
Abstract
A technique called arch-clamping was used at our institute to ensure perfusion of the lower body and brain during total arch replacement with frozen elephant trunk (TAR and FET). The aortic arch clamp is inserted between the left common carotid artery and the left subclavian artery after inserting the stented elephant trunk into the true lumen of the descending aorta during the procedure, and then clamps the aorta and graft together as the distal anastomotic edge of the aorta. After the arch clamp was in place, lower body perfusion was resumed through the femoral artery was resumed and time to circulatory arrest was reduced to approximately 4 min. Cardiopulmonary bypass (CPB) flow was gradually restored to full rate. Thereafter, the left carotid artery anastomosis was completed and rewarming began. Finally, during the rewarming period, other branches of the aortic arch and ascending aorta were reconstructed. In this paper, we describe the perfusion management strategy, discuss intraoperative monitoring parameters, and examine the feasibility of the technique from a perfusion perspective.
Keywords
Introduction
Compared to other types of cardiac surgery, TAR with FET is a complex procedure associated with higher mortality and morbidity rates. 1 In an open anastomosis of the distal arch of the aorta, specific perfusion strategies are employed to prevent hypoxic-ischemic damage to the brain and injury to the end organs of the lower body.2,3 In our institute, perfusion for TAR has evolved from straight deep hypothermic circulatory arrest (DHCA) to moderate hypothermic circulatory arrest (MHCA) plus antegrade cerebral perfusion (ACP) at a nasal temperature of 25°C. 4 Recently, arch-clamping technique has been applied to TAR and FET in some cases OF acute type A aortic dissection (ATAAD) at our institute. The aortic arch clamp was inserted between the innominate artery and the left common carotid artery and then clamped the aorta and graft together as the proximal suture edge. Once the arch clamps was fixed, perfusion of the lower body through the femoral artery was resumed and the CA time reduced to approximately 4 min, and ACP is provided through cannulas of the right axillary artery during the anastomosis of the distal aortic arch.
The perfusion management and the monitoring strategy were adapted to the requirements of the new technology. The purpose of this study was to describe the technique’s perfusion management strategy and examine the intraoperative monitoring parameters from a perfusion perspective and provide early outcome from thirty patients.
Method
Patients
From December 2020 to June 2021, sixty consecutive patients diagnosed with ATAAD underwent TAR and FET at Anzhen Hospital. Thirty patients using arch-clamping technique with modified perfusion management, other thirty patients underwent conventional TAR and FET surgery. The institutional review board approved the retrospective observational study and waived the informed consent.
Procedure
The surgical technique was described above. The prosthesis and material used in the procedure were as follows: Tetrafukat graft (Terumo; Vascutek Limited). A compressed stent-graft (Cronus; Microport Medical Co, Ltd, Shanghai, China) consists of a 10-mm stent-free vascular graft at the proximal end and a 10 cm self-expanding metallic stent-graft distally with variable diameters (24–30 mm) (Figure 1).
5
New stent artificial graft Cronus® of Shanghai Microport company.
The CPB circuit consisted of a hollow fiber oxygenator (Jostra Quadrox; Maquet Cardiopulmonary AG 71000, Hirrlingen, Germany), a heart-lung machine (Stockert S5; Sorin Group Deutschland GmbH, Munich, Germany), an uncoated polyvinyl chloride circuit (Tianjin Plastics Research Institute Co., Ltd., Tianjin, China) and an arterial filter (Fly Medical Healthcare Co., Ltd., Ningbo, China). The arterial line was bifurcated by a Y-connector to femoral arterial and right axillary cannula. The size of the direct femoral artery cannula was selected according to the size of the artery (Optisite Arterial Cannula, MEDOS BIOTECHNOLOGY, BMAA324, USA). The right axillary artery cannula was performed using a 20F cannula (Optisite Arterial Cannula, MEDOS BIOTECHNOLOGY, BMAA324, USA).
During the operation, the dual arterial line was used with a single pump head, after systemic heparinization, CPB was applied from the right atrium to both femoral and axillary arteries, and the left ventricular vent was placed through the right superior pulmonary vein. Myocardial protection was provided with histidine tryptophan ketoglutarate (HTK) solution and topical cooling. An aortic root surgery was performed during the cool-down period. After the nasopharyngeal temperature reached 28°C, the femoral line was clamped and lower body CA was initiated, the unilateral ACP was administered via the right axillary line at a rate of 5–10 ml/kg/min. Regional cerebral oxygenation saturation (rScO2) was monitored by near-infrared reflectance spectroscopy (NIRS; Suzhou Engin Biomedical Electronics, Jiangsu, China). ACP flow was correspondingly increased when the rScO2 drop exceeded 15% of baseline. After the ACP was established, the distal arch of the aorta was transected and the stented elephant trunk inserted into the true lumen of the descending aorta (Figure 2). Then, the stented suture edge was gently pulled out of the proximal end of the stent and the aorta was clamped together between the left common carotid artery and the left subclavian artery at the Z2 position of the aorta according to the method described by Mitchell et al., proposed zoning of the aortic arch(Figure 3).
6
Immediately after the arch clamps was fixed, the femoral arterial line was de-clamped, perfusion of the lower body was then resumed through the right femoral artery cannula along with ACP through the right axillary artery cannula from the single central perfusion. During anastomosis between the FET collar and proximal descending aorta, the CPB flow was restarted and gradually increased to total flow. The lower body CA lasted for approximately 4 min. Total CPB blood flow was adjusted to ensure rScO2 was greater than 85% of basal rScO2 and axillary flow of 5–10 mL/kg/min. After distal anastomosis, the atraumatic aortic clamps was withdrawn and the graft and its branches were clamped. The left common carotid artery was anastomosed first, after which the perfusion through both carotid arteries could be obtained, rewarming for the patient was started and total CPB flow was increased accordingly to 2.4 L/m2/min. After anastomosis of the proximal aorta was completed, the aortic clamp was removed, the left subclavian and innominate arteries were subsequently reconstructed (Figure 4). The stented elephant trunk inserted into the true lumen of the descending aorta. The new stent graft and the aorta was clamped together between the left common carotid artery and the left subclavian artery, circulation was then resumed, then femoral arterial line was de-clamped, and lower body and cerebral perfusion was provided through the femoral and right axillary lines. Surgical techniques. (A)Circulatory arrest, the open stented graft was directly deployed into the true lumen of the descending aorta. (B) The stent-free sewing edge was pulled out from the proximal end of the stent. (C) The stent and the aorta were clamped together between left common carotid artery and left subclavian artery at the aortic Z2 position. Then femoral arterial line was de-clamped, and cerebral and lower body perfusion were provided through right axillary and femoral lines respectively, the circulatory arrest was maintained for approximately 4 min. (D) Anastomosis the distal end of the 4-branched prosthetic graft to the FET collar and proximal descending aorta.
In the conventional method, arterial cannulation was achieved using the right axillary and femoral arteries of the bifurcated arterial line with a Y-connector from one central perfusion. Systemic CPB was discontinued at 25°C of target nasopharyngeal temperature. When the lower body CA needed to start, the femoral line was clamped with the decrease of perfusion rate. After clamping the proximal innominate artery, antegrade selective cerebral perfusion (ASCP) started at a rate of 5 ml/kg per min through the right axillary artery cannula. The distal aorta incorporating the stented elephant trunk was firmly attached to the distal end of the four-branched prosthetic graft using the “open” aortic method. After distal anastomosis, the graft and its branches were clamped, perfusion of the lower body was then resumed through the right femoral artery cannula along with ASCP through the right axillary artery cannula from the single central perfusion. The CPB flow was restarted and gradually increased to one-half of total flow. The left common carotid artery was anastomosed first, after which the perfusion through both carotid arteries could be obtained. Then, rewarming for the patient was started with the CPB flow gradually increased to total flow. The anastomosis of the left subclavian artery (LSCA) and the innominate artery completed the surgery.
Data collection and statistical analysis
Patients’ outcome and perfusion-related variables were retrospectively collected. Statistical analysis was performed with IBM SPSS 25.0. Categorical variables were presented as percentage and frequency. Continuous variables were presented as median (25th-75th percentile) or mean (±standard deviation) as appropriate.
Results
Flow distribution between axillary and femoral artery lines at three time points(mL/min).
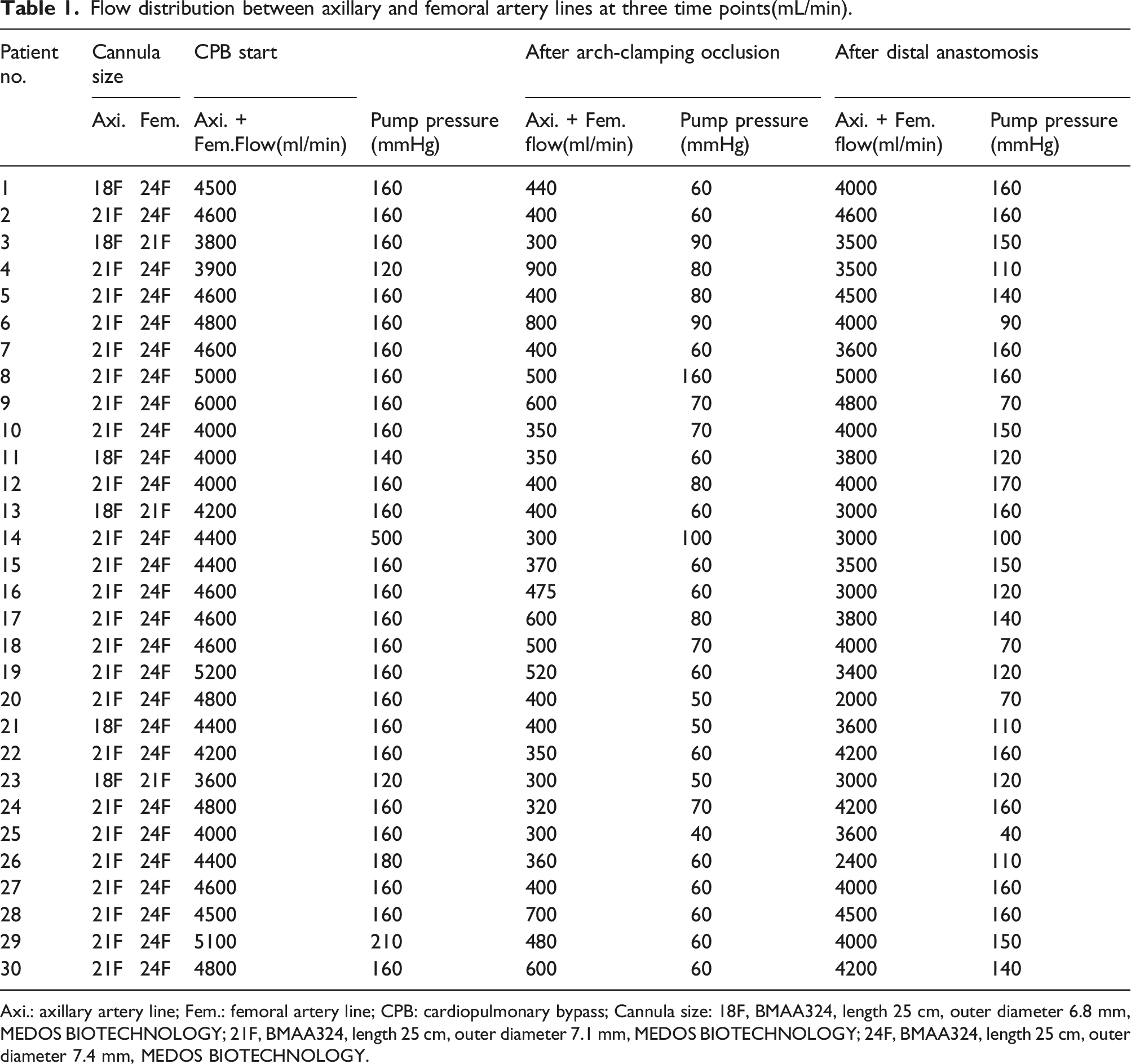
Axi.: axillary artery line; Fem.: femoral artery line; CPB: cardiopulmonary bypass; Cannula size: 18F, BMAA324, length 25 cm, outer diameter 6.8 mm, MEDOS BIOTECHNOLOGY; 21F, BMAA324, length 25 cm, outer diameter 7.1 mm, MEDOS BIOTECHNOLOGY; 24F, BMAA324, length 25 cm, outer diameter 7.4 mm, MEDOS BIOTECHNOLOGY.
Perfusion variables.
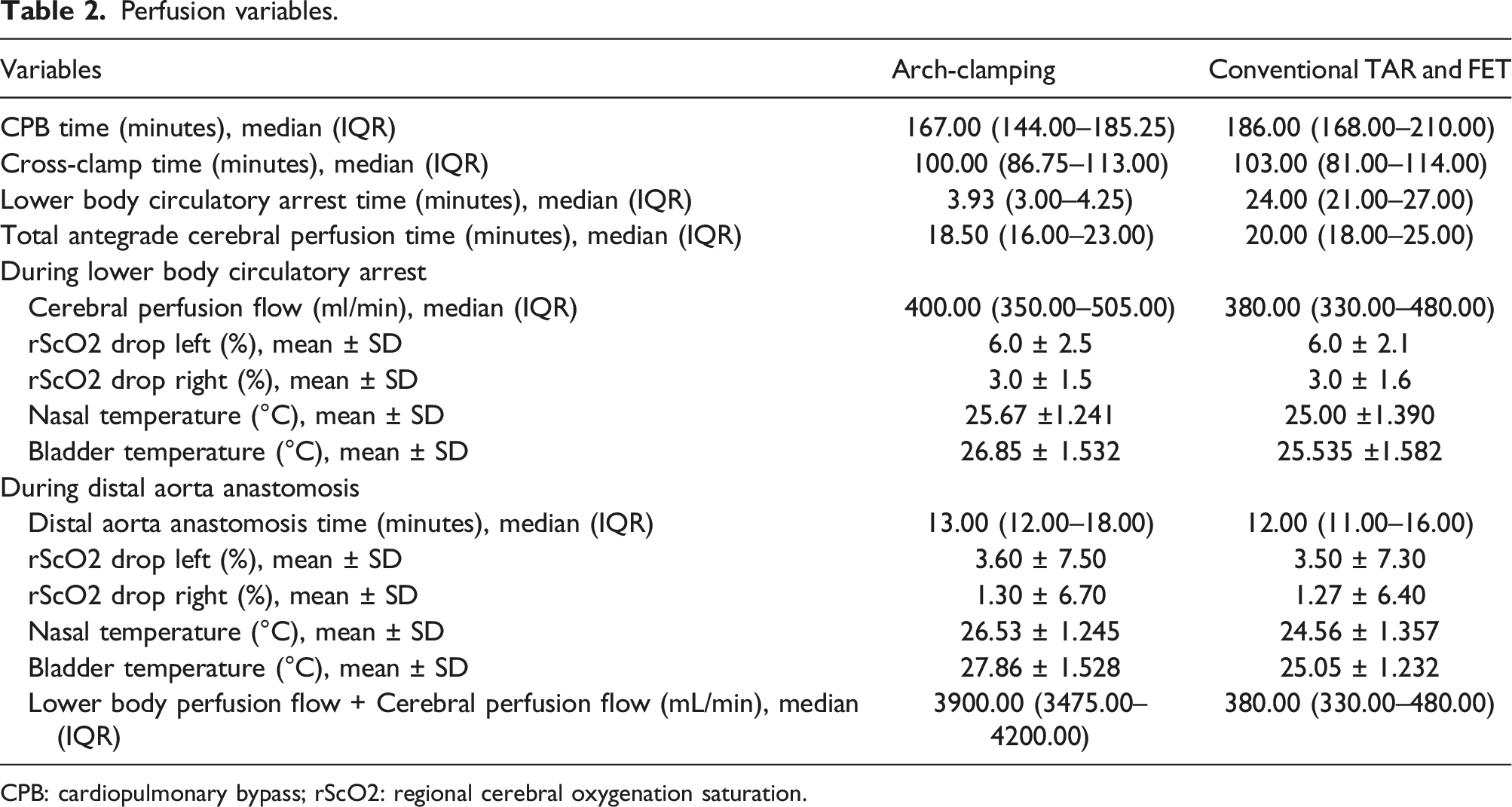
CPB: cardiopulmonary bypass; rScO2: regional cerebral oxygenation saturation.
Postoperative outcomes.
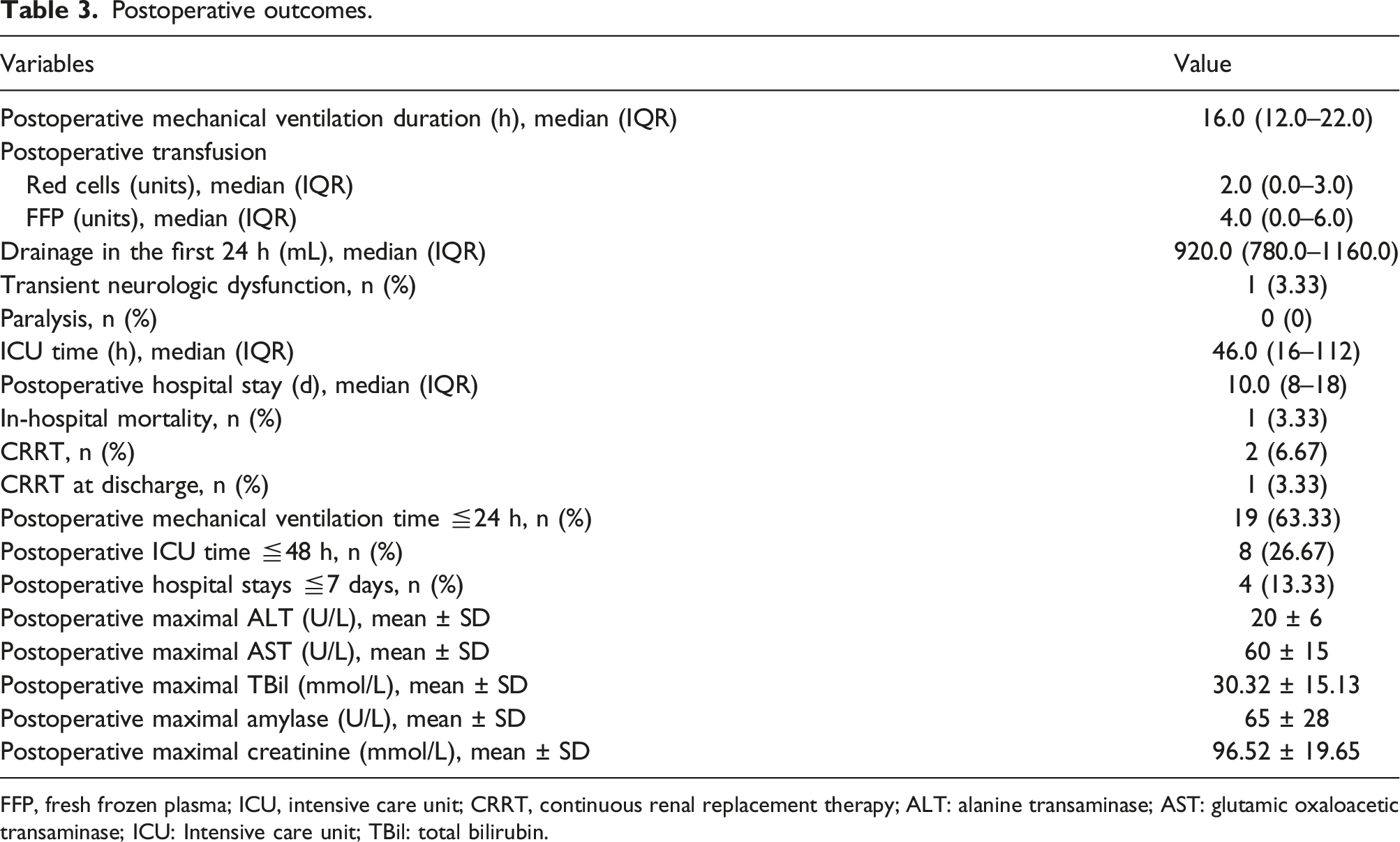
FFP, fresh frozen plasma; ICU, intensive care unit; CRRT, continuous renal replacement therapy; ALT: alanine transaminase; AST: glutamic oxaloacetic transaminase; ICU: Intensive care unit; TBil: total bilirubin.
Discussion
The present study provided detailed modified perfusion management of the aortic arch-clamping technique in FET-TAR. A recent study of 1708 cases of aortic arch surgery found that the risk of permanent neurological dysfunction and mortality increased when the unilateral antegrade cerebral perfusion time was more than 38 min and the temperature was less than about 24°C. 7 In addition, mortality and stroke are associated with a variety of factors, such as: Age, New York Heart Association score, coma, malperfusion syndrome, coronary artery bypass graft surgery and other factors identified in previous studies.8,9 The arch-clamping technique only changed the nature of extracorporeal circulation, and it is difficult to reverse the outcome in high-risk patients.
As perfusion flow of right axillary artery and right femoral artery lines is driven from a single roller pump, flow distribution depends on vascular resistance difference between the two perfusion sites and patient-specific, which is difficult to predict solely based on arterial cannula sizes and the ideal of lower body perfusion flow is unknown. In this series, were maintained above 50% of the target total flow (1800 ml/min, at 28°C), by postoperative biochemical results demonstrated that yielded satisfactory end-organ protection effect. To achieve appropriate flow distribution we recommend a thinner cannula for right axillary artery than right femoral artery cannula. If necessary, Hoffman clamp could be used to alter resistance difference between the two lines.
The arch-clamping technique clamps the aorta and graft together, effectively preventing the backflow from false lumen thought the femoral perfusion, and does not interfere with distal aortic arch anastomosis, not reduces the lower body flow and ensures a clear surgical field. That is the reason why target temperature is set at 28°C. If rScO2 drop >15% or ACP <5 ml/min falls, the Hoffman clamp on the femoral artery line can be used to increase axillary artery perfusion.
The major limitation of the study was the insufficient amount of patient. Further study is needed to demonstrate the clinical effect of the arch-clamping technique and modified perfusion management strategy. Second, the lack of randomized controlled trial design was another major limitation. Prospective controlled study is required to compare the arch-clamping technique with conventional method. Third, it was a single-center study and the experience might not be generalizable to other centers.
Conclusion
During anastomosis between the FET collar and proximal descending aorta in FET-TAR, the arch-clamping technique and modified perfusion management strategy could provide sufficient cerebral and lower body perfusion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Major Science and Technology Projects from Beijing Municipal Science and Technology Commission (No. Z191100006619093 and Z191100006619094) and National Science Foundation of China (No. 81970393).