
Abstract
Objectives
The aim of this systematic review is to assess the performance of graduated compression stockings (GCS) in comparison to no venous thromboembolism (VTE) prophylaxis in the prevention of hospital-acquired thrombosis in low-risk surgical patients undergoing short-stay procedures.
Methods
Aligning with PRISMA guidelines, online databases MEDLINE and EMBASE, Cochrane Library® and trial registries were searched. Eligible articles reported the VTE rate in low-risk surgical patients either receiving GCS or no VTE prophylaxis.
Results
Narrative synthesis was performed on a single eligible article. The included study arm consisted of participants undergoing knee arthroscopy with the use of GCS alone reporting a total of 29 VTE events (4.4%), 16 of which were asymptomatic DVTs (2.4%).
Conclusion
There is a complete lack of evidence to support the use of GCS in the prevention of HAT for low-risk surgical patients. An adequately powered trial is required to provide level-IA evidence to support this practice.
Keywords
Background
Hospital-acquired thrombosis (HAT) is defined as any venous thromboembolism (VTE)-related event within 90 days of hospital admission, 1 a term that encompasses both deep vein thrombosis (DVT) and pulmonary embolism (PE). HAT is associated with significant morbidity, mortality and healthcare associated costs. In the UK, the annual mortality of VTE is estimated to be between 24,000 and 32,000 fatalities per year, with an associated direct and indirect cost as high as £640 million per year. 2 Financial models in the United States have estimated the annual cost of HAT to be in the region of $9.0-$18.2 billion. 3
The introduction of the Commissioning for Quality and Innovation (CQUIN) payment framework mandated a 95% target for completion of VTE risk assessment for hospital inpatients within the UK National Health Service (NHS). This initiative has successfully resulted in a decline in HAT, with observed annual VTE-related deaths as low as 92% of the estimated expected rate for 2012 based on data from 2006–2007. 4 Despite national secondary care health interventions, HAT still accounts for significant morbidity and mortality with 57.1 VTE-related death per 100,000 hospital admission in 2018–2019 within the NHS. 1 Pulmonary embolism is a potentially fatal consequence of HAT. From 2018–2019, based on the Hospital Episode Statistics (HES) data from the NHS, there were 113,000 cases of PE in the UK. 5 This is considerably higher than the 79,000 cases reported from the 2012-2013 period. 6
After experiencing a DVT, an estimated 52.6% of patients go on to develop post-thrombotic syndrome (PTS) 7 as characterised by symptoms of chronic venous insufficiency such as leg pain, oedema and skin changes which are a significant source of morbidity and cost. 8
These complications compromise function and quality of life with a disability burden easily comparable to chronic obstructive pulmonary disease. 9 Prevention of HAT is therefore key in reducing morbidity, mortality and cost.
Previous modelling has estimated that the probability of untreated moderate-risk surgical inpatients developing HAT is as high as 15%, reducing to 4.1% with pharmacological and mechanical prophylaxis. 10 Most recently, a large randomised-controlled trial (RCT) assessing the use of GCS in addition to low molecular weight heparin (LMWH) for the prevention of VTE in moderate and high risk elective surgical patients estimated the rate of VTE to be as low as 1.4%. 11
However, little is known about the rate of HAT in low-risk surgical patients such as those undergoing day case procedures or those only requiring a short inpatient stay, with a short general anaesthetic time or loco-regional anaesthesia.
The UK National Institute for Health and Care Excellence (NICE) 2018 guidelines recommend that all patients undergo risk assessment to guide the prescription of pharmacological prophylaxis. 12 It also states that patients undergoing a procedure in which the anaesthetic and surgical time extends to 90 minutes receive a minimum of GCS to reduce the risk of HAT. Furthermore, it also recommends that patients undergoing abdominal, head, and neck procedures receive GCS – this includes low-risk procedures such as day case hernia repair. The interpretation of these guidelines has meant that patients receiving a general anaesthetic for a day case or short stay procedure receive GCS despite being ambulant and discharged early or on the same day. 12
The aim of this systematic review is to assess the benefit of graduated compression stockings in the prevention of venous thromboembolism in low-risk surgical patients.
Methods
This systematic review was undertaken in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines according to a pre-defined protocol. 13
Search strategy
The OVID® online platform was used to search MEDLINE and EMBASE databases on 11th March 2020 retrieving articles from 1946 to 2020. The Cochrane Library® online platform was used to search the Cochrane Database on 11/03/2020 to search for Cochrane evidence reviews. Corresponding online platforms or websites were used to search through the following RCT registries: ClinicalTrials.gov®, European Union Clinical Trials®, and the International Standard Randomised Controlled Trial Number (ISRCTN) Registry®.
The search strategy consisted of 45 search terms (see Figure 1) and was composed of key words and topic searches covering four themes: VTE, GCS, low-risk surgical patients, and RCTs. The searches were performed based on “Title and Abstract”. No automated field search limitations were imposed regarding date, study design or language. To increase the sensitivity of the search, the reference lists of included articles and relevant systematic reviews and evidence reviews12,14 were also screened using the same search criteria for further eligible articles.
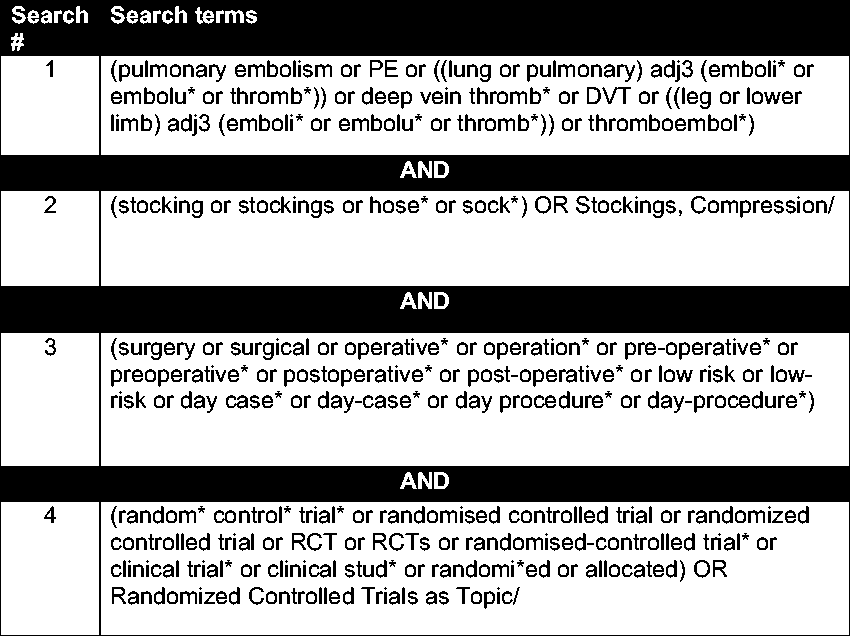
Search strategy executed on online platform OVID® used to search online databases MEDLINE and EMBASE.
Eligibility criteria
Eligible studies were those performed in secondary care recruiting low-risk surgical inpatients undergoing either short-stay or day-case benign (non-cancer) procedures. Short stay procedures have been defined as those requiring a length of stay less than 48 hours in duration. These procedures will be elective or planned. Emergency admissions are associated with an increased risk of HAT and hence would not be eligible.
Included articles had the following characteristics:
RCTs comparing the VTE rate in low-risk surgical patients undergoing day case or short stay procedures not prescribed GCS in comparison to those receiving GCS (standard practice) Single arms of an RCT reporting the VTE rate in low-risk surgical patients undergoing day case procedures not prescribed GCS or receiving GCS, i.e. single arms of RCTs were included Low-risk patients defined as per the UK Department of Health VTE Risk Assessment Tool
12
For studies that have been undertaken outside the UK, the population reported was compared to the UK Department of Health Risk Assessment Tool to assess eligibility
Excluded articles had the following characteristics:
Articles reporting study arms with more than one form of mechanical prophylaxis, e.g. intermittent pneumatic compression and GCS Articles reporting emergency surgical admissions Articles reporting surgical patients deemed moderate or high-risk of VTE as per the UK Department of Health VTE Risk Assessment Tool
12
Articles reporting non-original research, e.g. narrative review articles Articles in which the full-text was not available in the English language Conference abstracts that were not published as full-text publications in a peer-reviewed journal Articles that were duplicate publications, i.e. have been previously published as full-text publications Articles conducted using data from animals, i.e. non-human studies Case reports, retrospective cohort studies and quasi-randomised prospective studies
Conference abstracts were excluded as these have not undergone peer-review and a thorough scrutiny of methodology is important when making this comparison as it is subject to confounding variables with a likely small effect size. Case reports were excluded as the pathology and intervention are not novel and are unlikely to provide meaningful evidence. Cohort studies were excluded as this comparison is extremely likely to have confounding variables that are unlikely to be sufficiently controlled for outside an RCT setting.
Article screening
Articles retrieved from the online database search were screened against the inclusion criteria based on Title and Abstract by two reviewers (MM, HCY) independently using EndNote X9®. Mediation of articles to be included was carried out independently by a third reviewer (SS). Eligible articles then underwent full-text review again by two authors (MM, HCY).
Data extraction
Two reviewers (MM, HCY) extracted the data using a template in Microsoft Excel 2013©. Key data included: first author, title, year of publication, location, number of participants, intervention arm, control arm standard, procedure performed, length of stay (when reported), length of follow-up, definition of VTE event/diagnostic imaging used, number of DVT, number of PE, and mortality. Any discrepancies in the data extraction were mediated by a third reviewer (SS).
Quality assessment
The online platform GradePro® was used to undertake Grading of Recommendations Assessment, Development and Evaluation (GRADE).However, given the lack of data retrieved, all areas of quality assessment were deemed to be poor quality. Hence, there is low certainty in the outcomes reported.
Data synthesis
Data was analysed on the platform RevMan 5® with the intention of calculating I2 value prior to pooling the data. However, there was insufficient data to undertake quantitative synthesis. Therefore, a narrative synthesis was performed.
Results
Literature search
Searches of online databases and trial registries returned 439 articles, of which 314 were unique (Figure 2). After screening by two authors on title and abstract 282 articles were excluded.
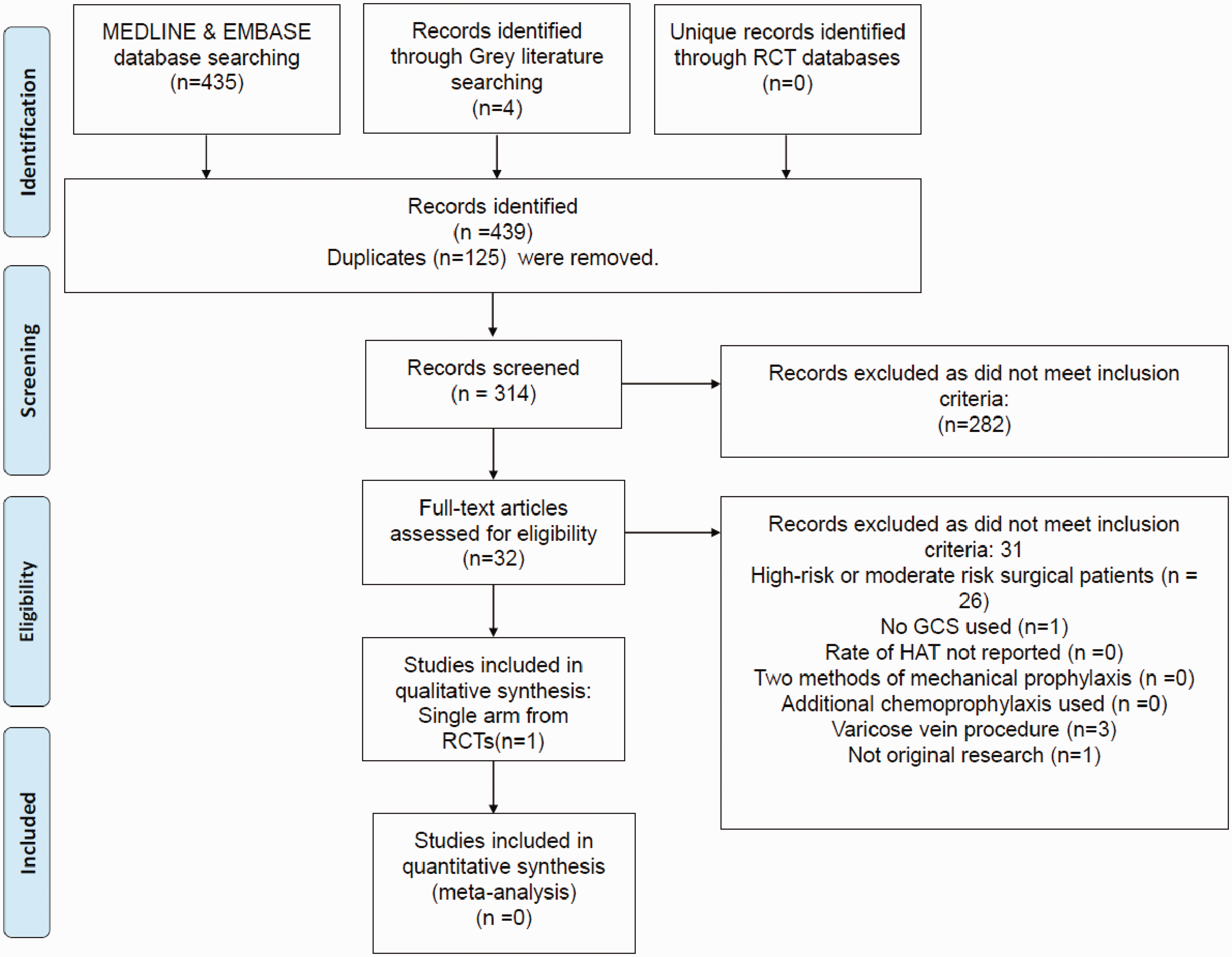
PRISMA flow-chart illustrating article screening and subsequent inclusion.
Subsequent full-text review of 32 articles took place. Importantly, a further 29 articles were excluded as they included patients at moderate or high-risk of HAT.15–43 After full-text exclusions took place, a narrative synthesis was performed on a single article. 44
Study characteristics (Table 1)
There were no RCTs identified comparing the use of GCS in comparison to no thromboprophylaxis in low-risk surgical patients. A single RCT from 2008 containing a study arm meeting the inclusion criteria was identified. 44 This study arm included 1761 low-risk patients undergoing knee arthroscopy receiving GCS alone for VTE prevention. The comparative arm included patients receiving low-molecular weight heparin. The study group consisted of young patients with a mean age of 42.3 years having arthroscopic procedures under loco-regional anaesthesia.
Study characteristics for included article.

RCT: randomised controlled trial.
Diagnosis of asymptomatic and symptomatic DVT was made via scheduled lower limb Doppler ultrasonography at day 8 post procedure. Symptomatic DVT and PEs were investigated based on symptomatology elicited by telephone follow-up. There was no screening for asymptomatic PE.
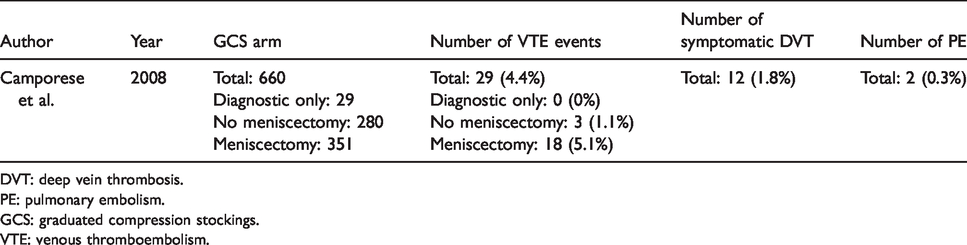
Rates of DVT and PE (Table 2)
There was a total of 29 VTE events (4.4%), 16 of which were asymptomatic distal DVTs (2.4%). The rate of symptomatic DVT was low with only 12 participants (1.8%) at 3 months reporting symptomatic DVT – with only 1 proximal symptomatic DVT (0.15%). A single patient suffered a symptomatic PE (0.3%).
Reported rates of VTE, symptomatic DVT and PE for included article.
DVT: deep vein thrombosis.
PE: pulmonary embolism.
GCS: graduated compression stockings.
VTE: venous thromboembolism.
Subgroup analysis demonstrated that the rate of VTE was lowest in diagnostic only procedures at 0%. The rate of VTE was highest in procedures involving meniscectomy (5.1%).
Quality of evidence
A single trial arm was identified, with no comparative studies identified. There is a high-risk of bias and hence the quality of evidence is low. All domains of the GRADE, such as indirectness, inconsistency, and imprecision, were graded as low certainty i.e. low quality.
Excluded RCTs assessing the use of GCS in comparison to no prophylaxis (see Table 3a)
There were 9 RCTs15–18,20,24,31,36,41 identified in the article screening process, consisting of moderate and high-risk surgical patients, assessing the use of GCS in comparison to no prophylaxis in the reduction of HAT. These articles were excluded from the review as they did not match the inclusion criteria of low-risk surgical patients. Articles consisted of participants undergoing major abdominal, major gynaecological, neurosurgical, joint arthroplasty, and varicose vein procedures. Notably, the varicose vein procedures were performed as a day-case procedure, however, interventions in such proximity to the deep venous system represent a higher risk of VTE.
Importantly, each of these studies included participants at much higher risk of VTE in comparison to those undergoing short stay or day case procedures. This is reflected by the rates of HAT in these articles generally being much higher in comparison to the 2% symptomatic HAT rate reported in the included study arm. Interestingly, the highest rate of HAT from these excluded articles was 48.9% in a study arm of participants undergoing major abdominal, pelvic, or thoracic procedures. 17
Excluded articles containing single study arms (see Table 3b)
There were 20 articles identified in the article screening process, which were subsequently excluded, consisting of moderate and high-risk surgical patients containing a single study arm assessing the use of GCS alone in the reduction of HAT.19,21–23,25–30,32–35,37–40,42,43 All of the study arms consisted of patients using GCS without the addition of LMWH. The rate of HAT was as high as 59.2% in patients undergoing knee surgery. The rate of HAT across study arms was highly variable with three articles reporting a rate of 0%.34,38,39
Discussion
This systematic review failed to identify any RCTs assessing the use of GCS in VTE prevention for low-risk surgical patients undergoing operations as a day case or short stay procedure. The evidence for the use of GCS in VTE prevention for low-risk surgical patients is poor. We have provided an update on this topic which, to our knowledge, is the first of its kind to specifically search for low-risk surgical patients. The Cochrane Review published in 2018 assessed the use of GCS in VTE prevention for medical and surgical inpatients also failed to identify any articles assessing the use of GCS in low-risk surgical patients. 14 Additionally, the NICE Evidence Review published in 2018 as part of the “Venous Thromboembolism in over 16 s” clinical guideline also failed to identify any articles in this topic area. 12
The single arm included in this review, published in 2008, provides useful data as a foundation for sample size calculation for future RCTs. The event rate of 4.4% in low-risk patients wearing GCS is higher than one would expect for ambulant patients not requiring admission. Duration to ambulation for knee arthroscopy is generally short. The higher than expected rate could be due to some participants remaining non weight-bearing on the operated side with the use of crutches. Most notably, those that underwent meniscectomy were non-weight bearing for 3 weeks. Sub-group analysis revealed that those undergoing arthroscopy without meniscectomy (n = 280) had 3 VTE events (1.1%), in comparison those that had meniscectomy (n = 351) suffered 18 VTE events (5.1%) i.e. those undergoing a more invasive procedure with a longer duration of immobility were more likely to suffer from HAT.
When designing an RCT, consideration is made of epidemiological data reporting pragmatic rates of HAT published outside of RCTs. Linked primary care databases in the UK have been used to estimate the rate of HAT after day case procedures. The symptomatic VTE rate for day-case cholecystectomy and inguinal hernia repair is approximately 0.3% using this population-level data. 45 These patients are given GCS for mechanical prophylaxis as standard practice. However, low-risk patients also encompass those with short-stays so the expected rate for an RCT would be marginally higher. Using the more conservative estimate identified in this review of 1.1% in low-risk early ambulant patients, in addition to the population-level data, it would be reasonable to conclude a purposefully conservative expected event rate of 0.5% in the intervention arm. For this intervention, one would likely use a superiority comparison based on a dichotomous outcome with a 0.5% difference at 90% power and a significance level of 5%. The primary outcome would likely be assessor-blinded symptomatic HAT at 90 days, with last follow-up being telephone consultation and only undertaking imaging when clinically indicated. For sufficient power for the primary outcome, 6254 participants per arm are required equalling a total sample size of 12,508. Allowing for 15% loss to follow up, the total sample, randomised 1:1 between the two groups, is 14,715 participants. The cost of a pragmatic trial of this size with a primary outcome of symptomatic HAT would be in the region of £1 million and take ∼5 years. The cost of a possible trial is significantly less than that is spent on GCS on low-risk patients in a single year within the NHS.
The results from studies containing patients at moderate and high-risk of HAT, which were excluded from this review, demonstrated a clear reduction in HAT for those wearing GCS in comparison to those with no prophylaxis (Table 3a). However, these studies included patients that are very likely to develop HAT (with rates of up to 48.9%) which represents an entirely distinct population to those patients at low-risk of HAT with estimated event rates of just 0.5 – 1%. These alarming rates of HAT are an important reminder that chemoprophylaxis is instrumental for high-risk patients. However, it does not support the use of GCS in low-risk patients as these studies represent a different patient cohort.
Study characteristics and rates of VTE from excluded articles consisting of moderate-risk and high-risk surgical patients.
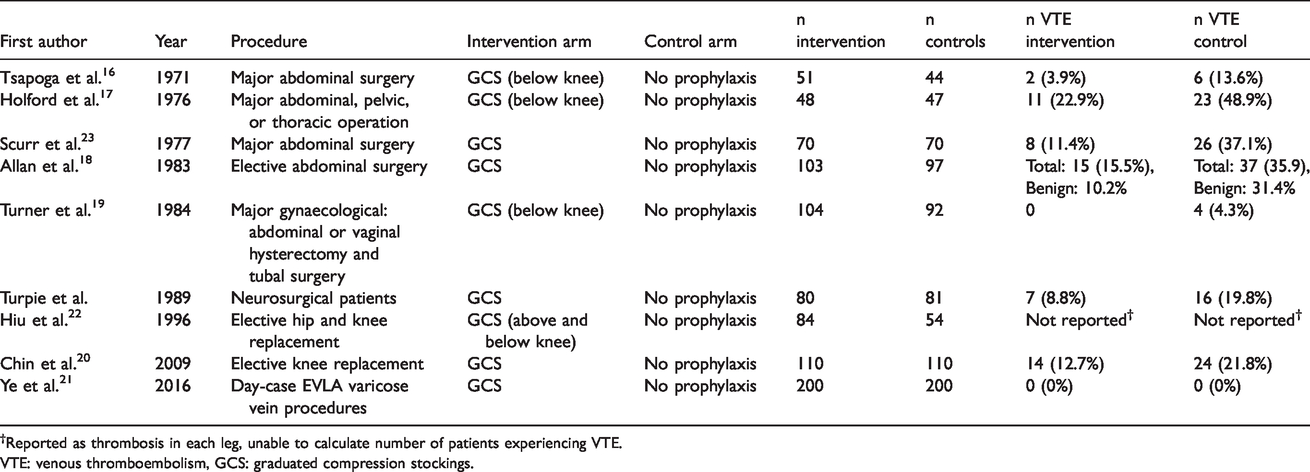
†Reported as thrombosis in each leg, unable to calculate number of patients experiencing VTE.
VTE: venous thromboembolism, GCS: graduated compression stockings.
Study details and from excluded study arms consisting of moderate-risk and high-risk surgical patients.
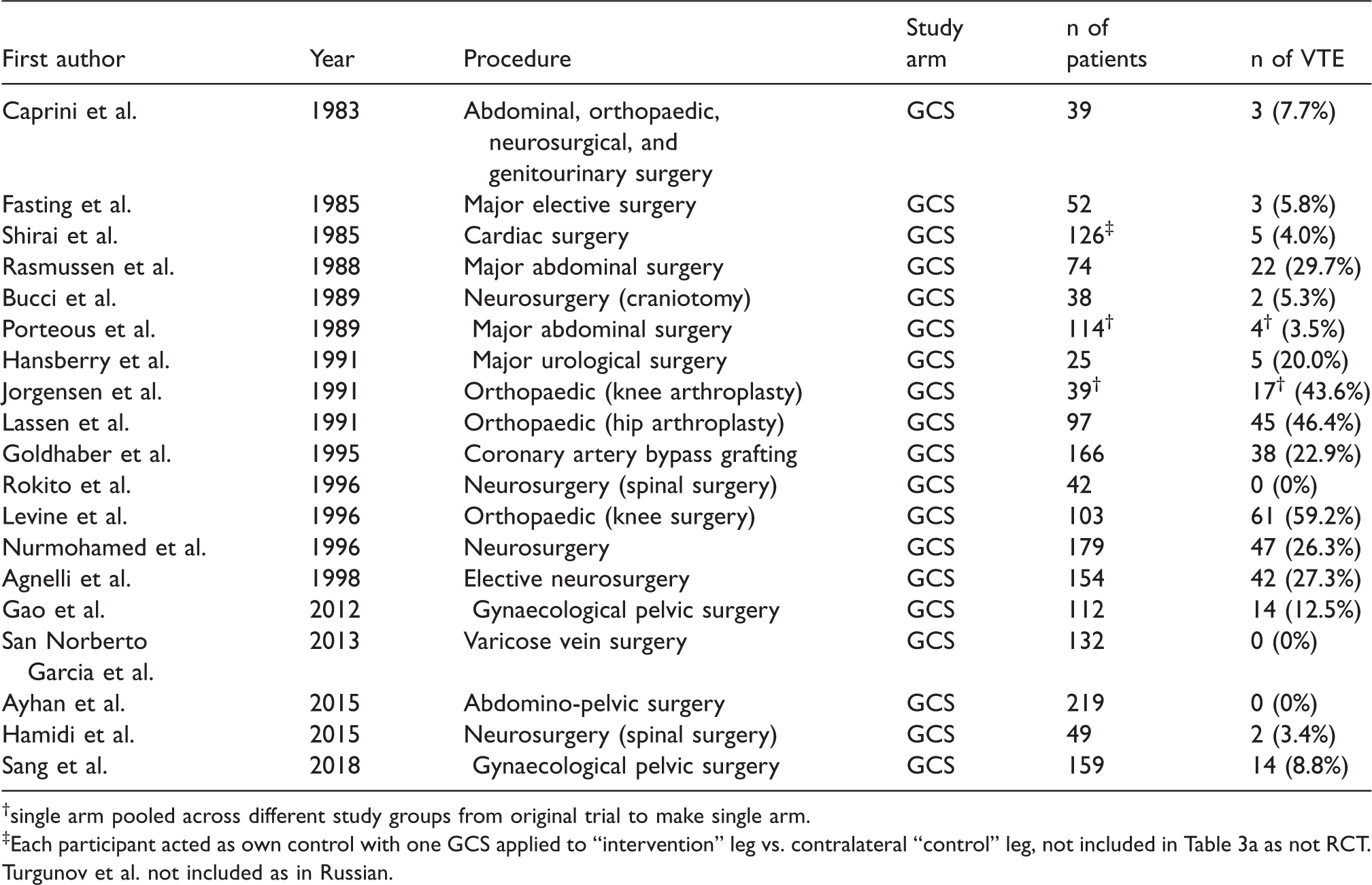
†single arm pooled across different study groups from original trial to make single arm.
‡Each participant acted as own control with one GCS applied to “intervention” leg vs. contralateral “control” leg, not included in Table 3a as not RCT.
Turgunov et al. not included as in Russian.
The findings of this article are important as GCS are associated with a significant cost and can have significant adverse effects. These resources can be re-distributed if proven to be ineffective. An example of this cost is the use of GCS in day case procedures. Within the UK NHS, the proportion of day case procedures has increased annually, in 2018-2019 35.6% of procedures performed as a day case without requiring overnight stay. 46 NHS HES reported 889,671 “miscellaneous” procedures undertaken in the 2018–2019 with a median length of stay of 1 day, notably a proportion of which will not use GCS. 47 This does not include an additional 130,110 abdominal wall procedures with a median length of stay of 1 day. 47
Together, it can be illustrated that there is up to 1-million day case interventions within the NHS over a one year period. Each pair of stockings costs between £3.86 and £9.12 and the cost for applying GCS to a patient is equal to £23, this making the unit cost of purchasing and applying GCS £26.86 – £32.12. 12 This cost for day case abdominal procedures alone would amount to approximately £38,55,000 per annum (equating to ∼€4,217,000 or ∼$4,736,000), without including the additional 889,671 miscellaneous procedures undertaken.
Furthermore, GCS have been reported as being associated with adverse outcomes such as discomfort, blistering, and formation of a constrictive band, and ischaemia which also have additional associated healthcare costs. 48
Recent presentation of the results from a large RCT assessing the use of GCS in addition to LMWH for the prevention of VTE in moderate and high risk elective surgical patients demonstrated that LMWH alone was non-inferior to the combination of GCS and LMWH for thromboprophylaxis. 11
This further brings into question the role of GCS in the prevention of VTE in the context of modern surgery and anaesthesia with, for example, minimally invasive techniques, early ambulation, enhanced recovery and shorter lengths of stay. However, limited inferences can be drawn from this trial as it included moderate to high-risk patients who were receiving LMWH. Nevertheless, the lack of additional efficacy suggests our assumptions of the added benefit of GCS may be displaced. This is on the background of large medical RCTs such as the CLOTS-1 trial which randomised 2518 acute stroke patients to either LMWH alone or dual prophylaxis and reported no difference for symptomatic or asymptomatic femoropopliteal thrombosis. 48
Limitations
Unfortunately, due to the lack of evidence supporting the use of GCS in low-risk surgical patients, only a single study arm was included in this review. This limits the conclusions that can be drawn on the performance of GCS in prevention of HAT in patients undergoing short-stay procedures.
A range of databases and trial registries were searched, in addition to existing evidence reviews, to identify eligible articles results in a comprehensive search strategy. However, articles not published in the searched databases may have been missed.
Lastly, the exclusion of conference abstracts could be criticised as excluding the latest research. However, conference abstracts were excluded as they had not undergone peer-review to ensure that any included data had been rigorously assessed prior to publication.
Conclusion
This systematic review has illustrated the lack of evidence relating to the use of GCS in the prevention of VTE for low-risk surgical patients.
The limited evidence base has resulted in lack of data to estimate VTE rates in low-risk surgical patients. This review provides a contemporary review of this evidence and offers a basis for future RCTs. A future RCT is required to provide level 1 evidence to support or refine current practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Infrastructure support for this work was provided by the NIHR Imperial Biomedical Research Centre.
Ethical approval
Not required as secondary research project.
Guarantor
AHD.
Contributorship
Study design: AHD, JS, MM, Smith S. Data collection: MM, HCY, Salim S. Data analysis: MM, HCY, Salim S, Smith S. Writing: MM, HCY, Salim S, Smith S, JS, AHD.
Acknowledgements
N/A.