
Abstract
Background
Del Nido cardioplegia (DNc) was designed for superior myocardial protection during cardiopulmonary bypass (CPB). We conducted a retrospective review to explore if DNc was associated with increase in systemic ventricle dysfunction (sVD) following pediatric CPB.
Methods and Results
This single-center, retrospective study included 1534 patients undergoing CPB between 2013 and 2016, 997 prior to center-wide conversion to DNc and 537 following. The primary outcome was new postoperative ≥moderate sVD by echocardiogram. Secondary outcomes included sVD of any severity and right ventricular dysfunction. Data was evaluated by interrupted time-series analysis. Groups had similar cardiac diagnoses and surgical complexity. Del Nido cardioplegia was associated with longer median (IQR) CPB [117 (84–158) vs 108 (81–154), p = 0.04], and aortic cross-clamp [83 (55–119) vs 76 (53–106), p = 0.03], and fewer cardioplegia doses [2 (1–2) vs 3 (2–4), p < 0.0001]. Mortality was similar in both groups. Frequency of sVD was unchanged following DNc, including predetermine subgroups (neonates, infants, and prolonged cross-clamp). Logistic regression showed a significant rise in right ventricular dysfunction (OR 5.886 [95% CI: 0.588, 11.185], p = 0.03) but similar slope.
Conclusions
Use of DNc was not associated with increased in reported sVD, and provided similar myocardical protection to the systemic ventricle compared to conventional cardioplegia but may possibly impact right ventricular function. Studies evaluating quantitative systolic and diastolic function are needed.
Introduction
Cardioplegia allows for the cessation of cardiac activity and provides a bloodless field essential for cardiac surgery. Conventional blood cardioplegia is comprised of solutions high in potassium that inhibit propagation of myocardial electrical activity by inducing cardiac arrest while cells remain in a depolarizer state. The solution requires dosing every 20–30 min to provide myocardial protection. Nevertheless, concerns have been raised for postoperative ventricular dysfunction due to inadequate protection, resulting from accumulation of intracellular sodium and calcium, particularly during prolonged periods of cardiopulmonary bypass (CPB).
Del Nido cardiopleia (DNc) was developed as an alternative agent to deliver myocardial protection over an extended duration of CPB, usually with only a single dose. 1 Cardiac arrest is induced through myocardium hyperpolarization and result in lower metabolic activity. The solution was formulated to reduce intracellular calcium, scavenge circulating oxygen free radicals, and reduce myocardial injury and edema. Del Nido cardioplegia is now used in numerous North American pediatric cardiac surgical programs, although there is little clinical research supporting these advantages. 2
Del Nido cardioplegia was implemented as the exclusive cardioplegia agent at the Hospital for Sick Children in 2015 based on a concensus and preference of the Division of Cardiac Surgery. Following its introduction, the frequency of postoperative ventricular dysfunction and associated sequelae continued to be observed. This study was undertaken to evaluate the impact of DNc on myocardial protection and new postoperative ventricular dysfunction. We hypothesized that DNc was not associated with a reduction in the frequency of new postoperative dysfunction of the systemic ventricle.
Patients and Methods
This retrospective, single-center study included all children (<18 years old) who underwent cardiac surgery with CPB between 1 January 2013 and 21 December 2016 at the Hospital for Sick Children, Canada. Patients were excluded if undergoing heart or lung transplantation. The institutional research ethic board approved the study and waived the need for patients’ consent. Demographic and surgical data were extracted from the cardiovascular surgery databases, and cardioplegia parameters were manually recorded from clinical perfusion records.
Cardioplegia and perfusion practices
Conventional cardioplegia was comprised of a customized blood cardioplegia solution based on the Plasma-Lyte 148 solution (Baxter, Deerfield, Illinois), to which glucose, potassium chloride, and magnesium sulfate were added. Base cardioplegia solutions were compounded by the inpatient pharmacy department and stored and delivered at 4–6oC. Dextrose, insulin, and bicarbonate were added to the base solution in the operating room immediately prior to surgery (Supplementary Table 1). On rare occasion, insulin and dextrose were excluded from repeated cardioplegia doses, when large volumes for body size of cardioplegia were delivered or in the event that early electrical recovery or persistence of electrical activity was observed. The base solution was diluted in blood, at a crystalloid-blood ratio of 1:2, and administered at an initial dose of 30 mL/kg, (maximum of 1L). Higher doses were given in setting of significant aortic valve incompetence and patients requiring direct coronary or retrograde delivery. Doses of 20 mL/kg were repeated at 20 min intervals or earlier if electrical activity was observed. For direct coronary injections, 7–10 mL/kg and 5–7 mL/kg were delivered down the left and right coronary arteries, respectively. The core temperature was allowed to drift 34°C, and active cooling used only when hypothermia to <32°C was indicated for the procedures.
Del Nido cardioplegia was introduced in August 2015 and used nearly exclusively thereafter. Del Nido cardioplegia was diluted in blood (4:1 crystalloid-to-blood) and delivered at 8°C. The initial dose of DNc was 20 mL/kg (maximum of 1 L), with repeated doses provided at 10 mL/kg, after approximately 40–60 min. For patients not requiring hypothermia, a core temperature of 34°C was initally targeted; gradually within the DNc era, patients with an anticipaited aortic cross-clamp time exceeding 60 min were cooled to 32°C.
Cardiopulmonary bypass circuits consisted of a Sorin S5 roller pump (Mirandola, Italy) with Sorin tubing packs (P.h.i.s.i.o-coated), and Maquet Quadrox i oxygenators (Getinge, Sweden) with hard-shell venous reservoirs (Softline–coated). Cardiopulmonary bypass prime consisted of PlasmaLyte A, 25% albumin, Manitou (0.25 g/kg), heparin (4 units/ml), cefazolin (30 mg/250 mL prime), 10% calcium chloride (targeting an ionized plasma calcium level of 0.3–0.5 mmol/L), and 8.4% sodium bicarbonate (20 mL/L). Packed red blood cells were used to maintain a hematocrit of >25%. Fresh frozen plasma was used for patients weighing <10 kg. Blood flow on CPB was maintained at 120–200 mL/kg for patients under 10 kg and 2.4–3.2 L/m2 for those above 10 kg. Continuous ultrafiltration was used on cases using Sorin DHF hemoconcentrators. Modified ultrafiltration was performed following CPB on patients weighing less than 15 kg or undergoing the Fontan operation. Alpha-stat blood gas management was predominantly used and shifted to a modified pH-stat strategy only when undergoing deep hypothermic circulatory arrest (DHCA). The cardioplegia temperature was controlled using the Sorin BCD Vanguard device (LivaNova PLC, London, UK) heat exchanger.
Outcomes
The primary outcome was the frequency of new moderate or greater dysfunction of the systemic ventricle (SVdys) reported on the echocardiogram immediately prior to hospital discharge. The pre-discharge study was selected as ongoing dysfunction would indicate a degree of persistent myocardial injury that was not influenced by perioperative inflammation and associated confounders. The dichotomous outcome was derived from the global assessment of ventricular function that was originally reported according to a six-point ordinal scale ranging from normal to severely reduced: 1) normal, 2) mild, 3) mild-moderate, 4) moderate, 5) moderate-severe, and 6) severe dysfunction. Quantitative measures of ventricular dysfunction (ejection fraction and fractional shortening) were missing from many studies and could not be used. Echocardiographic images were obtained by dedicated technologist and fellow trainees and were reported by a limited number of subspecialty cardiologists. Secondary outcomes included new SVdys in the intraoperative echocardiogram or in any postoperative study, and moderate or greater dysfunction of the right ventricle (RVdys)—in context of biventricular physiology—reported in any postoperative echocardiogram. The possible impact of acute and dynamic intraoperative loading changes on function assessment precluded its use as a primary outcome.
Statistical analysis
Descriptive data were presented as means and standard deviation, median and interquartile range, or frequency and proportions as appropriate. To describe the post-surgery outcomes, the proportion of patients with SVdys/RVdys were estimated and visualized over calendar time applying locally weighted scatterplot smoothing (LOWESS) to patient-level data, stratified by the period before and after the introduction of DNc. The data were visualized over the entire period (4 years) do identify general trends in the proportion of SVdys/RVdys, even prior to the introduction of DNc.
Time series data were then constructed, on a monthly basis, by aggregating the surgeries in which the patient developed the outcome postoperatively with the overall number of surgeries at that timepoint. Only surgeries completed after March 2014 were included to allow equal weighting of monthly proportions (i.e., 17 months before and after the introduction of DNc). The monthly proportions of surgeries with postoperative SVdys/RVdys were evaluated using interrupted time series analysis, 3 and an autoregressive regression model was applied to assess and quantify the impact of the introduction of Del Nido cardioplegia. The interrupted time series were implemented using autoregressive regression, in which DNc introduction and calendar time, centered at August 2015, were independent variables. Linear trends of the incidence rate before and after the introduction of the DNc were assumed. The 95% CIs and p-values were calculated using robust standard errors. A Durban–Watson test was used to assess the model fit.
The analyses assumed a significance level of 5% and were implemented using R v3.4.1 and SAS v9.3.
Results
Demographics and surgical characteristics.
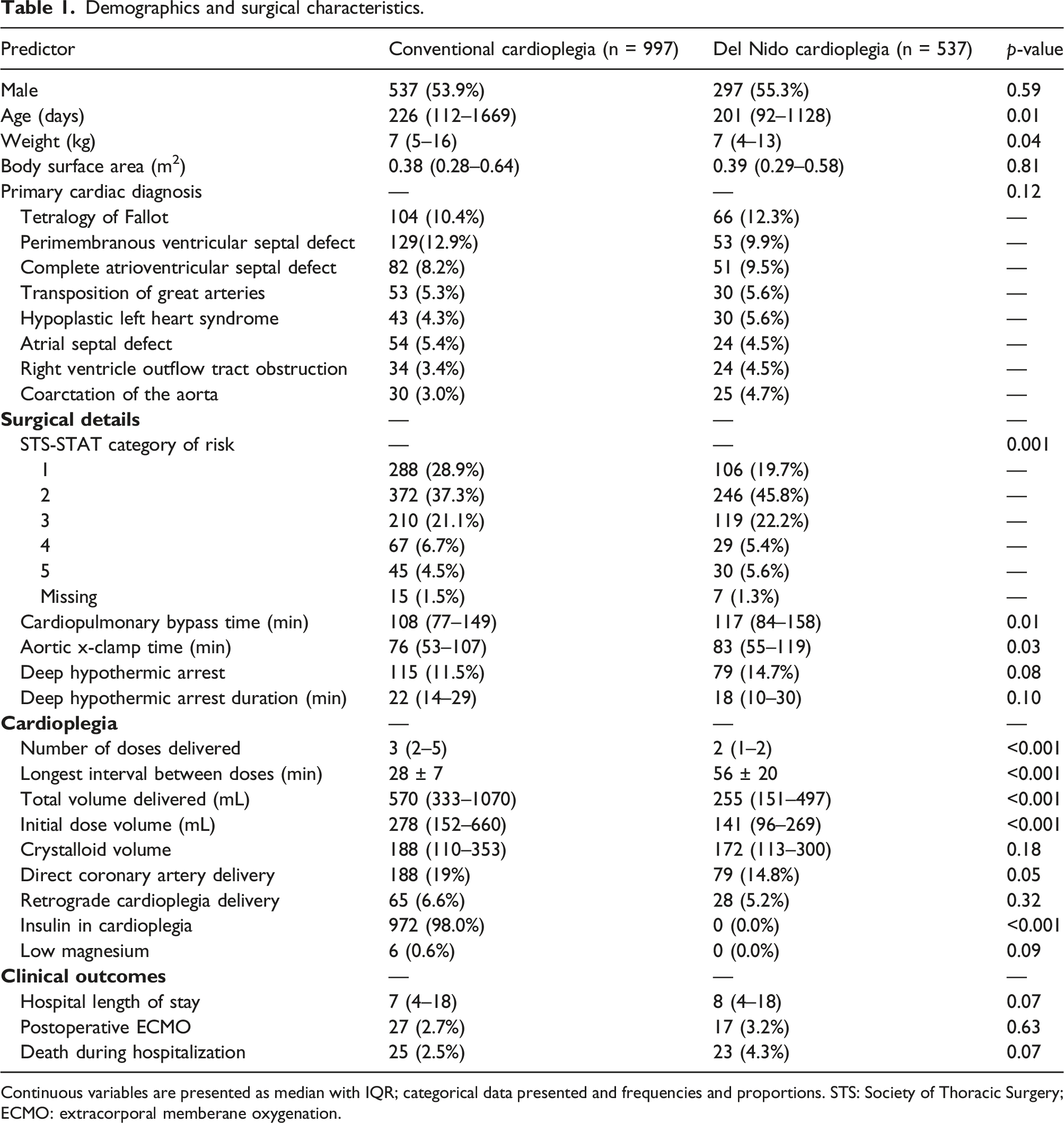
Continuous variables are presented as median with IQR; categorical data presented and frequencies and proportions. STS: Society of Thoracic Surgery; ECMO: extracorporal memberane oxygenation.
Delivery of DNc was associated with fewer doses of cardioplegia delivered over longer intervals. The Del Nido cardioplegia group received a median (IQR) of 2 (1–2) doses of cardioplegia on average (SD) every 56 ± 20 min, compared to 3 (2–4) every 29 ± 8 min in the conventional group. Route of cardioplegia delivery did not differ across the groups. Insulin was used exclusively (98.4%) in conventional cardioplegia.
Primary outcome
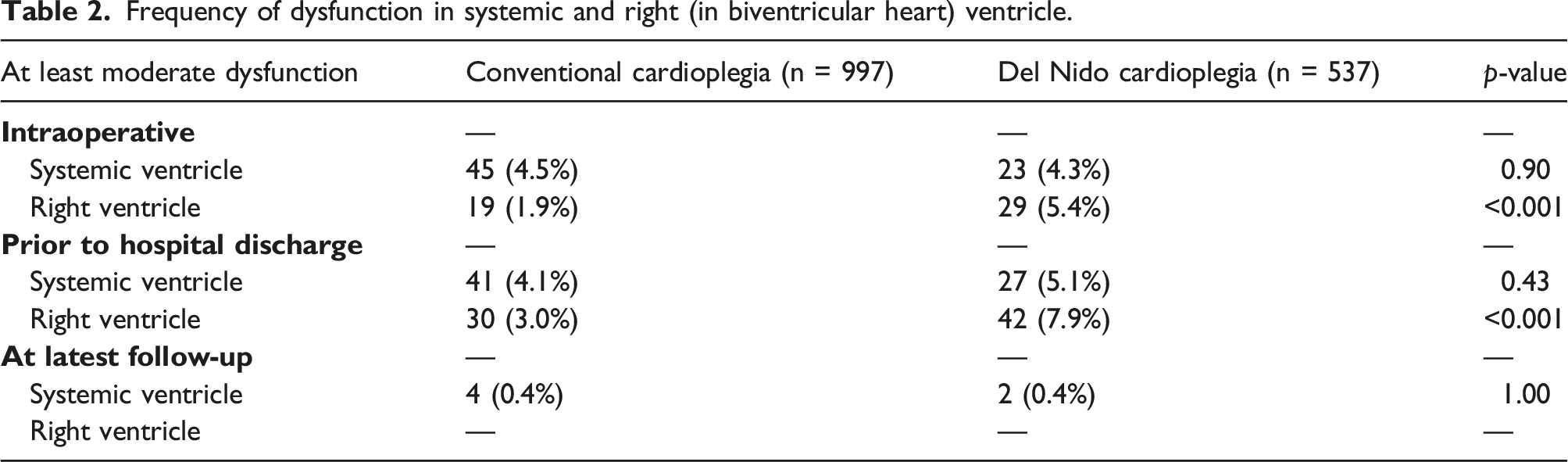
Frequency of dysfunction in systemic and right (in biventricular heart) ventricle.
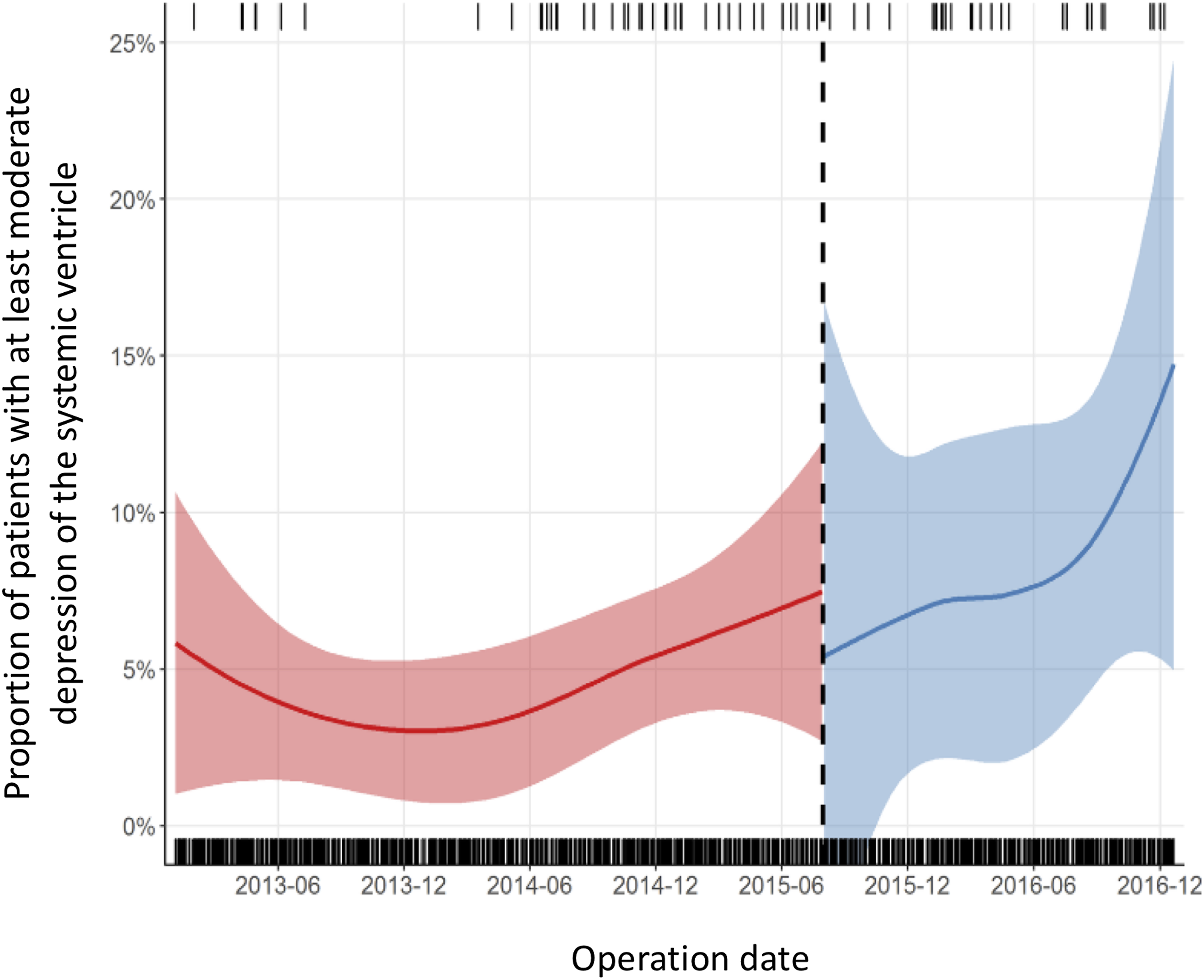
Stratified by the date of the introduction of DNc (dashed line), the proportion of operations in which patients experienced at least moderate postoperative depression of the systemic ventricle.
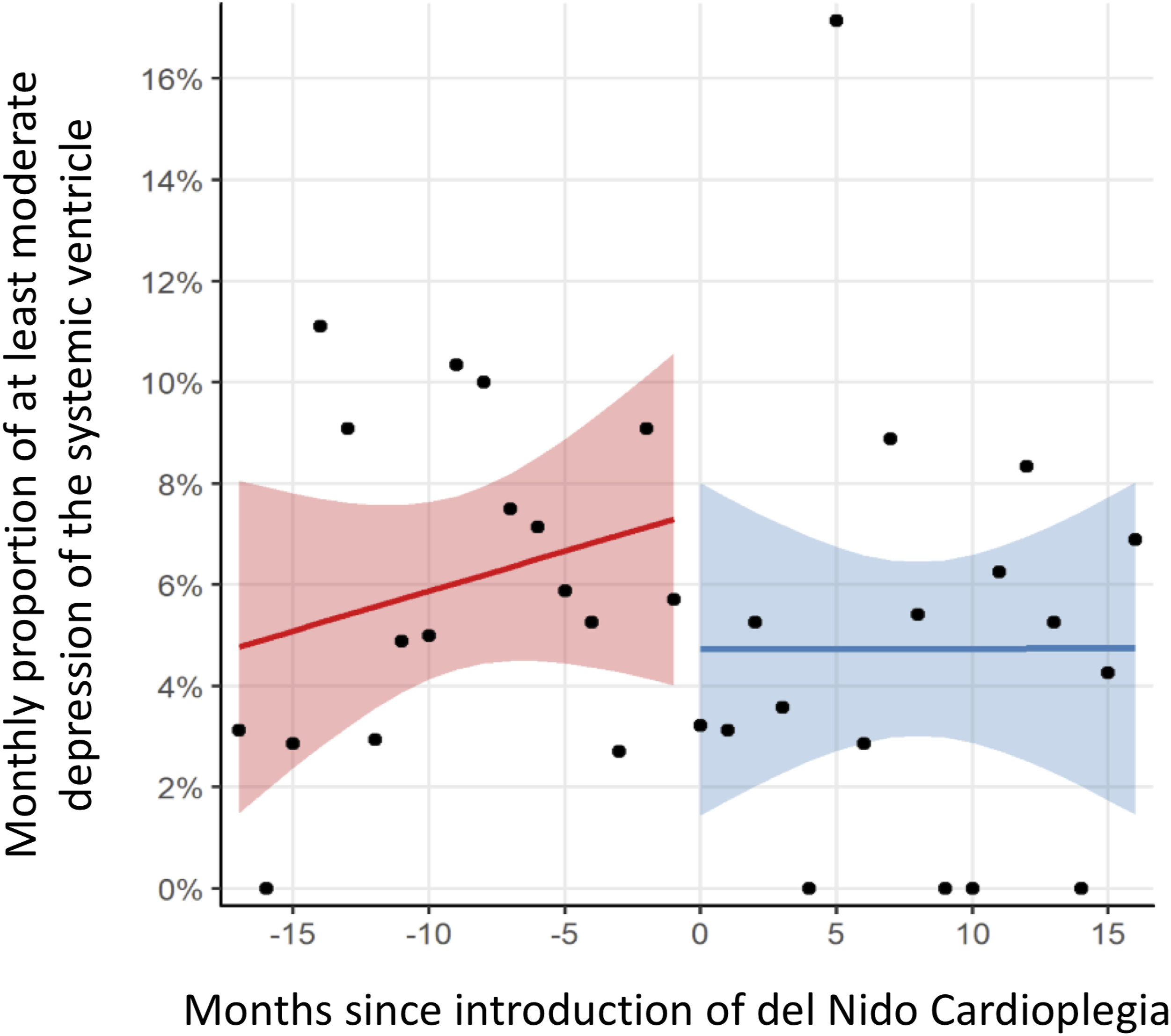
Regression model of monthly proportion of patients with at least moderate postoperative dysfunction of the systemic ventricle prior to hospital discharge before and after introduction of DNc.
Secondary outcomes
Del Nido cardioplegia was not associated with a change in intraoperative SVdys, with a frequency of 4.5% (N = 45) and 4.3% (N = 23) in the conventional and DNc groups (p = 0.90), respectively. Similarly, the interrupted time-series analysis of intraoperative SVdys suggested that DNc was not significantly associated with an immediate change in the primary outcome (coefficient (95% CI) = 0.2% (−5.8%–6.2%), p = 0.94), nor a difference in the time trend (95% CI) of the monthly proportions (0.1 (−0.5–0.7), p = 0.80) groups. (Figure 3) The findings were consistent across all previously identified high-risk groups. Regression model of monthly proportion of patients with at least moderate dysfunction of the systemic ventricle in the immediate postoperative echocardiogram before and after introduction of DNc.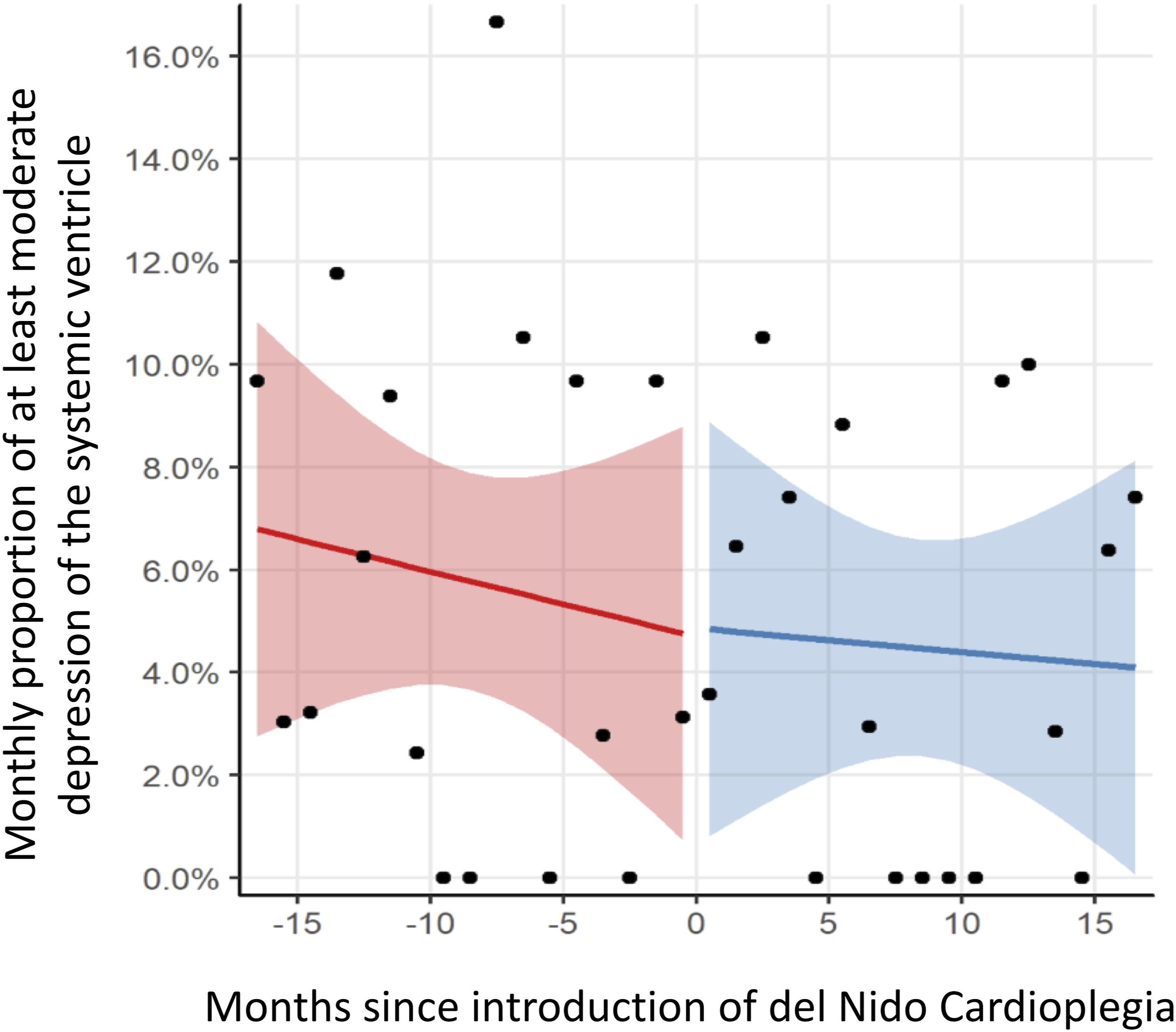
The overall frequency of RVdys trended higher following introduction of DNc (conventional 4% (N = 22) vs DNc 7.8% (N = 42), p = 0.06). Unlike SVdys, the monthly proportion of subjects with RVdys was stable prior to the transition to DNc; DNc was associated with an immediate increase of 5.89% (95% CI = [0.59–11.18], p = 0.029) in right ventricular dysfunction (Figure 4). Regression models showed an immediate increase in RV dysfunction (coefficient (95% CI) 5.89 (0.59–11.18); p = 0.03) but the time trend of RV dysfunction in either era (conventional and DNc) remained flat. An increase in RVdys were also noted intraoperatively, with an immediate increase in RV dysfunction (coefficient (95%CI) 7.35 (2.76–11.94); p = 0.002) and flat time trends in both conventional and DNc groups. A) Stratified by the date of the introduction of DNc (dashed line), the proportion of operations in which patients experienced at least moderate postoperative depression of the right ventricle, and B) regression model before and after introduction of DNc. The dashed line indicates the date of the initiation of DNc.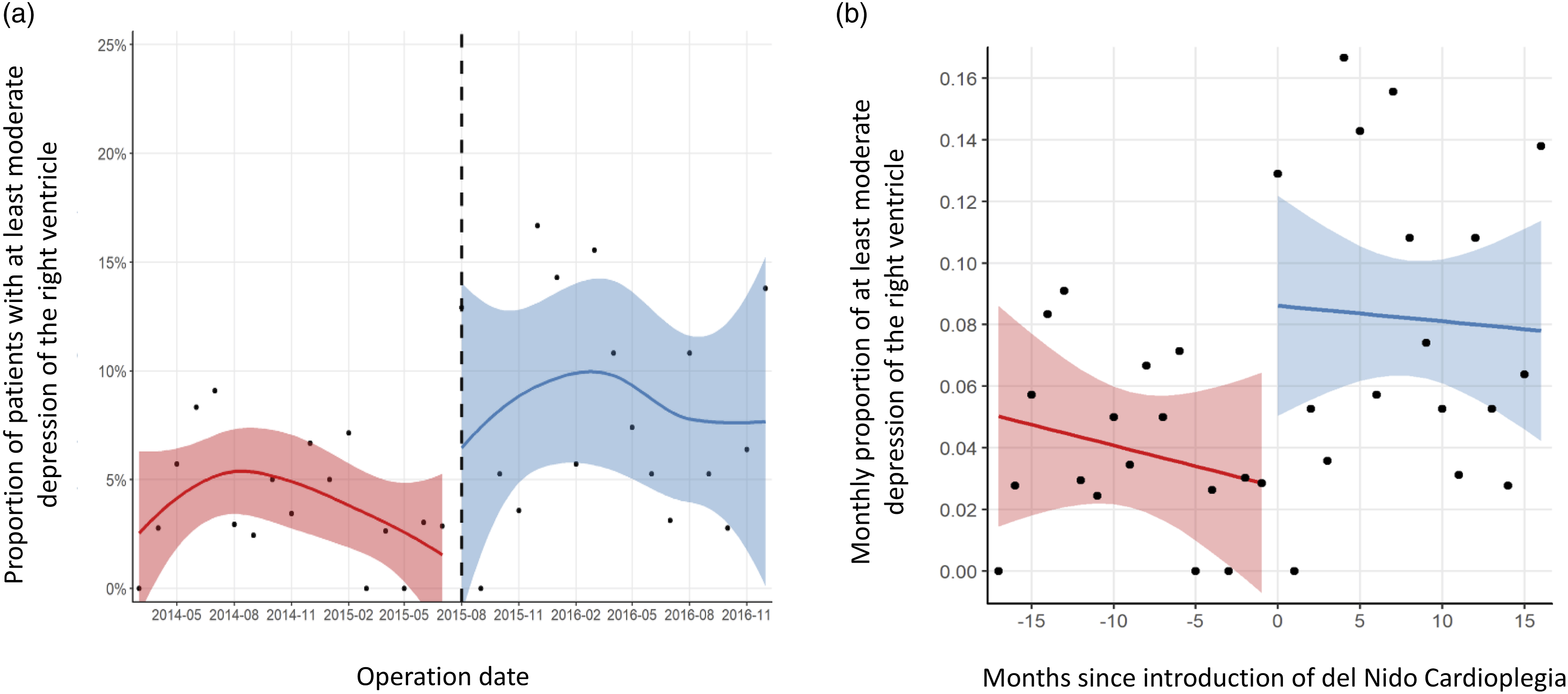
Del Nido cardioplegia was not associated with a change to postoperative ventricular dysfunction when including patients with new mild or mild-moderate ventricular dysfunction. Hospital length of stay, postoperative ECMO support, and mortality remained unchanged following introduction of DNc. (Table 2)
Discussion
Del Nido cardioplegia was developed as a single-dose agent to optimize myocardial protection, reduce injury and lower frequency of ventricular dysfunction. Our data suggests that the introduction of DNc during pediatric CPB surgery was not associated with a change in SVdys and a possible increase in RVdys, without a trend effect when compared to conventional cardioplegia use.
Postoperative SVdys in children who had normal preoperative function could be a consequence of inadequate myocardial protection. Injury arises from ischemia-reperfusion that triggers a high intracellular calcium and elevated oxygen free radicals. A time-dependent relationship exists between CPB and aortic cross-clamp and severity of myocardial injury, as longer intraoperative exposure is associated increased edema, higher frequency of low cardiac output, and the level of hemodynamic support. 4 The impact can have longstanding consequences leading to remote myocardial fibrosis and adverse ventricular remodeling.5,6 Nevertheless, producing cardiac standstill is unavoidable for the repair of complex congenital heart disease. DNc was designed to reduce the harmful metabolic effects of cardioplegia by arresting the heart in a hyperpolarized state, thereby reducing the trigger for intracellular calcium influx and lowering intracellular calcium accumulation.1,7 Lidocaine limits intracellular sodium and calcium buildup, and its impact is mitigated through the direct inhibition of magnesium sulfate; the use of bicarbonate reduces acidosis, and mannitol is added to reduce myocardial edema and scavange oxygen free radicals.
Despite its wide adoption, there is limited clinical evidence to support the proposed advantages of DNc in CPB surgery. In the largest pediatric randomized study of 100 children under 12 years undergoing repair of ventricular septal defect or tetralogy of Fallot, DNc was associated with higher cardiac output, an attenuated inflammatory response and less myocardial injury. 8 In contrast, smaller studies showed similar levels of inflammatory cytokines, myocardial injury biomarkers, and clinical outcomes.9,10 The observed benefits were attributed to the DNc solution, but the discrepancies across studies may actually highlight the clinical impact of reducing CPB time. 11 All the studies included patients with relatively low surgical complexity undergoing similar cardioplegia management strategies; however, the favorable clinical and biochemical results were demonstrated with a reduction in median CPB time of over 10% from conventional cardioplegia (p < 0.01). The benefits disappeared when including younger patients undergoing surgery with CPB and Aortic cross-clamp times that were approximately 1.5 and 2 times longer, respectively. In comparison, our study included mainly children undergoing the entire spectrum of surgical procedures. Use of DNc benefitted from fewer doses of cardioplegia over longer intervals and delivering less cumulative volume; nevertheles, despite similar surgical complexity, consistent surgical teams, and use of deep hypothermic circulatory arrest, CPB was longer by nearly 10 min and aortic cross-clamp by 7 min. The clinical relavence of this finding remains unclear, but, despite this, the frequency in postoperative ventricular systolic dysfunction was unchanged when compared to the preceding era using convertional cardioplegia. This increase also introduces the possibility of significant confounding, but both cardioplegia solutions were used in the same era during which we could not discern a difference in the range of surgical procedures or patient-level factors; during the time period, there was a no turn-over in surgical staff nor a major change in surgical management and decision making.
The observed trend of right ventricular impairment may be a reflection of increased surgical duration, including CPB and aortic crossclamp, rather than source of cardioplegia. Provision of adequate myocardial protection of the right ventricle in the setting of congenital heart disease is often challenged by ventricular hypertrophy and suboptimal temperature control of the anterior chamber, and therefore more vulnerable than the left ventricle to minor changes of CPB.12,13 Studies on the impact of DNc on right ventricular function are limited, but a small, randomized study suggested DNc was associated with a similar decline in echocardiographic signs of right ventricular function when CPB times were comparable to blood cardioplegia. 14 The findings of our study are unlikely to result from deleterious augmentation to right ventricular afterload secondary to respiratory dysfunction and positive pressure ventilation as the pre-discharge echocardiograms were usually completed on the cardiology floor once the patients were breathing spontaneously off supports.
Many surgical services have transitioned to DNc due to its induction of prolonged arrest by a single dose.1,2 Unlike the previous randomized studies,8-10 a median of two doses of DNc were provide at our institution. Initially, DNc was repeated after at most 60 min, and based on the discretion of the cardiac surgeon on a case-by-bases. Nevertheless, in response to emerging clinical concerns for ventricular dysfunction associated with poor DNc myocardial protection, institutional practice shifted to administer DNc every 40 min and cool the patient to 32oC whenever the aortic cross-clamp time was anticipated to exceed 60 min. The in vivo impact of this multi-dose DNc strategy is unclear; however, animal models have shown similar troponin leak and lower stroke volume and left ventricle pressure generation compared to single dose. 15 Redosing of DNc may only be necessary following 90 min of ischemia. 16
Previous cardioplegia-based studies focused on surrogate markers of myocardial injury, mainly biomarkers. 17 This study focused entirely on the association of DNc on ventricular systolic function, a standardized variable measured universally and reported in all of our institution’s echocardiograms. The impact of DNc on ventricular relaxation was not explored due to inconsistent capture of diastolic echocardiographic parameters, particularly in the imaging of low risk patients; however, clinical benefit may be conferred from the lower intracellular diastolic calcium concentrations associated with DNc in in vitro studies. 7 A strong link has been established between intracellular calcium accumulation following ischemia-reperfusion models, 18 and may explain the increased morbidity seen in those with diastolic dysfunction following adult CPB surgery. 19 The complicated early postoperative course associated with restrictive physiology following tetralogy of Fallot is well described; however, the clinical impact in pediatric CPB is not well understood.
This study has a number of important limitations. An experimental design may have been preferred over the retrospective nature of this study; however, an exceedlingly large sample size would be required to power for low event rate of important clinical outcomes prompted previous randomized studies to limit their outcomes to biochemical levels (e.g., troponin) and cardiac output indices. 17 Clinical echocardiogram reports were used for semi-quantitative assessment of ventricular function. Left ventricular ejection fraction and fractional shortening, and right ventricle fractional area shortening were preferred but were missing from a large proportion of postoperative studies. The association between the introduction of DNc and ventricular function was examined through population-based analyses. The interrupted time series analysis examined the system and not necessarily the intervention. Although no other surgical initiative was launched during this period, the benefits of DNc may have been offset by another, unmeasured factor. Specifically, possible confounders including intraoperative and postoperative vasopressor and inotrope use and blood transfusions, neither which could be collected nor quantified. The study results may reflect the learning curve associated with the introduction of a new practice rather than the cardioplegia’s myocardial protection. The degree of myocardial protection during the DNc period may also have been affected by the shift in core temperature control during the DNc period.
Supplemental Material
sj-pdf-1-prf-10.1177_02676591211054978 – Supplemental Material for Comparison between Del Nido and conventional blood cardioplegia in pediatric open-heart surgery
Supplemental Material, sj-pdf-1-prf-10.1177_02676591211054978 for Comparison between Del Nido and conventional blood cardioplegia in pediatric open-heart surgery by Alejandro A Floh, Shubhadeep Das, Maruti Haranal, Peter C Laussen, Lynn Crawford-Lean, Chun-Po S Fan, Luc L Mertens, Kyle Runeckles and Osami Honjo in Perfusion
Conclusion
The use of DNc was not associated with a change in SVDys. Fewer DNc doses provided similar myocardial protection to the systemic ventricle compared to conventional cardioplegia, however, may have possible negative impact on right ventricular systolic function. Further studies evaluating quantitative systolic and diastolic function are warranted.
Footnotes
Acknowledgments
We are grateful to the entire team of Perfusionists who assisted in the extraction of all perfusion-related data elements.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
REB approval
2017-04-07 (Research Ethics Board, Hospital for Sick Children # 1000057220)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.