
Abstract
Objective
To investigate the use of the aortic balloon occlusion technique to assist total aortic arch replacement (TAR) with frozen elephant trunk (FET) to shorten the lower body circulatory arrest (CA) time and raise the nadir temperature during cardiopulmonary bypass.
Methods
This retrospective study reviewed consecutive patients that underwent aortic balloon occlusion to assist TAR with FET and patients that received conventional TAR with FET procedures. Preoperative characteristics, perioperative characteristics and postoperative outcomes were compared between the two groups.
Results
The study included130 patients treated with aortic balloon occlusion and 230 patients treated with conventional TAR with FET. The 30-day mortality rate was similar between the aortic balloon occlusion and conventional groups (4.62% versus 7.83%, respectively). Multivariate analysis showed that aortic balloon occlusion reduced the incidence of acute kidney injury, hepatic injury and red blood cell transfusion. The application of aortic balloon occlusion reduced the mean ± SD CA time from 17.24 ± 4.36 min to 6.33 ± 5.74 min, with the target nadir nasal temperature being increased from 25°C to 28°C.
Conclusion
The aortic balloon occlusion technique achieved significant improvements in reducing complications, but this did not translate into lower 30-day mortality.
Keywords
Introduction
Total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique is the standard surgical technique used for treating complex aortic diseases in many aortic and vascular surgery centres.1–10 This surgical procedure is associated with more risks as the lower body undergoes circulatory arrest (CA) for 20–40 minutes,1,3,11,12 which requires complex cardiopulmonary bypass (CPB) and anaesthesia management in addition to the surgeon’s technique. The procedures to assist this complicated operation include: (i) setting a suitable deep-to-moderate hypothermic state to adapt the required period of CA time; (ii) exerting a moderate perfusion pressure/rate and perfusion timing that provide sufficient protection for the end organs, especially the brain and the kidneys; (iii) assuring the maintenance of body circulation before and after CPB with drug, fluid, transfusion and/or other measures; (iv) protecting the organs from severe damage caused by the operation and CPB. All these procedures aim to ensure the safe performance of the operation and successful postoperative management in order to achieve satisfactory outcomes.11–17
The aortic balloon occlusion technique uses an inflated balloon to occlude the descending aorta and therefore allow continuous perfusion through the femoral artery for the lower body 18 and the subsequent raising of the target nadir temperature setting point during CPB. Improved surgical procedures have resulted in new requirements for CPB management with regard to formulating a higher temperature setting point, modifying the perfusion rate during the aortic balloon occlusion so that it provides simultaneous flow to the brain and the lower body, and maintaining both the body circulation and protecting the damaged organ during the operation in order to accomplish the whole operation process. This study summarizes specific aspects of the adjusted operative strategy of patient management during and after CPB with the aortic balloon occlusion technique as undertaken at the Fuwai Hospital, National Centre for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China. The current study will provide a report of the early outcomes for this procedure at this centre.
Patients and methods
Study population and data collection
This retrospective study reviewed the in-hospital records of all consecutive patients that underwent the TAR and FET operation in Fuwai Hospital, National Centre for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China between August 2017 and February 2019; during which time the aortic balloon occlusion technique was initially applied, tested for safety by the authors and then gradually introduced to other surgeons in Fuwai Hospital. The indications for TAR with FET in these patients included: (i) for type A aortic dissection with a primary intimal tear distal to the aortic arch that needed to be sealed off by the FET to avoid postoperative development of dissection and prevent aneurysmal formation in the distal aorta; (ii) for complicated type B aortic dissection contraindicated for thoracic endovascular aortic repair; (iii) serving as one of the stages for the treatment of concomitant distal thoracic or thoraco-abdominal aortic replacement. 9 The authors and surgeons who were introduced to the aortic balloon occlusion technique during the study period would apply this technique unless it could not be achieved technically. The other surgeons who were in another team in our centre performed the conventional TAR with FET. All consecutive patients that underwent TAR with FET between August 2017 and February 2019 were included in this study. There were no patients excluded during this study period.
The institutional board of Fuwai Hospital, National Centre for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College approved this study (no. 20180528001) and waived the need for individual patient consent.
Surgical technique and perfusion strategy for the aortic balloon occlusion technique
Arterial cannulation was achieved using the right axillary and femoral arteries of the bifurcated arterial line with a Y-connector from one central perfusion (Figure 1a). Regional cerebral oxygenation saturation (rScO2) of the forehead was monitored by near infrared reflectance spectroscopy (Suzhou Engin Biomedical Electronics, Jiangsu, China). The axillary arterial line blood flow was monitored using an ultrasound flowmeter probe (Transonic Systems Inc, New York, NY, USA). Systemic CPB was discontinued at 28°C of target nasopharyngeal temperature. When the lower body CA needed to start, the femoral line was clamped with the decrease of perfusion rate. After clamping the proximal innominate artery, antegrade selective cerebral perfusion (ASCP) started at a rate of 5–10 ml/kg per min through the right axillary artery cannula. The Cronus stent elephant trunk (diameter 26 or 28 mm, length 100 or 120 mm; Cronus; MicroPort Endovascular Shanghai Co., Ltd., Shanghai, China) was released in the true lumen of the descending aorta. Then the aortic balloon (40 ml Coda Balloon Catheter; Cook Incorporated, Bloomington, IN, USA) in a sheath (16 or 18F; W.L. Gore &Associates, Inc., Flagstaff, AZ, USA) was deployed into the metal part of the stent graft and inflated by injection of 40 ml saline to compress the stent graft. Immediately after the balloon was fixed, perfusion of the lower body was then resumed through the right femoral artery cannula along with ASCP through the right axillary artery cannula from the single central perfusion. The CPB flow was restarted and gradually increased to one-half of total flow. The lower body CA lasted for approximately 5 min (Figure 1b). Immediately after distal anastomosis, the balloon was withdrawn and the graft and its branches were clamped. The left common carotid artery was anastomosed first, after which the perfusion through both carotid arteries could be obtained. Then, rewarming for the patient was started with the CPB flow gradually increased to total flow (Figure 1c). The anastomosis of the left subclavian artery (LSCA) and the innominate artery completed the surgery (Figure 1d).
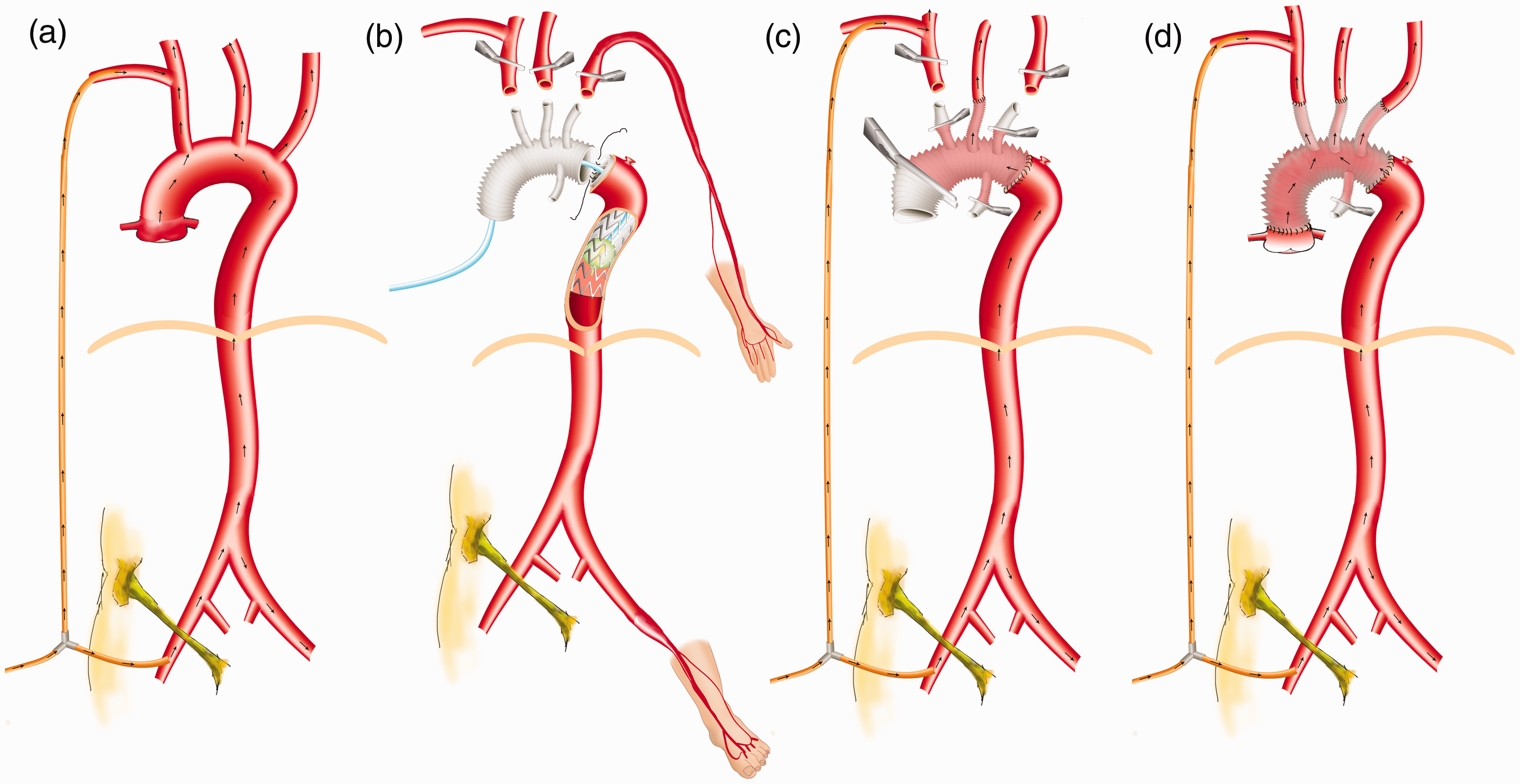
Illustration of the aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique to shorten the lower body circulatory arrest (CA) time and raise the nadir temperature during cardiopulmonary bypass (CPB). (a) CPB establishment. Femoral and axillary cannulations were provided from a bifurcated arterial line from one central perfusion. (b) Set up of aortic balloon occlusion apparatus terminated CA. (c) After achieving bilateral cerebral perfusion, CPB returned to target full perfusion flow and rewarming began. (d) TAR with FET operation finished before CPB withdrawal. The colour version of this figure is available at: http://imr.sagepub.com.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 19.0 (IBM Corp., Armonk, NY, USA).Continuous variables are presented as mean ± SD. For univariate comparison, normally distributed continuous variables were evaluated with Student’s t-test and continuous variables that were not normally distributed were evaluated using Mann–Whitney U-test. Categorical variables were compared using χ2-test. Binary logistic regression was performed on clinical events and checked with Hosmer–Lemeshow fitness before drawing any conclusions. The aortic balloon occlusion group had both the conditions of shorter lower body CA time and higher CPB temperature during CA, but the risk factor analysis of both study groups contained both variables of lower body CA time and CPB temperature. Neither lower body CA time nor CPB temperature could not be considered again in the risk factor analysis because the groups already contained both of these factors. Similarly, an emergency operation in the risk factor analysis described the emergency status of the patient when they were admitted to the hospital, in which the operation was performed on the day of admission or the next morning. Most cases were aortic dissection at an acute stage and thus being at an acute stage of aortic dissection could not be considered in the risk factor analysis because they were basically the same subgroup of patients. As a result, each multivariable analysis considered the following independent variables: categorical variables include aortic balloon occlusion group or conventional group, sex, cardiac surgery history, coronary artery disease history, concomitant coronary artery bypass graft, heavy smoker, emergency operation and aortic dissection extended to total abdominal aorta; and continuous variables included age (years), body mass (kg), height (cm), preoperative haemoglobin (g/l), preoperative platelet count (109/ml), preoperative leukocyte count (109/ml), preoperative percentage of neutrophils (%), preoperative D-dimer (μg/ml), preoperative fibrinogen degradation product (FDP; μg/ml), preoperative aspartate transaminase (U/l) and preoperative serum creatinine (μmol/l). For total transfusion during in-hospital stay, the re-examination value on postoperative day 1 of haemoglobin (g/l), platelet count (109/ml), leukocyte count (109/ml), percentage of neutrophils (%), D-dimer (μg/ml) and FDP (μg/ml) were also considered in addition to the previous independent variables. Major complications and clinical endpoints were reported according to the consensus statement from the International Aortic Arch Surgery Study Group. 19 In particular, acute kidney injury (AKI) was defined as serum creatinine (44–133 μmol/l) increased by >1.5 times baseline values (>200 μmol/l). Liver injury was defined as aspartate transaminase (15–40 U/l) increased by >1.5 times baseline values (>60 U/l) for more than 48 h. A P-value <0.05 was considered statistically significant.
Results
This retrospective study analysed data from 130 patients that received the new TAR with FET (aortic balloon occlusion group) procedure and 230 patients that underwent TAR with FET with lower body CA during distal aortic anastomosis (conventional group). The preoperative demographic and clinical characteristics of the two groups are presented in Table 1. The mean ± SD ages of the patients in the aortic balloon occlusion and conventional groups were 49.84 ± 12.21 and 48.00 ± 10.27 years, respectively. The aortic balloon occlusion and conventional groups were similar in terms of age, body mass, height, body surface area, proportion of males, proportion of heavy smokers, proportion with a history of coronary artery disease, time from symptom onset to the time of the operation and aortic pathology. Significantly more patients in the conventional group had a prior history of cardiac surgery and significantly fewer had aortic pathology at the subacute stage compared with patients in the aortic balloon occlusion group (P < 0.05 for both comparisons).The aortic branches were similarly involved by dissection in the aortic dissection cases (Figure 2).
Preoperative demographic and clinical characteristics of patients that either underwent the new aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique (aortic balloon occlusion group; n = 130) or TAR with FET with lower body circulatory arrest (CA) during distal aortic anastomosis (conventional group; n = 230).

Data presented as mean SD or n of patients (%).
*P < 0.05; for univariate comparison, normally distributed continuous variables were evaluated with Student’s t-test and continuous variables that were not normally distributed were evaluated using Mann–Whitney U-test. Categorical variables were compared using χ2-test.

The ratio of aortic dissection involvement in different segments and branches, expressed as percentage (%) to total cases of aortic dissection: 123 in aortic balloon occlusion group (upper value) and 221 in the conventional (lower value) total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique group. The colour version of this figure is available at: http://imr.sagepub.com.
The perioperative characteristics of the two groups are presented in Table 2. The aortic balloon occlusion group had a significantly shorter mean ± SD lower body CA time than the conventional group (6.33 ± 5.74 min versus 17.24 ± 4.36 min; P<0.001). The mean ± SD total operation time (from the first skin incision to the time in operating room before being transferred back to the intensive care unit [ICU]) was similar in both groups. The mean ± SD primary CPB time was significantly longer in the aortic balloon occlusion group compared with the conventional group (P < 0.05), but the mean ± SD operation time after CPB was significantly shorter in the aortic balloon occlusion group (P < 0.001). A significantly higher proportion of patients required a secondary CPB in the conventional group compared with the aortic balloon occlusion group (P = 0.006).
Perioperative characteristics of patients that either underwent the new aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique (aortic balloon occlusion group; n = 130) or TAR with FET with lower body circulatory arrest (CA) during distal aortic anastomosis (conventional group; n = 230).

Data presented as mean SD or n of patients (%).
aFor univariate comparison, normally distributed continuous variables were evaluated with Student’s t-test and continuous variables that were not normally distributed were evaluated using Mann–Whitney U-test. Categorical variables were compared using χ2-test; NS, no significant between-group difference (P ≥ 0.05).
CPB, cardiopulmonary bypass; ASCP, antegrade selective cerebral perfusion.
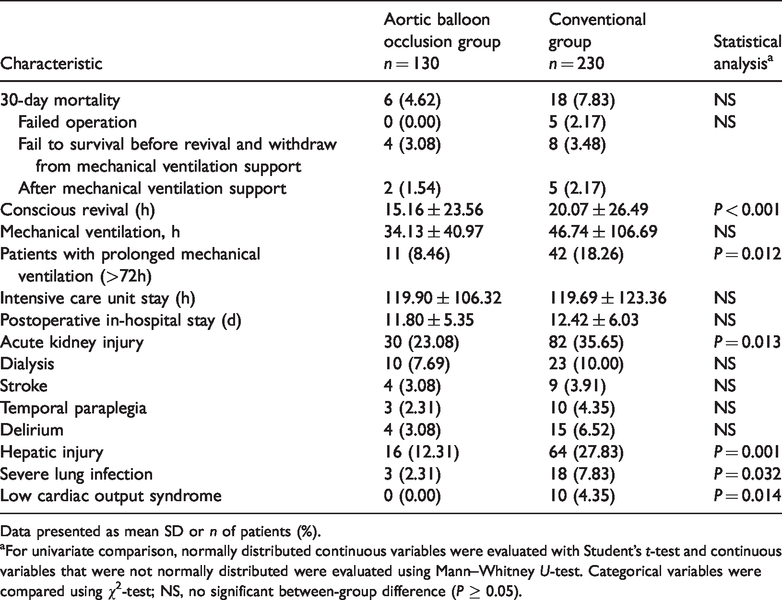
Univariate comparisons showed that the 30-day mortality rate was similar in the aortic balloon occlusion group compared with the conventional group (4.62% versus 7.83%, respectively) (Table 3). The patients in the aortic balloon occlusion group were revived significantly earlier from anaesthesia than the conventional group (P < 0.001), but the total mechanical ventilation support time was not significantly different between the two groups. The ICU stay and the postoperative in-hospital stay were similar between the two groups. The aortic balloon occlusion group had significantly less prolonged mechanical ventilation (>72 h), low cardiac output syndrome, less severe lung infection and less hepatic injury compared with the conventional group (P < 0.05 for all comparisons). The proportion of patients with AKI was significantly lower in the aortic balloon occlusion group compared with the conventional group (P = 0.013), but this resulted in similar rates of dialysis in the two groups.
Postoperative characteristics of patients that either underwent the new aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique (aortic balloon occlusion group; n = 130) or TAR with FET with lower body circulatory arrest (CA) during distal aortic anastomosis (conventional group; n = 230).
Data presented as mean SD or n of patients (%).
aFor univariate comparison, normally distributed continuous variables were evaluated with Student’s t-test and continuous variables that were not normally distributed were evaluated using Mann–Whitney U-test. Categorical variables were compared using χ2-test; NS, no significant between-group difference (P ≥ 0.05).
With regard to changes in temperature during the operation, system cooling was started at a mean ± SD of 3.29 ± 2.38 min in the aortic balloon occlusion group and at 3.17 ± 4.47 min in the conventional group (Figure 3). The aortic balloon occlusion group reached the target nasal temperature of 28°C at a mean ± SD of 24.18 ± 6.88 min of CPB and the conventional group reached the target nasal temperature of 25°C at a mean ± SD of 33.50 ± 10.59 min of CPB, after which time lower body CA could be started if necessary. For the aortic balloon occlusion patients, ASCP was started at a mean ± SD of 60.44 ± 28.71 min when the nasal and rectal temperatures naturally distributed to 27.41 ± 1.06°C and 29.00 ± 1.91°C, respectively. For the conventional TAR with FET patients, ASCP was started at a mean ± SD of 47.39 ± 24.50 min when the nasal and rectal temperatures were 25.37 ± 1.34°C and 28.46 ± 2.55°C, respectively. At a mean ± SD of 100.32 ± 33.84 min and 80.66 ± 28.43 min for the aortic balloon occlusion and conventional groups, respectively, both groups finished anastomosis of the left common carotid artery as the perfusion through both hemispheres was obtained; then rewarming began. At a mean ± SD of 153.96 ± 39.68 min and 146.25 ± 38.62 min, the rectal temperature was warmed up to 35°C, in the aortic balloon occlusion and conventional groups, respectively. Then the CPB could be stopped if necessary.

Temperature changes over time during cardiopulmonary bypass (CPB) in patients that either underwent the new aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique (aortic balloon occlusion group; n = 130) or TAR with FET with lower body circulatory arrest (CA) during distal aortic anastomosis (conventional group; n = 230). (a) Nasal temperature; (b) rectal temperature. Data presented as mean ± SD. The colour version of this figure is available at: http://imr.sagepub.com.
With regard to changes in perfusion rate during the operation, Figure 4 presents the results recorded from the CPB reports. Right axillary and femoral arterial cannulations were provided from a bifurcated arterial line from one central perfusion with a controllable perfusion pressure, but the exact perfusion rate allocation of the axillary and femoral arterial cannulations was unknown and this was recorded in the present study. Before the aortic arch was resected, the perfusion rate allocation of the axillary/total ratio was approximately one-third. During the TAR procedure when the aortic arch was completely resected, axillary perfusion proceeded with clamped innominate artery and the perfusion rate allocation of the axillary/total ratio was approximately one-quarter. When the TAR procedure completed, the axillary/total ratio was approximately one-third again similar to the value before the lower body CA started.
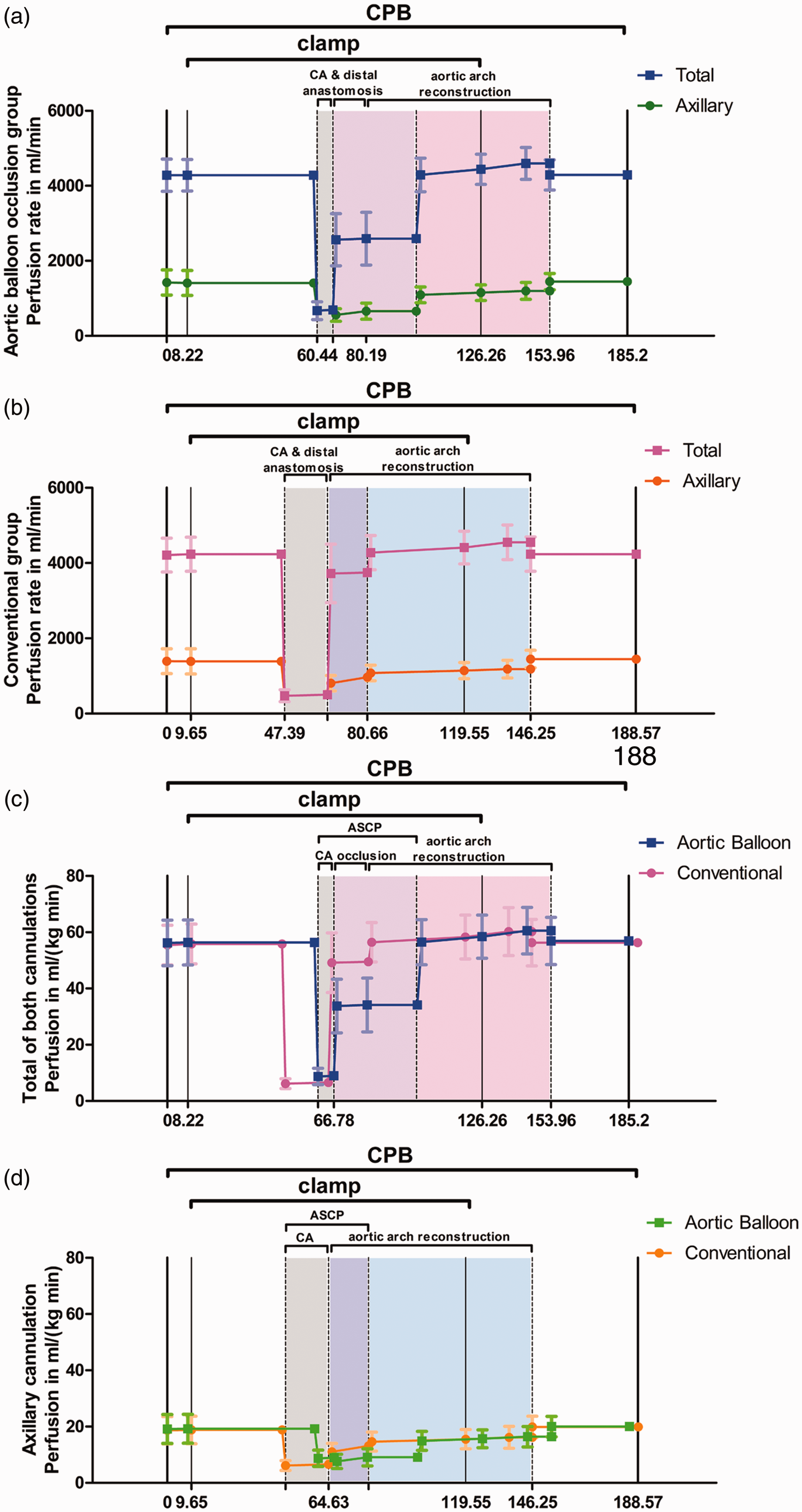
Perfusion rate changes over time during cardiopulmonary bypass (CPB) in patients that either underwent the new aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique (aortic balloon occlusion group; n = 130) or TAR with FET with lower body circulatory arrest (CA) during distal aortic anastomosis (conventional group; n = 230). (a) Total and axillary cannulation rate in ml/min in the aortic balloon occlusion group; (b) total and axillary cannulation rate in ml/min in the conventional group; (c) total rate in ml/kg per min in both groups; (d) axillary cannulation rate in ml/kg per min in both groups. Data presented as mean ± SD. ASCP, antegrade selective cerebral perfusion. The colour version of this figure is available at: http://imr.sagepub.com.
With regard to changes in CPB pressure during the operation, Figure 5 presents the monitored blood pressure (BP) of the left radial artery and the foot dorsal artery. The left radial artery catheterization measured BP represents the perfusion pressure of the upper part of the body from the right axillary artery. The foot dorsal artery was catheterized on the non-cannulated side (mostly the left side) and measured the BP of lower part of the body (Figure 1b). During aortic arch reconstruction, perfusion of the organs in the upper body was only from the right axillary artery cannulation, perfusion of the organs in the lower body was only from the right femoral artery cannulation; and all of the blood was mixed and drained back to the CPB machine for oxygenation. Figure 5b shows a greater discontinuity of the lower body perfusion gap in the conventional group compared with the aortic balloon occlusion group. Under normal conditions, the foot dorsal artery BP was higher than the radial artery BP, but when aortic dissection was involved in and occluded the LSCA or left external iliac artery, the monitored radial artery BP and foot dorsal artery BP would drop. The mean ± SD radial artery BP monitored before CPB was 66.22 ± 13.14 mmHg and 67.49 ± 12.01 mmHg in the aortic balloon occlusion and conventional groups, respectively, while the mean ± SD foot dorsal artery BP before CPB was 66.60 ± 13.16 mmHg and 68.14 ± 13.03 mmHg in the aortic balloon occlusion and conventional groups, respectively. The difference of radial artery BP and foot dorsal artery BP was not significant, suggesting that the occlusion of the left external iliac artery affected foot dorsal artery BP more greatly. If the monitored radial artery BP or the foot dorsal artery BP was low after the TAR procedure, concomitant bypass to the aortic arch branches or femoral artery was performed. The anastomosis of LSCA also made the radial artery BP much higher because it could be affected by femoral perfusion afterwards.

Monitored blood pressure over time during cardiopulmonary bypass (CPB) in patients that either underwent the new aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique (aortic balloon occlusion group; n = 130) or TAR with FET with lower body circulatory arrest (CA) during distal aortic anastomosis (conventional group; n = 230). (a) Radial artery blood pressure; (b) foot dorsal artery blood pressure. Data presented as mean ± SD. ASCP, antegrade selective cerebral perfusion; LSCA, left subclavian artery. The colour version of this figure is available at: http://imr.sagepub.com.
With regard to the early clinical outcomes, multivariate analysis results showed that risk factors for 30-day mortality were heavy smoker (odds ratio [OR] 7.090; 95% confidence interval [CI] 1.491, 33.707; P = 0.014], emergency operation (OR 34.731; 95% CI 3.537, 341.021; P = 0.002), preoperative percentage of neutrophils (OR 1.104; 95% CI 1.009, 1.207; P = 0.031) and CPB time (OR 1.010; 95% CI 1.005, 1.014; P < 0.001) (Table 4). The conventional surgical method was one of the significant risk factors for postoperative acute kidney injury, hepatic injury and having a conscious revival time >12 h (P < 0.05 for all three outcomes), but it was not related to the other clinical outcomes. The total CPB time was shown to be a risk factor for 30-day mortality, dialysis, prolonged mechanical ventilation (>72 h) and severe lung infection. Postoperative stroke and temporal paraplegia failed to find risk factors in this model. Thus, all significant risk factors (OR > 1 for a positive risk factor) and all risk factors with a nonsignificant P-value but P < 0.1 are shown in the appropriate tables.
Multivariate analysis of the risk factors for clinical outcomes in patients that either underwent the new aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique (aortic balloon occlusion group; n = 130) or TAR with FET with lower body circulatory arrest (CA) during distal aortic anastomosis (conventional group; n = 230).

*Not significant but P < 0.1.
CPB, cardiopulmonary bypass; Scr, serum creatinine; CABG, coronary artery bypass graft; FDP, fibrinogen degradation product; AST, aspartate transaminase; POD1, postoperative day 1.
Patients undergoing surgery requiring CPB are at high risk for bleeding. 20 Red blood cell (RBC) transfusion during CPB was triggered if the haematocrit fell below 20% (an approximate haemoglobin of 70 g/l). In the current standard protocol at this institution, RBCs were transfused if the haemoglobin fell below 80 g/l.21,22The aortic balloon occlusion and conventional groups were primed with a mean ± SD of 1654.88 ± 203.47 ml and 1673.81 ± 220.97 ml bloodless prime in the circuit tubing, respectively, which is a risk for haemodilution. During CPB, 33.08% (43 of 130) and 33.91% (78 of 230) of patients in the aortic balloon occlusion and conventional groups, respectively, required RBC transfusion into the running bypass system; with a mean ± SD of 4.44 ± 1.86 and 4.77 ± 2.61 units used in each group, respectively (Table 5). Multivariate analysis showed that RBC perfusion requirement during CPB was not affected by application of aortic balloon occlusion (shorter lower body CA with higher nadir temperature) (Table 6). Aortic balloon occlusion reduced RBC transfusion requirement and the requirement for RBC transfusion of ≥3 packages (≥6 units) after CPB during operation and total during in-hospital stay. Aortic balloon occlusion did not reduce plasma and platelet transfusion. A longer CPB time was a risk factor for a requirement for transfusion of RBCs, plasma and platelets. In addition to age, female sex, cardiac surgery history and blood examination of FDP, most risk factors that were identified in this model were haemodynamic factors. The requirement for blood cell (RBCs and platelets) transfusions were inversely related to body mass, preoperative blood cell count (operative transfusion) and postoperative blood cell count (total transfusion). Since CPB destroyed all coagulation factors, plasma transfusion requirement was positively related to body mass. Because whenever body mass appeared as a risk factor in relation to RBC and platelet transfusion, the OR was <1, which suggests that the higher the mass, the less likely RBC transfusion was performed. The opposite was true for plasma transfusion. For blood cell counts: (i) the higher the preoperative haemoglobin was, the less operative RBC transfusion was required (haemoglobin OR < 1); (ii) the level of postoperative haemoglobin could result from less operative damage or more operative transfusion. Nevertheless, the higher the postoperative haemoglobin was, the less RBC transfusion was required during in-hospital stay (postoperative haemoglobin OR < 1); (iii) the difference between pre- and postoperative platelet count was a sensitive indicator of operative damage. Thus, the higher the preoperative platelet count was, the more RBC transfusion was required during in-hospital stay (platelet count OR > 1). While the greater that the postoperative platelet count was, the less RBC transfusion was required during in-hospital stay (postoperative platelet count OR < 1). These results came out in pairs; if one of the pair was removed from consideration, the other one would no long be significant. The platelet transfusion results were almost the same as the RBC transfusion results. In particular for point (iii), the difference between pre- and postoperative haemoglobin also reflected the operative damage and reflected this in platelet transfusion risk factor analysis. Some additional intraoperative clinical events that were analysed in the same model are presented in Table 7.
Transfusion and blood biochemistry data for patients that either underwent the new aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique (aortic balloon occlusion group; n = 130) or TAR with FET with lower body circulatory arrest (CA) during distal aortic anastomosis (conventional group; n = 230).

Data presented as mean SD or n of patients (%).
aFor univariate comparison, normally distributed continuous variables were evaluated with Student’s t-test and continuous variables that were not normally distributed were evaluated using Mann–Whitney U-test. Categorical variables were compared using χ2-test; NS, no significant between-group difference (P ≥ 0.05).
RBC, red blood cell; CPB, cardiopulmonary bypass; FDP, fibrinogen degradation product; AST, aspartate transaminase; Scr, serum creatinine.
Multivariate analysis of the risk factors for blood transfusion in patients that either underwent the new aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique (aortic balloon occlusion group; n = 130) or TAR with FET with lower body circulatory arrest (CA) during distal aortic anastomosis (conventional group; n = 230).

*Not significant but P < 0.1.
RBC, red blood cell; CPB, cardiopulmonary bypass; FDP, fibrinogen degradation product; AST, aspartate transaminase; POD1, postoperative day 1.
Multivariate analysis of the risk factors for perioperative clinical events in patients that either underwent the new aortic balloon occlusion technique that was used to assist total aortic arch replacement (TAR) with the frozen elephant trunk (FET) technique (aortic balloon occlusion group; n = 130) or TAR with FET with lower body circulatory arrest (CA) during distal aortic anastomosis (conventional group; n = 230).

*Not significant but P < 0.1.
CPB, cardiopulmonary bypass; Scr, serum creatinine.
Discussion
Over the past 10 years of performing TAR with FET, the lower body CA time has been gradually shortening due to surgical skill improvement and CA temperature has been rising.1,11,12,16,23The current study institution is using 25–26°C as the safe standard CA setting point, which was predicated on an expected mean of 17 min of lower body CA. This routine 25–26°C was already a much higher temperature level than that which was initially reported (18–20°C). 23 For conventional TAR with FET, the CA temperature could not be higher if the lower body CA time could not be further shortened by the surgical method. Raising the CA temperature was reported to have very limited effect on AKI. 16
The aortic balloon occlusion technique offers consistent lower body perfusion and provides a sufficient time window to perform aortic arch procedures. To ensure the safety of the procedure, the CA temperature setting point must be synchronized with an expected shorter lower body CA time as well as ensuring cerebral protection. The nasal 28°C strictly selected as the cooling setting point to make sure the brain could tolerate the 5 min of ASCP and lower body CA. The 28°C setting point significantly shortened the cooling and rewarming times in the aortic balloon occlusion group compared with the conventional group. The trajectories of temperature also showed that the nasal temperature rewarmed faster than the rectal temperature due to the uneven distribution of the arterial lines, despite the fact that the surgeons at this study institution routinely use an ice hat to slow the cerebral rewarming speed to achieve parallel upper and lower rewarming processes. Since the speed of rewarming is limited by the rectal temperature, when the rectal temperature had reached 35°C this was defined as the end of rewarming. This was also the earliest time that the CPB could be stopped, otherwise the rewarming resumes despite the procedure being finished.
With the natural distribution of the perfusion rate from one single perfusion pump, the quantity of perfusion that the brain received in relation to the total perfusion rate was crucial to judge the safety of the cerebral protection of the operation, so this current study measured the precise perfusion distribution of the cerebral and systemic arterial lines. The recommended ASCP rate was 10–15 ml/kg per min and the bilateral cerebral perfusion rate was 20–30 ml/kg per min.24,25 Before CA was commenced, the axillary perfusion accounted for one-third of the total perfusion. During lower body CA, ASCP, which was total flow, was continuously set at 10–15 ml/kg per min and the femoral perfusion was clamped. When aortic balloon occlusion was set up, the femoral perfusion clamp was released. If the total flow was set at 1/2–3/4 of the target full perfusion rate, the axillary perfusion rate was approximately 10–15 ml/kg per min. When the left carotid artery was reconstructed, the total flow returned to the target full perfusion with the axillary perfusion accounting for one-quarter of the total perfusion, approximately 15 ml/kg per min. When all of the surgical procedures were completed, the axillary perfusion accounted for one-third of the total perfusion, similar to the preoperative level. For normal cases, the current authors recommend a thinner cannula for the axillary artery than the femoral artery cannula to achieve appropriate flow distribution. A Hoffman clamp could be used to alter the resistance difference between the two lines. For example, if rScO2 drops > 15% of baseline or ASCP < 5 ml/kg per min, a Hoffman clamp could be used on the femoral artery line.
The perfusion of the cerebral and systemic arterial lines was controlled by the perfusion pressure. However, perfusion would not flow to an occluded branch or even to an occluded aortic true lumen. Thus, the operative monitoring of the upper and lower limbs was crucial for validation of the proper aortic pressure, which equalled the end-organ perfusion pressure. The arterial catheter pressure of the radial artery and foot dorsal artery should be kept between 50–70 mmHg to ensure the proper perfusion to the brain and kidneys. In the case of diagnosed or confirmed cerebral or renal arterial disease, the monitored pressure should be kept at a higher value (in the 70s mmHg) to prevent postoperative stroke and AKI.
The present study retrospectively reviewed consecutive patients that underwent TAR with FET to study the effect of the aortic balloon occlusion technique. The present study had several limitations. First, it only presented data from within a recent time period (i.e. since the invention of the technique in August 2017). Thus, all consecutive data were used to perform the multivariate analysis, which made the findings of the multivariate analysis more convincing. The findings of the univariate comparisons were less convincing because they contained bias. As a result, the number of patients was enough to find risk factors for many, but not all kinds of the clinical outcomes. For example, the study was not able to identify risk factors for postoperative stroke or paraplegia. Secondly, the study lacked long-term follow-up because it focused on the early postoperative outcomes only.
In conclusion, the aortic balloon occlusion technique achieved significantly lower rates of postoperative AKI and hepatic injury as well as less need for RBC transfusion, but these changes did not translate into significantly less dialysis or 30-day mortality. In our opinion, this technique remains highly recommended for patients that are predisposed to risk factors in order to prevent postoperative complications. The aortic balloon occlusion technique is not only very friendly for new surgeons that are using the TAR with FET procedure, but it is also suitable for experienced surgeons who are performing TAR with FET on more severely ill patients. Balancing and maintaining sufficient cerebral and lower body perfusion is crucial during the CPB procedure. Continued research into CBP management of the aortic balloon occlusion technique should be directed toward getting the precise temperature, CBP flow and pressure to optimize intraoperative care.
Footnotes
Acknowledgements
The authors thank Miss Shuang Han, who is a MD and PhD candidate from Shandong University Cheeloo College of Medicine, for her figure drawing.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Beijing Municipal Science and Technology Commission, China (Major Special Project no. Z181100001718197).