
Abstract
Introduction
Extracorporeal cardiopulmonary resuscitation (ECPR) is associated with improved outcomes in select populations, however, crisis resource management (CRM) in this setting is logistically challenging. This study evaluates the impact of ECPR simulation on self-perceived confidence and collaboration of intensive care unit team members.
Methods
This is a prospective observational study analyzing data obtained between July 2018–December 2019. This study focused on non-surgical members of critical care team consisting of pediatric intensivists, resident physicians, registered nurses, respiratory therapists. Participants were expected to perform cardiopulmonary resuscitation (CPR) during the ECPR event, participate in code-team responsibilities and provide ancillary support during cannulation. Pre- and post-simulation surveys employed the Likert scale (1 = not at all confident, 5 = highly confident) to assess self-perceived scores in specified clinical competencies.
Results
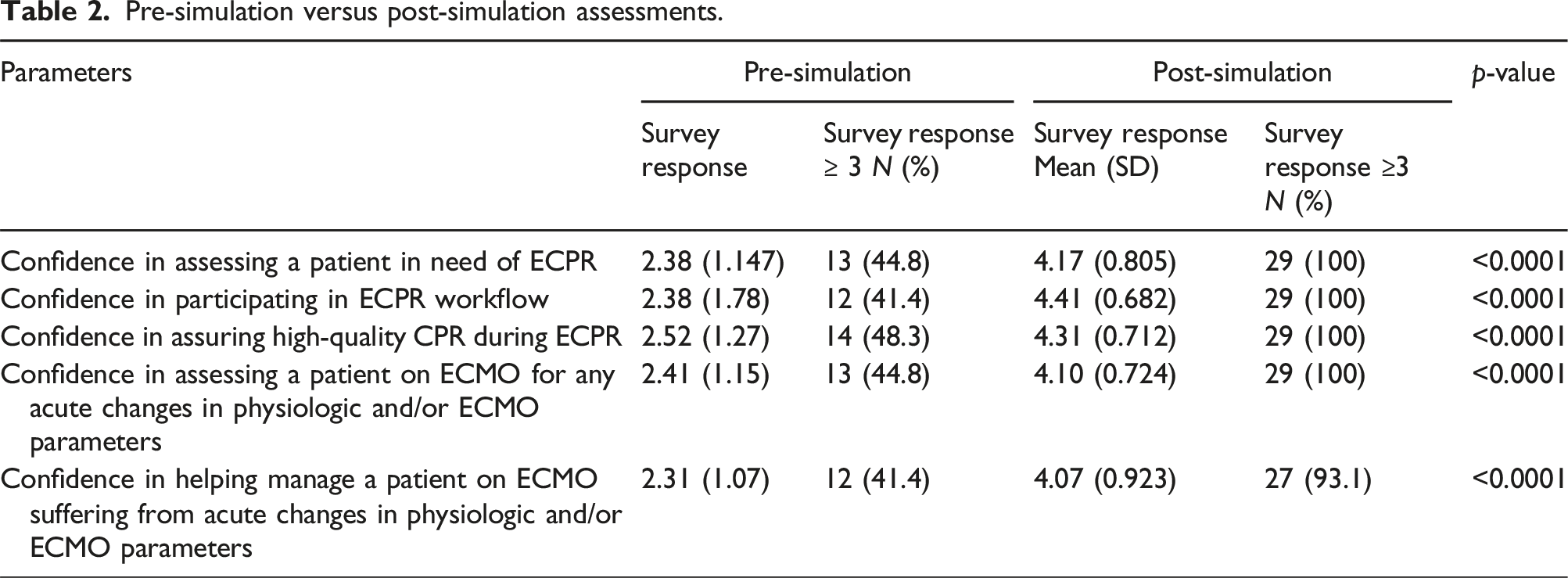
Twenty-nine providers participated in the simulation; 38% had prior ECPR experience. Compared to mean pre-study Likert scores (2.4, 2.4, 2.5), post-simulation scores increased (4.2, 4.4, 4.3) when self-evaluating: confidence in assessing patients needing ECPR, confidence in participating in ECPR workflow and confidence in performing high-quality CPR, respectively. Post-simulation values of
Conclusion
This study demonstrated preliminary feasibility of pediatric ECPR simulation in enhancing independent provider confidence and team communication. This self-perceived improvement may establish a foundation for cohesive CRM, in preparation for a real life ECPR encounter.
Introduction
Pediatric cardiac arrest accounts for a quarter of all pediatric mortalities and, compared to adult cardiac arrest, has contrasting outcomes after intervention primarily due to inherent underlying pathophysiology. 1 The standard intervention for pediatric cardiac arrest is cardiopulmonary resuscitation (CPR), within the pediatric advanced life support (PALS)) algorithm. In refractory cases of arrest, escalation of therapy to extracorporeal cardiopulmonary resuscitation (ECPR) is gaining traction. Formally, ECPR is defined as extracorporeal support initiation during conventional CPR or when repetitive arrest events occur without return of spontaneous circulation (ROSC) for >20 min1 1 Current evidence in adults suggests an improvement in survival as well as better neurologic outcomes after ECPR compared to conventional CPR. In children, while existing data is certainly not as robust, there is moderate evidence demonstrating similar outcome improvements.2–5
Notable resuscitation factors that determine outcomes of ECPR include quality of CPR before and during ECMO cannulation as well as adequacy of circuit flow. There is conflicting data regarding impact of duration of CPR prior to extracorporeal membrane oxygenation (ECMO) cannulation and outcomes following ECPR.6–9 Nonetheless, to provide a high-quality ECPR, the resuscitation team must establish a cohesive and coordinated workflow with the surgical team to minimize interruptions to compressions during cannulation. These elements are derived from a broader logistical framework known as crisis resource management (CRM).10,11At its core, CRM represents a fundamental set of cognitive and interpersonal principles such as situational awareness, role clarity, communication, prioritization, and debriefing. 12
In pediatrics, simulation has been identified to be an important method for overcoming both provider and trainee clinical knowledge gaps, thereby improving patient safety and quality of care.2,13,14 For critical, and often infrequently encountered situations such as ECMO or ECPR, pre-emptive provider education is pivotal to overcome situational unfamiliarity.15,16 Thus, our aim was to integrate a simulation-based educational curriculum in order to enhance the confidence and awareness of cardiac intensive care unit (CICU) team members during the ECPR encounter.
Methods
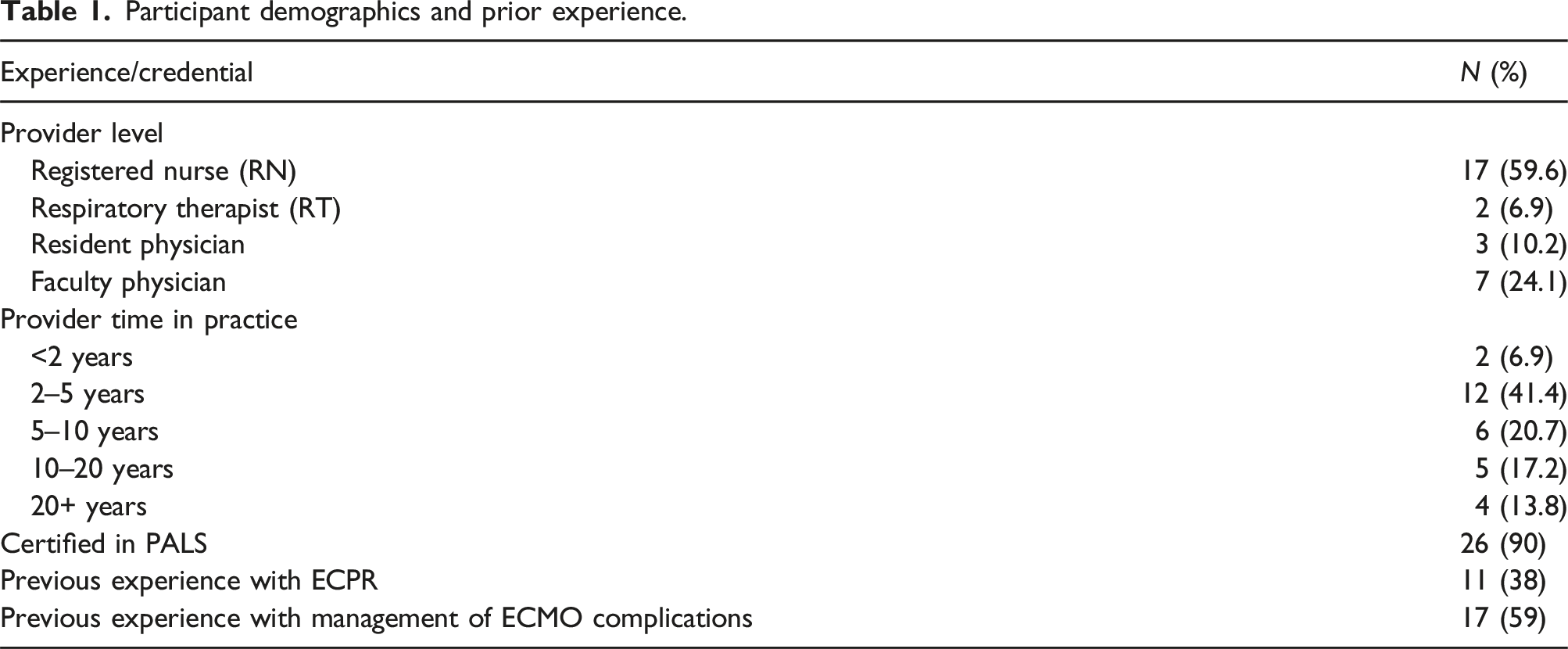
This is a prospective study conducted between July 2018–December 2019 that examined data collected during simulation exercises at the Children’s Hospital of San Antonio/Baylor College of Medicine. Institutional review board (IRB) approval was obtained and written consent was obtained from all participants prior to study initiation [H-41102]. As this study’s intent was to investigate the impact of simulation on non-surgical members of the ECPR activation team, study participants included: pediatric intensivists, pediatric resident physicians, registered nurses, and respiratory therapists. In order to minimize variation introduced by prior experience, participants were included only if they reported no previous formal ECMO or ECPR simulation training. Though included as members of the physical simulation, surgeons and ECMO specialists/technicians were not included in the analysis. Demographic information was collected from participants to better elucidate provider training level, number of years in practice, certification status, and any previous experience managing patients on ECMO.
The simulation scenario was adopted from a common, real-life, PICU ECPR scenario of cardiac arrest in a child with worsening bradycardia due to acute hypoxemia related to acute, severe asthma. The scenario had clear objectives and a structured design based on the well-recognized simulation design standards published by the International Nursing Association for Clinical Simulation and Learning Standards.17,18
Each participant was expected to function in their normal roles and scopes of practice within the scenario. The pediatric intensivist carried out the role of code team leader, with assistance from the resident physician. The respiratory therapist performed airway and ventilator management when necessary. The nursing staff was responsible for medication preparation, medication administration, event documentation and cardiopulmonary resuscitation. Scenarios were conducted in the hospital simulation center, which is distant from standard patient care areas, to avoid jeopardizing patient care, study participants’ privacy, or confidentiality. The ECPR manikin was designed only for veno-arterial cannulation through the right carotid artery and right internal jugular vein and is displayed in Figure 1. Simulation manikin with reusable carotid and internal jugular vascular conduits for right neck veno-arterial cannulation.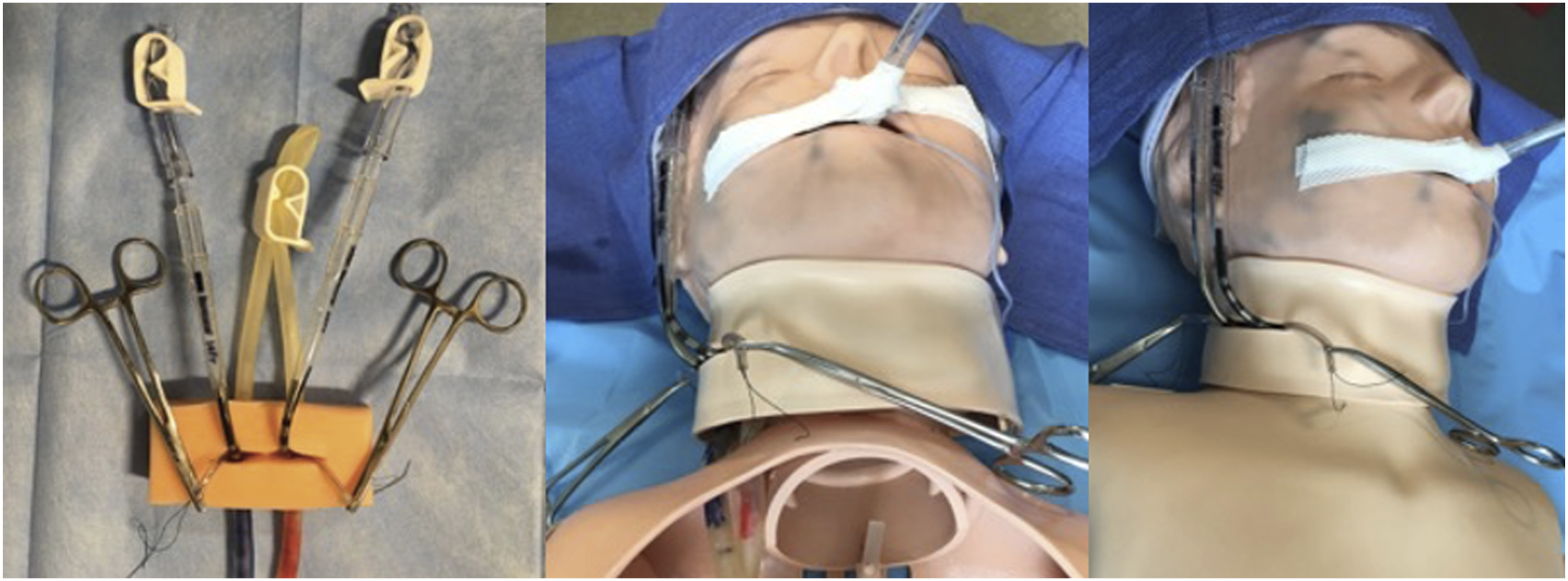
The simulation technician prepared the manikin as well as all the simulation resources such as code cart, gowns, masks, and monitor settings. Before initiating the scenario, participants were educated about the logistics of simulation, location of all clinical supplies, and familiarized with details of the pre- and post-simulation questionnaires. Before starting the scenario, participants completed the pre-simulation questionnaire to assess their initial confidence level in assessing and managing a child in need of ECMO. Subsequently, the nurse educator provided orientation about the manikin at the bedside and verbalized the case vignette to the participants in order to provide clinical context for the impending simulation. The simulation team appointed one of the nurse participants to be the primary bedside/code nurse. During the scenario, the simulation technician altered the patient’s clinical parameters on the monitor to reflect real time response to interventions while the facilitator observed the participants through the control room. The manikin itself did not have interactive or remotely controlled physiologic features, thus participants implemented therapies based upon the vital signs and parameters displayed by the technician on the monitor.
At the conclusion of the scenario, the facilitators conducted structured video debriefing sessions, specifically so that recorded footage could be replayed and analyzed more critically. The previously validated Debriefing Assessment for Simulation (DASH) model was integrated, which is based upon evaluating human growth in experiential contexts specifically in regards to participant thought processes and synthesis of actions. 19 Thus, debriefing focused on verbally exploring the teamwork, communication, collaboration, and overall medical management experienced in the scenario. Participants shared observations regarding efficiency and cohesiveness of closed loop communication throughout the simulation and its influence on delivery of ECPR. After the video debriefing, participants completed the post-simulation questionnaire.
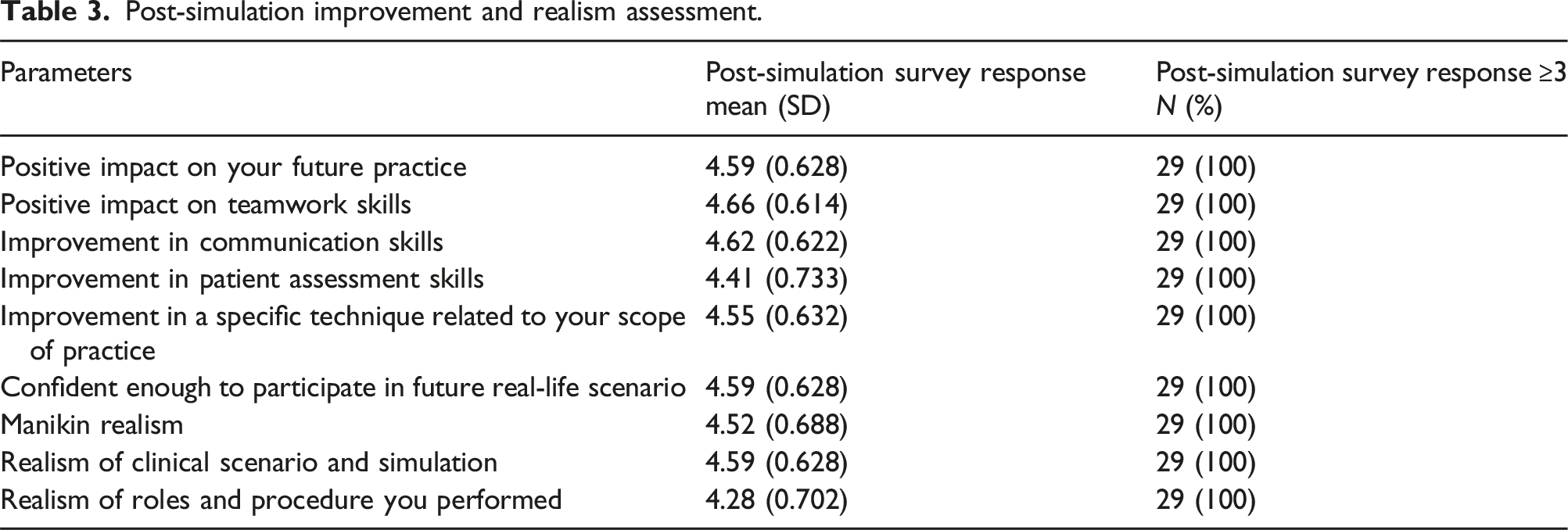
We utilized pre- and post-simulation questionnaires that employed the Likert scale (1 = not at all confident, 5 = highly confident) to assess self-perceived scores in specified clinical competencies, both before and after simulation. These included (1) confidence in assessing a patient in need of ECPR, (2) confidence in participating in the ECPR workflow, (3) confidence in assuring high-quality CPR during ECPR, (4) confidence in assessing a patient on ECMO for any acute changes in physiologic and/or ECMO parameters, and (5) confidence in helping manage a patient on ECMO suffering from changes in physiologic and/or ECMO parameters (Supplement 1). The assessments, provided insight on the scenario’s impact on practice, teamwork, communication, and assessment skills. 20 Participants were then asked to gauge improvement in ECPR performance as well as their confidence in entering a similar clinical situation in future, based on a Likert scale (1 = not at all, 5 = a lot/highly). (Supplement 2). Participants also assessed the perceived realism of the ECPR manikin, the clinical scenario, and realism of stress experienced during the simulation. Chi-squared/Fisher’s exact tests were used to compare categorical variables with significant set at p < .05.
Results
Participant demographics and prior experience.
Before completing the simulation exercise, 45% (n = 13) reported confidence in assessing a patient in need of ECPR, 41% (n = 12) said they were confident in participating in ECPR and 48% (n = 14) said they were confident in assuring high-quality CPR during and ECPR encounter. 45% (n = 13) said they were confident in assessing a patient on ECMO, while 41% (n = 12) reported they were confident in managing a patient on ECMO for any acute changes in physiologic parameters.
Pre-simulation versus post-simulation assessments.
Post-simulation improvement and realism assessment.
Discussion
Our pilot study introduces the preliminary benefits of a simulated ECPR training environment to develop the confidence and coordination of pediatric intensive care team members. Overall, participants subjectively reported significant improvement in assessment and management of patients in need of ECPR as well as increasing confidence levels during emergent cannulation and resuscitation. We believe that this simulation exercise shows feasibility in improving elements of crisis resource management by teaching situational awareness and provider communication.
Existing literature discussing ECPR simulation is quite limited. Most studies largely consist of investigations into adult resuscitation training,21–24 while those examining pediatric ECPR are scarce.25–27 Briefly, ECPR simulation has been associated with decreased time to cannulation and full ECMO flow, both of which are invaluable prognostic benchmarks. 28 However, to date, no studies examine the attitudes and reactions of the non-surgical intensive care providers following focused ECPR simulation.
The ECPR workflow, from initial identification of arrest to initiation of full support, necessitates all involved providers to not only be confident in their own scopes of practice, but also in the competencies of those around them. As such, the cannulating surgeons must be assured that the pediatric intensivist, advanced practice providers, critical care nursing staff, respiratory therapist and other staff can administer critical medications, perform effective CPR, and deliver stable ventilatory support throughout the entire resuscitation event in order to maximize patients’ chances for survival. We demonstrate that this level of both self- and situational confidence can be nearly doubled through simulation training, especially in a heterogenous group with varying years of experience, training backgrounds, and previous exposure to ECMO.
A notable drawback to existing simulation programs is the lack of a standardized ECPR curriculum across ECMO centers. Particularly in pediatrics, allocating simulation resources for this type of ‘rare’ event would have been difficult to accomplish two or three decades ago, however this paradigm shifted when ECPR was initially incorporated into the formal PALS guidelines in 2005 and reiterated in each subsequent focused update.29–31 To further this point, Sawyer et al.’s report quantified the use of ECPR in pediatric cardiac arrest to be over 25% from 2014–2016. 32
Even more recently, a survey of 40 hospitals with non-cardiac ECPR programs reported an average of approximately six activations per year, though dedicated simulation programs were identified in only 55% of centers. 33 This disparity is likely to increase even more if both cardiac and non-cardiac programs were to be examined. Thus, a concerted and standardized approach to educating and training both surgical and non-surgical intensive care providers is undoubtedly warranted. Our findings exemplify a feasible method of assuring independent provider confidence and awareness. It is our hope that these skills serve as a foundation for cohesive CRM, should these participants be involved in a true ECPR encounter in the future.
Limitations
The primary limitation of this study is the small participant sample size. As this investigation was intended to be a pilot study, it is our hope that the encouraging results will incite future large-scale simulation studies both at our institution and others across the nation. Additionally some may identify omission of cannulation and other procedural data as a limitation. However as previously discussed, the intent of our study was to specifically to focus on perspectives of the non-cannulating ICU team, as these providers are pivotal in ensuring ongoing patient resuscitation before, during and after cannulation events. Future studies may warrant integration of surgeon feedback in order to assess the realism of the cannulation process. Finally, we acknowledge the inherent limitations of subjectively data derived from participant perception. Now that we have established data from this small pilot study, we hope to construct upcoming studies using objective scoring rubrics completed by masked reviewers.
Conclusions
This pilot study demonstrated preliminary feasibility of pediatric ECPR simulation in improving situational confidence of intensive care team providers. Future investigations with more objective measures of CRM-related skills may help identify further provider knowledge gaps in optimizing workflow within the ECPR process.
Supplemental Material
Supplemental Material - Implications of pediatric extracorporeal cardiopulmonary resuscitation simulation for intensive care team confidence and coordination: A pilot study
Supplemental Material for Implications of pediatric extracorporeal cardiopulmonary resuscitation simulation for intensive care team confidence and coordination: A pilot study by Toluwani Akinpelu, Nikhil R Shah, Karen Weaver, Nicole Muller, James McElroy and Utpal S Bhalala in Perfusion
Supplemental Material
Supplemental Material - Implications of pediatric extracorporeal cardiopulmonary resuscitation simulation for intensive care team confidence and coordination: A pilot study
Supplemental Material for Implications of pediatric extracorporeal cardiopulmonary resuscitation simulation for intensive care team confidence and coordination: A pilot study by Toluwani Akinpelu, Nikhil R Shah, Karen Weaver, Nicole Muller, James McElroy and Utpal S Bhalala in Perfusion
Footnotes
Author note
Meeting Presentation: The abstract was presented as a podium presentation at the 2023 Critical Care Congress in San Francisco, CA. (January 21-24, 2023)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.