
Abstract
Introduction:
Survival rates for cardiac arrest remain low. Extracorporeal cardiopulmonary resuscitation (ECPR) may offer a survival advantage in carefully selected patients. There is limited published data on ECPR in the UK and therefore this study aims to describe the last 11 years provision and outcomes of ECPR in the UK.
Methods:
This was a multicentre retrospective cohort study in the UK. Centres offering Extracorporeal membrane oxygenation (ECMO) as a potential support in the UK were identified at the first UK ECPR Summit. All centres were asked to submit data on their veno-arterial (VA) ECMO and ECPR patients between 1st January 2012 and 31st December 2022.
Results:
Over the 11-year period, 2117 patients received VA-ECMO in the UK with 963 survivors at 6 months (45.5%). Of these there were 302 ECPR runs with 92 survivors (30.5%). ECPR contributed to 14.3% of the total VA ECMO runs, with wide between-centre variation ranging from 5.4% to 73.3%. Centres provided a detailed dataset for 129 of the 172 consecutive ECPR cases for a 5-year period to 31st December 2022. The mean (SD) age was 46 ± 5 years, 77% were male and 48.9% presented with a shockable rhythm. The leading cause of cardiac arrest was ischaemic heart disease (45%). Only 14% achieved transient or sustained return of spontaneous circulation prior to initiation of ECMO flow, with mean time CPR to full ECMO flow of 52.5 ± 17.1 min. Percutaneous cannulation was performed in 85.3% of cases, with 51.9% of these procedures taking place in the cardiac catheter laboratory.
Conclusion:
In an UK cohort of VA ECMO and ECPR patients, the survival rates were comparable to other international registries. The variation in practice highlights the need to explore and address inequity of access to ECMO and ECPR services.
Introduction
Survival from cardiac arrest in the United Kingdom (UK) remains low and relatively unchanged over the last decade. 12 The national in-hospital cardiac arrest audit shows a survival to hospital discharge of 21.6%. 1 In out-of-hospital cardiac arrest, survival is 27% in patients presenting with ventricular fibrillation or tachycardia (VF/VT) 2 at 30 days, and only 8.1%–8.6% overall. 2 In refractory cardiac arrest, defined as more than three cycles of advanced life support without return of spontaneous circulation, this proportion is even lower. Survival rates non-linearly decrease with every minute of cardiopulmonary resuscitation (CPR), with <1% 30-day good neurological survival by 35 min of CPR. 3
ECMO is an innovative therapy that can be deployed rapidly both in and out of hospital, effectively supporting the function of the heart and the lungs. It is therefore an attractive solution to cardiac arrest with 20,675 adult ECPR patients reported to the Extra Corporeal Life Support Organisation (ELSO) registry with 31% survival to discharge or transfer. 4
Three randomised control trials have been published since 2020. ARREST 5 demonstrated a 43% survival to hospital discharge with ECPR and 7% in the conventional CPR group (p ⩽ 0.0001). Prague OHCA 6 found 31.5% survival in the ECPR group and 22% in standard care (p = 0.09). These were both single centre studies of experienced ECPR systems. A third trial, INCEPTION, 7 was multi centre and showed no difference between the two groups with 14/70 (20%) survival in the ECPR group and 10/62 (16%) in the conventional CPR group (p = 0.52).
ECPR has been performed in the UK for over a decade but there is lack of data on activity and outcomes. To date only three British services have published service level data, all of which reported small numbers of patients. A semi-rural helicopter emergency medical service (HEMS) transported seven patients to a metropolitan ECMO centre in a 4-year period, of which two were treated with ECPR. 8 The eventual outcomes were not reported. A metropolitan HEMS team reported treating five patients with ECPR commenced pre-hospital as a feasibility study conducted over 27 trial days during a 6 month and subsequent 7-month period. Two of these patients survived with clinical performance category score (CPC) three at hospital discharge. 9 Finally, an established ECMO centre in a specialist cardiac hospital treated 13 patients with ECPR in a 1-year period of which 9 (69.2%) survived with CPC score 1 or 2. The authors included a comparator group of 22 patients treated with ECPR prior to a system change in the preceding 3 years of which 2 (9.1%) survived. 10
Given the paucity of published data this study aimed to describe the last 11 years of UK provision and outcomes of ECPR.
Methods
This was a retrospective, multi-centre study in the United Kingdom. VA-ECMO centres in the UK were identified through the first UK ECPR Summit in 2023. 11 All centres were asked to submit data on adult patients receiving VA ECMO & ECPR with 6-month survival data between 1st January 2012 and 31st December 2022 from their local database or international registry submissions. As such, no additional ethical approval was necessary. ECPR was defined as VA ECMO cannulation during refractory cardiac arrest with ongoing CPR. 12 Further detailed data on the ECPR cohort was collected for activity between 1st January 2018 and 31st December 2022 including age, sex, aetiology of cardiac arrest, first documented rhythm, return of spontaneous circulation, duration of CPR, time of arrest to ECMO flow, location of cannulation, highest lactate prior to ECMO flow, use of distal perfusion cannula & left ventricular unloading strategies, survival to decannulation and to discharge home. Results were provided by institutions as individual or grouped patient data and therefore statistical analysis was limited to mean and standard deviation only on GraphPad Prism version 10.1.0 for Windows, GraphPad Software, Boston, Massachusetts USA.
Results
The UK VA-ECMO hospitals contributing to this study were Aberdeen Royal Infirmary, Bristol Royal Infirmary, Freeman Hospital, King’s College Hospital, Glenfield Hospital, Golden Jubilee National Hospital, Harefield Hospital, Royal Brompton Hospital, Royal Papworth Hospital, St Bartholomew’s Hospital, Guy’s & St Thomas’ Hospitals, University Hospitals Birmingham and Wythenshawe Hospital.
All centres submitted data for overall number and survival in VA ECMO and ECPR. In the detailed ECPR analysis one centre did not submit data so 43 cases are missing for this analysis (Appendix 1).
VA-ECMO
Over the 11-year period a total of 2117 patients received VA-ECMO in the UK. There were 963 survivors (45.5%) (Figure 1). There was variation in survival outcomes at 6 months over the 11 year period from 12% to 58.6% (Figure 2).
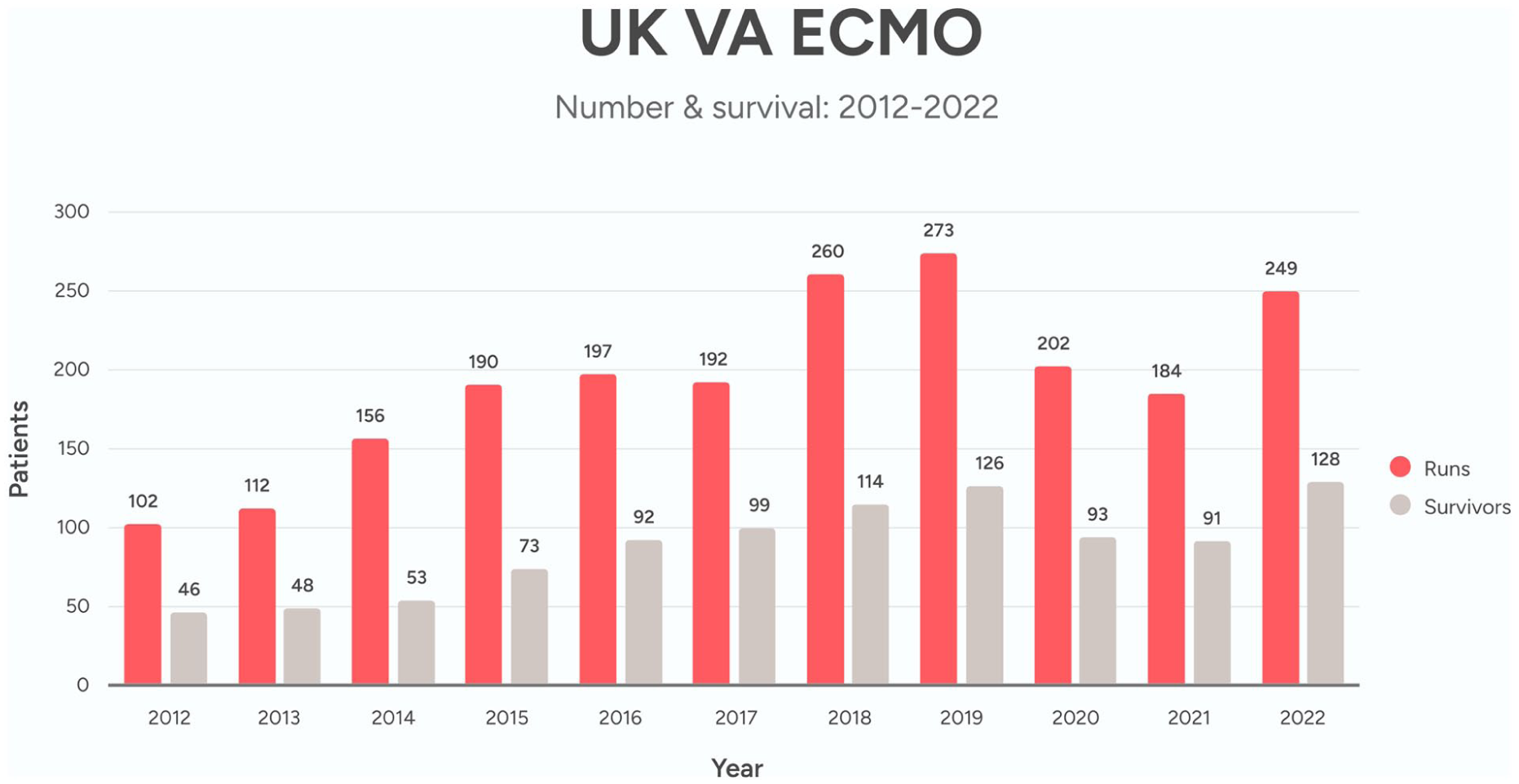
UK VA-ECMO activity & survival 2012–2022.
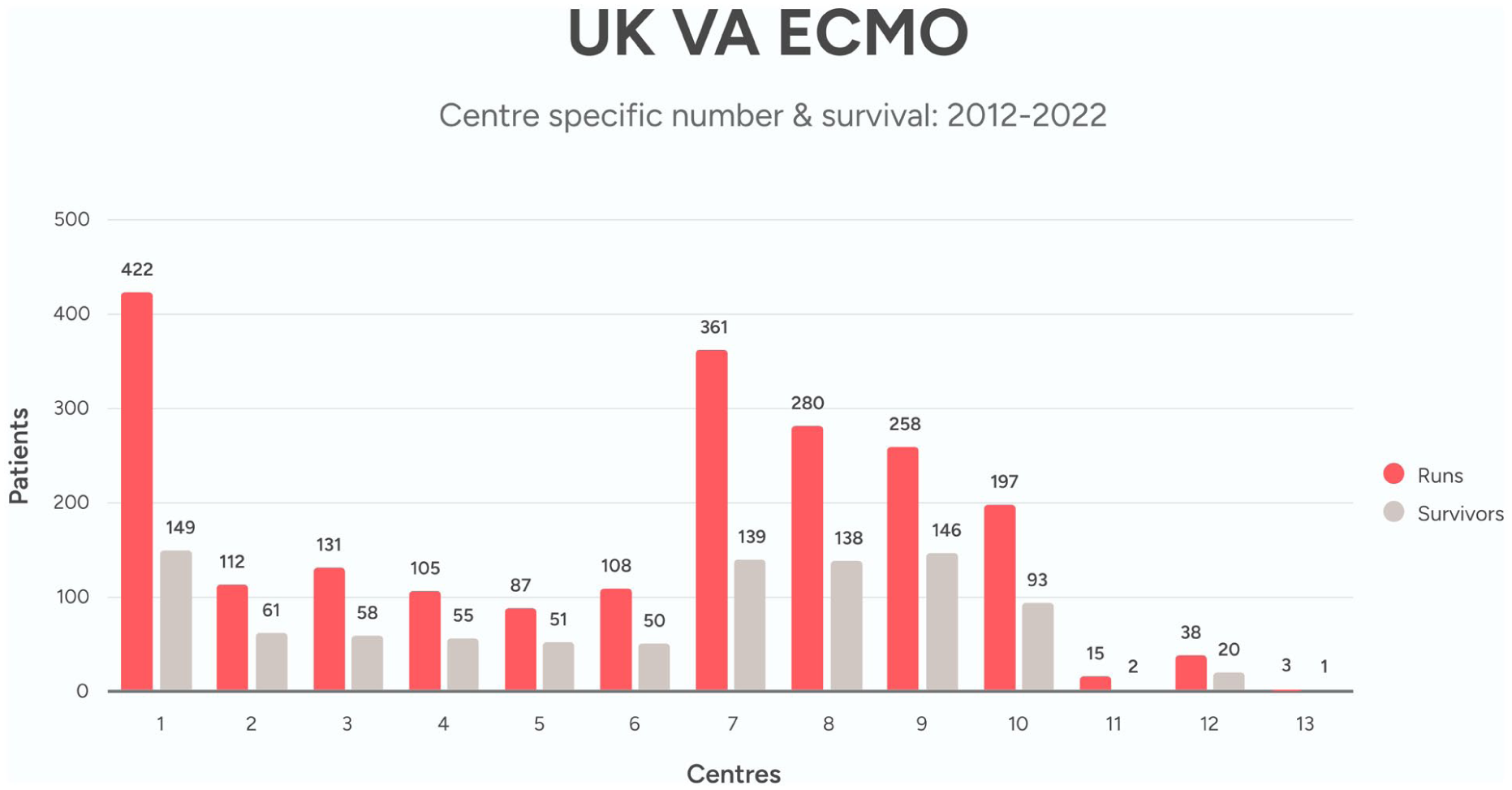
UK VA-ECMO activity & survival 2012–2022 by centre.
ECPR
Of the 2117 patients treated with VA ECMO during this 11-year period, 302 received ECPR. Of these, 92 survived to discharge home (30.5%) (Figure 3). ECPR formed a low proportion of total VA ECMO runs at 14.3% but this varied between centres from 5.4% to 73.3% (Figure 4). Survival for ECPR also varied considerably from 17.5% to 100%.
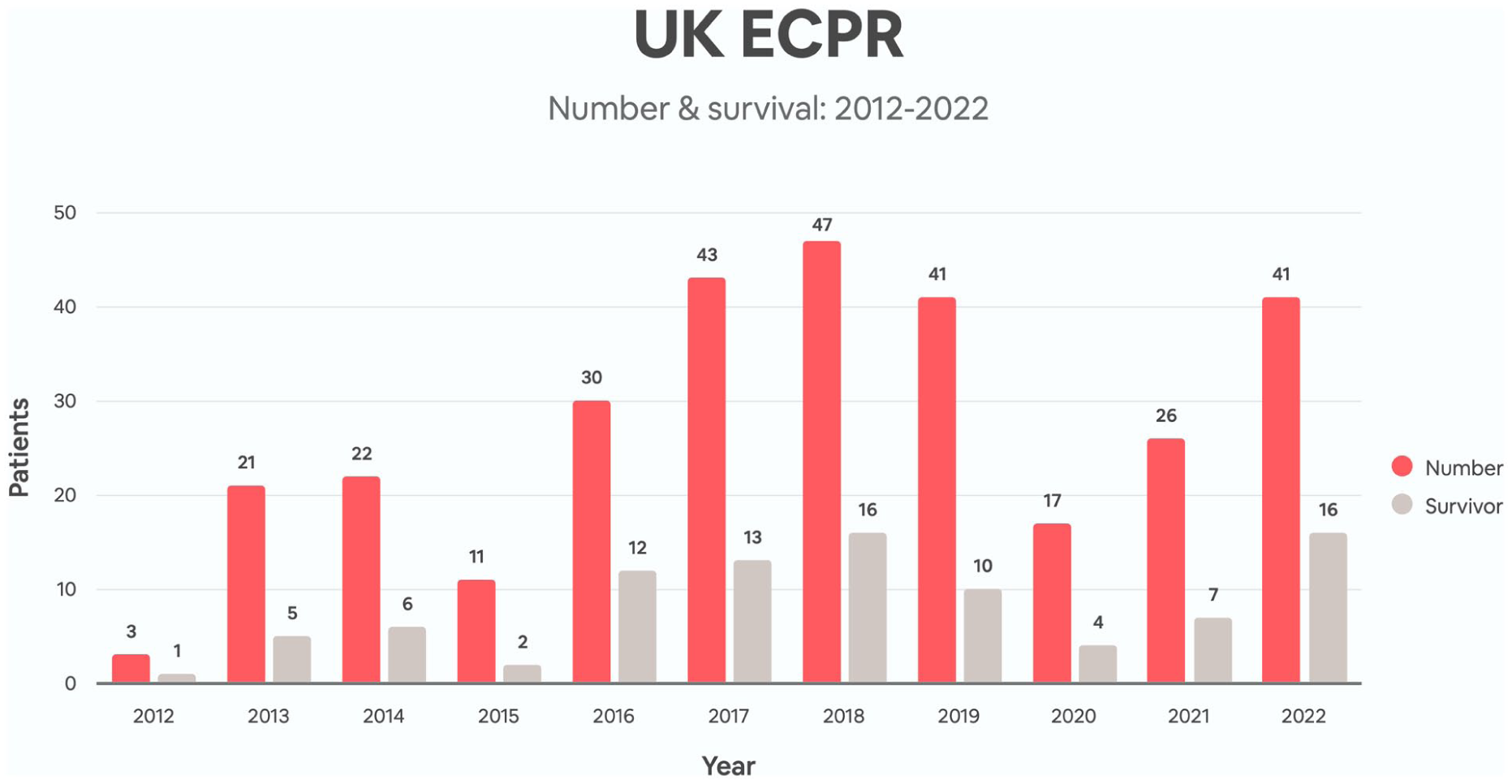
UK ECPR activity & survival 2012–2022.
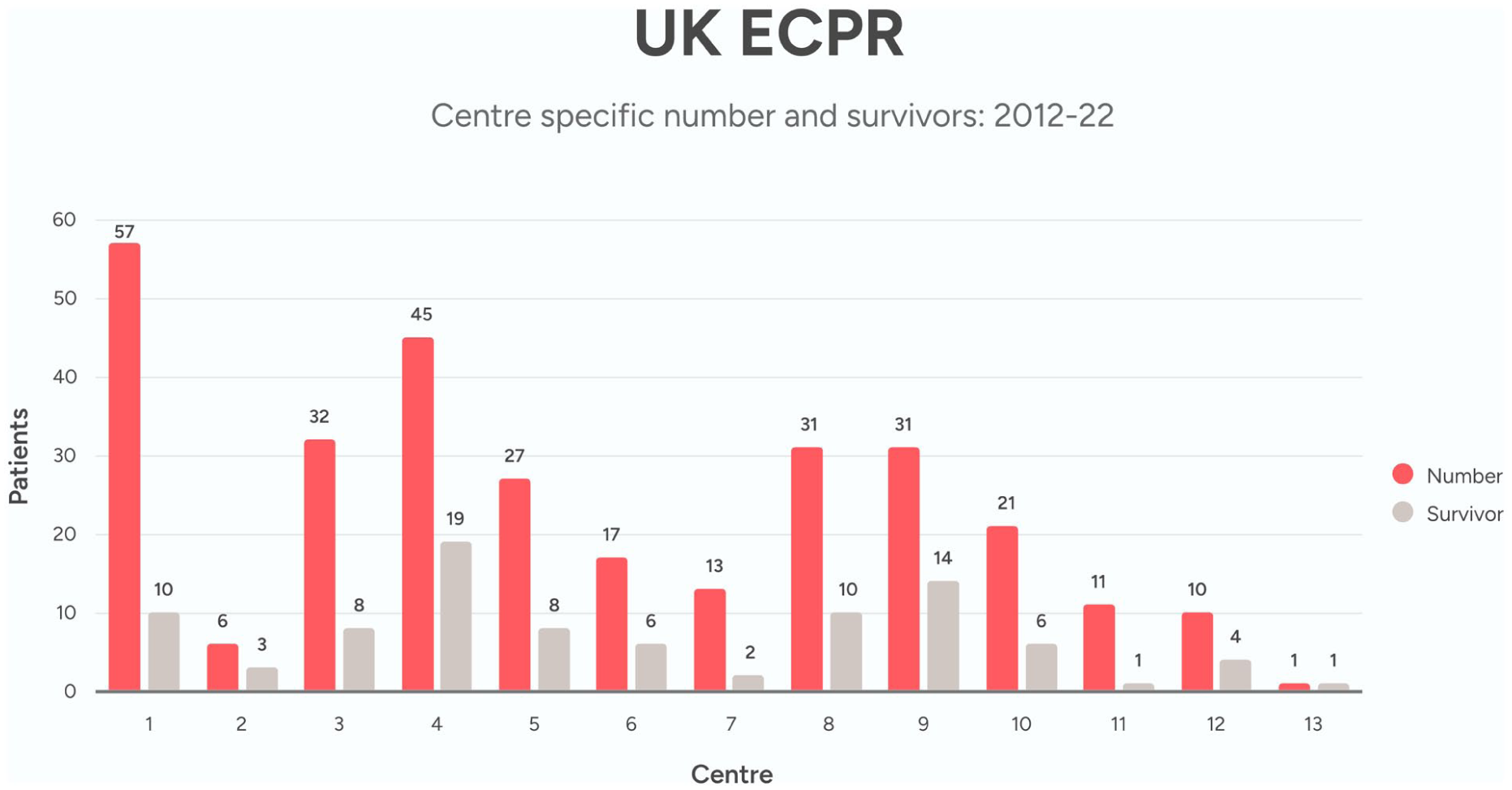
UK ECPR activity & survival 2012–2022 by centre.
ECPR 5 year detailed data
Between 1st January 2018 to 31st December 2022 a total of 172 patients received ECPR in the UK. Detailed data were available for 129 cases (75%) (Table 1).
UK ECPR Cases 2018–2022 (129 of 172 total cases).
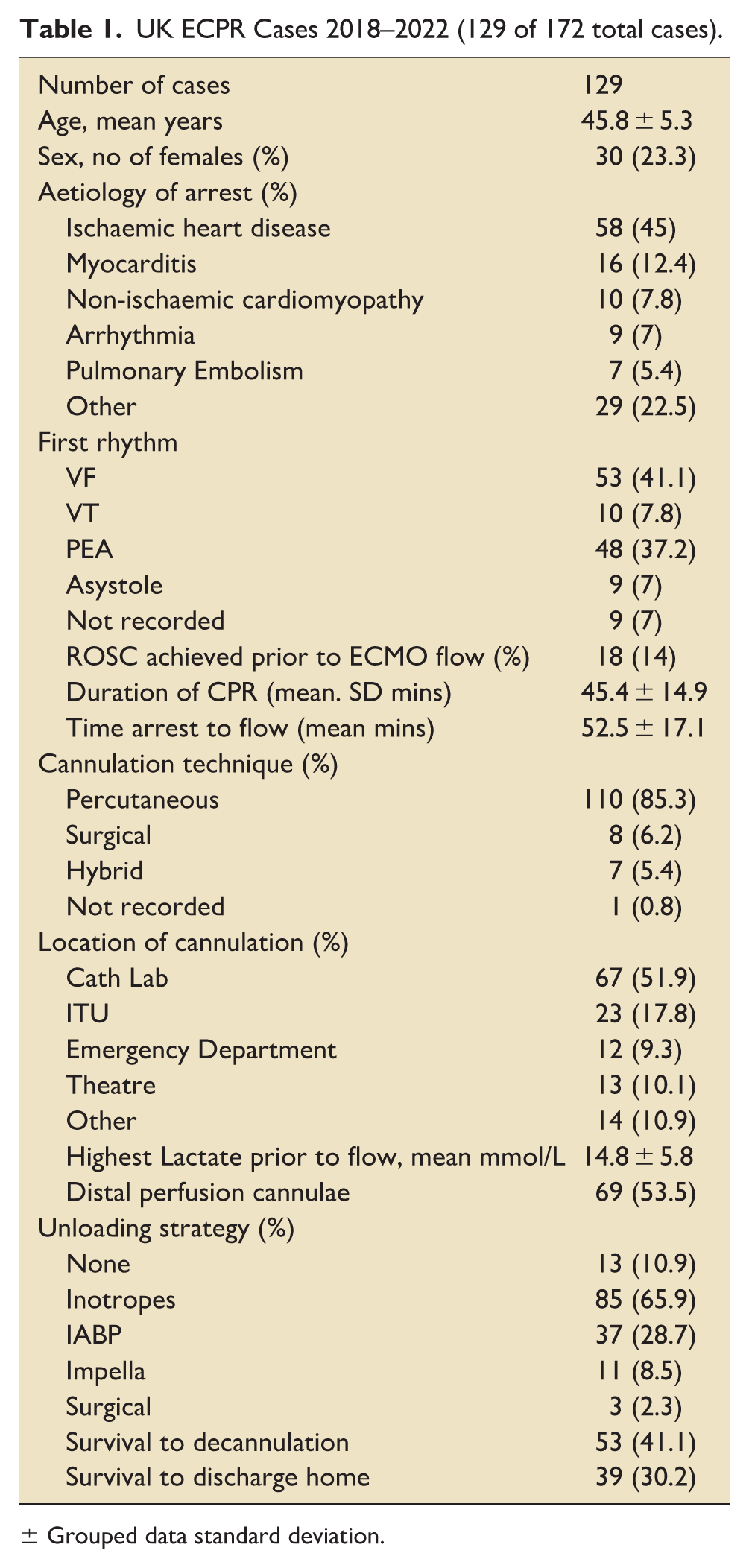
± Grouped data standard deviation.
Population
The mean age was 46 ± 5 years and 77% of cases were male. The principal cause of arrest was ischaemic heart disease in 58 (45%) of cases and shockable rhythms occurred as the initial rhythm in 63 (48.9%) cases. Mean duration of CPR was 45.4 ± 14.9 min with 18 (14%) cases achieving return of transient or sustained spontaneous circulation at any point prior to ECMO flow. The mean time from start of arrest to initiation of ECMO flow was 52.5 ± 17.1 min.
Technique
The primary technique of cannulation was percutaneous in 110 (85.3%) of cases, with 67 (51.9%) being performed in the cardiac catheter lab. Distal limb perfusion cannulae were sited in 59 (53.5%) of cases and 51 (39.5%) required a second mechanical circulatory support device for left ventricular unloading.
Outcomes
Outcomes in this detailed 5-year analysis matched the overall 11 year period in the UK with 39 (30.2%) surviving to discharge home.
Discussion
This is the first study to report the use of VA ECMO and ECPR across the UK.
Overall, 2117 patients were treated with VA ECMO over the 11-year study period and that the survival of this cohort was in line with that reported in an internationally registry (UK 45.5% vs Extracorporeal Life Support Organisation (ELSO) World Registry 47%). 4
ECPR patients reported in this UK cohort had a 30.5% survival which also corresponds to internationally reported ELSO registry survival rates. This was an unwell cohort with only 14% achieving return of spontaneous circulation prior to ECMO flow and the average lactate was 14.8 ± 5.8 mmol/L. In patients with refractory cardiac arrest ECMO is typically instituted once cannulation has commenced, despite return of circulation, owing to the high risk of recurrent arrest or profound cardiogenic shock. Patients receiving ECPR tended to be young, presenting with VF or VT with ischaemic heart disease as the leading cause of arrest. The proportion of ischaemic aetiology was comparable to the studies that included PEA 6 but much lower than those only including VF/VT5,7 only trials. Most cannulations were percutaneous and achieved within 1 h of cardiac arrest. The centres listed are not geographically well spread across the UK with Wales and Northern Ireland notably having no centre performing ECPR or indeed ECMO. Though the cause of death was not available across all institutions, international experience most often cites refractory shock and neurological causes. 13
There was considerable variation in the number of patients treated with ECPR between the centres ranging from 1 to 57 in the 11-year study period. The assumption is that this is likely multifactorial in origin including; fluctuating critical care capacity; experience and availability of cannulators; differing inclusion and exclusion criteria; differing standard operating procedures in support delivery, weaning and neuroprognostication; geographical and population variation.
Though outcomes in the UK matched that of registry data, this should be interpreted cautiously due to the small number of highly selected patients. The outcomes also include early-stage data by higher volume centres prior to system and service refinements had been undertaken to improve outcomes. 14 Lower volume ECPR centres were able to produce similar proportions of survivors, a feature not seen in the INCEPTION trial. 7
The UK supported considerably fewer patients with ECPR than comparable nations. 4 The UK has a population of nearly 67 million and is the 6th largest global economy by gross domestic product (GDP). Around 80,000 OHCA are reported per year by the UK ambulance services and survival is persistently low at 8.6%. 2 However, over the 11-year period only 302 patients were treated with ECPR in the UK, compared to for example 124 patients randomised to an ECPR arm of a study in a single city of 1.3 million people over 7 years. 6 The primary reason for this is that ECPR is not routinely available across the UK. Notably, there is not yet an ECPR system that has demonstrated the capability of equitably servicing any health system or nation. 7
There were significant limitations to the study, most importantly a quarter of the data collection was incomplete for the 5-year detailed analysis. Data was difficult to collect in some centres due to a lack of historical records or excessive time needed to extract detailed information. Data was also submitted by some centres as grouped results over a period of year to maintain anonymity of patients. This restricted the ability to perform any advanced statistical analysis of the data. Furthermore, there were inadequate details available to make any meaningful assessment of the more granular elements of the demographics, physiology and clinical progress.
This study is the first to quantify the use of VA ECMO and ECPR in the UK and was the product of collaboration between every centre offering ECMO in the nation in 2023. This gives a useful overview of the current volume of work and the clinical outcomes. Data was collected and presented as part of the UK’s first ECPR summit in June 2023 driving national conversation on the subject and an agreement for regular meetings and formalised collaboration.
Conclusion
Cardiac arrest remains associated with poor outcomes and ECPR offers a potential intervention to improve survival considerably in carefully selected patients. Although ECPR is being delivered in the UK, it is currently at low volumes and with significant regional disparities. A nationally standardised registry is needed to understand practice, establish benchmarks, drive further research and foster collaboration. This will help share best practices, develop standardised criteria, regional systems of care and explore innovative funding strategies to support broader access and implementation.
Footnotes
Appendix
Acknowledgements
Georg Auzinger, Eilidh Beaton, Matthew Charlton, Jo-anne Fowles, Elton Gelandt, Stefan Gurney, Chris Harvey, Nick Haslan, Phil Leadbeater, Dominic Lowcock, J McNicol, Hayley Robertson, Robert Loveridge, Charlotte Poulton, Sachin Shah, Philippe Simard, Andrew Sinclair, Adrian Wagstaff, Andrew Hadley-Brown, Dinesh Yoganantham.
Abbreviations
CPR cardiopulmonary circulation, CPC clinical performance category score, ECMO extracorporeal membrane oxygenation, ECPR extracorporeal membrane oxygenation resuscitation, ELSO Extracorporeal Life Support Organisation, NHS National Health System, UK United Kingdom, VA veno-arterial, VF ventricular fibrillation, VT ventricular tachycardia.
ORCID iDs
Ethical considerations
All centres were asked to submit data from their current local database or international registry submissions. As such, no additional ethical approval was necessary.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Waqas Akhtar has received educational grants from Abiomed, Abbott, Chalice, Medtronic, Takeda and Resuscitec and speaker honoraria from Abiomed. Alex Rosenberg received educational grants and speaker honoraria from Getinge, Resusciteic, Abiomed. Eftychia Galiatsou and Sofia Pinto received speaker honoraria from Abiomed. Alain Vuylsteke received consultancy fees from Inspira Technologies. Brijesh Patel received speaker honoraria from Johnsons & Johnson, Medtronic and participates on a Novartis board.
PPI
Patients were not involved in the design and conduct of this research.