
Abstract
Severe cases of hydrocarbon aspiration requiring Extracorporeal Membrane Oxygenation (ECMO) are rarely reported in pediatrics, and 90% of hospitalized patients have a relatively benign clinical course. We describe a 14 month-old female with accidental hydrocarbon ingestion and aspiration due to organic makeup brush cleaner that suffered severe ARDS and multiorgan failure, successfully managed with ECMO and surfactant. She was decannulated after a total of 72 hours on ECMO, extubated on hospital day 15 (HD 15), and discharged home in her normal state of health after one month in the hospital. ECMO and adjunctive therapies such as surfactant may be helpful in the management of severe hydrocarbon pneumonitis and there are limited reports of ECMO as a supportive method for these pediatric patients.
Keywords
Case report
A previously healthy 14 month-old female presented with altered mental status, cough, and cyanosis. She was found with an open bottle of “organic makeup brush cleaner” (Figure 1) with cleaner covering her lips, face, and hands. She immediately started coughing and became somnolent with peri-oral cyanosis. Her father then induced vomiting by digital stimulation and her mental status worsened with intermittent apnea. This prompted transport to the ED where she was intubated for lethargy and acute respiratory failure (Figure 2(a)). The makeup brush cleaner contained “>30 aliphatic hydrocarbons” with only 1 ingredient specifically detailed - 2,2,4,4,6,8,8-heptamethylnonane, confirmed later by GC/MS as the sole ingredient. Bottle of the makeup brush cleaner. Progression of chest radiographs through intubation and ECMO cannulation.
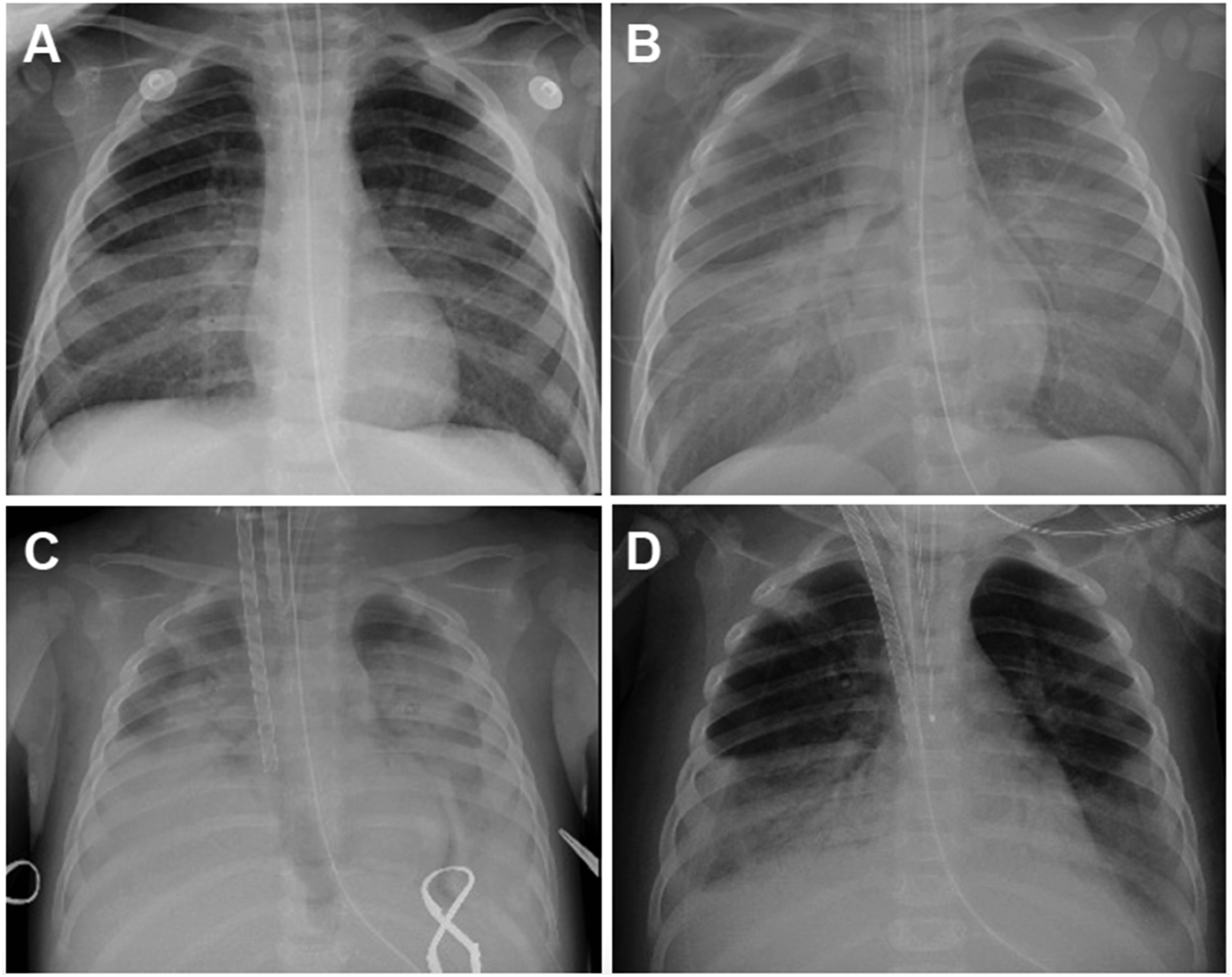
In the pediatric intensive care unit she rapidly developed severe ARDS with an oxygenation index (OI) of 27. Despite inhaled nitric oxide (40 ppm), proning, and paralysis, her OI increased to 56 with worsening bilateral opacities (Figure 2(b)). She developed shock refractory to vasopressors and high-dose steroids.
Her hospital course was further complicated by a fulminant systemic inflammatory response, with large bilateral pleural effusions, ascites, and abdominal compartment syndrome. Her fluid overload required hemofiltration, diuretics, and peritoneal drain placement. An echocardiogram demonstrated reduced biventricular systolic function and left ventricular ejection fraction of 18%. Due to refractory shock and hypoxia, she was cannulated onto veno-arterial (VA) ECMO on HD 1 (Figure 2(c)) requiring maximum support with a cardiac index (CI) of 2.5 L/min/m2. On HD 2, she received a single dose of surfactant (Curosurf) 2.5 mL/kg by endotracheal lavage with an immediate decrease in ECMO support need from a CI of 2.5 to 2.0 L/min/m2 and a 10% reduction in ECMO FiO2 need within 2 hours. The peak inspiratory pressure (PIP) was also able to be weaned within an hour of surfactant administration to maintain the same tidal volumes on the ventilator. She was successfully decannulated after 72 hours of ECMO (Figure 2(d)).
Her hospital course was subsequently complicated by spontaneous pneumothorax requiring tube thoracostomy. A chest CT demonstrated extensive areas of lung necrosis (Figure 3). She was successfully extubated on HD 15, weaned to room air on HD 25, and discharged home on HD 35 without respiratory support and in her usual state of health. Chest CT on hospital day 11 demonstrating bilateral lower lobe lung necrosis.
Discussion
Hydrocarbons are a common and potentially lethal component in numerous household items. 1 They are primarily manufactured for use as a fuel source, however also have widespread use in paint thinners and other petroleum distillates such as furniture polishes, solvents, and cleaners. 2 The clinical course of accidental hydrocarbon aspiration or inhalation is usually mild with coughing, vomiting, and central nervous system depression as common presenting symptoms. 2 Severe cases of a rapid chemical pneumonitis, ARDS, and multiorgan failure are more classically described with exposure to kerosene and paint thinner exposures. There are no known demographics or clinical factors that are significant prognostic indicators of disease severity. 2 The severity of the clinical course in this case is unique due to what is generally thought of as a more innocuous household source - an organic makeup brush cleaner.
After entering the lung, hydrocarbons destroy surfactant and directly damage lung parenchyma, leading to a progressive chemical pneumonitis, necrotizing bronchopneumonia, and refractory hypoxia. 3 Studies have documented detrimental long term pulmonary effects of hydrocarbon pneumonitis which lead to chronic lung disease in adulthood. 4 Cardiac dysrhythmias are also reported, 2 particularly with aromatic or halogenated hydrocarbons causing sensitization of the myocardium to catecholamines.
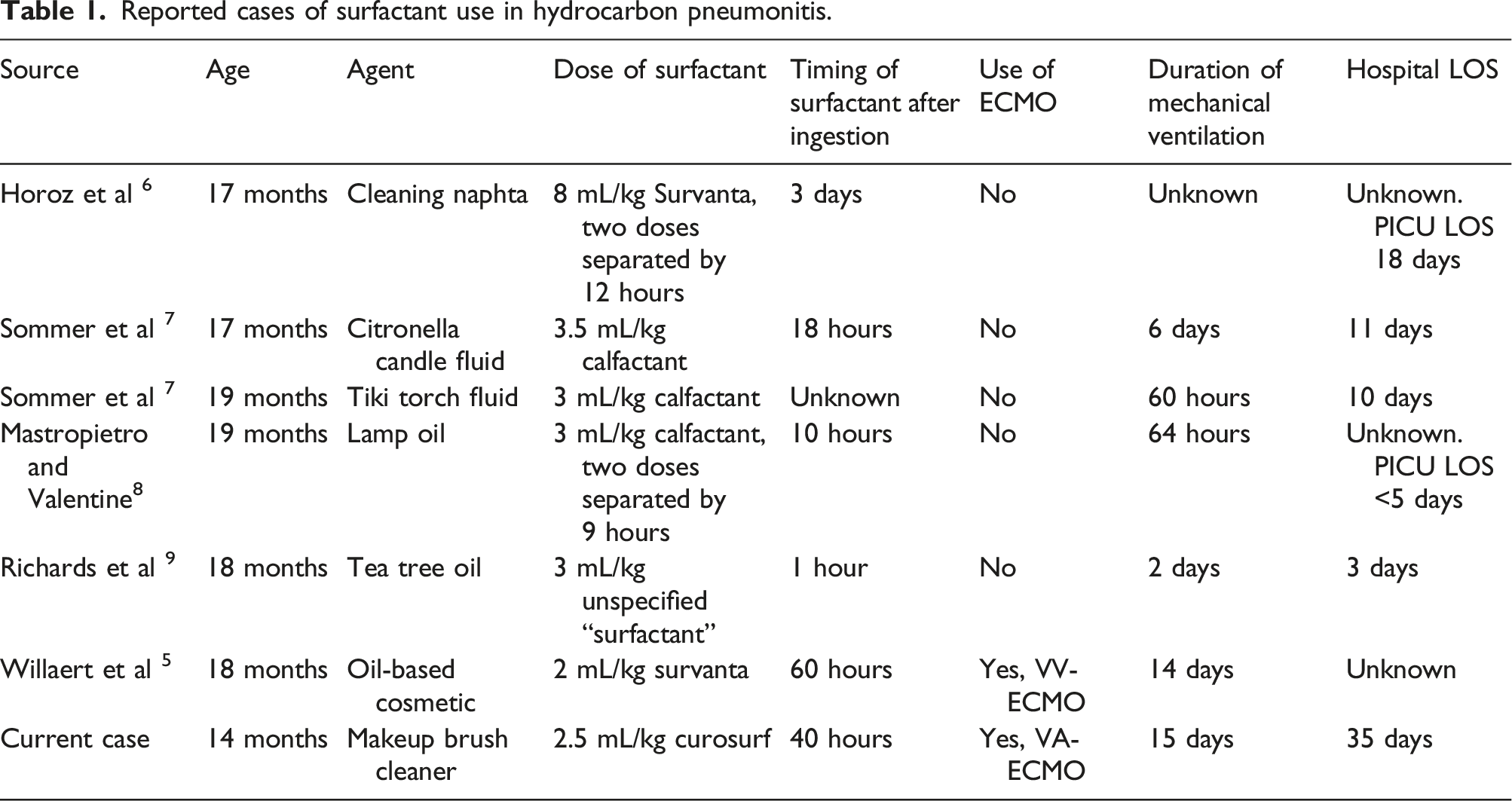
Reported cases of surfactant use in hydrocarbon pneumonitis.
Conclusion
The use of ECMO remains a rare, yet promising therapy in recovery from severe ARDS due to hydrocarbon aspiration. Surfactant as an adjunctive therapy should be considered early in severe intoxications and it may decrease the duration of ECMO, although further studies are needed. This case highlights the development of severe ARDS and multiorgan failure following an ingestion of an aliphatic hydrocarbon-based makeup brush cleaner, requiring the shortest reported ECMO course possibly facilitated by the addition of surfactant.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Written authorization was obtained by the patient’s legal guardians for the publication of this case report. There are no financial or personal conflicts of interest to report.