
Abstract
Background and purpose
Extracorporeal membrane oxygenation (ECMO) continues to play an essential role in organ support in cardiogenic shock or acute respiratory distress syndrome and bridging to transplantation. The main purpose of the present survey was to define which clinical and organizational practices are adopted for the administration of physiotherapy in adult patients undergoing ECMO support worldwide.
Methods
This international survey was conceived in November 2021. The survey launch was announced at the 10th EuroELSO (European ELSO chapter) Congress, London, May 2022.
Results
The survey returned 32 questionnaires from 29 centers across 14 countries. 17 centers (53.1%) had more than 30 intensive care unit beds available and most (46.8%) were able to care for five to 10 patients on extracorporeal life support simultaneously. The predominant physiotherapist-to-patient ratio was 1:>5 (37.5%); physiotherapy was available 5/7 days and 7/7 days by 31.2% and 25% respectively. Respiratory physiotherapy was not defined by a specific protocol in most centers (46.8%) while 31.2% declared that the treatment commences less than 12 h after sedation is stopped/reduced. Mostly, early physiotherapy in non-cooperative ventilated patients was provided within the first 48 h (68.6%) and consisted of as passive range of motion, in-bed positioning, and splinting. Postural passages and sitting were provided to patients and walking was included in those advanced motor activities which are part of the treatment.
Conclusion
Physiotherapy in patients on ECLS is feasible, however substantial variability exists between centers with a trend of delivering not protocolized and understaffed rehabilitation practices.
Keywords
Background
Cardiogenic shock and acute respiratory distress syndrome are major causes of morbidity and mortality worldwide, requiring intensive care including extracorporeal life support, and represent an immense social and long-term health burden.1–3 Extracorporeal membrane oxygenation (ECMO) plays an essential role in the management of these conditions by facilitating organ support bridging patients to recovery or transplantation.4,5 Continuous improvement in oxygenators, pumps and circuit design 6 have resulted in decreased device complexity and size, as well as enhanced safety and portability. Nevertheless, ECMO remains a high-risk therapy with numerous known complications such as bleeding, thrombosis, and infection.7–10 Further, disability after ICU stay and long-term mechanical ventilation is frequent with a substantial number of patients needing prolonged hospital stay and rehabilitation.11–13 Early physiotherapeutic interventions and rehabilitation have been implemented to improve outcomes for ECMO candidates14–18; however, careful patient selection is crucial to ensure favorable outcomes.19–21 Although several studies describe physiotherapeutic practices for patients while on ECMO support,22–44 there is a need for more detailed information about physiotherapy provision and management.
Respiratory physiotherapy plays a crucial role in secretion removal, improving lung volumes and gas exchange and reducing work of breathing. 39 It is a first-line intervention constituted of several techniques including manual and mechanical techniques such as deep breathing, airway clearance, respiratory muscle training, assisted coughing, noninvasive ventilation, and expiratory flow acceleration. The latter can be used to promote secretion clearance using different techniques,45,46 including PEEP-ZEEP (positive end-expiratory pressure-zero end-expiratory pressure) which imposes a gradual PEEP on the respiratory system followed by an abrupt reduction to zero cmH2O.
The aim of the current survey is to evaluate clinical and organizational practices adopted for the administration of physiotherapy in adult patients undergoing ECMO support worldwide.
Methods
The survey questionnaire was approved by members of EuroELSO Scientific and Steering Committees. The survey was largely promoted through the Organization Web site, social media channels (Figure 1) and during the 10th EuroELSO Congress in London, May 4th – 6th, 2022. Data entry was enabled between April 30th and 15 June 2022. Screenshot of survey announcements via social media on EuroELSO channels.
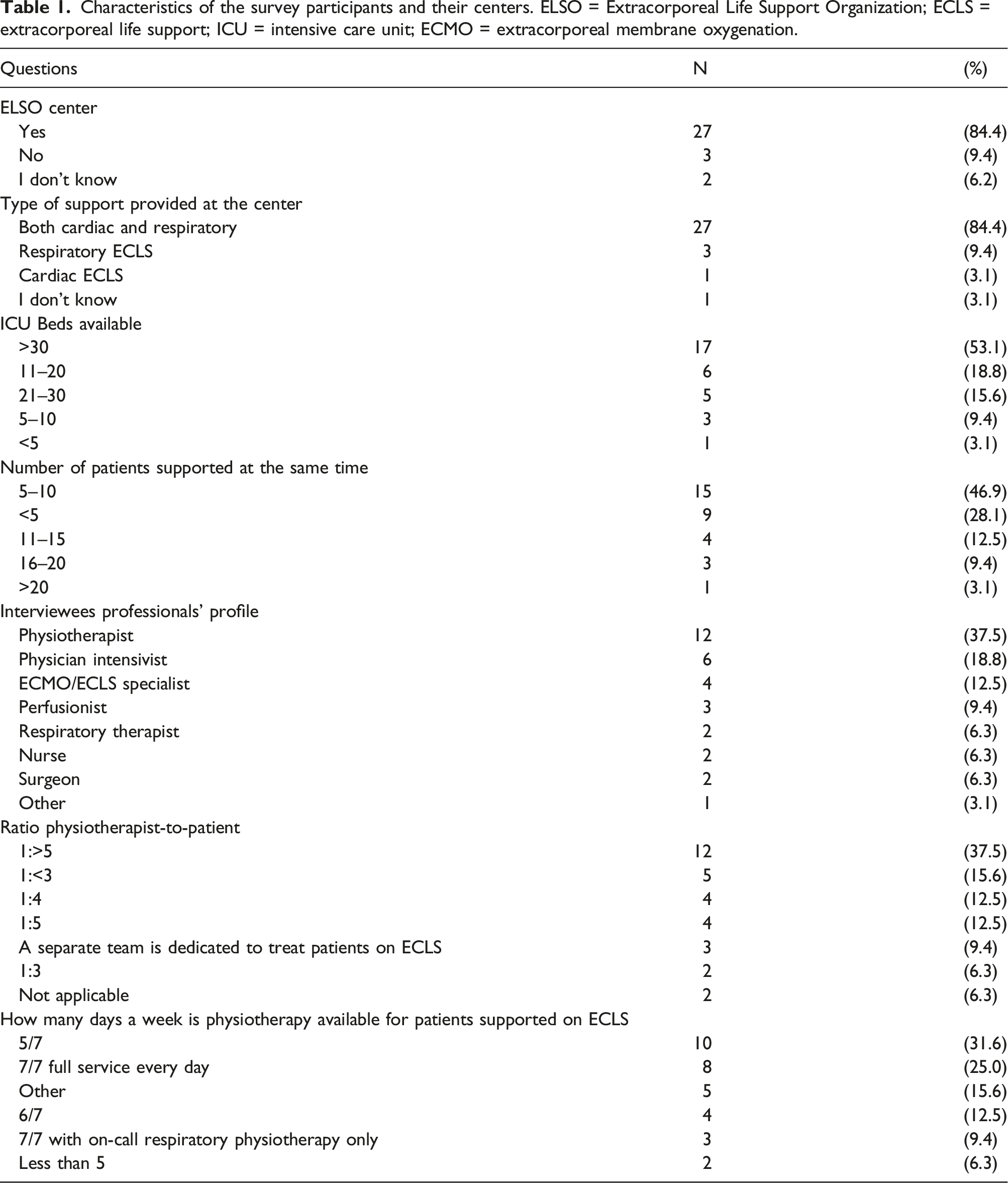
Characteristics of the survey participants and their centers. ELSO = Extracorporeal Life Support Organization; ECLS = extracorporeal life support; ICU = intensive care unit; ECMO = extracorporeal membrane oxygenation.
In accordance with General Data Protection Regulation, no respondent data was stored. Institutional Review Board review was considered to be exempt prior the data such that individual subjects cannot be identified in any way. Participation in the survey was voluntary. Results are presented as descriptive statistics.
Results
The survey returned 32 questionnaires from 29 centers across 14 countries (Figure 2). Most respondents were from ELSO centers hosting both cardiac and respiratory support and were physiotherapists (Table 1). 17 centers (53.1%) had more than 30 ICU beds available and most (46.8%) were able to care for five to 10 patients on extracorporeal life support simultaneously. The predominate ratio of physiotherapist-to-patient was 1:>5 (37.5%); physiotherapy was available 5/7 days and 7/7 days by 31.2% and 25% respectively (Table 1). However, five respondents provided the following alternative information on this specific aspect providing different options: 5 days a week, reduced service over a weekend for rehabilitation and respiratory therapy and overnight on-call seven days per week; 7/7 with on-call and enhanced weekend services; 5/7 days, with 24/7 on-call and emergency respiratory service at weekends; 5/7 twice a day; 5 days usual service, 2 days respiratory treatments plus rehabilitation as able. Geographical distribution of the survey participants: 32 respondents from 29 centers (14 countries) completed the survey.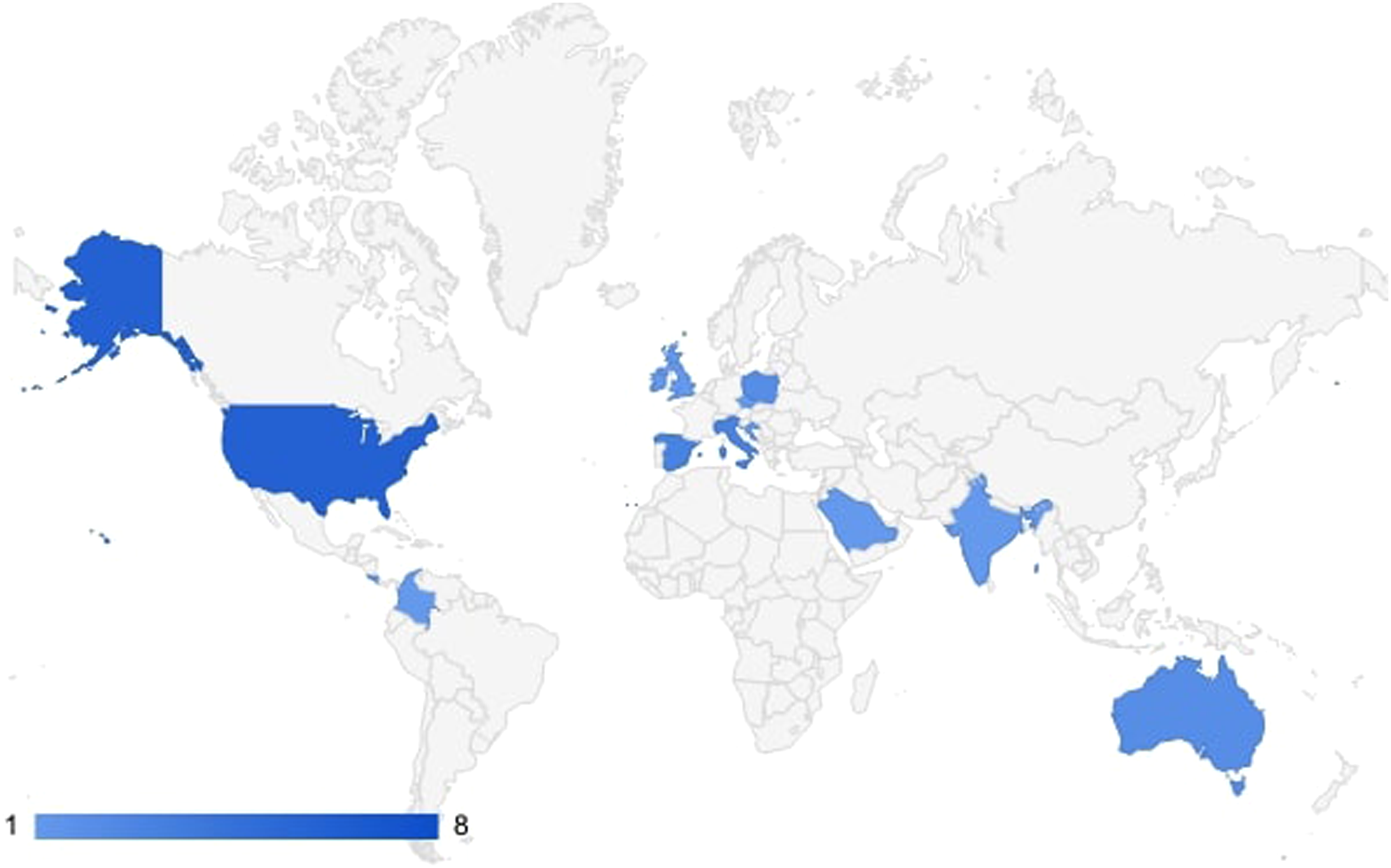
Respiratory physiotherapy
Respiratory physiotherapy in ECLS. ECLS = extracorporeal life support; RASS = Richmond Agitation-Sedation Scale; MI-E = mechanical insufflation-exsufflation; ACBT = active cycle of breathing techniques; CPAP = continuous positive airway pressure; PAP = positive airway pressure; IPPB = intermittent positive pressure breathing; FET = forced expiratory technique; VPEP = vibratory positive expiratory pressure; PEP = positive expiratory pressure.
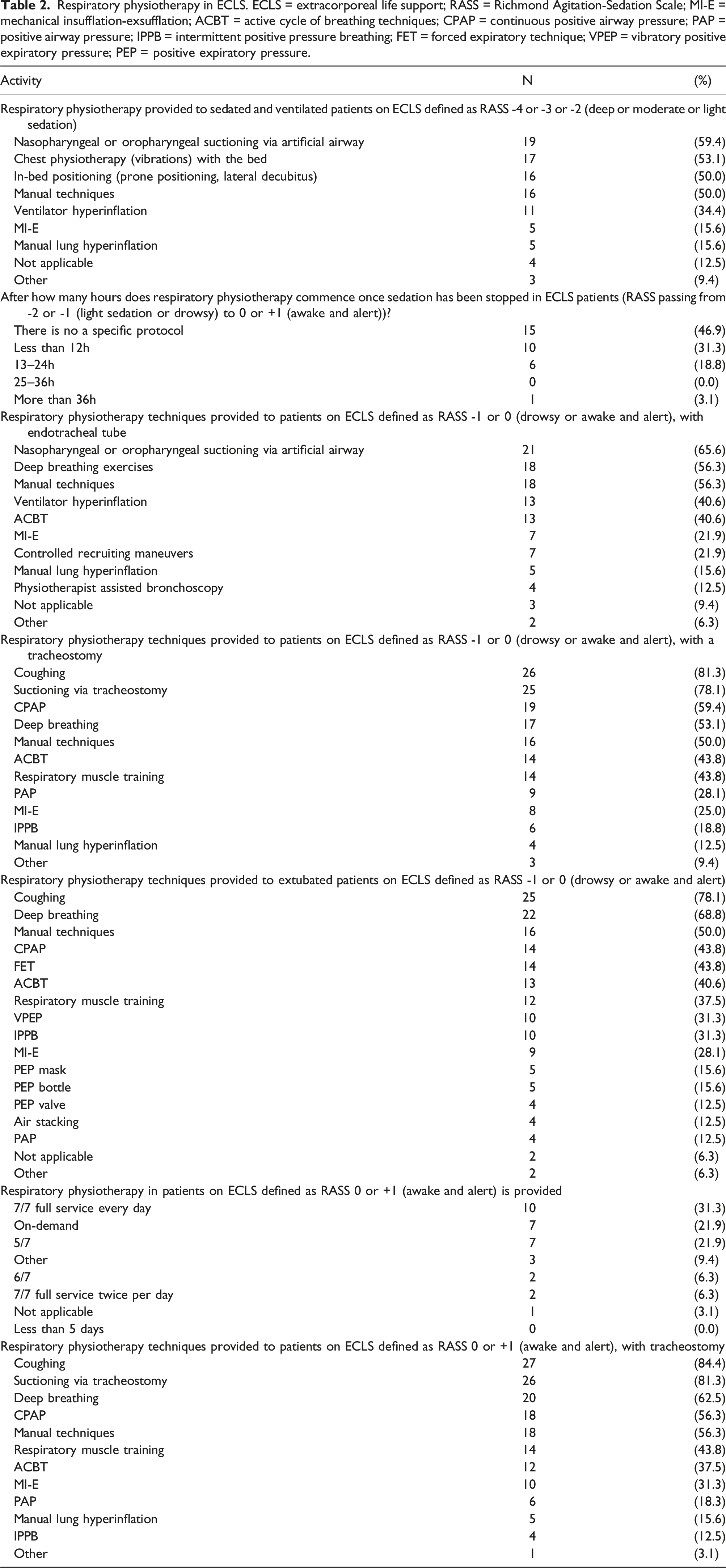
In those drowsy or awake and alert patients with the endotracheal tube, respiratory physiotherapy mainly consisted of nasopharyngeal or oropharyngeal suctioning via artificial airway and deep breathing exercises (Table 2). One respondent indicated that treatment was not based on the RASS.
Coughing, together with deep breathing and suctioning were the most reported interventions in those drowsy or awake and alert patients with or without a tracheostomy. One respondent highlighted that ventilator hyperinflation was provided as a respiratory treatment in this group. Respiratory treatments were mostly described as available on 7/7 full service every day (31.2%) or provided on demand (21.8%), or on a 5/7 basis (21.8%) (Table 2) in awake and alert patients. Three respondents provided additional details highlighting patients would be reviewed a minimum of 5 days per week for rehabilitation, which would include respiratory assessment with reduced service over the weekend; treated 5/7 twice a day, or as required.
Motor activity/exercise
Physiotherapy and exercise in ECLS. ECLS = extracorporeal life support; RASS = Richmond Agitation-Sedation Scale; ECMO = extracorporeal membrane oxygenation.
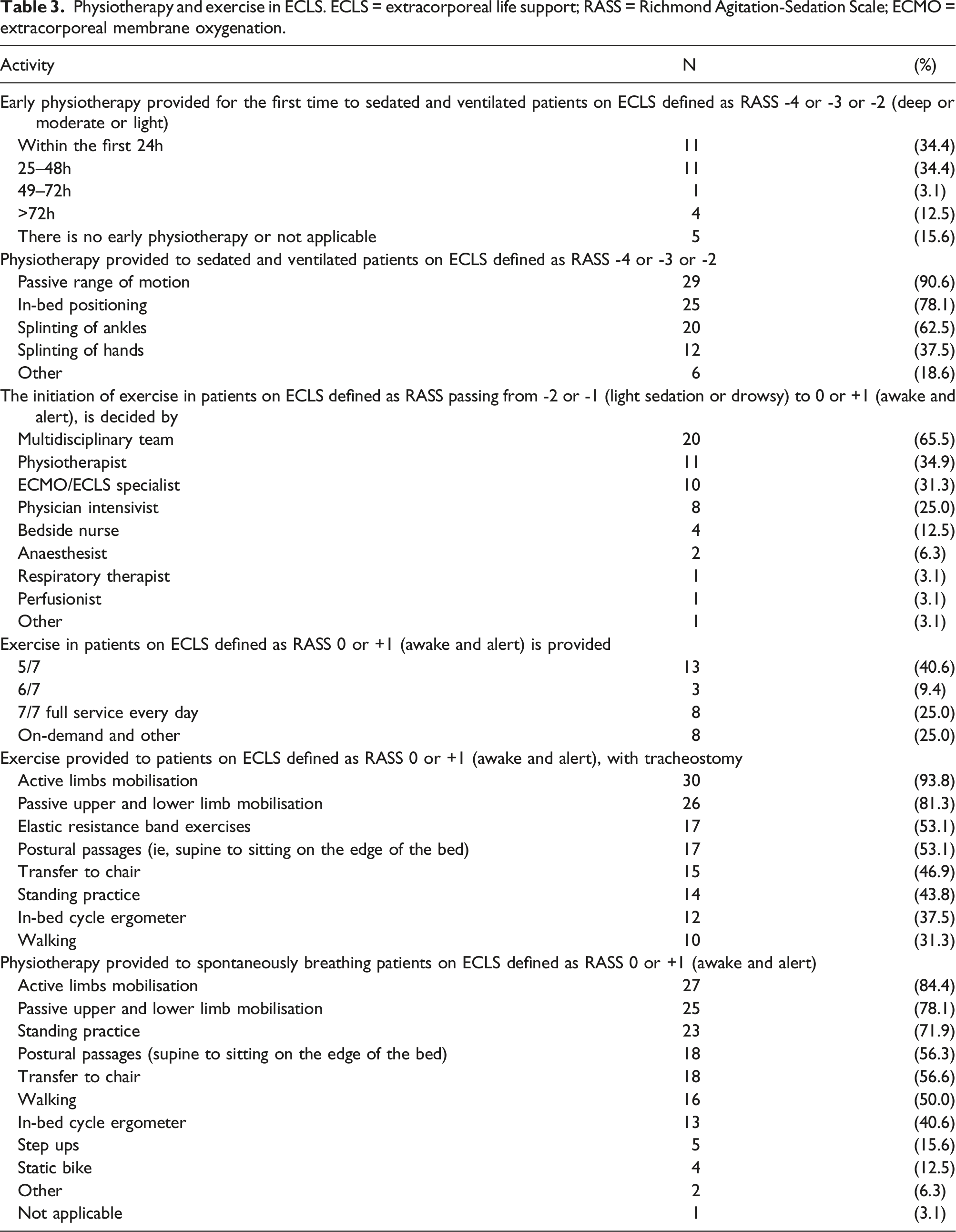
In light sedated and awake and alert patients, the initiation of exercise is mainly decided by the multidisciplinary team, physiotherapist, and ECMO/ECLS specialist; an interviewee has specified the patients take an active role in such decision.
Exercise in awake and alert patients is provided 5/7 days by most centers (40.6%); one respondent highlighted they provide physiotherapeutic treatment twice a day. Patients with endotracheal tube are mostly subjected to passive and active limb mobilization, postural passages, and elastic resistance band exercises (Table 3). Spontaneously breathing patients with or without tracheostomy continue these activities but more attention is given to standing practice and transfer to chair together with other active exercises (Table 3).
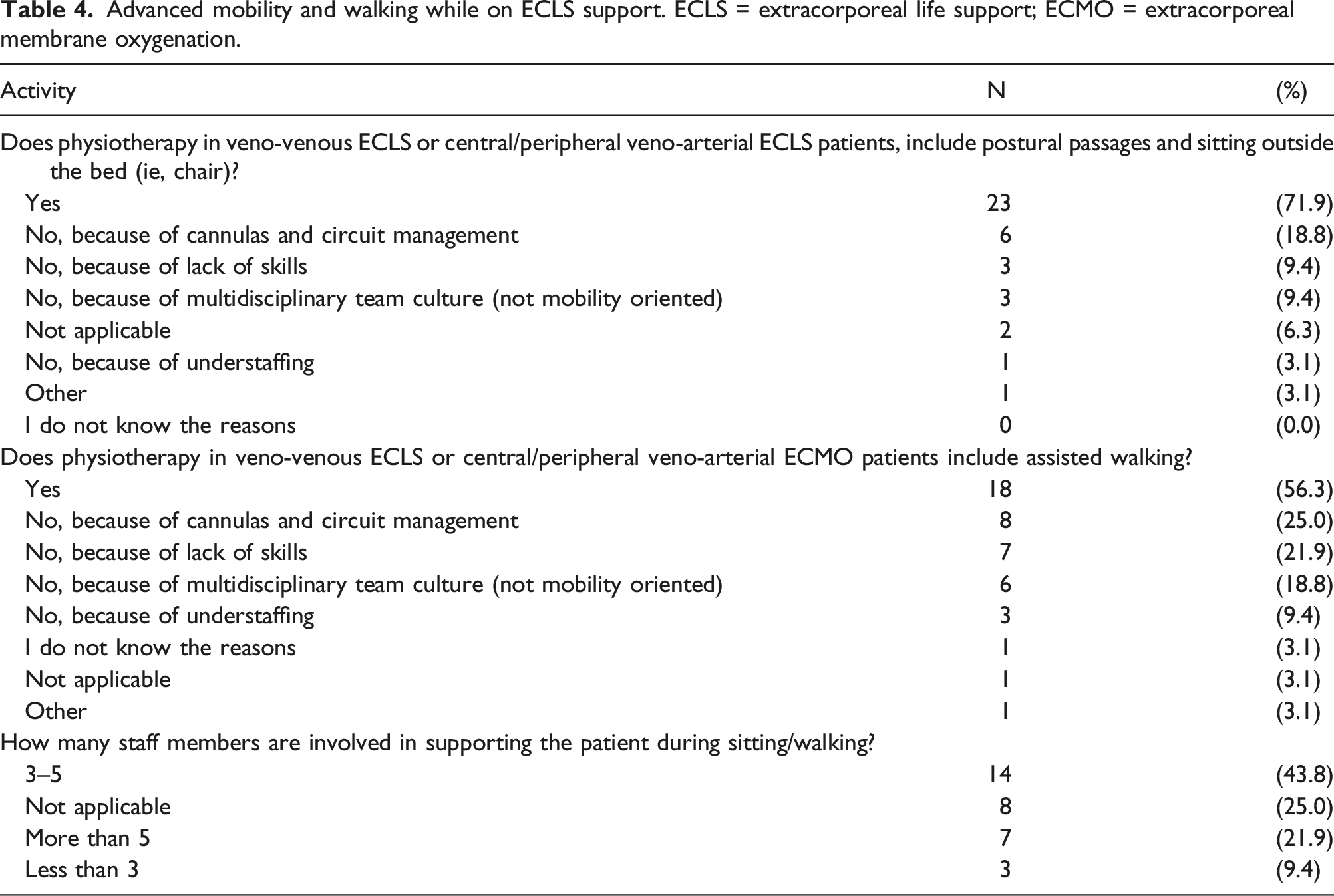
Walking while on ECMO; advanced mobility
Advanced mobility and walking while on ECLS support. ECLS = extracorporeal life support; ECMO = extracorporeal membrane oxygenation.
Discussion
This is the first structured survey focused on the current physiotherapeutic interventions for patients with extracorporeal support. Detailed information about physiotherapy practices was collected with responses from 14 countries. The main finding is that there is a substantial variability between centers, that much of the physiotherapeutic interventions are not protocolized and that rehabilitation is commonly understaffed. Multidisciplinary teamwork strongly characterizes extracorporeal life support, and different professional profiles are involved in the pathway of care. In this survey, 37.5% respondents were physiotherapists, but it is not known if physiotherapists were consulted on responses submitted by other multidisciplinary team members. Most responses came from centers with >30 ICU beds; however, the majority had 10 beds or fewer for patients on ECLS.
From a service provision perspective, the results show that there is reasonably good availability of respiratory physiotherapy throughout the week, weekend and around the clock.
The Guideline for the Provision of Intensive Care Services recommends the ratio of 1:4 physiotherapist to patient in ICUs. 47 However, most centers responded having a ratio of >1:5 physiotherapist to patients, which could be more than five and is not quantified. These findings highlighted again the problem of understaffed physiotherapy teams, although, separate and dedicated rehabilitation teams may also be available for patients on ECLS. On the other hand, understaffing is common when considering rehabilitation personnel deployment as it has been observed during the COVID-19 pandemic. Interestingly, some centers declared having no physiotherapy services – it is not known whether respiratory and rehabilitation services are performed by other members of the multidisciplinary team.
Most centers commenced physiotherapy early, within the first 48 h of admission. The provision of passive and active rehabilitation is graded based on the level of sedation of the patient and their airway. As patients are more awake, they are more interactive and more engaged in their treatment, it is allowing the transition from passive and invasive techniques such as suctioning to more independent options such as active cycle of breathing techniques and deep breathing exercises. Many reported the use of positive pressure and deep breathing as part of the physiotherapy repertoire. This is an interesting practice point given the evidence supportive of protective lung ventilation. 48 It is also interesting to note that respiratory physiotherapy starts so early in the admission and hence future work should explore the timing and nature of respiratory physiotherapy, especially the role of positive pressure ventilation.
Within ECMO centers who responded to the survey, there is a significant focus on passive and active rehabilitation and this commences within 48 h of admission for the majority of centers. Active rehabilitation such as standing, and walking is also being performed in patients regardless of whether they are self-ventilating or have an oral endotracheal tube or a tracheostomy. Physiotherapy for patients on ECLS is evolving in complexity with further developments in commencing and continuing rehabilitation within multidisciplinary teams. When analyzing motor activities, standing practice is largely implemented across centers, including using a verticalization bed. About half of responding centers were capable to provide active walking to patients supported on ECLS. The “Walking on ECMO” procedure is a complex multidisciplinary activity with the potential for both device and patient associated complications. Furthermore, responding to emergency complications on ECLS, especially when away from the bedspace is challenging. Simulation and training may help make such procedures less stressful and avoid potential harm. This survey reflects the findings of other studies describing the implementation of standing and walking for patients on extracorporeal life support.28,30,38,39 The barriers for rehabilitation or weaning are previously described. 49 Within this, there is also a large variety in staffing required for safe mobilization on ECLS. The survey did not collect data to give clear reasons as to why physiotherapy staffing is inadequate, however in the experience of the authors, financial and logistic constraints and a reduced physiotherapy workforce are potential contributors, especially the absence of a mobility culture (Table 4) and underestimation of the rehabilitative needs. Research in the field of ICU rehabilitation might encourage proactive actions from managers and stakeholders. Increasing awareness of the importance of rehabilitation in critical settings is essential to break down organizational and logistic barriers.
Limitations
The main limitation in the interpretation of the results is the low response, which allows only descriptive characteristics and no generalizability. The sampling can be at risk of bias as no systematic sampling was performed. Furthermore, this questionnaire was conducted during an era where we still experienced an exponential increase in ECMO cases, especially since we were in a COVID-19 pandemic with limited resources available whilst ECMO has been proven as a viable option for COVID-19 ARDS. No complex analyses regarding center characteristics, age groups, patient categories, modes, and so on can be performed due to the survey database design. Further, participants from Asia or Africa are underrepresented.
A deficit in protocolized practices with a very heterogeneous approach makes it difficult to characterize the practice in a short survey. Thus, the questionnaire did not include any questions regarding complications of physiotherapy, especially during “Walking on ECMO” procedure. This survey is the first step in structured evaluation of available physiotherapy procedures, and the second step would be assessing complications and even outcomes.
Conclusion
The main finding of this EuroELSO-approved survey is, that physiotherapy in patients on ECLS is feasible, however a substantial variability exists between centers with a trend of delivering not protocolized and understaffed rehabilitation practices. Multidisciplinary care strongly characterizes physiotherapy in patients supported on ECLS, and different professional profiles are involved in the pathway of care. This survey might support the need for an international network dedicated to ongoing research on physiotherapy in patients supported on ECLS.
Supplemental Material
Supplemental Material - Physiotherapy for patients on extracorporeal membrane oxygenation support: How, When, and Who. An international EuroELSO survey
Supplemental Material for Physiotherapy for patients on extracorporeal membrane oxygenation support: How, When, and Who. An international EuroELSO survey by Massimiliano Polastri, Allaina Eden, Antonio Loforte, Andrea Dell’Amore, Marta Velia Antonini, Jordi Riera, Nicholas A Barrett and Justyna Swol
Footnotes
Acknowledgements
We kindly thank all survey participants.
We thank Louisa Fraederich, Annika Jaeckel, Katja Barthel, Alexandra Held, and Christian Reim from INTERPLAN (Hamburg, Germany) for their support in the survey announcement and data collection.
We also thank the members of EuroELSO Steering and Scientific Committees, Jan Belohlavek, Jana Assy, Jo-Anne Fowles, Jonathan H. Smith, Konstanty Szuldrzynski, Leen Vercaemst, Mark Davidson, Matteo DiNardo, Mirko Belliato, Peter P. Roeleveld, Robert Smith, Simon Finney, Thomas Müller, Felix Hennig, Tim Jones, Luis Pinto, Alain Combes, Matthieu Schmidt, Aparna Hoskote, Martin Balik, Mikael Broman, Antonella Degani, Dirk Donker, Peter Schellongowski, Chirine Mossadegh, Christian Karagiannidis, for survey approval and support in survey design.
Authorship
Conceptualization and survey design: Justyna Swol, Massimiliano Polastri, Antonio Loforte, Andrea Dell’Amore.
Revision of the survey design: Allaina Eden, Antonio Loforte, Andrea Dell’Amore, Nicholas A. Barrett, Marta Velia Antonini, Jordi Riera
Manuscript drafting: Massimiliano Polastri, Allaina Eden.
Manuscript revision: Allaina Eden, Antonio Loforte, Andrea Dell’Amore, Justyna Swol, Nicholas A. Barrett, Marta Velia Antonini, Jordi Riera, Massimiliano Polastri
All authors have read and approved the submitted version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.