
Abstract
Objective
To reach consensus on which complications of varicose vein treatments physicians consider major or minor, in order to standardize the informed consent procedure and improve shared decision-making.
Methods
Using the e-Delphi method, expert physicians from 10 countries were asked to rate complications as “major” or “minor” on a 5-point Likert scale. Reference articles from a Cochrane review on varicose veins were used to compose the list of complications.
Results
Participating experts reached consensus on 12 major complications: allergic reaction, cellulitis requiring intravenous antibiotics/intensive care, wound infection requiring debridement, hemorrhage requiring blood transfusion/surgical intervention, pulmonary embolism, skin necrosis requiring surgery, arteriovenous fistula requiring repair, deep venous thrombosis, lymphocele, thermal injury, transient ischemic attack/stroke, and permanent discoloration.
Conclusion
An international consensus was reached about what physicians consider to be major complications of varicose vein treatments. This consensus may assist in standardizing the information physicians discuss with patients prior to varicose vein treatment.
Introduction
The possible complications discussed by physicians with patients prior to varicose vein (VV) treatment vary.1,2 The “major” and most frequently occurring complications are usually discussed. However, no uniformity exists on which specific major complications should be discussed.
Understanding and agreeing upon which major complications to discuss with patients would harmonize how physicians inform their patients and obtain informed consent. This would also help physicians to engage patients in shared decision-making, if multiple similarly effective treatment options are available. However, for effective shared decision-making to take place, it is crucial that patients are aware of the possible major complications to be able to adequately balance the benefits and harms of the available treatment options.
In a joint venture the American Venous Forum and the Society of Interventional Radiology developed reporting standards to harmonize and standardize the reporting of postintervention complications. 3 These reporting standards facilitate the comparison of results between studies and improve the overall quality of clinical research on venous disease. However, this document was not designed to specify those specific major complications that should be discussed with patients in the consulting room.
We therefore set out to reach consensus on which specific complications following VV treatment are major and which are minor using the expert opinions of VV physicians throughout Europe and North America.
Methods
Delphi method
The Delphi method is a widely recognized iterative process designed to achieve consensus from a group of experts using a series of questionnaires interspersed with feedback. Electronically distributed questionnaires are predesigned and completed by experts. Subsequent questionnaires are adapted based on the results of the previous version. The process stops when consensus is reached. 4
Experts
With the permission of the organizers of the 2015 VEITH symposium and via the Dutch Society for Vascular Surgery, we invited European and North American vascular surgeons, dermatologists, and phlebologists to participate in this electronic Delphi study.
Listing of complications
The list of possible complications was composed by presenting both 30-day and long-term complications of sclerotherapy, foam sclerotherapy, endovascular procedures, and open surgery.5–17 We extracted all complications from reference articles in the Cochrane systematic review on VV treatment of Nesbitt et al. 18 Since the different treatment options for VV have many possible complications in common, these complications were all included in one questionnaire. The first round started with a total of 20 complications.
Treatment complications can lead to mild, moderate, or severe sequelae. Therefore, all complications were described extensively, based on the three-tiered severity scoring system from reporting standards for other vascular diseases.19–21 For example, the complication “arteriovenous fistula” is divided into a “mild” level arteriovenous fistula if no additional intervention is required, a “moderate” level if endovascular repair is required, and a “severe” level if surgical repair is required. If the complication or its severity was not stated in the reporting standards, we used the Clavien–Dindo classification 22 together with information from the reference articles or daily practice. A few complications had only two levels of severity, for example discoloration that resolves after six weeks and permanent discoloration. To avoid ranking bias when composing the surveys, the complications were presented in alphabetical order.
Composing the surveys
As is shown in Figure 1, the differing levels of complication severity were introduced in a stepwise manner to avoid extensive surveys containing all 20 complications, each with up to three levels of severity.
Flowchart to introduce different severity levels of complications into the five DISCOVAR Delphi rounds.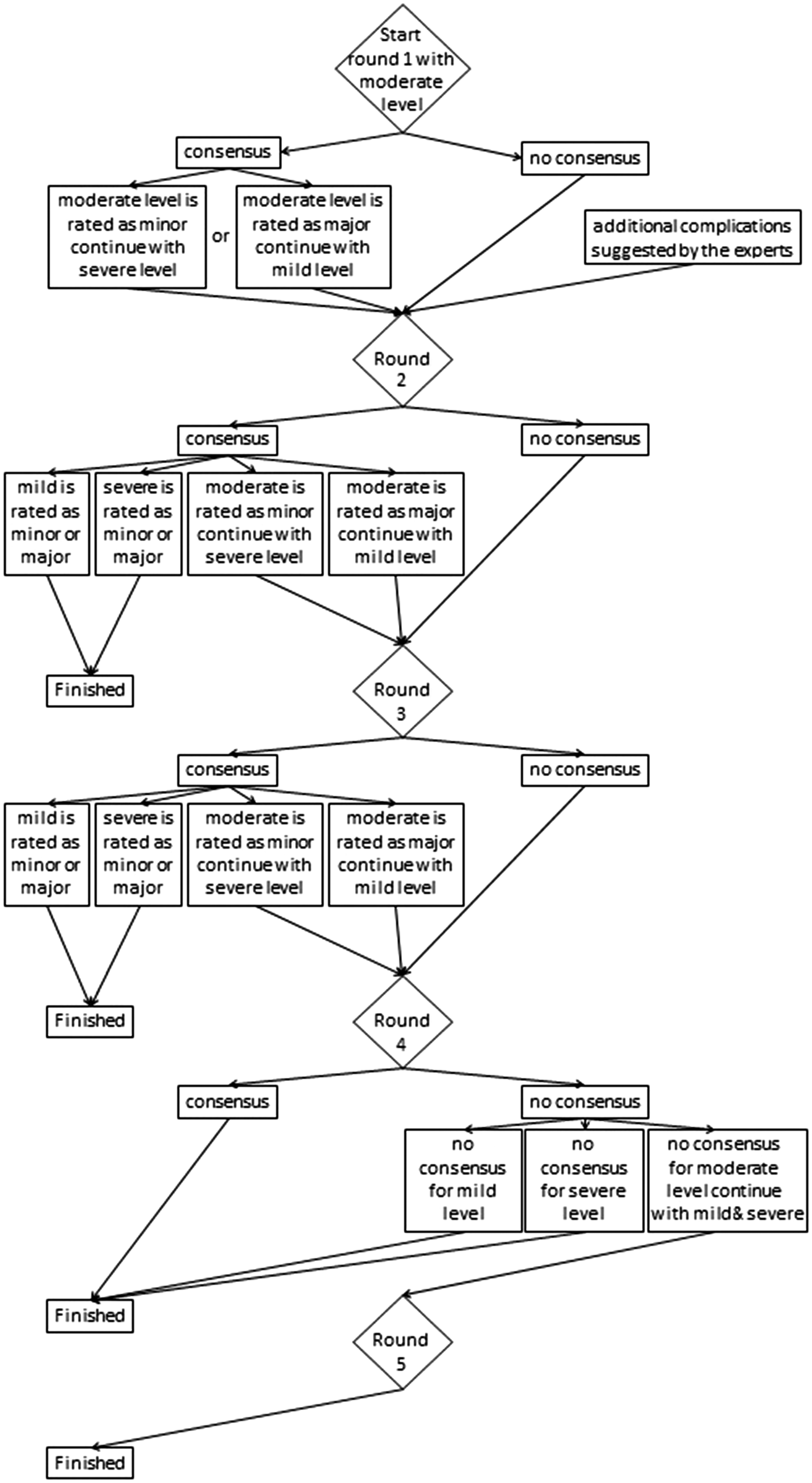
The first Delphi round started by presenting the moderate level of severity for complications. If the physicians rated this moderate level as a minor complication, the assumption was made that the corresponding mild level would also be deemed minor. In the next round the experts were asked to rate the severe level of this complication. Similarly, if the experts rated a moderate complication as major, the severe level was also deemed major. The experts were then asked to rate the mild level of the same complication in the next round.
For complications with only two levels of severity, the choice whether to start the first Delphi round with the mild or the severe level was made randomly. When consensus was reached on one level of severity, the same assumptions as mentioned in the previous paragraph were made. For instance, if a severe level was deemed to be a minor complication, the mild level was also assumed to be minor as well and vice versa.
If consensus was not reached in the first round, the physicians were asked to rate the same complication again in the next round. In subsequent rounds, each complication was now presented accompanied by the percentages of agreement obtained from the previous round. This allowed physicians to adjust their own rating based on the ratings of others.
Study conduct
SurveyMonkey (San Mateo, California, USA), an online survey tool, was used to develop and distribute the surveys. The complications presented in the survey were rated by the physicians using a 5-point Likert scale, ranging from 1 (definitely minor) to 5 (definitely major). If at least 80% of physicians rated a complication with a Likert score of 1 or 2, this complication was considered to be minor. Likewise, if 80% of the physicians rated a complication with Likert score 4 or 5, this complication was considered to be major.
During the first round, the physicians were able to propose any additional complications they considered to be missing from the survey. These complications were then included in the second round. In each round, physicians were given at least two weeks to respond to the survey.
Four Delphi rounds were planned as this was considered sufficient for reaching consensus. However, after fourth round we added a fifth round to ask physicians to rate the remaining complications that had not been presented in previous rounds due to the stepwise manner of introducing the complications.
Data analysis
The internal consistency of the first Delphi round was calculated using Cronbach’s alpha using IBM SPSS Statistics version 23 (Armonk, New York, USA). A Cronbach’s alpha outcome of 0.7 or higher is considered to be acceptable and an outcome of 0.9 or higher is considered excellent. 23
Results
For this Delphi study we invited 43 vascular surgeons, five dermatologists, and one phlebologist to participate. Eleven vascular surgeons and one phlebologist accepted our invitation and participated in the first round (response rate of 24%). The physicians performed a median number of 300 (range 200–1500) VV interventions annually. Physicians from the first Delphi round were affiliated to medical centers in the United States of America, Austria, the United Kingdom, and the Netherlands. Six vascular surgeons and one phlebologist participated in the final round (14% response rate).
In the first round, physicians proposed the following additional complications: contact allergy, arteriovenous fistula, transient ischemic attack or stroke, and incomplete obliteration. The Cronbach’s alpha score was 0.93.
List of complications on which consensus was reached for varicose vein treatment.
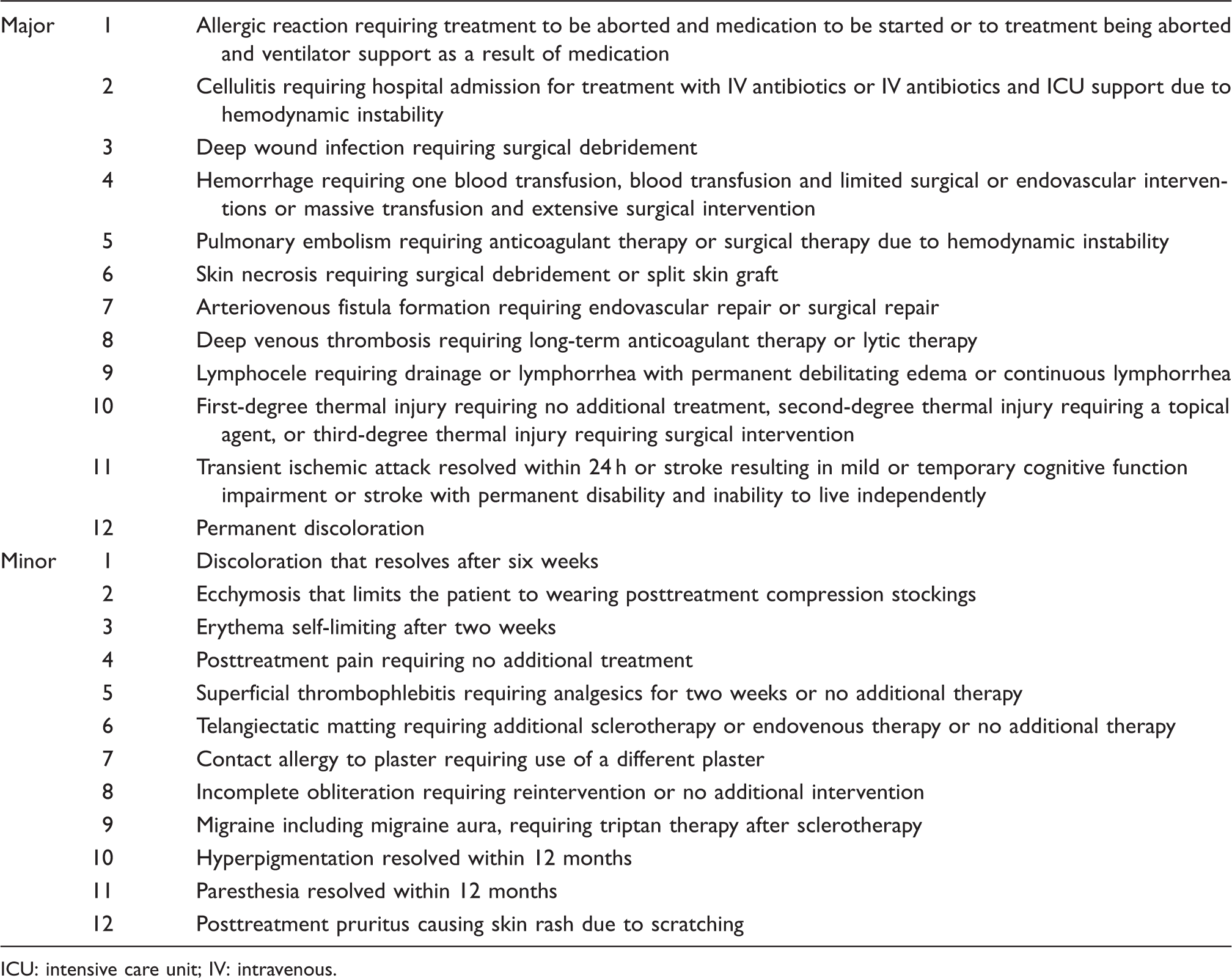
ICU: intensive care unit; IV: intravenous.
Discussion
Our Delphi study shows that physicians reached consensus on 12 major and 12 minor complications of VV treatment. The consensus on these complications may assist physicians when informing patients about the associated potential risks of the VV treatments for which the patient is eligible.
To decide which complications should be discussed with patients prior to treatment remains a difficult but important topic. On the one hand, physicians want their patients to be fully informed about their possible treatment options. On the other hand, physicians do not want to frighten or overwhelm patients by presenting every potential complication. 24 For example, most VV physicians will not discuss the risk of stroke with permanent disability after foam sclerotherapy due to an air embolism in patients with a patent foramen ovale. 25 Nevertheless, many patients do want more information than is given by their physicians. 26
Legislation on informed consent in the United Kingdom requires physicians to discuss the risks a reasonable person in the patient’s position would deem of significance or the risks deemed of significance by this particular patient. 27 In the Netherlands, the Royal Dutch Medical Association (KNMG) provides information on informed consent, which is also based on court rulings. The KNMG states that complications occurring in more than 1% of patients must be discussed, in addition to those major complications that occur less often. 28 Unfortunately, both the UK and Dutch laws and professional societies do not provide detailed information about the type of major or significant complications physicians need to discuss. Also for minor complications, perhaps the arbitrary cutoff point of 1% should be lower for VV treatment, since it is often performed for non-limb-threatening symptoms or cosmetic reasons.
The consensus reached in our study appears to provide an appropriate group of major complications to discuss with patients. However, this is currently only based on what physicians deem to be major complications for discussion with the patient. Future studies should analyze if patients agree that these are the complications they want to be informed about. Combining the physician’s view and the patient’s view may help to close the physician–patient information gap 29 and could empower VV patients to engage in shared decision-making. This seems particularly relevant for VV patients because of the existence of several treatment options, including no treatment (at least initially). All these options have their merits and disadvantages and can be weighed against the patients’ burden of disease. Thus, information should be provided about complications that might influence a reasonable patient’s view on a treatment. 30 The consensus list of major complications from our Delphi study may assist VV physicians on deciding which complications to discuss with their patients.
The strengths of this study are first of all that the participating physicians were experienced and originated from four different countries practicing Western medicine. This suggests that the results of our study are valid for a wide range of Western countries. Second, the items in our first survey round had a high Cronbach’s alpha score. This indicates that the questions asked belonged to a single construct, which is likely since all items were about possible complications after VV treatment. Third, the list of complications was quite comprehensive, since few additional complications were added based on the suggestions of the physicians.
One of the limitations of this study may first be the limited number of physicians that participated in our Delphi study and the withdrawal of five out of 12 experts after the first round. However, the literature suggests that the more participants, the lower the possibility of reaching consensus. Panel sizes of 5–30 participants are recommended. 4 Hence, we believe our panel size was sufficient throughout the Delphi rounds. Second, none of the invited dermatologists participated in our study. Thus, unfortunately, no insight was gained into the expert opinion of dermatologists with regard to which complications from VV treatment they would deem minor or major. Perhaps, this absence of participating dermatologists may have led to an underestimation of the severity of cosmetic complications. Third, only physicians practicing Western medicine were invited. It is unclear whether involving participants from non-Western countries would have altered the consensus reached here.
In conclusion, this Delphi study rendered international consensus about which complications of VV treatment are considered minor and which major. This consensus may help to harmonize the information that physicians discuss with their patients prior to VV treatment.
Collaborators in the DISCOVAR study in alphabetical order
We would like to thank the following experts for participating in our Delphi study as part of the venous DISCOVARstudy group.
SA Black1, JR Boyle2, K Gibson3, MS Gohel2, JA Lawson4, MH Meissner5, MC Mooij4 and HJ Welch6
1Department of Vascular Surgery, Guy's and St Thomas Hospital, London, UK
2Department of Vascular Surgery, Addenbrooke's Hospital, Cambridge, UK
3Lake Washington Vascular Surgeons, Bellevue, USA
4Centrum Oosterwal, Alkmaar, The Netherlands
5Department of Surgery, University of Washington Medical Center, Seattle, USA
6Department of Vascular Surgery, Lahey Hospital and Medical Center, Burlington, USA
Supplemental Material
Supplemental material for Treatment of varicose veins, international consensus on which major complications to discuss with the patient: A Delphi study
Supplemental Material for Treatment of varicose veins, international consensus on which major complications to discuss with the patient: A Delphi study by Sylvana ML de Mik, Fabienne E Stubenrouch, Dink A Legemate, Ron Balm and Dirk T Ubbink in Phlebology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the AMC Foundation which was not involved in any way in the study design, data collection, data analysis, or interpretation of results.
Ethical approval
Ethical approval was not applicable. This article is a Delphi study in which only the expert opinion of vascular surgeons was used.
Guarantor
DTU.
Contributorship
SMLM: study design, data collection, data analysis, writing. FES: study design, data collection, writing. DAL: study design, data collection, data analysis, writing. RB: study design, data collection, data analysis, writing. DTU: study design, data collection, data analysis, writing. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.