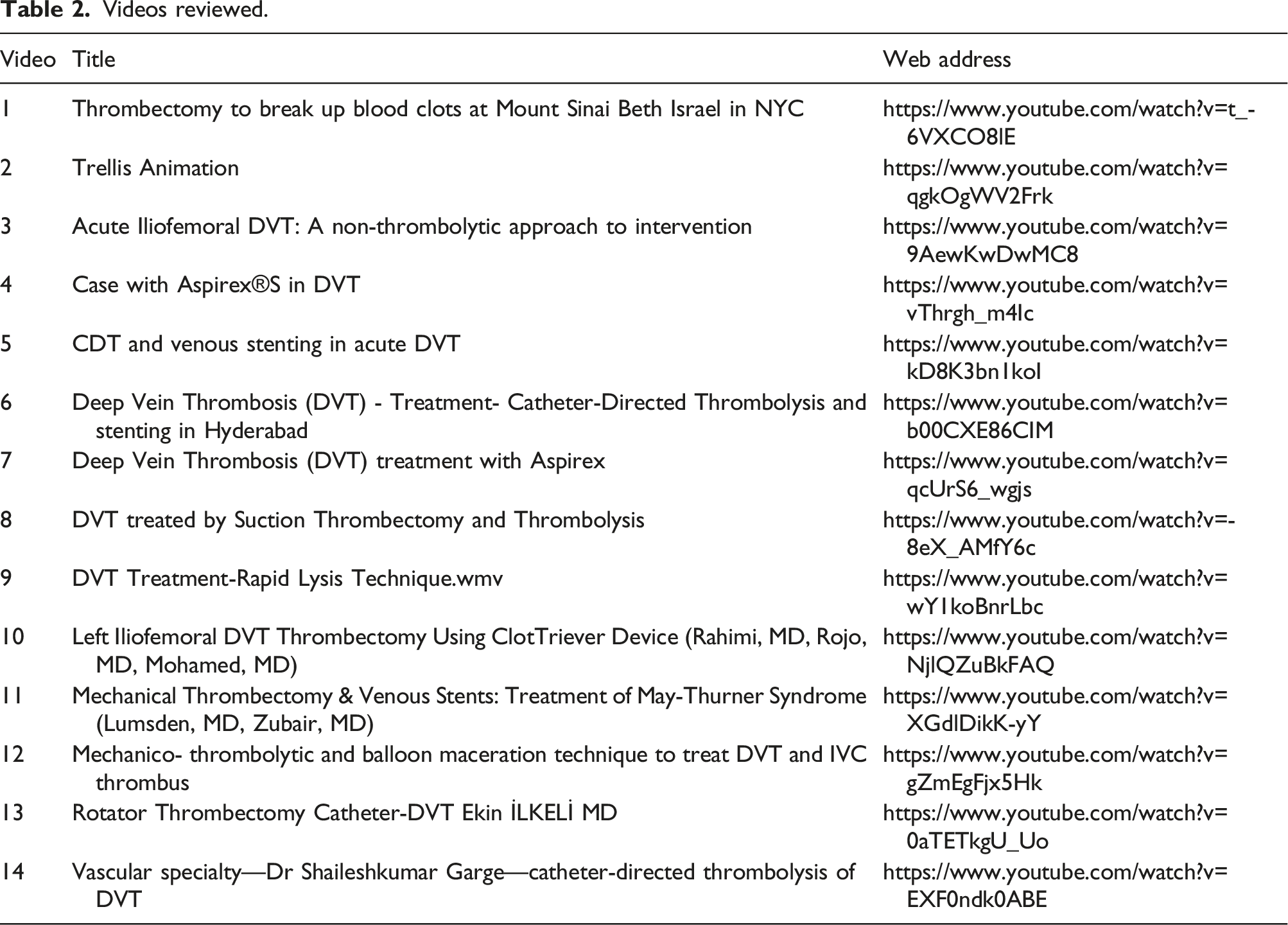
A total of 854 YouTube® videos were identified, yielding 268 unique video presentations. A fifth (62/268, 23.1%) of the videos were oriented towards patients. Out of 138 videos covering lower extremity DVT and oriented towards medical professionals, 48 (34.8%) were medical lectures, 43 (31.2%) were conference recordings, 13 (9.4%) were videos focused on a medical device, 12 (8.7%) were videos of ultrasound tutorials, 6 (4.3%) were miscellaneous medical videos not focused on procedural techniques, and 16 (11.6%) were procedural technique videos. Three procedural technique videos were not on simple endovascular thrombectomy or thrombolysis, yielding a final total of 14 videos that satisfied the inclusion criteria (Figure 1 and Table 2). These videos scored a median of 12.0 out of 26 (48%; range 5.5–18.0, IQR 8.5–16.0) total quality score (sum of content, accountability, and production metrics). Flow diagram for video selection. Videos reviewed.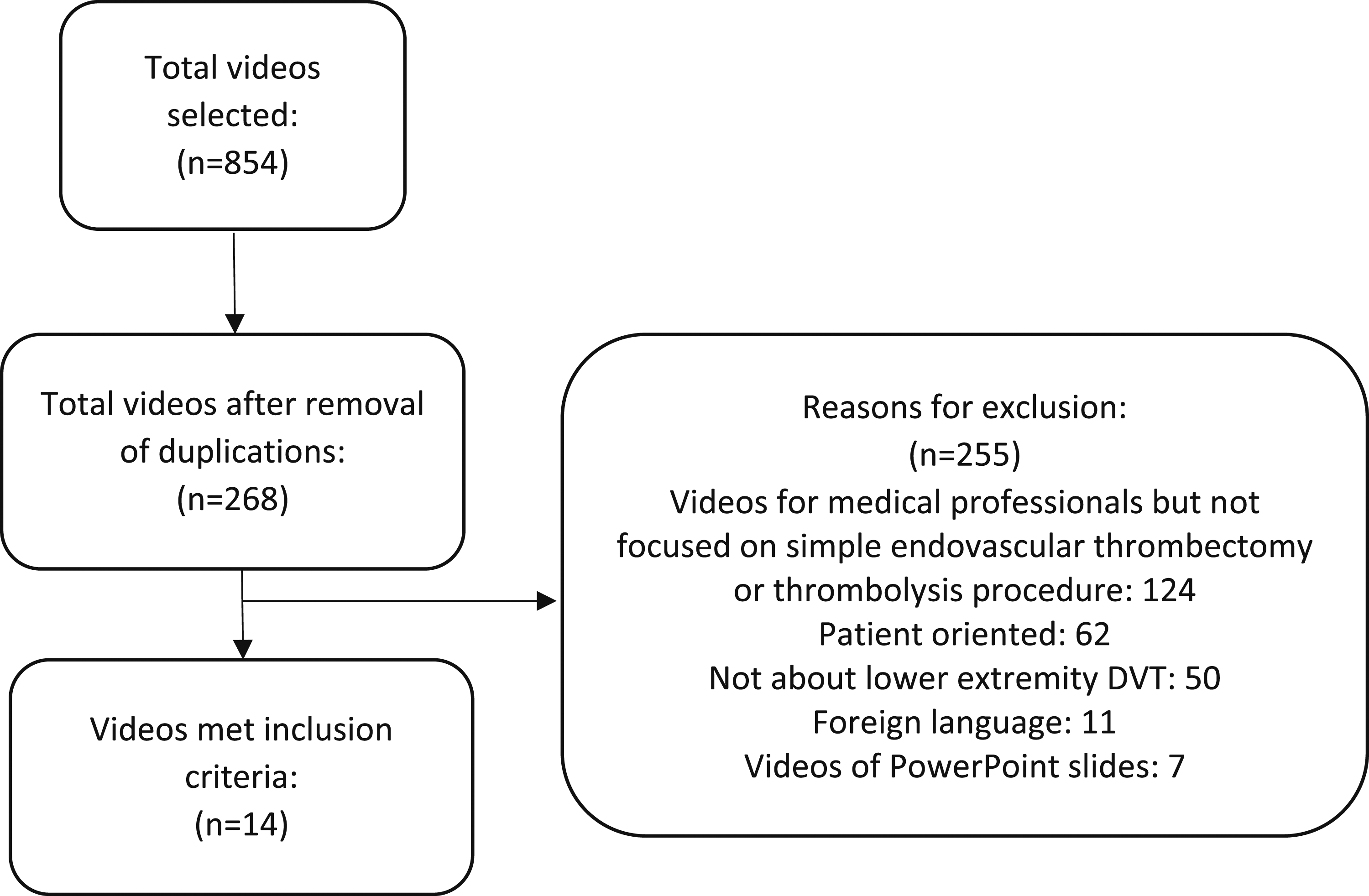
General video information
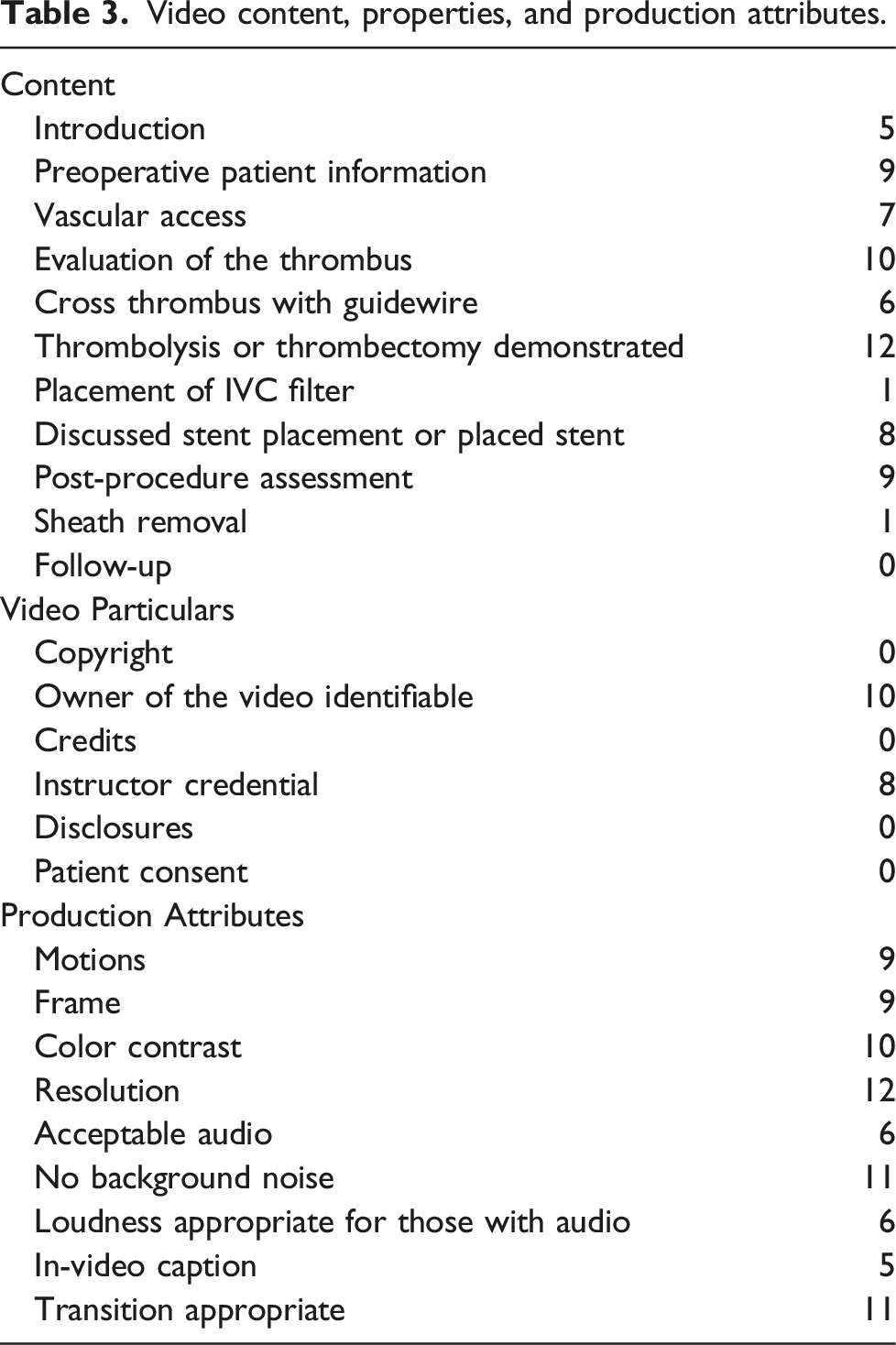
Video content, properties, and production attributes.
Content
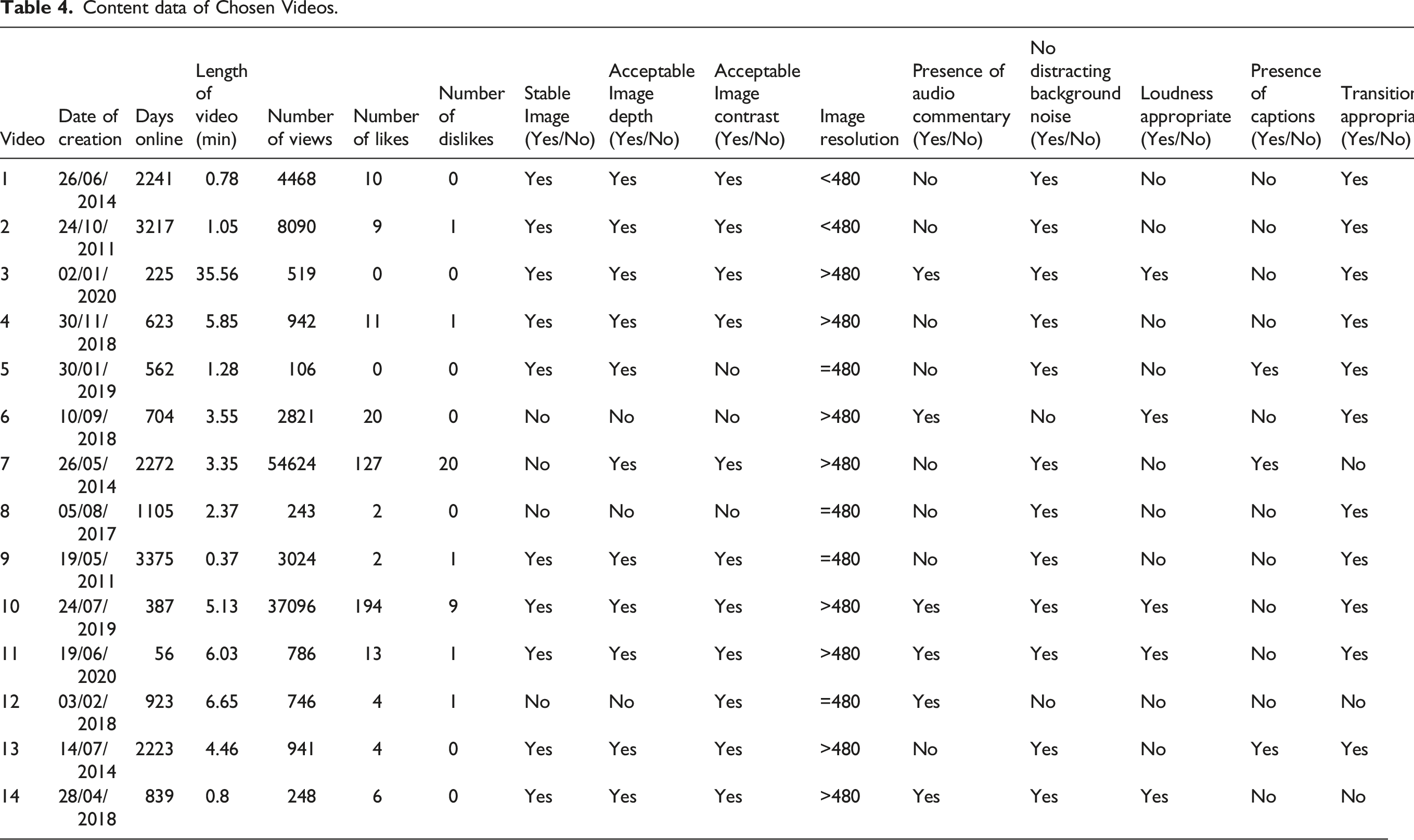
Content data of Chosen Videos.
Accountability
Videos scored a median of 2.0 out of 6.0 (33%; range 0.0–2.0, IQR 1.0–2.0) for accountability. None of the videos had video credits, disclosures, copyright information, or documented the patient’s consent for disclosing information on the Internet (Table 4). Ownership of the video can be inferred in 10 (71%) videos, and 8 (43%) videos did disclose the credentials of the narrator or the owner. Higher accountability scores were associated with higher educational content scores (Kendal’s tau 0.53, p = .03).
Production
Videos scored a median of 5.5 out of 9.0 (63%; range 3.0–9.0, IQR 4.5–8.0) for production attributes (Table 4). Most videos performed well on several production criteria—12/14 (86%) had acceptable resolution, 11/14 (79%) did not have background noise, 11/14 (79%) had appropriate transition, 10/14 (71%) had appropriate color contrast, 9/14 (64%) had stable images, and 9/14 (64%) had adequate framing. Videos performed less well in having a satisfactory audio commentary 6/14 (43%), although all videos with audio commentary had appropriate loudness. Only 5 (36%) videos had in-video captions. There was no correlation between the year of video upload a publication on the YouTube® platform and the production quality (Kendall’s tau 0.27, p = .23), showing no improvement in production attributes or a learning curve.
Discussion
Our study found that the amount of useful YouTube® educational content on DVT thrombolysis/thrombectomy for the trainee is scant, with a large majority focused on patient education and medical lectures. While most videos had acceptable production attributes, they fell short on accountability and were noted to have wide variations in educational content. Remarkably, not a single video discussed patient consent for publication in an open online forum. None of the videos were comprehensive in terms of discussing all the necessary technical steps in performing a DVT thrombolysis/thrombectomy.
Vascular surgery as a field is fairly underrepresented in terms of educational YouTube® content for resident surgeons. From an educational perspective, a stand-alone video should supplement the traditional didactic and hands-on training for trainees, and the content of the video should demonstrate the main teaching points that would be sufficient to achieve mastery of the technique. Doenges and Reed performed a study on carotid endarterectomy (CEA) videos on YouTube® and evaluated simple technical aspects such as conventional versus eversion CEA and techniques of closure of the arteriotomy. The authors classified videos having key technical components of the procedure as “high-quality” but did not provide a granular analysis of video content. Their study documented the scarcity of substantive videos on CEA on this media platform. 6 Furthermore, Pitcher et al. in their study on YouTube® videos discussing common femoral artery access noted that only a minority of videos demonstrated ultrasound-guided access—the current standard of care. 7 This reflects that content available on YouTube® is not only limited in quantity but may also lack robust educational quality and not be in line with up-to-date practice and care standards. In fact, this may mislead trainees who utilize this platform for their education. In our study, only a small number of videos detailed most procedural steps—with most videos barely discussing IVC filters, post-operative follow-up, and surveillance. There is no gatekeeper or standard applied before upload on this public website, and content is curated after upload based on social media guidelines and not educational quality. Videos directed towards trainees and/or supervising staff should be peer-reviewed and follow an acceptable set of guidelines and a checklist similar to reporting guidelines used to publish articles in the peer-reviewed press. Currently, no reporting guidelines for multimedia presentations have been put forward by the Vascular Societies.
Accountability-related data from the videos were poor. None of the videos had disclosures, video credits, or copyright/ownership information and only approximately half disclosed the credential of the narrator. This is particularly important since accountability information allows the viewers to judge the credibility of the presented information and copyrights prevent unauthorized replication of content. Most concerning, however, is that while 7 out of the 14 videos in our study provided preoperative patient information, none of them disclosed patient consent for presenting patient data. An article by Hood et al. in the British Medical Journal demonstrates the sequence of steps necessary in order to record patient videos for educational and demonstration purposes. 16 It is important to remember that patient consent is required not only for publishing a video online but even for the recording of the procedure in the operating room or endoscopy suite. This respect for patient autonomy is a basic tenet of medical practice, and future video content should be cognizant of disclosing informed consent prior to displaying patient media. You Tube® is now collaborating with several medical institutions to review health content on the platform in order to reduce the level of misleading or inadequate information by unpublishing and eliminating faulty content but currently has not adopted an empiric ranking system but rather uses the viewers’ opinion (like or dislike) to act a crowd-sourced ranking system.
While endovascular thrombolysis or thrombectomy of lower extremity DVT videos had acceptable production quality with over 75% of videos meeting more than half of the production attributes, this is significantly lower than patient-oriented videos for colorectal cancer screening from our unpublished work. 17 This is possibly because DVT thrombolysis/thrombectomy videos were mainly from individual users rather than institutionally affiliated YouTube® channels and so were resource-constrained. Videos on institution-affiliated YouTube® channels have greater resource allocations and receive more professional technical support. Furthermore, as noted by Doenges and Reed, 6 the quality of current YouTube® videos pertaining to trainee education in vascular surgery is considered modest at best. Utility of operating room camera capabilities, while performing endovascular surgery, can result in high-quality footage that can be used to teach trainees. 6 Audio commentary accompanying videos can significantly improve reach and impact and allow assimilation by even junior residents in training. Creating such high-quality content and incorporating media-based online resources in interventional education can be achieved by a collaborative effort between individual residency programs and the principal professional societies.
The SCORE curriculum currently has 14 vascular surgery-related videos and none were related to thrombolysis/thrombectomy of lower extremity DVT. The SVS YouTube® channel has 4700 subscribers and has achieved a broad platform for streaming committee reports, town halls, annual research meetings, and videos for patients. However, the Society of Vascular Surgery Channel has had no new updates for 10 years (https://www.youtube.com/user/SVSChannel). It is important to iterate that learners and established faculty will browse different video sources for their education. A study from the University of Iowa found that YouTube® and the SCORE portal were the most common sources of videos used by learners, while faculty preferred societal web pages and commercial videos. 3 Understandably, while learners try to incorporate the basics of the procedure, faculty is focused on updating or expanding their knowledge of recent technological advances. These observations highlight that curating the content of video needs to be cognizant of the different sets of consumers that may be interested in the presentations for fundamental education and advanced professional development. Finally, it is important to acknowledge that factually incorrect content is in abundance, and verified/trusted sources should be sought by learners and faculty to ensure appropriate material based on the standard of care is presented in high-quality video production.
Our study has notable limitations, including its design in the form of a cross-sectional study assessing YouTube® content (which is very dynamic) at a given point in time. There has been a diffusion of educational content across multiple video platforms (https://openmd.com/directory/medical-videos) and social media sites (X [aka Twitter] ® , TikTok®, Linked In®, and Threads®) and their content is not well cataloged and searchable for use or for research. While we sought to capture the video media that the average video-browsing customer would most likely encounter, we acknowledge that this study does not serve as a systematic review due to the abundance of internet data. The paucity of videos pertaining to the topic evaluated is another limitation that hinders the generalization of our findings. However, a concept that we do wish to draw attention to is the scarcity of verified/trusted YouTube® educational content and the relative under-representation of vascular surgeons in producing high-quality educational videos on endovascular procedures. Evaluating such video content over a broader topic in vascular surgery on YouTube® and on other platforms will be a focus of future work.
Conclusion
There are very few YouTube® videos that focus on the technical aspects of DVT thrombolysis/thrombectomy. Existing videos vary significantly in educational content and have poor accountability metrics and suboptimal production attributes, which diminishes their educational value for a trainee. This study has identified a need for the provision of curated, peer-reviewed, high-quality resources directed to the education of interventional trainees and guidelines for the production of procedural videos that professional societies can endorse. The ideal video should have an introduction with educational objectives and provide a stable Image with an appropriate Image depth, Image contrast, and Image resolution. It should transition appropriately between scenes and encompass the entire designated procedure. A well-executed audio commentary enhances the content without any distracting background noise. The presence of captions and illustrations, as appropriate, improves visual education. A separate narrator from the operator also improves the flow of the video.
Footnotes
Author contributions
Study design: all authors
Data collection: all authors
Statistical analysis: all authors
Data interpretation: all authors
Manuscript draft: all authors
Critical revision: all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s note
This paper was presented in part at American Venous Forum, 32nd Annual Meeting, Virtual (Mar 3–6, 2021).
Guarantor
Mark G Davies.