
Abstract
Objectives
Methods
A multicenter, randomized, placebo-controlled, blinded study was conducted in patients with great saphenous vein incompetence and symptomatic and visible superficial venous disease. Co-primary endpoints were physician-assessed and patient-assessed appearance change from Baseline to Week 8.
Results
A total of 117 patients received treatment (38 placebo, 39 PEM 0.5%, 40 PEM 1%). Physician-rated vein appearance at Week 8 was significantly better with PEM (p = 0.001 vs. placebo); patient-assessed appearance trended similarly. Polidocanol endovenous microfoam provided improvements in clinically meaningful change in patient-assessed and physician-assessed appearance (p < 0.05), need for additional treatment (p < 0.05), saphenofemoral junction reflux elimination, symptoms, and QOL. In PEM recipients, the most frequent adverse event was superficial thrombophlebitis (35.4%)
Conclusions
Endovenous thermal ablation + PEM significantly improved physician-assessed appearance at Week 8, increased the proportion of patients with a clinically meaningful change in appearance, and reduced need for additional treatment. www.clinicaltrials.gov (NCT01197833)
Introduction
Varicose veins are extremely common worldwide, occurring most frequently in women.1–3 The most common clinical presentation of superficial venous incompetence is failure of the saphenofemoral junction (SFJ) of the great saphenous vein (GSV). 4 In recent practice, the proximal GSV has been most commonly treated with endovenous thermal ablation [ETA, e.g. radiofrequency ablation (RFA)]. ETA is not suitable for treatment of the distal (below-the-knee) GSV as it is associated with increased nerve injury. 5 It cannot treat tortuous veins and tributary or distal varicosities. 5 Therefore, other modalities are used to treat these types of veins.6–8
Physician-compounded foam, made with sclerosant and room air, has been reported as relatively safe. 9 However, there are numerous case reports of patients with significant neurological events including stroke, seizure, and transient ischemic attack due to gas embolism following treatment with foams made with nitrogen-rich room air.10–15 Polidocanol endovenous microfoam (PEM 1%, Varithena [polidocanol injectable foam], BTG International Ltd.) has been developed as a low-nitrogen microfoam for the treatment of varicose veins. The proprietary canister delivers microfoam with consistent physical characteristics, while the low-nitrogen characteristic allows rapid bubble absorption following injection into the vein.
The objective of the current study was to evaluate the efficacy and safety of PEM (0.5% and 1.0%) compared with placebo when used following ETA during the same treatment session in patients with SFJ incompetence, GSV reflux, and venous disease manifested by both symptomatic and visible varicosities.
Methods
This was a multicenter, randomized, placebo-controlled, parallel-group, blinded, phase 3 study conducted to evaluate the efficacy and safety of PEM 0.5% and 1.0% in combination with ETA (either laser or RFA) in the same treatment session. Patients were followed up for six months.
The study was conducted at seven investigator sites in the USA in accordance with the principles of the Declaration of Helsinki (1996). The protocol and informed consent form were approved by the relevant institutional review boards (Schulman Associates IRB, Inc., Cincinnati, OH; Chesapeake Research Review, Inc., Columbia, MD). All patients provided written informed consent.
Patients
Patients aged 18–75 years old were eligible if they had SFJ incompetence (reflux > 0.5 s) associated with incompetence of the GSV (where SFJ incompetence was the predominant source of reflux) and superficial venous disease manifested by both symptoms and visible varicosities. Patients had to be candidates for ETA of the proximal incompetent GSV who also required treatment for visible varicosities. Other entry criteria included a Clinical, Etiology, Anatomy, Pathophysiology (CEAP) grade C2-5; a score of ≥7 points on question 1 of the modified Venous Insufficiency Epidemiologic and Economic Study – Quality of Life/Symptoms (m-VEINES-QOL/Sym) questionnaire (described below); a patient-assessed rating for appearance of varicose veins of “moderately noticeable” or worse on the Patient Self-Assessment of Visible Varicose Veins (PA-V3) instrument described below; and a physician’s live rating for appearance of varicose veins of “moderate” or worse on the Independent Photography Review – Visible Varicose Veins (IPR-V3) instrument described below.
Treatment
Study drug could be used above and below the knee for visible varicosities and incompetent areas of the GSV system or tortuous areas of the saphenous trunk not treated with ETA. Patients were randomized prior to ETA on a 1:1:1 basis by a central automated interactive voice response system to receive ETA and either PEM 0.5% or 1.0% or placebo. Randomization was stratified by modality (laser, RFA) and Baseline PA-V3 score. The randomization of patient treatment assignments was generated by United BioSource Corporation (Blue Bell, PA, USA).
Unblinded ETA was immediately followed by treatment with either double-blind PEM (patients and care providers) or single-blind placebo (patients) in total volumes of ≤15 mL. Placebo was prepared and patient blinding to the administration of study drug was maintained as described previously. 16
Assessments
Appearance
The IPR-V3 and PA-V3 instruments for the assessment of varicose veins appearance were designed during the PEM development program according to FDA guidance.17,18
An IPR Panel of three experts independently scored standardized photographs (Baseline, Week 8, Month 6) for varicose veins appearance using the IPR-V3 instrument to arrive at the IPR-V3 score; response options were none (0 points), mild (1 point), moderate (2 points), severe (3 points), and very severe (4 points).17,18 Photographs were presented in random order. Reviewers were blinded to time point and treatment group.
Patients assessed the “live” appearance of their varicose veins, without reference to baseline photographs, using the PA-V3 instrument (Screening, Baseline, Week 4, Week 8, Month 6). Response options were Not at all noticeable (0 points), Slightly noticeable (1 point), Moderately noticeable (2 points), Very noticeable (3 points), and Extremely noticeable (4 points). 17
Overall post-treatment change in appearance was rated by patients using the Patient Global Impression of Change in Appearance (PGIC-Appearance) questionnaire to arrive at the PGIC score and by one IPR Panel reviewer using the Clinician Global Impression of Change in Appearance (CGIC-Appearance) questionnaire to arrive at the CGIC score at time points through Month 6. The assessor rated the change as Much worse (−3 points) to Much better/Much Improved (+3 points). 19 The clinician reviewer, blinded to treatment but not time point, reviewed Baseline and Week 8 (and Month 6) photographs of the patient’s leg side-by-side on a screen. To determine whether patients achieved a clinically meaningful change in appearance, responder analyses were performed. Patients who responded Moderately improved on the PGIC instrument (or had this reviewer rating [CGIC]) were considered to have achieved clinically meaningful change.
Additional assessments
Investigators determined the Venous Clinical Severity Score (VCSS) at Screening, Week 8, and Month 6.20,21 The VEINES-QOL/Sym instrument was modified for the study by shortening the four-week recall period to one week and adjusting the response options accordingly (m-VEINES-QOL/Sym) 22 and was administered at Baseline, Week 4, Week 8, and Month 6.
The need for additional treatment between Week 8 and Month 6 for residual varicose veins ≥3 mm in diameter (CEAP Clinical class ≥2) of the GSV system of the treated leg was recorded. Duplex ultrasound examination of superficial and deep veins was conducted at Baseline to confirm the treatment plan, and at Weeks 1, 4, and 8, and Month 6 for safety surveillance. Physiological response to treatment was assessed using duplex ultrasound in the patients who were treated for baseline residual reflux>0.5 s in the incompetent segments of trunk veins (distal GSV). Response to treatment in this subset was defined as elimination of reflux through the distal GSV and/or complete occlusion of the GSV.
Adverse events (AEs) monitoring was conducted through Week 8. Between Week 8 and Month 6, only serious AEs and venous thrombi events (proximal or distal thrombi and/or pulmonary emboli) were recorded. All patients were monitored for venous thrombi at Weeks 1, 4, and 8, and Month 6 via duplex ultrasound. Scans were more rigorous than the quality benchmark Intersocietal Commission for the Accreditation of Vascular Laboratories 2010 standards. All deep veins were interrogated with both compression and color flow from the malleoli upwards, at 2-cm intervals, including the veins of the calf muscle (gastrocnemius, soleal). Any venous thrombi in the PEM clinical program were reviewed and adjudicated by an independent venous thromboembolic event review board (VTERB) as previously described. 16 Venous thrombi were managed according to the site investigators’ usual practice, with additional duplex ultrasound examinations conducted until thrombi resolved or stabilized. Anticoagulant therapy of diagnosed deep vein thromboses (DVTs) was used at the investigators’ discretion and, when provided, was consistent with American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis guidelines. 23
Data analysis
Primary endpoints
The co-primary efficacy analysis compared absolute change from Baseline to Week 8 in IPR-V3 and PA-V3 scores for patients treated with ETA + PEM 0.5% and 1.0% dose concentrations (pooled) versus ETA + placebo using analysis of covariance (ANCOVA). Data summaries and listings were performed using SAS, Version 9.1.
Other endpoints
ANCOVA was conducted to analyze absolute change from Baseline to Week 8 in VCSS and m-VEINES-QOL scores. The Cochran–Mantel–Haenszel (CMH) Chi-square test, stratified by site, compared proportion of patients achieving clinically meaningful change and proportion who received additional treatment between Week 8 and Month 6 for residual varicose veins ≥ 3 mm in diameter.
To adjust for multiplicity, analysis of other endpoints was planned according to a hierarchical testing scheme. While one primary co-endpoint did not reach statistical significance, comparative results of other efficacy endpoints are still presented, although their p-values should be considered nominal. Missing data were imputed using the method of last observation carried forward for the co-primary endpoints.
Sample size
Sample size was selected to provide 95% power to detect an absolute difference of 0.65 in the change from Baseline at Week 8 on the IPR-V3 scale between the ETA + PEM group (using pooled PEM dose groups) and the ETA + placebo group, assuming a standard deviation of 0.80, using a two-sample t-test and a two-sided α = 0.05 significance level and allowing for ∼10% dropout.
Results
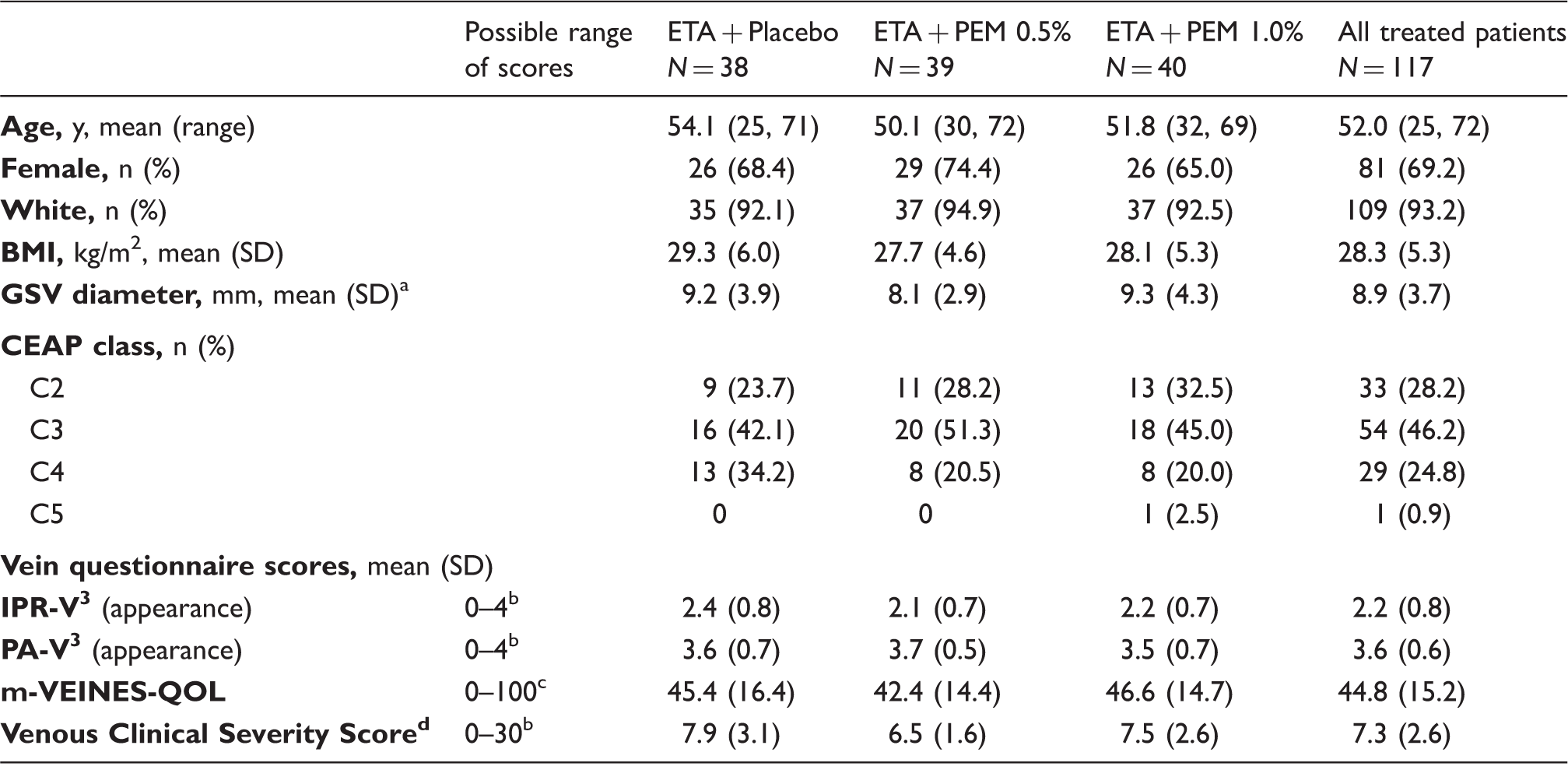
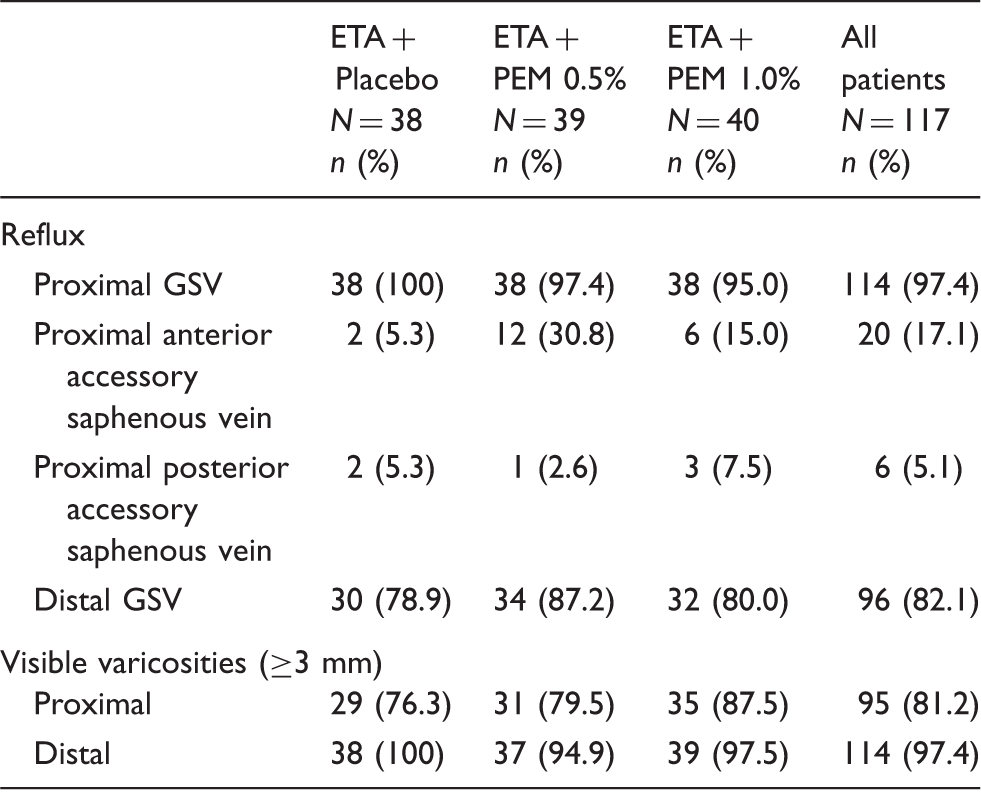
A total of 234 patients were screened; 117 received treatment (Figure 1). Baseline demographics and questionnaire scores were similar across treatment groups (Table 1). The distribution of CEAP Clinical classifications was C2 28%, C3 46%, C4 25%, and C5 1% (Table 1). Patients’ assessment of varicose veins appearance was higher than physicians’ [mean 3.6 vs. 2.2 points, possible score range 0–4, where 4=Very severe (IPR-V3) or Extremely noticeable (PA-V3)]. Distribution of reflux location was generally similar across groups as shown in Table 2 (proximal GSV in 97.4% of patients; anterior accessory GSV, 17.1%; posterior accessory GSV 5.1%). Laser and RFA were equally distributed among patients. The median volume of PEM administered was 12.0 mL and 13.0 mL in the PEM 0.5% and 1.0% groups, respectively.
Patient disposition. All patients who received treatment had endovenous thermal ablation therapy immediately prior to treatment with polidocanol endovenous microfoam (PEM) ablation or placebo. Patient demographics and baseline characteristics. BMI: body mass index; SD: standard deviation; GSV: great saphenous vein; CEAP: clinical, etiology, anatomy, pathophysiology. Screening values, only reported for veins with reflux, n = 38 for each treatment group, total N = 114. Lower scores indicate better status on IPR-V3, PA-V3, and VCSS instruments. Higher scores indicate better health status on m-VEINES-QOL instrument. Assessed at screening. Reflux and visible varicosities at Screening. Proximal refers to above the knee. Distal refers to below the knee.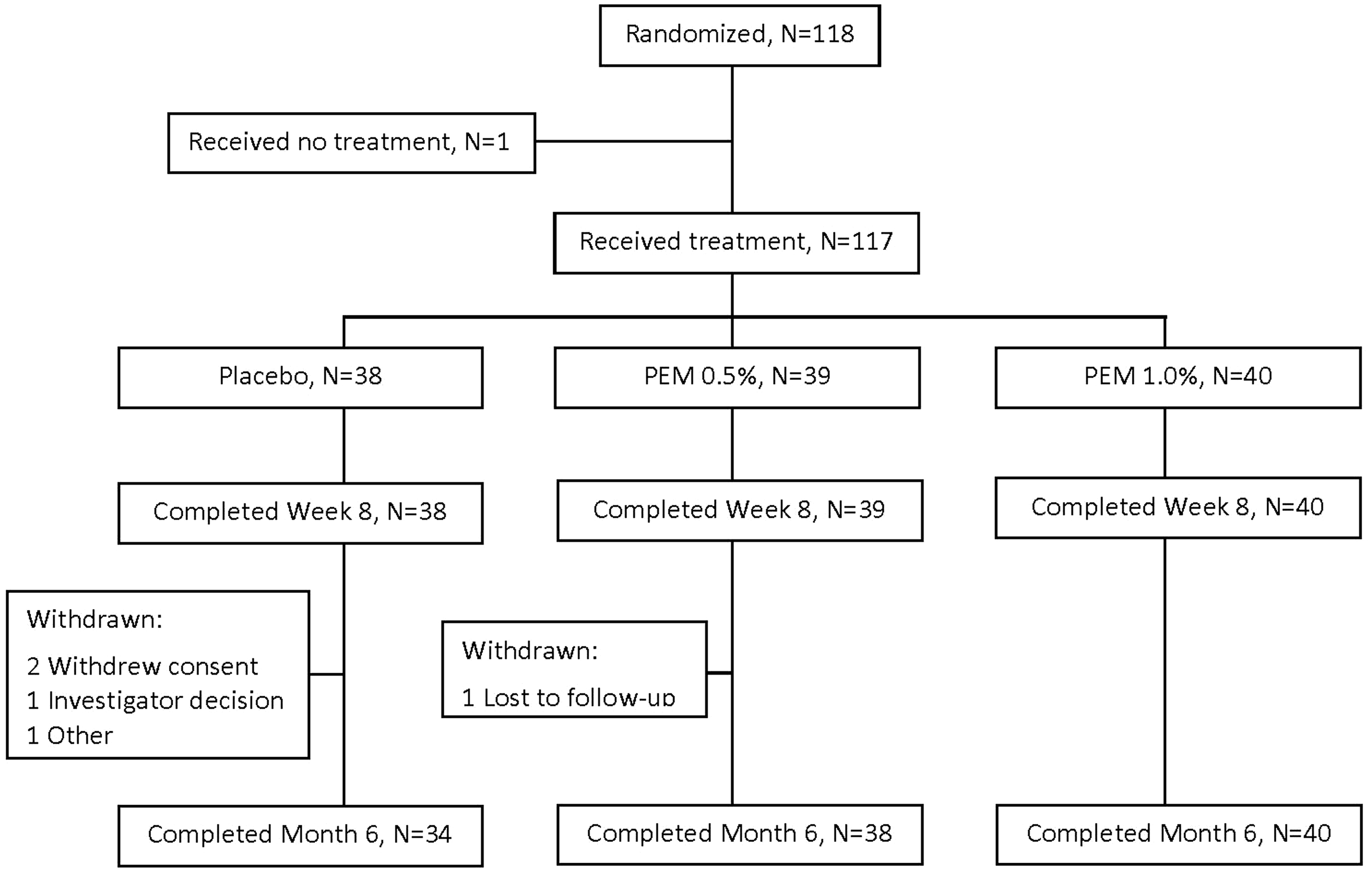
Efficacy
Appearance assessments
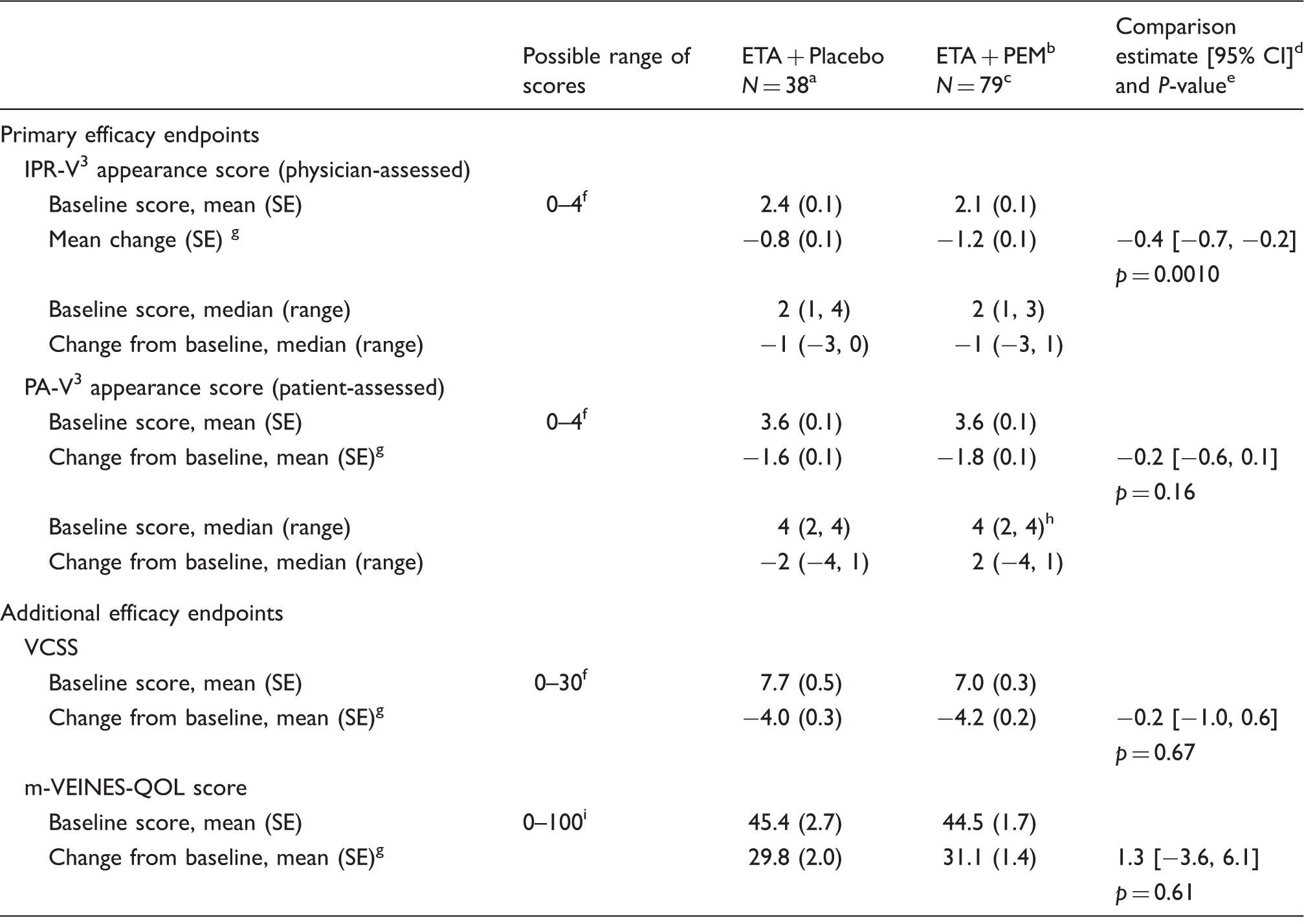
The mean decrease (improvement) from Baseline was greater at Week 8 for pooled PEM than for placebo for both IPR-V3 (−1.2 vs. −0.8 points, p = 0.001) and PA-V3 (−1.8 vs. −1.6 points, p = 0.16), although only IPR-V3 change score reached statistical significance (Table 3). The comparison of the individual dose concentrations of PEM (0.5%, 1.0%) with placebo showed a similar pattern for both IPR-V3 and PA-V3 scores. Figure 2 shows a patient before and after treatment with ETA + PEM 1%.
Photographs of a study patient who received ETA and PEM 1%. The patient was a 36-year-old white female with BMI 30.1 kg/m2. Efficacy endpoints at Week 8. CI: confidence interval; SE: standard error; ETA: endovenous thermal ablation. n = 37 for VCSS. Pooled PEM groups (0.5% + 1.0% concentrations). n = 77 for m-VEINES-QOL scores. 95% confidence interval for the comparison of ETA + PEM vs. ETA + placebo based on adjusted means, unadjusted for multiple comparisons. p-value for comparison is 2-sided significance level for paired comparisons. Lower score indicates better status on IPR-V3, PA-V3, and VCSS instruments. Adjusted mean change from baseline at Week 8: least square means from analysis of covariance (ANCOVA) model with treatment group and site as class variables and the corresponding baseline score from the questionnaire as a continuous covariate. n = 77 patients with both a baseline value and a value at the corresponding visit. Higher scores indicate better status on m-VEINES-QOL instrument.
A significantly higher proportion of patients achieved clinically meaningful change with (pooled) PEM than with placebo for both IPR-V3 (Week 8: 83.5% vs. 57.9%, p = 0.004; Month 6: 70.9% vs. 42.1%, p = 0.001) and PA-V3 (Week 8: 72.2% vs. 55.3%, p = 0.06; Month 6: 67% vs. 50%, p = 0.034) (Figure 3).
Percentage of patients with clinically meaningful change in appearance as assessed by clinicians (IPR-V3 score) and patients (PA-V3 score) after treatment with endovenous thermal ablation and either placebo or PEM (pooled 0.5% and 1.0%).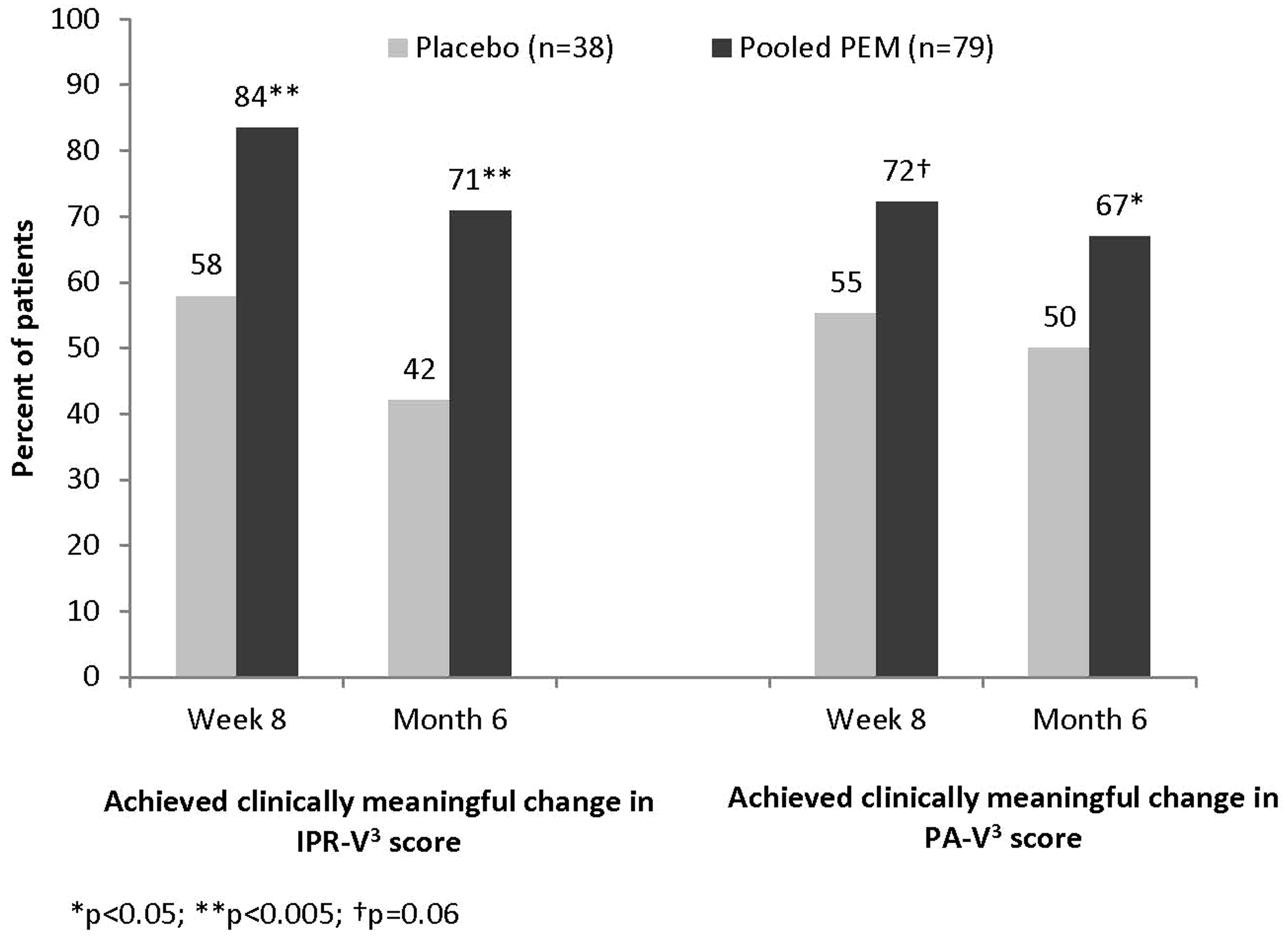
Other efficacy endpoints
Change scores for VCSS and m-VEINES-QOL at Week 8 were slightly better for PEM recipients than for placebo recipients, although none of the between-group differences were statistically significant (Table 3). Results were similar for between-group differences at Month 6.
PEM significantly reduced the proportion of patients who received additional treatment for residual varicosities between Week 8 and Month 6 (13.9% PEM recipients vs. 23.7% placebo, p = 0.037) (Figure 4(a)). The most common additional treatment was liquid (n = 5) or foam (n = 14) sclerotherapy (this sclerotherapy was not PEM, as treatment with PEM was not allowed after the initial treatment by protocol), with 18.4%, 12.8%, and 12.5% of patients receiving it in the placebo, PEM 0.5%, and PEM 1.0% groups, respectively.
(a) Percentage of patients who did not require additional treatment between Week 8 and Month 6 and (b) Percentage of patients for whom endovenous thermal ablation (ETA) eliminated saphenofemoral junction reflux (SFJ).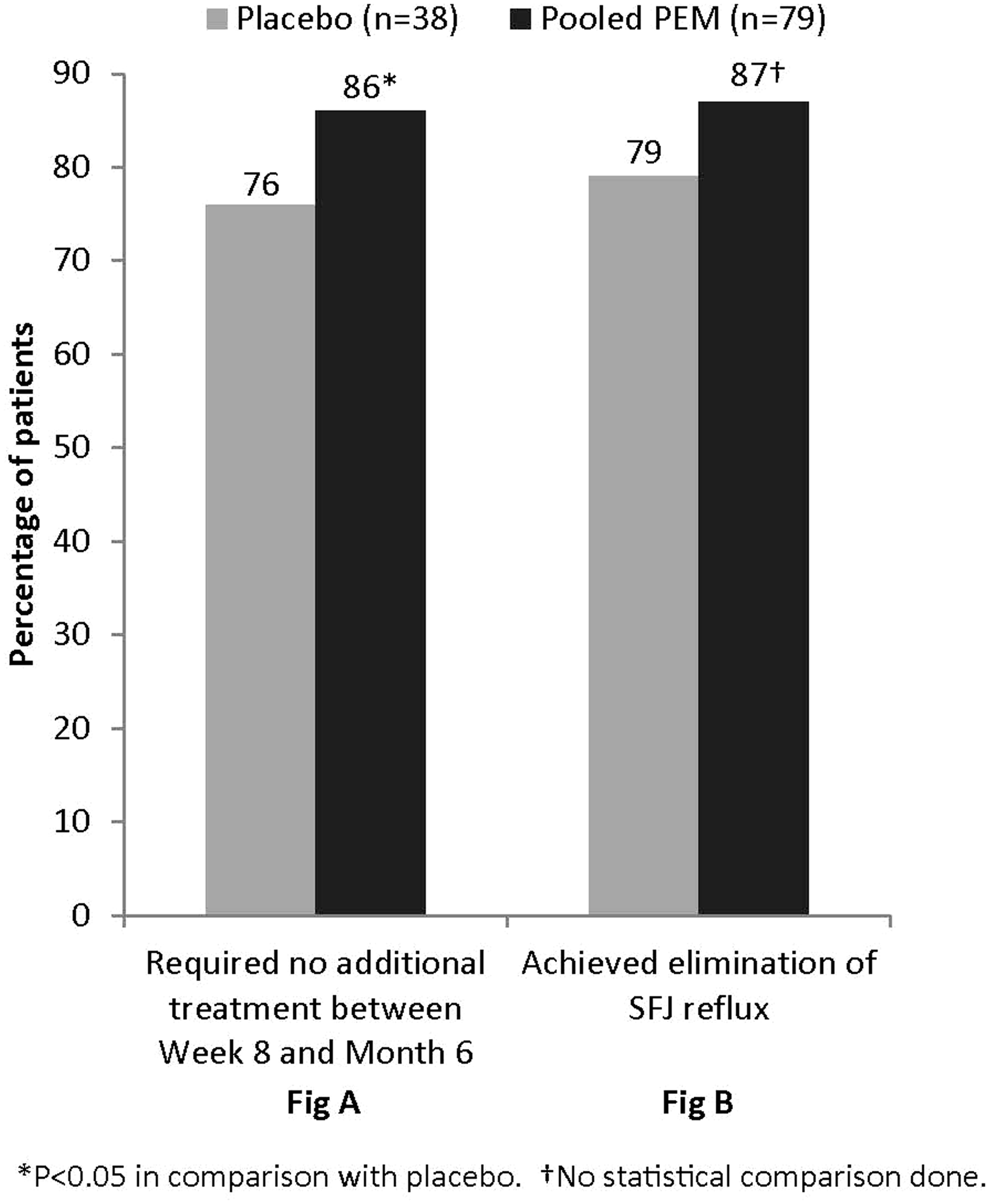
Elimination of reflux through the SFJ was achieved in 30/38 (78.9%) ETA + placebo recipients compared with 69/79 (87.3%) ETA + PEM recipients (Figure 4(b)). The subset of patients with incompetent distal GSVs at baseline comprised 19 (pooled) PEM recipients and 1 placebo recipient. In this subset, physiological response to treatment was achieved in 16/19 (84.2%) of PEM recipients and 0/1 placebo recipient. No statistical comparisons were conducted due to the small numbers of patients.
Safety
Adverse events with incidence ≥3% in either PEM group through Week 8.
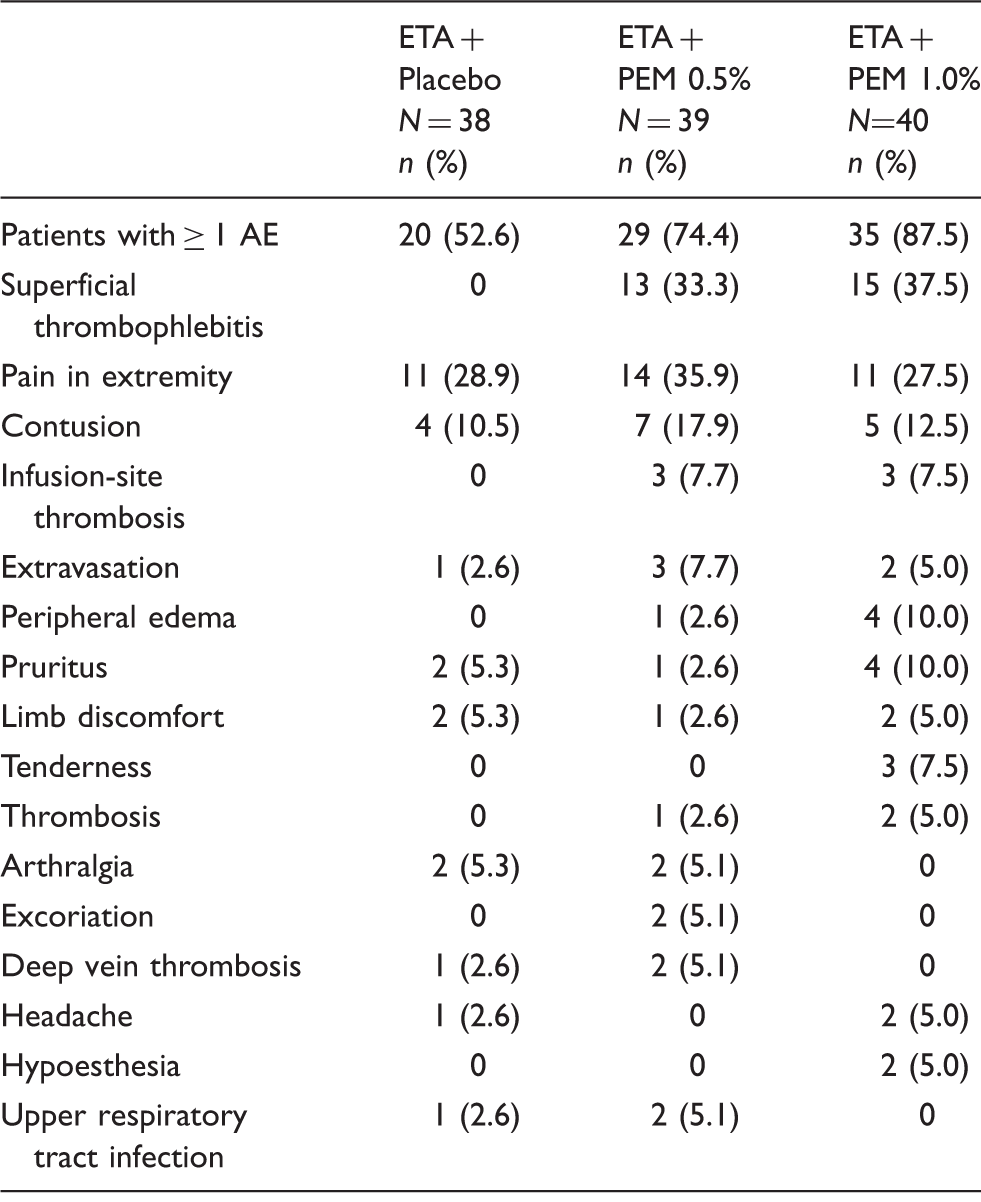
AE: Adverse event; PEM: polidocanol endovenous microfoam.
Discussion
To assess the benefit of using PEM to treat tortuous superficial varicose veins and other GSV segments not treated by ETA, PEM (or placebo) was administered immediately following ETA in the same treatment session. ETA effectively ablates trunk veins and reduces most symptoms of elevated hydrostatic venous pressure. Consequently, the primary study endpoint was change in varicose vein appearance as assessed by experts (IPR-V3 score) and patients (PA-V3 score) at Week 8. To our knowledge, no previous controlled trial has assessed the effect of combination therapy on varicose vein appearance.
At baseline, patients rated appearance as more noticeable than did the experts, which highlights the concept that physicians and patients use assessment tools in different ways. The more objective expert evaluation is based on a broader understanding of disease severity, and the experts used the scale as a continuous variable. The clinician assessment of appearance significantly favored the addition of PEM to ETA (p = 0.001), and the patient assessment showed a similar trend. By Month 6, the percentage of patients who achieved a clinically meaningful benefit in appearance, assessed by both clinicians and patients, was significantly higher with the addition of PEM (p < 0.05). Significantly fewer PEM recipients required additional treatment for varices between Week 8 and Month 6 (14% PEM vs. 24% placebo, p < 0.05), therefore, some patients clearly benefit from treatment with ETA and PEM in the same session.
Treatment of the proximal GSV by ETA alone was expected to alleviate most of the symptoms of GSV incompetence. Consistent with this, VCSS and m-VEINES-QOL scores showed numerically greater (although not statistically significant) improvements with ETA + PEM compared with ETA + placebo. ETA alone for the proximal GSV does not address the often multiple sources of clinical reflux. As concomitant treatment, PEM was used effectively in the distal GSV, accessory saphenous veins, and tributary varices.
Most publications report GSV closure rates, these being 90–95%. 26 In this study, interestingly, at Week 8, ETA therapy alone eliminated SFJ reflux in only 79.9% of ETA + placebo recipients compared with 87.3% of ETA + PEM recipients.
King et al. 6 reported that concomitant treatment with laser and foam therapy was highly efficacious in the treatment of reflux of the GSV and small saphenous veins and their tributaries, and that patients had significantly improved quality of life. Theivacumar et al. 27 compared three therapies in patients with GSV incompetence that extended below the knee: laser above the knee only (group A), laser both above and below the knee (group B), and laser above the knee combined with foam sclerotherapy below the knee (group C). They concluded that extending laser ablation below the knee and the addition of foam sclerotherapy improved symptom resolution.
Combination treatment with ETA and PEM was generally well tolerated. The AEs observed were those typical of the treatments administered. During detailed ultrasound safety surveillance, three patients had isolated gastrocnemius vein thrombosis detected and three patients had DVT detected. The DVTs occurred in two patients in the PEM group and in one in the placebo group; these thrombi resolved or stabilized within 13–50 days.
Conclusions
The addition of PEM to ETA significantly improved physician-assessed appearance scores and reduced the proportion of patients who had residual SFJ reflux and the proportion who received additional treatment. Additionally, there was a consistent trend throughout the other study endpoints that suggested improved efficacy with the addition of PEM to ETA therapy compared with placebo and ETA.
Footnotes
Acknowledgements
The authors acknowledge David Wright, MB, FRCS, for his participation in the design and execution of the Varithena clinical program; June Manns and Ellen Evans for the scientific and operational management of the study; John Ilgenfritz (United BioSource Corporation, Blue Bell, PA) and Claire Daugherty for statistical support; Tuli Ahmed (JetStream Clinical, LLC) for medical writing assistance (funded by Biocompatibles, Inc., a BTG International group company); and Naissan Wesley, MD and Derek H. Jones, MD (both of Skin Care and Laser Physicians of Beverly Hills) and Glenn Jacobowitz, MD (New York University School of Medicine) for independent photography review of standardized digital photography. DW, JM, EE, and CD are current or former employees or consultants of BTG International group companies.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MV and AG were investigators and their sites received funding from the sponsor for their participation in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was sponsored by Provensis Ltd (a BTG International group company). Varithena is manufactured by BTG Biocompatibles Ltd on behalf of Provensis Ltd.