
Abstract
Coronary artery bypass grafting remains the treatment of choice for a large cohort of patients with significant coronary disease. Despite the increased use of arterial grafts, the long saphenous vein remains the most commonly used conduit. Long-term graft patency continues to be the Achilles heel of saphenous vein grafts. This is due to the development of intimal hyperplasia, a chronic inflammatory disease that results in the narrowing and occlusion of a significant number of vein grafts. Research models for intimal hyperplasia are essential for a better understanding of pathophysiological processes of this condition. Large animal models resemble human anatomical structures and have been used as a surrogate to study disease development and prevention over the years. In this paper, we systematically review all published studies that utilized large animal models of vein graft disease with a focus on the type of model and any therapeutic intervention, specifically the use of external stents/mesh.
Keywords
Introduction
The long saphenous vein (LSV) is the most commonly used conduit in cardiac surgery; however, its use is complicated by an increased risk of late stenosis or occlusion due to the development of intimal hyperplasia (IH) and accelerated atherosclerosis.1,2 IH is a chronic inflammatory process characterized by an activation and subsequent switching of the vascular smooth muscle cells (VSMCs) from a quiescent state to a synthetic proliferative and its migration to the intimal layer. 2 The development of IH is a complex process that is not fully understood. Many small and large animal models were developed over the years to study the pathophysiology of IH and/or to try and modify it using different therapeutics. In this review, we systematically look at the studies that utilized large animals in the field of IH and vein grafts disease and the therapeutics used with especial focus on the external stents/mesh which are external scaffolds that are made of different materials which can make then stiff around the vessel of just soft material that just wrap the graft with some of them able to be loaded with different therapeutic agents and can be placed around the veins during surgery which made them an interesting venue to explore by cardiac surgeons, considering the ability to place them on vein during surgery without significantly affecting the flow or length of surgery.
Methods
A systematic review was performed using methods described in Cochrane Handbook for Systematic Reviews of Interventions. 3 A protocol was registered prospectively on International Prospective Register of Systematic Reviews (PROSPERO) (CRD42021262342). The study adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
The aim of the review was to systematically review studies of vein grafts IH using large animals with detailed description of the different models of grafting and any therapeutic methods used.
Search strategy
Three reviewers (FO, LM, and SL) independently performed each step of the literature search. Electronic searches were conducted using the Cochrane Central Register of Controlled Trials, MEDLINE, and EMBASE without date or language restriction from inception to the end of December 2020. A full description of the search terms is listed in the Supplementary Materials. In addition, the reference lists of all retrieved articles were manually searched for further relevant studies not previously identified. Each reviewer independently screened the title and abstract to first identify relevant articles. Next, the full text of each article was independently screened. After each stage, agreement on included studies was reached through discussion.
Study Eligibility
The inclusion criteria were 1. Any in vivo large animal studies investigating the development or modification of IH in vein grafts in any large animal model.
Exclusion Criteria included the following: (1) studies that did not look at IH and focused on other parameters such as flow pattern studies or acute thrombosis, (2) small animal studies, (3) animal studies that were designed to look at IH in the setting of arterio-venous fistula, (4) studies that used synthetic tissue or focused on tissue engineering, (5) transplant-related diseases, (6) studies looking at venous patch grafts, (7) ex vivo studies using large animal tissue, (8) arterial graft models, and (9) abstracts.
Data Extraction
A standardized form was developed to extract data from the included studies for assessment of study quality and evidence synthesis. This form was tabulated using Microsoft Excel 2016 (Microsoft, Redmond, Washington). Data extraction first considered data from figures, tables, and graphs (using digital ruler software where appropriate), followed by data extraction from the main text. Data extracted to the standardized form was categorized under the following headings: author, title, year, journal, research aims and objectives, subjects examined, cell type examined, sequencing method, research methodology, and key findings. Data extraction was performed by three authors (FO, MZ, and LM), and any discrepancies were resolved by discussion.
Bias and Quality Assessment
Quality was assessed using the ARRIVE Essential 10 guidelines checklist. 4 For assessment of the risk of bias, a modified version of this tool specific for animal intervention studies, SYRCLE, was utilized. 5 Following data extraction, the authors (FO, LM, and SL) performed quality and risk of bias assessment. Any discrepancies were resolved by discussion between all authors.
Data Synthesis
A narrative synthesis of all included studies was performed, with all relevant data tabulated where appropriate. For all outcomes, data was extracted in text format or as mean +/− standard deviation for numerical values. Where applicable, continuous variables were summarized with standardized mean difference, and dichotomous data was summarized with risk and odd ratios. Where relevant data was missing, authors were contacted (where possible); otherwise, data was presented as described in the article or supplementary data. Given the anticipated diversity of outcome measures, limited scope for statistical analysis was expected and as such, meta-analysis was not undertaken.
Results
A flow diagram showing the results of the searches is shown in Figure 1. Initial search identified 3049 records, which was reduced to 2841 after the removal of duplicate. Of these, 2100 were excluded as it did not report the outcome of interest, and 601 were not relevant. The remaining 140 records were re-assessed, and 86 papers were finally included. An additional 13 papers were identified from the reference’s searches, and 99 were finally included in this review. The studies included were over a span of more than 30 years (1985–2020) and included three species (dogs in 55 studies, porcine in 39 studies, and sheep in 5 studies).
Flow diagram of study selection.
Dog models
Fifty-five papers were identified to use a dog model of IH and are summarized in Table 1.6–60
Summary of studies using the dog model of vein grafts IH.

Different models were designed to study the development of IH. This included using femoral vein–femoral artery interposition in 23 studies (in situ or reversed),14,17,18,20,23–25,30,32–38,40,42,51,52,55,56,58,60 jugular vein–carotid artery interposition grafts in 12 studies,12,16,19,29,31,41,46,49,50,54,57,59 jugular vein–femoral artery interposition graft in 7 studies,6–9,11,39,48 cephalic vein–femoral artery interposition graft in 2 studies,47,53 femoral vein–carotid interposition in 2 studies,21,22 saphenous vein–femoral artery interposition model in 2 studies,15,27 Jugular vein to both the carotid and femoral arteries in 1 study, 13 jugular vein to carotid artery and femoral vein to femoral artery in 1 study (in situ or reversed), 26 and 1 study used different types of venous and arterial interposition models. 10 The saphenous vein end to side between the LAD and aorta was used in 2 studies,43,45 and 2 studies utilized a femoropopliteal-saphenous vein end to the side model.28,44
The dog model additionally included the step of developing a poor run off model in 12 studies, all using the femoral vein–femoral artery model.17,20,23–25,32,33,37,38,40,52 This model was originally described by Morinaga et al. 17 where all tributary arteries distal to the saphenous artery in the posterior limb are ligated and severed, except for a superior branch of the posterior femoral artery. Thus, a condition of poor runoff is created. Four weeks after the first surgical procedure, when the collateral vessels seem to be fully developed, the femoral artery and vein are exposed, and a segment of femoral vein is interpositioned into the femoral artery.
None of these were a diabetic model with 2 papers reporting the use of hypercholestolemic dogs.19,22
Nineteen of these studies used a drug as an intervention to modulate IH which included a wide range of medications such as liver oil, ibuprofen, rapamycin, and selective inflammatory inhibitors.6–9,11,19,22,26,29,30,33,40–42,49,52,57–59 Other treatment modalities included the use of antisense oligomers, decoys, adenovirus, radiation, different storage or harvest methods, and external stents including biodegradable and drug eluting stents. Few studies looked at the difference between in situ and reversed veins which were of no clinical value in CABG; however, these studies highlighted an important role for EC preservation in the modulation of IH.12,28,31
One study looked at the role of using an in-house developed rapamycin-eluting biodegradable PLA-CL film applied externally in a femoral vein to femoral artery interposition and femoral artery to femoral artery model where three concentrations of rapamycin were used. In the vein graft models, the ratio of intimal area was significantly decreased only in the high concentration group compared with control at 4 weeks, while all concentrations were able to suppress IH in the arterial grafting model. The inhibition of neointimal growth was associated with reduced cell proliferation, as evidenced by proliferating cell nuclear antigen immunostaining and diminished alpha-actin positive vascular smooth muscle cells. 51
Using different sizes of expanded polytetrafluoroethylene (ePTFE) as external stents (4, 6, and 8 mm) in a model of femoral vein to femoral artery interposition grafts, Zou et al. showed that stents with different size can exert similar effect on the prevention of IH at 4 weeks after surgery. 55 A biodegradable PLA-CL mesh external stent (8 mm) was compared to a nonabsorbable stent and no stent control in a femoral vein to femoral artery interposition grafts model. At 12 months, the endoluminal circumferential and the vein graft length was significantly smaller in the PLA-CL and nonabsorbable groups than that in the control group. Similarly, the mean intimal–medial thickness was less in PLA-CL and nonabsorbable stent groups compared to the control group. Interestingly, all grafts that had the biodegradable stent were patented compared to the nonabsorbable and control groups. 60
Porcine model
Thirty-nine papers were identified to use a porcine model of IH and are summarized in Table 2.61–99
Summary of studies using porcine model of vein grafts IH.
Thirty-three studies used the saphenous vein–carotid interposition graft model,61–81,86–90,92,96–99 3 papers used the jugular vein–carotid artery interposition as a model82,93,95 and end to side in 1 study. 85 The saphenous vein was used as a self-designed double-layer autologous graft to femoral artery in 1 study 94 and the mammary vein to the LAD end to side in 1 study. 91
There were no poor run-off models. Three studies used a hypercholestolemic model which was high fat diet induced or hypercholestolemic minipigs64,85,95 and 1 diabetic model. 65
The most common intervention used in this model was external stents, which was of different material or sizes. This model was driven by the Bristol Heart institute since the early 1990s. Violaris et al. 78 used this model to investigate the role of using a 4 mm external porous polytetrafluoroethylene stent. At 4 weeks, all grafts showed an increase in external size, but this was restricted by stenting. Furthermore, there was an increase in the cross-sectional area of the tunica media and tunica intima; however, stented grafts showed less enlargement of the media but greater enlargement of the intima. Thus, wall size was, therefore, similar in stented and unstented grafts. The group concluded that the use of 4-mm external stents is unlikely to benefit as the final luminal size is thought to be of paramount importance in maintaining long-term patency. The group revisited the use of different sizes of stents when Izzat et al. 71 used a VP1200 polyester Locknit tube externally supported with helically wound polypropylene stent sizes (5-mm, 6-mm, and 8-mm diameter). At 4 weeks after grafting, total wall thickness was decreased in all stented grafts compared to unstented grafts. However, neointimal thickness was only reduced when using 6-mm and 8-mm stents but not by 5-mm stents. The concern raised by the group previously in term of intimal encroachment of the intima into the lumen was significantly reduced when using the 6- or 8-mm stents versus unstented grafts. Both neointimal and medial cell proliferation were significantly reduced by all three stents compared with unstented grafts, which was further supported by Angelini et al. 63
Using 8 mm external stents, Mehta et al. 76 compared morphological changes and PDGF expression in stented grafts and contralateral unstented grafts in the same pigs, 6 months after graft implantation, and demonstrated that reduced medial thickening, neointima formation, and cell proliferation were sustained in externally stented grafts, and these effects were associated with a significant reduction in PDGF expression. Jeremy et al. 73 using the 6-mm grafts further investigated the mechanisms involved in the modulation of IH by external stents and showed an essential role for PGI2 and NO in promoting microangiogenesis in the adventitia of stented vein grafts, which may in turn minimize graft hypoxia which is an established contributory factor to neointima formation.
These results encouraged the use of other types of external stents material such as a compliant Phynox mesh tubing (a wrought cobalt–chromium–nickel–molybdenum–iron Alloy) which similarly showed significant reduction of IH in stented grafts. 84 George et al. 70 used two different stent materials contra-laterally in the same pigs. One comprised an 8-mm diameter macroporous polyester velour tube and the other an 8-mm diameter microporous PTFE tube. One month after surgery, macroporous stents significantly reduced neointimal and medial thickening compared with microporous stents. Macroporous stents significantly reduced the percentage of cells expressing PDGF and PCNA compared with microporous stents. Adventitial microvessel formation occurred across macroporous stents but was markedly suppressed by microporous stents. This data clearly demonstrated the importance of porosity in external stents in reducing neointima.
To further understand the mechanisms involved in regulating IH by external stents, Angelini et al. 64 used the 8-mm-polyester locknit velour tube externally with polypropylene in pigs fed on a high-fat diet and only animals that achieved a plasma cholesterol level of at least 8 mmol/L were included in the study to maximize the stimulus for graft cholesterol accumulation. Further plasma cholesterol determinations were carried out in these pigs at the time of graft harvest. The group noted that stenting reduced graft cholesterol concentration significantly. Furthermore, foam cells were observed in unstented grafts but not in stented grafts. Moreover, vascular cell adhesion molecule 1 was strongly expressed in intimal and medial cells in unstented compared to stented grafts. More understanding of the mechanisms involved in modulating IH came from Dashwood et al.66,67 using the 8-mm stents showed that neural reorganization plays a role in vein graft failure, possibly through the local release of mitogens; the prevention of this reorganization contributes to the inhibitory effect of the external stent on neointima formation.
Another study by Jeremy et al. 72 used external placement of polyglactin (Vicryl) sheaths (8 mm in diameter) and showed that these polyglactin sheaths significantly reduced intimal thickness, medial thickness, and the percentage of proliferating cells compared with unsheathed controls after 4 weeks. Interestingly, there was a pronounced accumulation of macrophages, giant cells, EC, and microvessels within and surrounding the biodegradable sheath compared with controls, suggesting that this stents may reduce medial and intimal thickening through inflammatory cell–mediated angiogenesis. When looking at the long-term effect of such a stent, Vijayan et al. 77 showed a persistent reduction in neointimal thickening at 6 months even after the degradation of the stent itself, confirming the important potential role of using a biodegradable external stent as a novel approach to ameliorating the problem of intimal hyperplasia that plagues these grafts.
Five studies used drugs including orally administered medications including penicillamine, endothelin 1(A) receptor antagonist BSF 302,146, aspirin-nitric oxide adduct, or folic acid and showed promising results by reducing vein graft thickening and promotes positive remodeling.65,80,81 Adenovirus transfer was used in a small amount of studies and included Ad overexpressed in the proapoptotic gene p53, Nogo-B, or soluble vascular cell adhesion molecule (sVCAM) (Ad.CB-sVCAM) with promising results .82,86,90
Other modulation methods included the use of fibrin glue, prophylactic brachytherapy, photochemical tissue passivation (PTP) treatment, ultrasound-mediated tissue inhibitor of metalloproteinase (TIMP-3) plasmid, periadventitial rapamycin-eluting microbeads, and using the vein as a double layer to restrain excessive distension, 83,85,87,89,92,94,96 all with encouraging results during the time of study except for the periadventitial rapamycin-eluting microbeads as the initial effect of rapamycin was not sustained, and there was no therapeutic benefit evident in 12-week grafts . 92
Sheep model
Five papers were identified that used a sheep model and are summarized in Table 3.100–104
Summary of studies using porcine model of vein grafts IH.
The models included the jugular vein to carotid artery interposition model in 2 studies,101,103 radial vein to carotid artery in 1 study, 102 the femoral vein to carotid artery in 1 study, 104 and 1 saphenous vein to femoral artery as the end to side mode. 100
None of these studies was designed as a poor run-off, and none of them was a diabetic or hypercholesteremic model.
These studies were designed to study the role of using an external mesh/stent to modulate IH except for the saphenous vein model 100 that was a descriptive study of a new model of vein graft disease.
Barra et al. compared the impact of using a constrictive mesh tube to no mesh and suggested that 4 months after surgery, the use of mesh was associated with more normal endothelium and moderate and regular intimal thickening. 101
Similarly, Krejca et al. 102 used a newly designed 4-mm polyester fiber (torlen/dacron). The mean intimal wall thickness was assessed at different times (up to 12 weeks) and was consistently significantly less than the control graft weeks with a smooth endothelial layer with intact nuclei and when looking at the potential mechanisms involved in the protective effect of this new stent, it was noted that it can be related to the downregulation of VEGF-A.
Klesius et al. 104 compared the short-term impact (4 weeks) of using three different stents chosen based on ex vivo work performed by the group and included a newly designed polyester stent, microporous PTFE stent grafts, and metallic biocompound stents. In addition, the group investigated the long-term (6 months) effect of using the polyester stent in a femoral vein to the carotid interposition model and concluded that the new macroporous polyester stent led to significantly higher reduction of neointimal hyperplasia and luminal encroachment compared to the native vessel. It proved superior to PTFE stenting, while the biocompound material failed to prove its efficacy.
Risk of Bias and quality assessment
Risk of bias using the modified SYRCLE is presented in Figure 2. There was no sufficient information regarding sequence generation or random housing. All the other fields showed that the risk of bias was low or unclear with some minor concern of high risk of bias regarding baseline characteristics in 3 studies,9,13,101 selective reporting in 3 studies,9,13,60 incomplete outcome data in 1 study, 60 and other sources of bias in 3 studies 9,52,92
Risk of bias assessment.
Quality assessment using the ARRIVE Essential 10 is presented in Figure 3. Overall, all studies clearly presented information regarding inclusion/exclusion criteria, outcome measures, statistical methods, experimental animals, and procedures and results. There was no clear data regarding randomization, and 23 studies did not report clear number of animals used.17,18,20,23,25,27,33,34,36,38,50,60–62,65,67,74,75,78,82,90,97,98
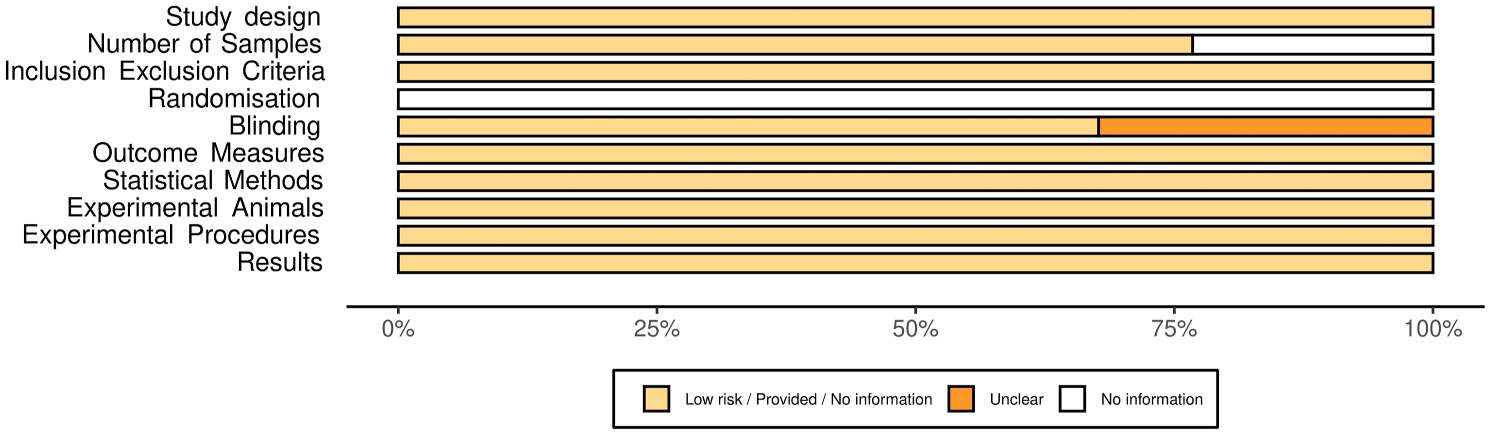
ARRIVE quality assessment.
Discussion
Saphenous vein graft IH remains a major problem for patients undergoing CABG, despite many years of research. It is accepted that IH is a chronic inflammatory disease that is associated with the proliferation and migration of SMC from the media to the intima coupled with MMP changes.1,2 However, there remain significant gaps in our understanding of the complex processes that take place when a vein is implanted into arterial circulation. While cellular models can be used and undoubtedly yield useful data,105–107 the comparatively simplistic nature of these systems makes insights gained from such models limited when it comes to translation. Considering unfeasibility of studying vein grafts disease temporal progression and mechanisms in the human body directly, different small and large animal models were developed as a surrogate. Large animal models complement small animal studies with the added value of longer lifespan, better size match, and the fact that they are genetically more closely related to humans.
The most common two large animals used are the dog and porcine model. Most of the studies attempted a simplistic vein interposition grafting of a segment of vein to arterial circulation which although useful does not truly represent the end to side anastomosis in the human body. Very limited work been carried out using an end to side model between a vein and a coronary artery in large animals, and this can be related to the difficulty of carrying out such a procedure and recovering these large animals for a prolonged period. In addition, it is important to remember that there are different genetic differences that exist among these animal groups and humans and that genetic regulation and interplay can differ. 108 However, it seems that the canine, porcine, and sheep immune system shares many similarities to that of the human system, making them a very appealing model to study inflammatory responses.109–111 Moreover, in pigs, intravenous or intralymphatic cannulations can be performed and blood or lymph samples taken for several days without the stress effect that is present in restrained rodents or sheep, for example. 110
Despite such limitation, the use of large animal models has been instrumental in improving our understanding of the disease progression as their size is a particular advantage for physiological models such as cardiovascular diseases. They are also outbred and, therefore, representative of population diversity. Furthermore, it allowed the use of different therapeutic interventions to modulate the inflammatory processes or suppress SMC activity to try to modulate IH.
Over the years, many encouraging results from animal studies failed to translate into human with the exception of very few such as the early work by Weglarz et al. in a study that aimed to assess plaque formation in saphenous vein grafts (SVGs) covered by an external Dacron stent in comparison with the classical technique which showed inferior results when using the external stents. 112 More encouraging results were reported in the VEST trials and others which showed that external stenting mitigates saphenous vein graft remodeling and significantly reduces diffuse intimal hyperplasia and the development of lumen irregularities after coronary artery bypass surgery.113–116
The selection of the most appropriate model is not an easy task and need to take into account the disease studied, available funding, and most importantly the 3 Rs (replacement, reduction, and refinement). 117 The 3 Rs concept should be essential when considering the use of animals especially in the current era where alternative ex vivo perfusion systems and different bioreactors are available. These are capable of mimicking some of the complex hemodynamic conditions related to vein grafting and allow the administration of different treatments or sampling the vein graft at different time points, thus allowing for at least partial replacement and reduction by focusing the research at specific time points, resulting in the reduction of animals required. 118
Supplemental Material
sj-pdf-1-prf-10.1177_02676591221091200 – Supplemental material for Large animal model of vein grafts intimal hyperplasia: A systematic review
Supplemental material, sj-pdf-1-prf-10.1177_02676591221091200 for Large animal model of vein grafts intimal hyperplasia: A systematic review by Oluwatomini Fashina, Riccardo G Abbasciano, Liam W McQueen, Shameem Ladak, Sarah J George, Sadeeh Suleiman, Prakash P Punjabi, Gianni D Angelini and Mustafa Zakkar in Perfusion
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.