
Abstract
Objective
Awake Extracorporeal Life Support (aECLS) with active mobilization has gained consensus over time, also within the pediatric community. This individual patient data (IPD) meta-analysis summarizes available evidence on pediatric aECLS, its feasibility, and safety regarding sedation weaning, extubation, and physiotherapy.
Methods
PubMed/Medline and Cochrane Database were screened until February 2022. Articles reporting on children (≤18 years) undergoing aECLS were selected. IPD were requested, pooled in a single database, and analyzed using descriptive statistics. Primary outcome was survival to hospital discharge. Secondary outcomes included extubation during ECLS, physiotherapy performed, tracheostomy, and complications.
Results
Nineteen articles and 65 patients (males:n = 30/59,50.8%) were included. Age ranged from 2 days to 17 years. ECLS configurations included veno-venous (n = 42/65, 64.6%), veno-arterial (n = 18/65, 27.7%) and other ECLS settings (n = 5/65, 7.7%). Exclusive neck cannulation was performed in 51/65 (78.5%) patients. Extubation or tracheostomy during ECLS was reported in 66.2% (n = 43/65) and 27.7% (n = 18/65) of patients, respectively. Physiotherapy was reported as unspecified physical activity (n = 34/63, 54%), mobilization in bed (n = 15/63, 23.8%), ambulation (n = 14/63, 22.2%). Complications were reported in 60.3% (n = 35/58) of patients, including hemorrhagic (36.2%), mechanical (17.2%), or pulmonary (17.2%) issues, and need for reintubation (15.5%). Survival at discharge was 81.5% (n = 53/65).
Conclusion
Awake ECLS strategy with active physiotherapy can be applied in children from neonatal age. Ambulation is also possible in selected cases. Complications related to such management were limited. Further studies on aECLS are needed to evaluate safety and efficacy of early physiotherapy and define patient selection.
Keywords
Introduction
Extracorporeal life support (ECLS) has been increasingly applied as a safe, effective, and feasible method for patients toward recovery, transplant, or other permanent mechanical circulatory support devices.1,2 The ever-present scarcity of healthcare resources and the necessity to provide cost-effective care have challenged this concept. However, despite the initial skepticism and poor outcomes in terms of mortality and morbidity, advanced technologies, human dedication, and experience allowed for ECLS to grow more decisive in survival, 3 reduce comorbidities, 4 and enable early rehabilitation. 5
The human factor is, however, the latest challenge in the ECLS research field. Evidence on the importance of awake patients’ contribution to the ECLS recovery process is lacking, potentially due to many centers’ resistance to adopting a more innovative strategy where patients are active in the treatment. The invasiveness of the device and the possible issues related to its practice are the most common barriers to this approach, which leads to a more conservative practice with patients bed-bound and sedated.
6
Contrarily, the patient becomes the central focus of what is called “awake ECLS” (aECLS): a technique based on the concept that allowing active patient participation will favor a rapid recovery, less chronic comorbidities, reduced psychological as well as psychiatric complications, and improved survival.7,8 The aECLS approach aims to reduce invasive mechanical respiratory support with the help of lower analgesia and sedation doses, allowing early rehabilitation,
9
normalized oral intake,
10
and regained consciousness for reduced anxiety and collaborative engagement in daily tasks and decisions (when age-appropriate)
11
(Figure 1). Early mobilization and extubation during ECLS support have been described mainly in adult patients but have been advocated and performed in a few pediatric series. Indeed, comprehensive data about this strategy in children is missing. Conservative versus awake ECLS strategy.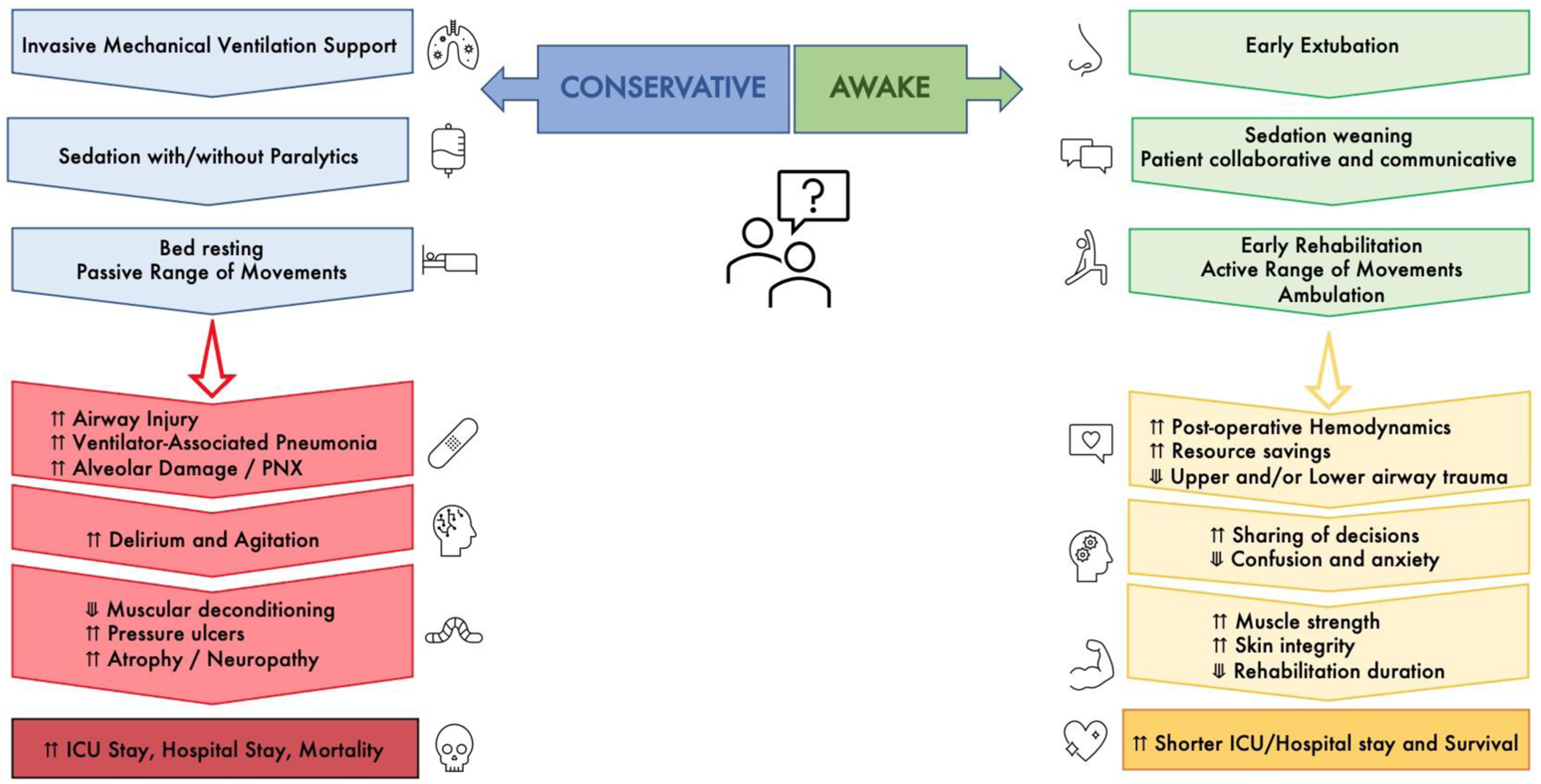
This individual patient data (IPD) meta-analysis summarizes available evidence on pediatric aECLS, its feasibility, and safety correlated to analgesia, sedation and respiratory support weaning, and physiotherapy.
Material and methods
Data sources and search strategies
The protocol for the meta-analysis was completed according to PRISMA guidelines and registered with PROSPERO (Registration No. CRD42021245883) before the start of the literature screening. PubMed/Medline and Cochrane Database of Systematic Reviews were screened from inception to February 2022. Further details of the search strategy are provided in Supplemental Materials. Initial search results were merged and imported into EndNote® 20 (Clarivate Analytics, Philadelphia, PA, USA). After removing duplicates, two independent reviewers (M.C. and G.C.) assessed the remaining titles and abstracts for inclusion using a free, open-source citation screening program. 12 Two authors (M.C. and G.C.) retrieved and independently assessed full texts of relevant articles. Disagreements over articles’ appropriateness for inclusion were resolved by consensus. Reference lists of assessed full texts were screened for further suitable studies. 13
Population, intervention, and outcome
We included randomized clinical trials, cohort studies, case reports, and case series reporting single patient data. Single patient data were requested if not already available. Conference abstracts, books, articles not written in English, reviews, and animal studies were excluded. The population of interest included hospitalized pediatric patients (age ≤18 years old) supported with ECLS and undergoing an aECLS strategy, including weaned analgesia and sedation, reduced invasive mechanical ventilation to extubation, and active physiotherapy up to ambulation. The exclusion criteria were identified as adults (>18 years old) and patients supported with durable ventricular assist devices. Studies presenting only interventions referred to as “early passive Range of Movement (RoM) rehabilitation” or focused on chest physiotherapy without proven aECLS strategy were excluded. The primary outcome measure was survival at discharge. Secondary outcome measures included feasibility outcomes (active physiotherapy executed, extubation achieved, tracheostomy performed), safety outcomes (adverse events while supported on aECLS: cannula dislodgement, bleeding, hemodynamic instability, respiratory deterioration requiring reintubation, circuit malfunction, delirium, local trauma, neurological sequelae), ECLS cannulation strategies, intensive care unit (ICU) length of stay (LoS), and hospital LoS. Definitions from the Extracorporeal Life Support Organization (ELSO) Registry were used to characterize ECLS-related complications. 14
Data extraction and risk-of-bias assessment
Using a standardized electronic report form, data were extracted into a dedicated database by the primary reviewer (M.C.) and checked for accuracy by a second reviewer (G.C.). Extracted variables are detailed in Supplemental Materials. Two reviewers (M.C. and G.C.) independently assessed risk-of-bias in individual studies; consensus resolved disagreements. Case reports were assessed by applying the JBI Critical Appraisal Tool 15 to evaluate the methodological quality of case reports and case series.
Data synthesis
Data were summarized using descriptive statistics (median, [inter-quartile range, (IQR)] or frequency [n, %]) as appropriate. Complication rates are expressed in terms of affected patients, not single episodes. Subgroup analyses were performed by age groups defined as neonates (0–28 days), infants (1-12 months), toddlers (1–4 years), children (5-10 years), adolescents (11-18 years), and ECLS support type (veno-venous vs veno-arterial ECLS). The Kolmogorov–Smirnov test assessed all continuous variables for normal distribution. Non-normally distributed variables were analyzed with the Wilcoxon-Mann-Whitney or Kruskal-Wallis test. Categorical variables were compared using Chi-square. Fisher’s exact test with a statistical significance level of 5% was applied if at least one of the expected counts was <5. Missing values were not imputed. A p-value ≤0.05 was considered statistically significant. All analyses were performed using SPSS version 26 (SPSS Inc., Chicago, IL, USA), and graphs were plotted with Prism 6 (GraphPad, San Diego, CA, USA) or InDesign CS4 (Adobe, San José, CA, USA).
Results
Literature search
A total of 1265 abstracts were identified through a literature search, and 19 articles reporting on 65 patients were selected for inclusion (Figure 2 and Supplemental Table 1). From the reference list analysis, no additional publications were found. The earliest article was published in 2011, followed by a growth in the trend of publications and a decrease after the beginning of the COVID-19 pandemic (Supplemental Figure 1). It included patients who received aECLS between 1996 and 2020. Data completeness is reported in Supplemental Table 2. Flowchart.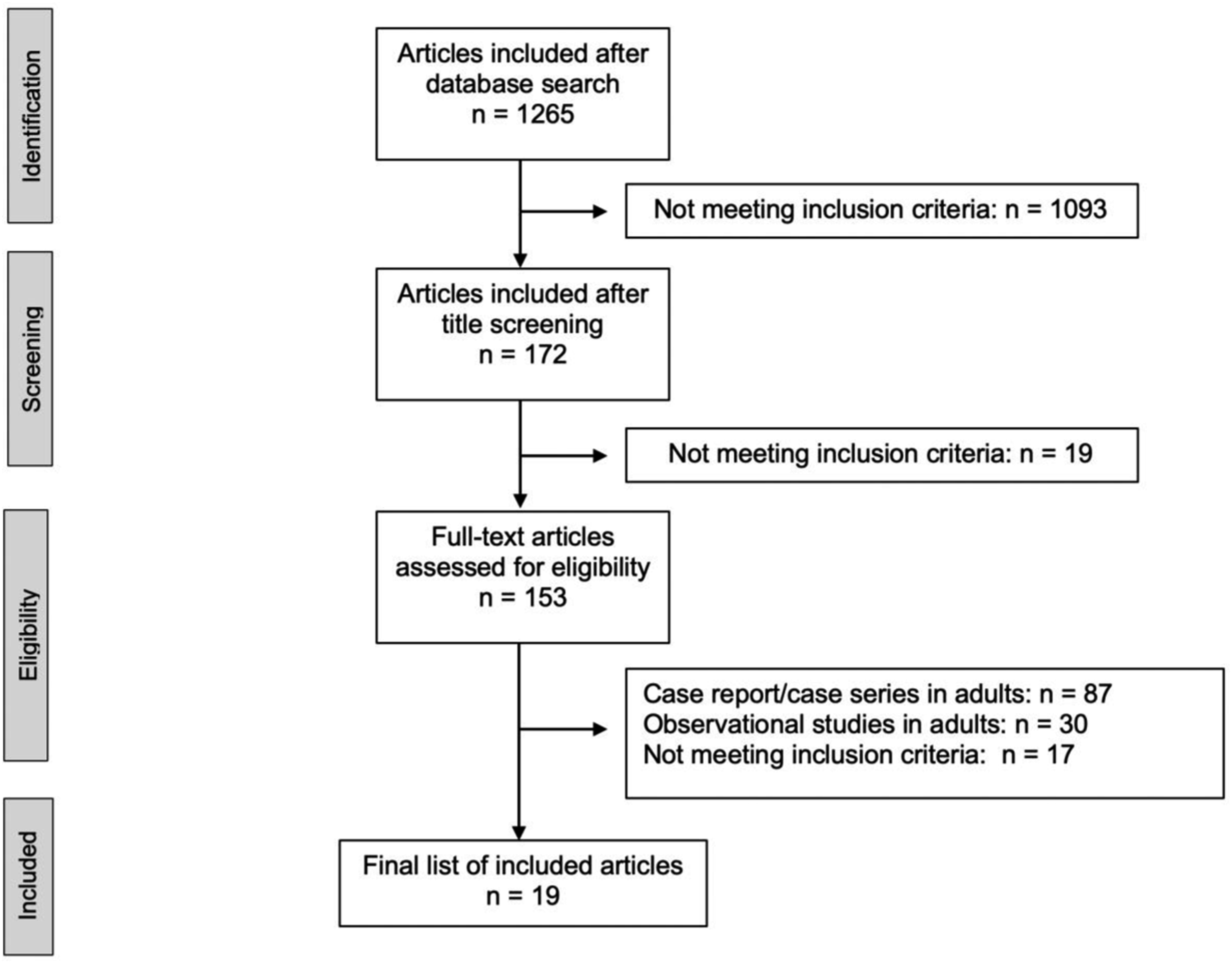
Patient characteristics and ECLS indications
ECLS practice and configurations are represented in appropriate age subcategories.
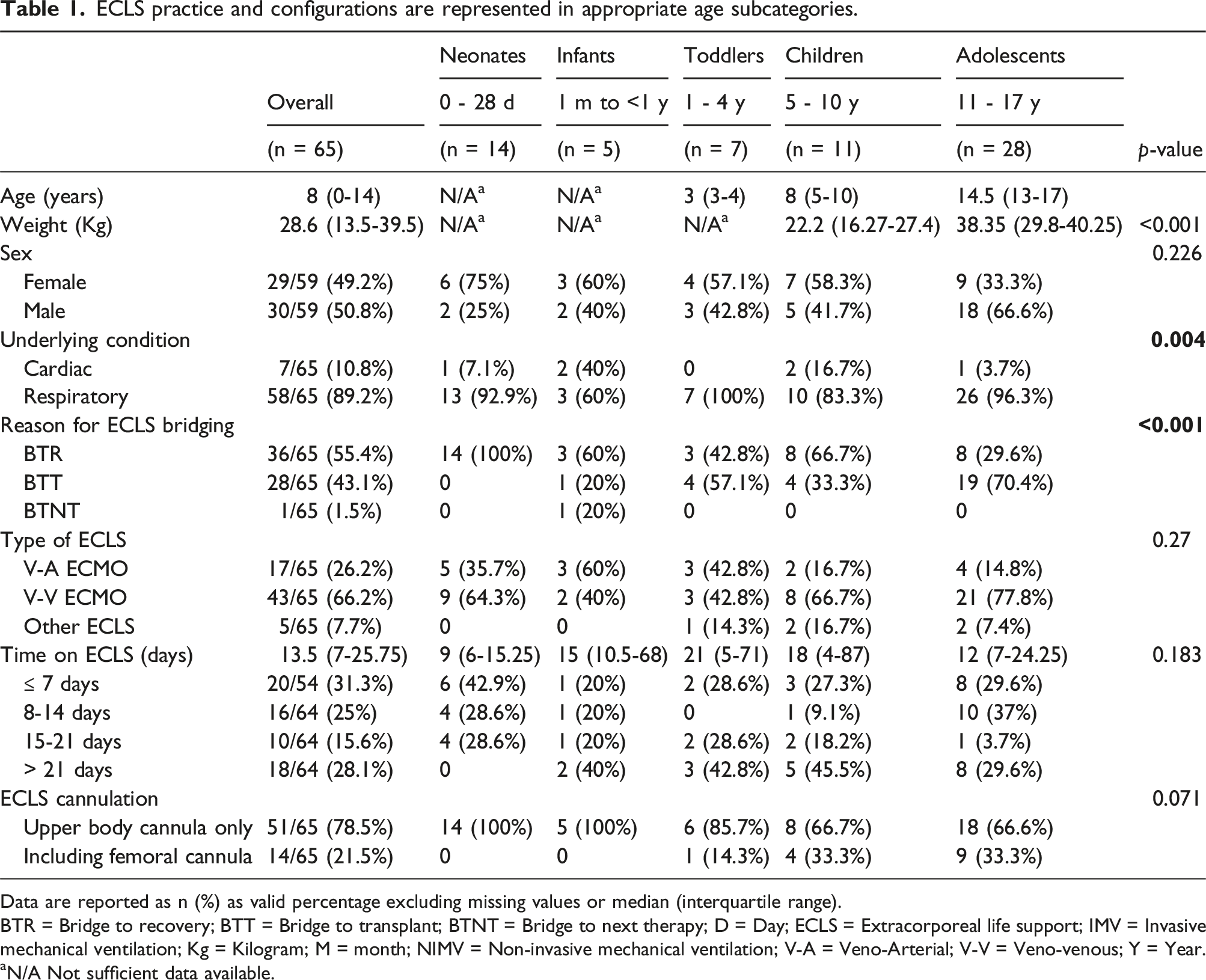
Data are reported as n (%) as valid percentage excluding missing values or median (interquartile range).
BTR = Bridge to recovery; BTT = Bridge to transplant; BTNT = Bridge to next therapy; D = Day; ECLS = Extracorporeal life support; IMV = Invasive mechanical ventilation; Kg = Kilogram; M = month; NIMV = Non-invasive mechanical ventilation; V-A = Veno-Arterial; V-V = Veno-venous; Y = Year.
aN/A Not sufficient data available.
This collection of case reports represented the wide variety of clinical indications for ECLS support in the pediatric population: 10.8% (n = 7/65) cardiac, such as cardiogenic shock 16 and more general chronic heart failure4,6,21,24; 89.2% (58/65) respiratory, such as refractory respiratory failure in previously healthy children6,17–20,25–28,31 and rescue therapy bridging to airway surgery 22 including unique clinical diagnoses for children with cystic fibrosis20,21,27,28 and congenital diaphragmatic hernia.6,19
Extracorporeal life support details
Veno-venous (V-V) ECLS accounted for 64.6% (n = 42/65) of cases, veno-arterial (V-A) for 27.7% (n = 18/65), and other ECLS types for 7.7% (n = 5/65). Most patients (n = 51/65, 78.5%) underwent upper body cannulation (V-V: n = 33/51, 64.7%; V-A: n = 16/51, 31.4%), but a femoral cannula was present in 21.5% (n = 14/65) of patients (Table 1, Supplemental Table 3). ECLS duration was reported in most studies (n = 64/65, 98.4%), showing median values of 13.5 days (IQR 7-25.75). Twenty-eight patients (n = 28/64, 43.8%) remained on ECLS for over 14 days (Table 1).
Awake ECLS and respiratory support
All patients in this review were considered “awake” as they included at least one of the inclusion criteria related to their conscious state, respiratory support, or physiotherapy activity.
Respiratory practice during ECLS is represented in appropriate age subcategories.
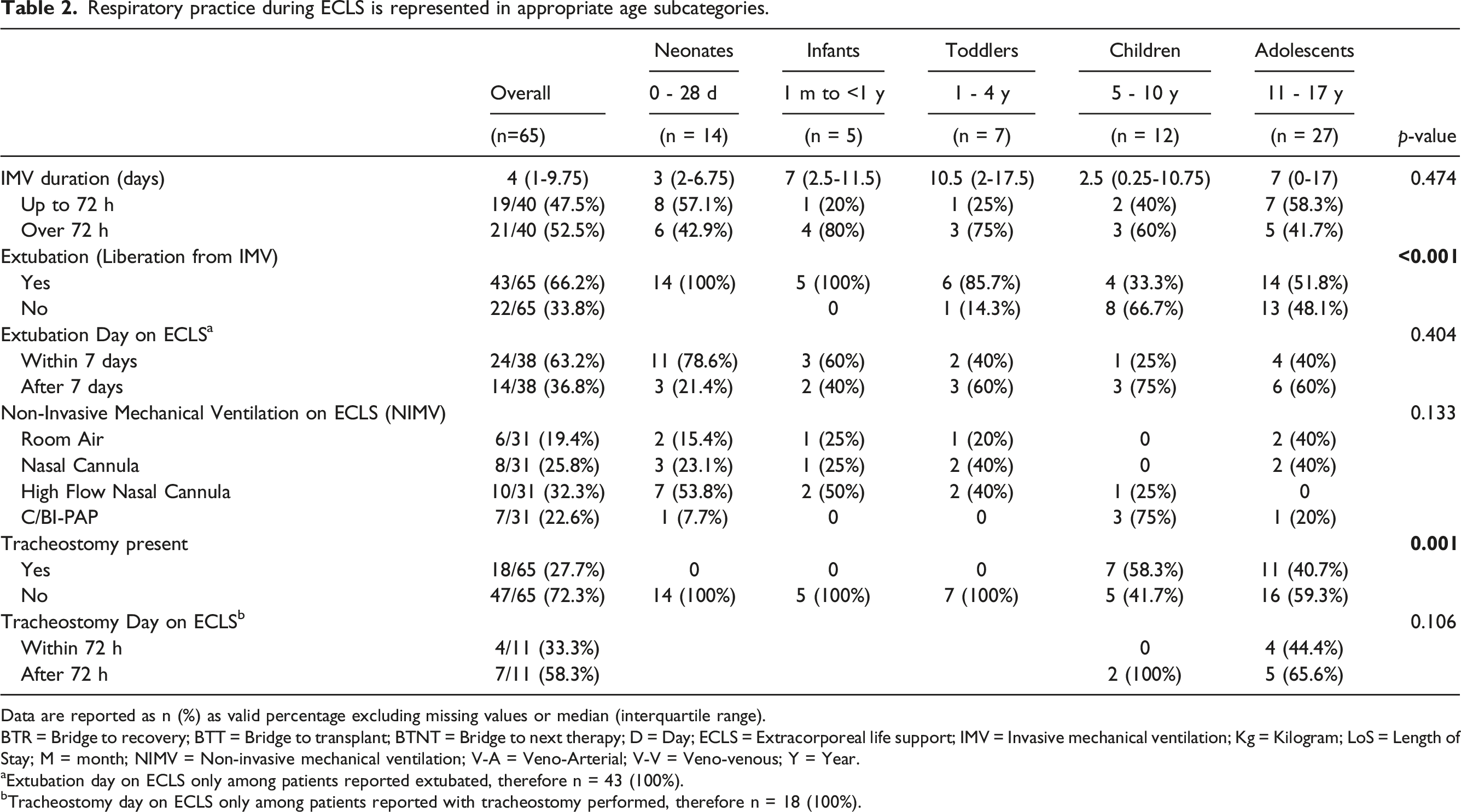
Data are reported as n (%) as valid percentage excluding missing values or median (interquartile range).
BTR = Bridge to recovery; BTT = Bridge to transplant; BTNT = Bridge to next therapy; D = Day; ECLS = Extracorporeal life support; IMV = Invasive mechanical ventilation; Kg = Kilogram; LoS = Length of Stay; M = month; NIMV = Non-invasive mechanical ventilation; V-A = Veno-Arterial; V-V = Veno-venous; Y = Year.
aExtubation day on ECLS only among patients reported extubated, therefore n = 43 (100%).
bTracheostomy day on ECLS only among patients reported with tracheostomy performed, therefore n = 18 (100%).
Non-invasive mechanical support (NIMV) was reported in 31 cases (n = 31/43, 72%), and self-ventilation in room air was reported in 16% (n = 5/31) of patients. Tracheostomy was present in 27.7% (n = 18/65) of cases (V-V ECLS: n = 17/42, 40.5%, p = .011; V-A ECLS: n = 1/18, 5.5%, p = .014, Supplemental Table 5). Only two patients received tracheostomy within the first 24 h of support.29,30 When comparing the presence versus absence of tracheostomy (Supplemental Table 6), both populations showed a higher incidence of underlying respiratory conditions, BTT, ECLS duration longer than 21 days, with a configuration including V-V and upper cannula, and incidence of hemorrhagic complications. Patients with tracheostomy had higher ambulation success (n = 7/17,41.2% and n = 6/21,28.6%) and longer ICU LoS (n = 6/10,60% and n = 12/14,85.7%), while patients without showed a higher incidence of mechanical (n = 5/21,23.8% vs none) and cardiovascular (n = 4/21,19% vs none) complications, and a more achieved extubation rate (n = 18/21,85.7%).
Elements showing statistical significance with whether liberation from IMV was performed before or after 7 days from ECLS cannulation (Table 2, Supplemental Table 4, Supplemental Table 5) were the following: underlying conditions (p = .01), ECLS duration (p = .003), NIMV mode (p = .046), survival at discharge (p = .012) and absence of complications (p = .007).
Physiotherapy
Physiotherapy practice during ECLS is represented in appropriate age subcategories.
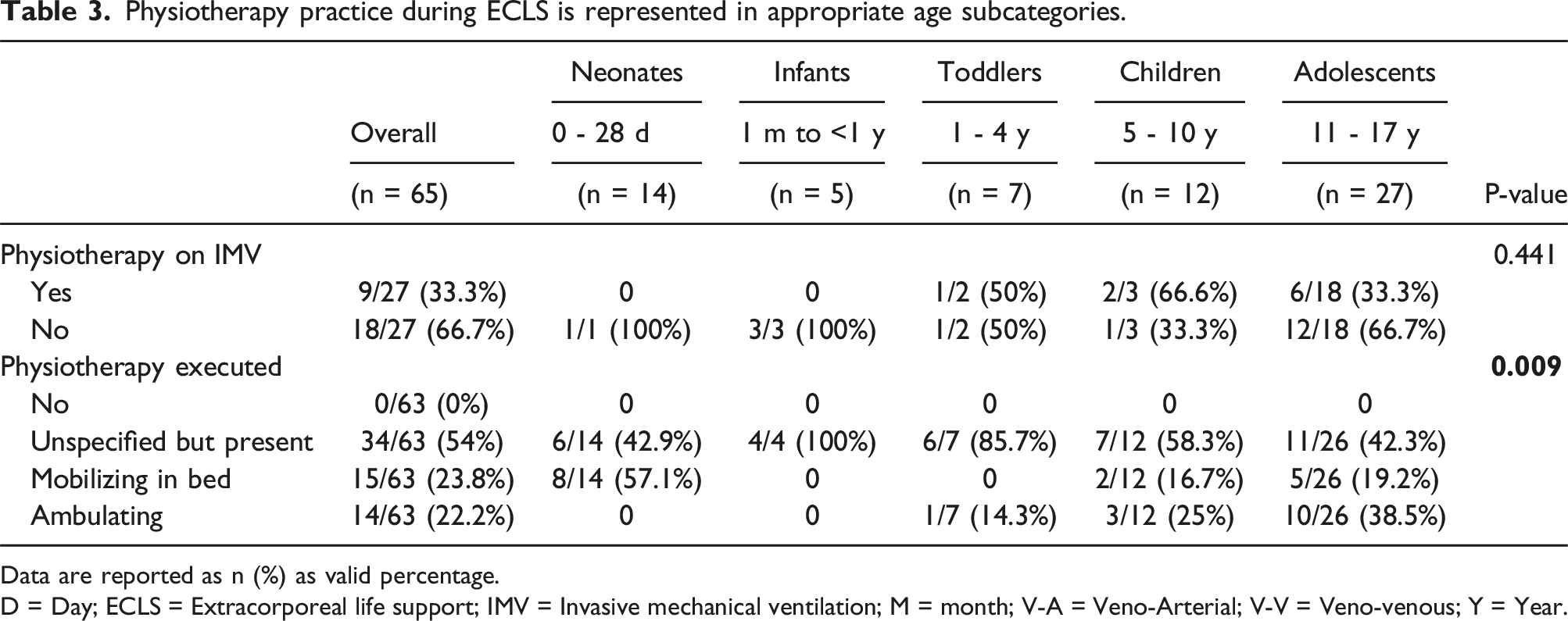
Data are reported as n (%) as valid percentage.
D = Day; ECLS = Extracorporeal life support; IMV = Invasive mechanical ventilation; M = month; V-A = Veno-Arterial; V-V = Veno-venous; Y = Year.
Overall, 33.3% (n = 9/27) of patients on IMV performed physiotherapy, in which two-thirds were supported on V-V ECLS and nearly half of the cohort successfully ambulated (n = 4/9, 44.5%).29,31 Levels of physiotherapy differed between age groups (p = .009) (Table 3, Supplemental Figure 2). Ambulation differed based on ECLS indication (p = .002), extubation (p = .005), tracheostomy (p = .028), hospital stay (p = .003) and survival at discharge (p = .04).
Complications during ECLS
Outcomes during ECLS are represented in appropriate age subcategories.
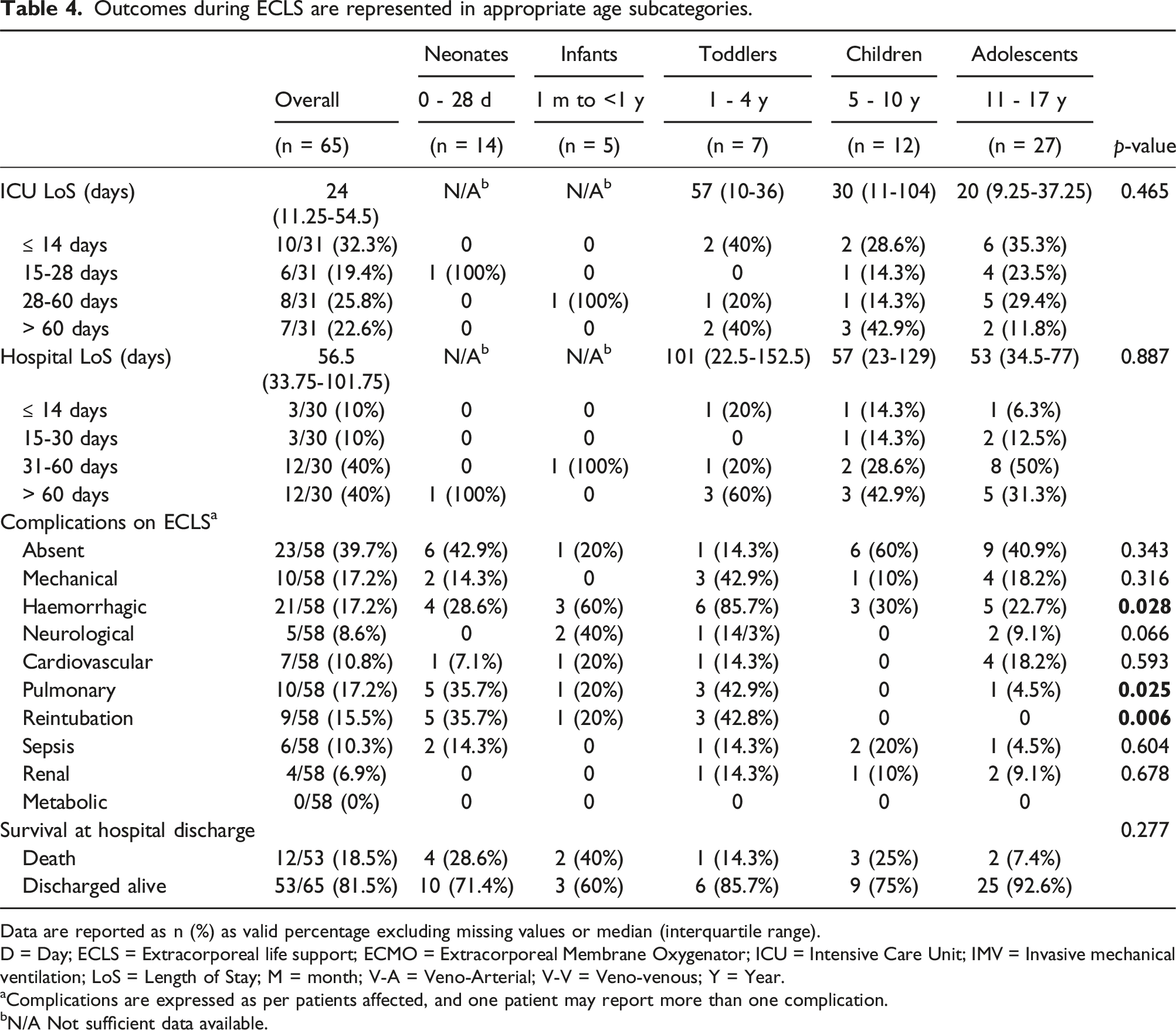
Data are reported as n (%) as valid percentage excluding missing values or median (interquartile range).
D = Day; ECLS = Extracorporeal life support; ECMO = Extracorporeal Membrane Oxygenator; ICU = Intensive Care Unit; IMV = Invasive mechanical ventilation; LoS = Length of Stay; M = month; V-A = Veno-Arterial; V-V = Veno-venous; Y = Year.
aComplications are expressed as per patients affected, and one patient may report more than one complication.
bN/A Not sufficient data available.
Survival, intensive care unit, and hospital stay
ICU duration was reported in 47.7% (n = 31/65) of patients, with a median value of 24 days (11.25-54.5), while hospital stay was reported for 46.2% (n = 30/65) of patients, median of 56.5 days (33.75-101.75) (Table 4). Overall survival at discharge was 81.5% (n = 53/65), with 22.2% (n = 4/18) reported in V-A and 83.3% (n = 35/42) in V-V ECLS. All ambulatory patients survived.
Discussion
This review illustrates the aECLS strategy as safe and feasible in all pediatric age subgroups. In fact, despite the complications reported in 39.7% of the population examined (n = 23/58), none were significant concern causes supporting the safety aspect investigated. The study has three main findings for the achievement of this approach. First, the analgesia and sedation weaning enabled a more conscious state, reducing delirium/withdrawal syndrome, facilitating communication, and the ability to follow active instructions. Second, the invasive ventilation support via endotracheal airway was decreased to either self-ventilation with or without NIMV or to more long-term invasive support via tracheotomy. Third, early physiotherapy was implemented at any stage of the ECLS run according to the conscious state and patient’s tolerance, with age-appropriate interventions and irrespective of any existent respiratory support type.
Conscious state
The achievement of children on ECLS to be cognitively present in the daily routine was consistent with the improved analgesia and sedation weaning practice.4,6,20,28,31 Benefits ranged from reduced withdrawal, 16 reduced IMV duration,3,4,6,20,28,31 improved communication for further cooperation and emotional support with the healthcare team and family,4,6,16,27,28 and bedside school lessons attendance. 16 A crucial benefit for children was improved nutritional intake, leading to better weight preservation and energy to participate in rehabilitation, an improved outlook, and reduced anxiety.4,17,19,27,32 The latter was carefully considered by Schwartz et al. 20 for selected populations, such as previously healthy children with acute lung injury experiencing a stressful state due to air hunger after sedation weaning, resulting in a successful awake state. Costa et al. 19 highlighted their success in initiating a neonatal enteral and oral feeding trial. Due to their limited adipose and lean tissue reserves, inadequate nutritional intake was advised against with a focus on preventing infection, multi-organ failure, hospital duration, and mortality.17,33,34
Only two studies reported using evaluation tools to monitor their tolerance to pain and/or agitation to create a safe environment and practice for children to be consciously awake while supported on ECLS6,16,17; however, without further details on medication parameters or titration, score targets, duration, treatments implemented. Turner et al. 25 and Zebuhr et al. 17 mentioned only their intervention on sedation, such as minimization or interruption, with no further details except the patient tolerance observation through nonverbal clues, vital signs, and ECMO flow by the latter.
Respiratory practice and outcomes
Liberation from mechanical ventilation was feasible for most of the included patients. Anton-Martin et al. 6 supported the practice of extubation if ECLS alone had met the metabolic demand, and the consequent advantages were faster resolution of pulmonary inflammation and the opportunity to prevent physical deconditioning. The practice was encouraged due to the undesirable necessity of sedation to maintain the tolerance of the endotracheal tube acting as an irritant, 6 possibly responsible for airway trauma, especially in cases of bridging to airway surgery.22,35,36 If extubation was not possible, tracheostomy and aggressive IMV weaning were arranged. 31 In the social context, opposition to extubation from family members did not arise. 6
Despite the current limitations and lack of consensus on general tracheostomy practice, timing and complications, 37 and more pediatric-related issues such as the need for an open procedure in the operating room, granulation, and tracheal stenosis,20,30 advantages were listed in some of the articles analyzed. Improvements observed included sedation and analgesia weaning, the possibility of intermittent ventilation implementation, reduced hospital length of stay and morbidity compared to patients on IMV, rehabilitation access due to improved airway stability and communication, facilitated enteral nutrition, and enhanced care delivery during the pre-transplant waiting period.17,18,20,25,30 Schwartz et al. 20 Described tracheostomy performed at bed space in children as feasible, supporting the challenge of known risks with the advantages of reduced morbidity during transfer, reduced cost, and the safety of having the same team to look after the patient.
Rationales supporting physiotherapy during ECLS
Several studies report that active mobilization programs during ECLS for any clinical indications resulted in safe and feasible outcomes4,17,20,24,27,28 and decreased post-ECLS physical rehabilitation needs and deconditioning,16,31 positively impacting critical illness neuropathy and myopathy. Indeed, an ambulatory ECLS status is likely to improve severe acute illness, length of stay, IMV duration, and survival.4,23 To address the uncertainty regarding ambulatory ECLS in children not previously healthy, Turner et al. 25 described a higher tolerance for dyspnea in chronically ill children under those circumstances.
While most patients in this study participated in physiotherapy, minimal details were provided regarding completed exercises or therapy input specifics. Shkurka et al. 43 suggest that the whole spectrum of exercises and activities should be considered for pediatric ECLS patients, including developmental positioning, resistance exercises, bed bikes, seating, and mobility. Several authors have described out-of-bed cuddles as suitable for neonatal patients.16,19 Turner et al., 25 report the use of strengthening exercises, standing, and walking with adolescent ECLS patients. Physiotherapy must be adjusted based on the child’s age, baseline developmental level, and neurological insults. 43
In long ECLS runs, early rehabilitation in children is believed to be pivotal to avoid a significant impact on motor response during growth. 21 Early rehabilitation and the aECLS approach are highly beneficial in postoperative outcomes, especially for transplant candidates. 30 This allows them to extend transplant candidacy 19,27,30 due to the limited organs available and the long waiting list.28,30 Zebur et al.17describe how the improved recovery supported by aECLS led to avoiding transplantation in a previously healthy child affected by ARDS. Despite ECLS being accepted as a fundamental approach to a successful bridge to transplantation, implementing the aECLS strategy was reportedly considered vital to obtain acceptable early outcomes and improved graft survival. 31 Its absence might be regarded as a contraindication to transplant itself.38,39 Cardiac rehabilitation was also analyzed by Amao et al., 21 resulting in a more beneficial outcome when aggressive physical and respiratory rehabilitation were combined to target physical function improvement instead of solely exercise to improve dynamic motion.
With a focus on facilitating physical movement, the following technical elements were reported as crucial. In V-A ECLS, when cannulas are inserted in one groin, 28 adequate cannula fixation and a large cannula (according to the patient’s anatomy) are mandatory to prevent respiratory decompensation and reintubation. 28 During V-V ECLS, the single site cannulation via bicaval dual-lumen cannula was recommended, despite the difficulties in children due to limited sizes, recirculation, limited/no patient collaboration, hemolysis, and risk of infection.34,36,40 Few reviews highlighted single-site cannulation as a sufficient treatment for hypercapnia/hypoxia, enabling longer runs, early rehabilitation, and optimal nutritional support by potentially eating normally.18,32 Interestingly, Schmidt et al. 27 brought attention to successful physical rehabilitation even when their decision shifted from a single cannula site to a dual cannulation strategy in both legs during V-V ECLS.
An innovative approach was described by Maeda et al., 26 who adopted the Berlin Heart cannulas for the V-V ECLS configuration, resulting in reduced recirculation, improved ambulation with the exit of cannulation in the abdomen, and right ventricular function maintained normal without deconditioning. The new configuration is supported by Stephens et al.'s newly published case series., 41 highlighting the increased cannula durability and security, as well as safety with the location away from the neck and expected decreased skin erosion due to less frequent resuturing. Similarly, Vijayakumar et al. 24 described their successful experience using the TandemLife Protek-Duo 42 cannula in a 14-year-old patient due to its unique curvature, allowing stability, less recirculation, and positioning manipulation, facilitating early rehabilitation and ambulation.
When femoral cannulation was required, Schmidt et al. 27 Proposed the Biomedicus (Medtronic Inc. Minneapolis, Minn) femoral cannula characterized by higher flexibility and resistance to bending, with a plate underneath, sutures, and transparent chlorhexidine drape for better fixation and monitoring of the cannula site.
The transition from V-A to V-V ECLS support was also urged if the priority for the patient’s recovery shifted to physiotherapy and ambulation. 17
Protocols and Multidisciplinary team requirements
Several studies reported the beneficial post-ECLS outcome in the presence of an experienced and specialized ECLS team.6,16,17,27 To ensure adequate staff capacity to support advanced rehabilitation treatment in the aECLS approach, Zebur et al. advised defining physical rehabilitation as a medical procedure to ensure staff availability and emphasize its relevance.
Several studies outlined prerequisites for implementing the aECLS strategy, including sedation weaning, tracheostomy, evaluation scores for pain and agitation, serial bronchoscopy before extubation, patient and circuit daily screening for compliance and efficiency, and personalized physiotherapy program.6,16,17,27 However, elements such as the intent and anticipated ECLS duration at the time of cannulation, ECLS circuit and patient hemodynamic stability, readiness and commitment of the team, readiness for reintubation, ECLS alone providing sufficient oxygenation, and discussion and consensus provided by families were also included.6,16,17,19,21,25,27,31 Interestingly, Turner et al. declared that patients supported on ECLS had access to transplant only if ambulatory status was achieved. 25
Despite the emerging evidence from single-center case reports of active physiotherapy’s benefits, no published guidelines were available until a recently published document by Shkurka et al. offered a useful initial tool designed to guide each center’s local policy and be adjusted accordingly. 43
Safety and survival
Overall, the aECLS strategy did not lead to more severe complications about a conservative approach with fully sedated patients,6,16,17,20,27 with an impressive 39.7% of cases reporting the absolute absence of complications and 81.5% of children discharged alive from the hospital.
Limitations
Several limitations characterize this review, such as small sample size, retrospective data collection, single institution data collection, young adults in addition to children, and limited information in the literature on ambulatory ECLS in children. These studies are likely subjected to further confounding additional risks of recall bias, selective outcome reporting, and selective analysis reporting biases, thereby excluding patients with complicated or adverse outcomes. The missing data in essential variables (such as weight) may cause biased estimates, reducing efficiency. Information regarding pain and sedation assessment tools, score targets, and medication adjustments during activities are extremely scarce despite the potentially huge impact they may have on future guidance and recommendations. Moreover, despite applying clear inclusion criteria, we cannot eliminate the possibility of missing some crucial cases aggregated in a more extensive series. Therefore, it is pivotal to consider these when interpreting the results of this study.
Conclusion
Our study shows the safety and feasibility of the aECLS strategy in children, presenting different clinical backgrounds and indications, ECLS mode, and cannula configurations, with varying levels of physiotherapy and respiratory status achieved mainly due to age limitations. This review encourages a more profound exploration of the “Awake ECLS” notion based on the flourishing evidence of benefits witnessed and the fundamental concepts of liberation from IMV and physiotherapy practice. Nevertheless, more consistent and standardized practice is necessary to evaluate outcomes more systematically and objectively. Multicenter randomized controlled trials are required.
Supplemental Material
Supplemental Material - Individual patient data meta-analysis on awake pediatric extracorporeal life support: Feasibility and safety of analgesia and sedation weaning, liberation from mechanical ventilation, and physiotherapy
Supplemental Material for Individual patient data meta-analysis on awake pediatric extracorporeal life support: Feasibility and safety of analgesia and sedation weaning, liberation from mechanical ventilation, and physiotherapy by Marta Cucchi, Silvia Mariani, Michal J. Kawczynski, Emma Shkurka, Fabio Ius, Giuseppe Comentale, Aparna Hoskote and Roberto Lorusso in Perfusion.
Footnotes
Author contributions
Marta Cucchi: Concept/design, Data collection, Data analysis/interpretation, Statistics, Drafting article, Critical revision of article, Approval of article. Silvia Mariani: Concept/design, Data collection, Data analysis/interpretation, Statistics, Drafting article, Critical revision of article, Approval of article. Michal J. Kawczynski: Statistics, Critical revision of article, Approval of article. Emma Shkurka: Critical revision of article, Approval of article. Fabio Ius: Critical revision of article, Data collection, Approval of article. Giuseppe Comentale: Critical revision of article, Approval of article. Aparna Hoskote: Concept/design, Data analysis/interpretation, Critical revision of article, Approval of article. Roberto Lorusso: Concept/design, Data analysis/interpretation, Critical revision of article, Approval of article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Roberto Lorusso is a consultant for Medtronic, Getinge, Abiomed and LivaNova, and an Advisory Board Member of Eurosets and Xenios: all honoraria are paid to the University for research support.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.