
Abstract
Myocardial protection during cardiac surgery is crucial for preventing ischemia-reperfusion injury and preserving myocardial function. Cardioplegia, a solution used to induce electromechanical cardiac arrest, is the fundamental method for myocardial protection during on-pump procedures. Del Nido cardioplegia, developed in the 1990s, has gained increasing popularity in adult cardiac surgeries over the past two decades. Del Nido cardioplegia is a crystalloid-based solution used to achieve depolarized arrest. Its mechanism of action also involves preventing intracellular calcium overload, a key driver of reperfusion injury. Numerous studies have evaluated the safety and efficacy of del Nido cardioplegia in adult cardiac surgeries, including coronary artery bypass grafting and valve procedures. Compared to standard blood cardioplegia, del Nido cardioplegia has demonstrated reduced hemodilution, transfusion requirements and shorter cardiopulmonary bypass times due to its extended arrest duration. Many studies have reported lower levels of myocardial injury biomarkers and improved myocardial functional recovery with del Nido cardioplegia. It has also been associated with reduced defibrillation requirements, which is attributable to the antiarrhythmic effects of lidocaine. While some studies have reported no significant differences in outcomes between del Nido cardioplegia and blood cardioplegia, others have favored del Nido cardioplegia in terms of myocardial protection, postoperative cardiac function, and perioperative morbidity. The choice between cardioplegia solutions remains subjective and dependent on surgeon preference and institutional practices. However, del Nido cardioplegia has emerged as an acceptable alternative to traditional cardioplegia, offering potential advantages in adult cardiac surgeries.
Keywords
Introduction
Despite surgical advances in today’s era, myocardial damage is still common. 1 Myocardial protection is a collection of techniques used to reduce myocardial oxygen consumption and alleviate the effects of ischemia-reperfusion injury. 2 In its broadest sense, myocardial protection refers to any drugs and strategies used to preserve or shield myocardial cell structural integrity from the damaging effects of its hypoxic state. 3
During cardiac surgery, when cardiopulmonary bypass is being utilized, administration of cardioplegia has been known as the fundamental method for myocardial protection. Selecting the type of cardioplegia plays a significant role.4–6 Cardioplegia enables a bloodless and reversibly motionless field during cardiac surgery.7–9 It is used to render the heart electromechanically quiescent and inactive, together with a reduction in metabolic demands and the attenuation of ischemia-reperfusion injury, 10 which is still an obstacle following cardiopulmonary bypass and cardioplegic arrest. 3
Cardioplegia was first developed in 1955. 11 With the conclusion of the 20th century, multiple distinct types of cardioplegia were introduced, each having its advantages and disadvantages. 12 St Thomas Hospital cardioplegia has, for the past few years, been widely considered to be the standard choice of cardioplegia for the adult population. 5 Del Nido cardioplegia has been demonstrated to be proven effective for infant and paediatric cardiac surgery since 1995. 13 Del Nido cardioplegia provides a long arrest period and was initially made to be used for neonatal and paediatric myocardial protection, due to its compatibility with the immature myocardium. The use of del Nido cardioplegia in adults has been successful and continuous since 2003. 14 It is being used in adult cardiac surgeries, such as coronary artery bypass grafting (CABG) and valve surgeries.13,15 Existing studies have proved that del Nido cardioplegia is preferable in terms of efficacy and myocardial protection.7,13,16,17 It especially helps to alleviate myocyte injury caused by intracellular calcium accumulation. 18
History of cardioplegia and the dawn of del Nido cardioplegia
Sidney Ringer, a clinician and physiologist, based in England, published a series of experiments in 1883 that demonstrated that potassium could lead to diastolic arrest. 19 Ringer’s research in 1894 showed cessation of myocardial function when a hyperkalemic solution was used to perfuse cardiac tissue. 20
Melrose carried out the first cardioplegic arrest in a canine model of cardiopulmonary bypass by utilizing 77 mmol/L concentration of potassium citrate and obtained positive results.12,19 Immediate cardiac arrest was established, and the heart underwent quiescence for 30 minutes before beginning to beat again. There was no myocardial damage or arrhythmias noticed when the electrical function was restored. Hence, Melrose et al. suggested that reversible cardiac arrest induced by high potassium citrate might improve the safety of cardiac surgery. 19 A reversible cardiac arrest produced using blood along with concentrated potassium citrate was briefly used in clinical practice in 1955. 20 Following this, in 1957, Dr Lam coined the term cardioplegia. 19
Soon, thereafter, the use of the Melrose technique was abandoned due to reports of rigor, dysrhythmias, and myocardial necrosis caused by the solution. 21 Hyperkalemic solutions were immediately connected to potassium-related cytotoxicity and were demonstrated to cause contractile dysfunction, ventricular fibrillation, and myocyte death in both experimental and human investigations. It was abandoned for a long time due to intense disagreement. Following this, different approaches, such as topical and deep hypothermia were utilized, however, these approaches did not provide better outcomes. 19
Since Melrose’s solution was discovered to cause myocardial necrosis and increased postoperative mortality, subsequent research and substance modification led to the emergence of cold, low potassium cardioplegia. 22 Several cardioplegic interventions were introduced throughout Europe in the 1960s by H.J. Brettschneider and U. Kirsch. 20 Brettschneider (1964) proposed a low sodium and zero calcium solution which included histidine, tryptophan and ketoglutarate as buffering and substrate adjuncts, as an additional option after almost 15 years of research. This is when, in 1975 Sondergaard et al. reported its successful use in 100 aortic valve surgeries with a low mortality rate. 23 Although it was intended for cardiac surgery, it was not frequently used and eventually found other purposes, like organ transplantation. 19
Soon, in the mid-1970s, both the UK and the USA witnessed the reintroduction of cardioplegic solutions with less than 40 mM of potassium content.19,23 It was re-established in the United States in 1970 by W.A. Gay and P.A. Ebert. 20 In the UK, Hearse and Braimbridge in London developed St Thomas cardioplegia which was used to cause diastolic arrest. 19
Therefore, cardioplegia with increased potassium concentrations has been used frequently since 1978. 20 Following this cold blood cardioplegia was introduced, 22 along with the Buckberg solution, which is a blood-based hyperkalemic cardioplegia and was the most common solution used around the globe. 19
Blood cardioplegia has been shown to produce less hemodilution and has the accompanying benefit of the presence of haemoglobin and dissolved oxygen, which provide optimum oxygen-carrying capacity. Therefore, during the interval of cardiac ischemic arrest, with blood cardioplegia more oxygen is delivered. 24 Systemic inflammatory response syndrome triggered by cardiopulmonary bypass appears to be diminished by blood cardioplegia, which brings about positive changes in systemic microcirculation and delivery of oxygen. 25
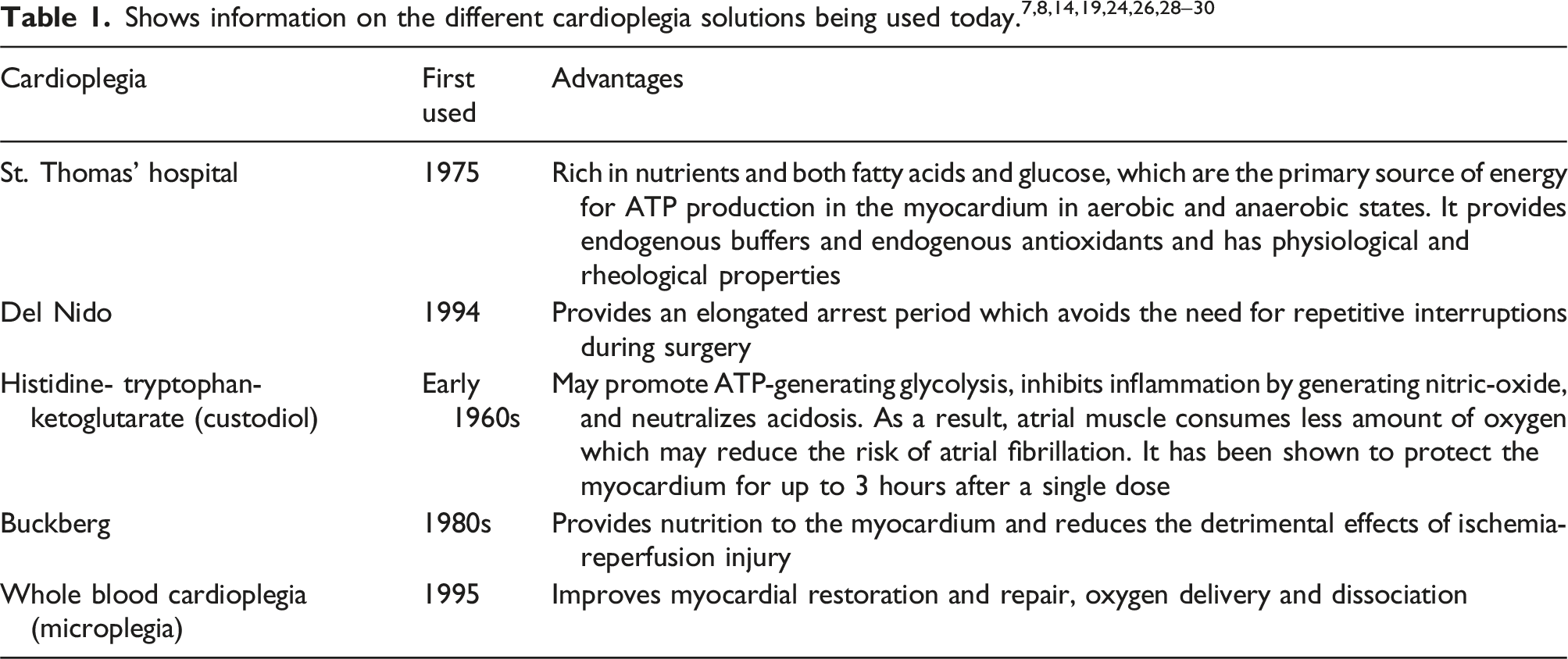
Early in the 1990s, researchers at the University of Pittsburgh, Pennsylvania, created a unique formulation for cardiac protection. 15 It was later patented by this team, which included Dr Pedro del Nido, Dr Hung Cao-Danh K, Dr Eric Sommers, and Dr Akihiko Ohkado.31,32 It was first used at the Children’s Hospital Boston in 1994. 32 One part of a patient’s oxygenated whole blood is mixed with four parts Plasma-Lyte A, which makes up the original del Nido cardioplegia, which was administered antegrade at a temperature of 8 °C–12 °C and a single dose was administered every 90 minutes.24,31
The researchers at the University of Pittsburgh did not have a well-defined delivery protocol, yet their outcome measurements were accurate and unique. They measured intracellular calcium, lactate buildup, intracellular buffering, and myocardial ATPs but the authors failed to mention the details of how they measured the parameters and the findings. 31
Ashlynn Ler et al. summarized that in recent years, the use of del Nido cardioplegia in adults has shown promising results with regard to safety and myocardial protection. It is used in various adult cardiac procedures, like CABG, aortic valve surgeries, and adult congenital repairs. 33
Del Nido cardioplegia and its constituents
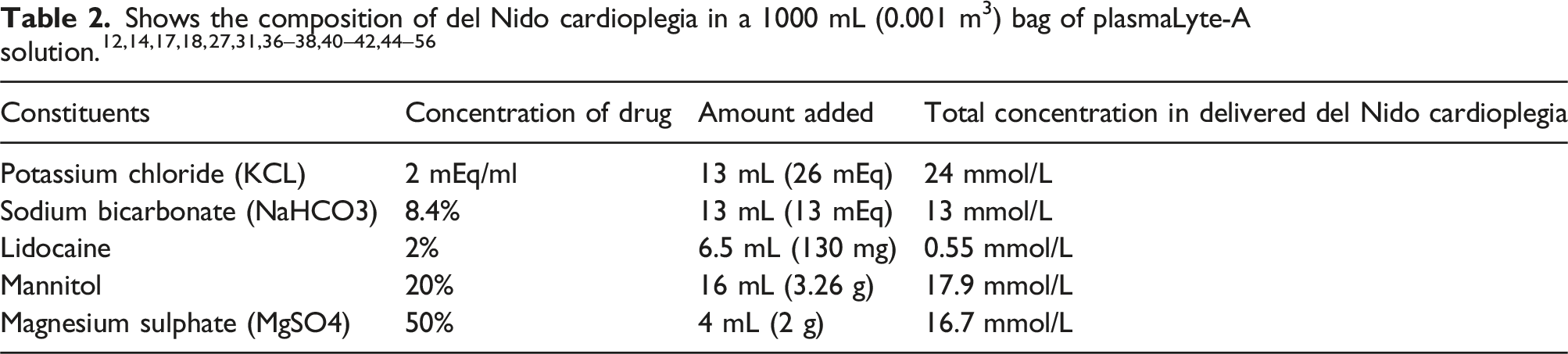
It has a pH of 7.4. 17 Potassium chloride is the main component as it provides depolarized arrest of the heart. 46 Even though the added concentration of potassium is 26 mmol/L, according to Matte et al. the delivered concentration would be 24 mmol/L after mixing and dilution with the crystalloid base and the one part of blood. 31 Bicarbonate acts as a buffer maintaining intracellular pH levels by scavenging excess hydrogen ions, while magnesium sulphate is a calcium channel blocker.12,31,34 It is important to note that del Nido cardioplegia excludes the addition of calcium to the base solution.12,31 Mannitol is an additive that is an osmotic diuretic used to prevent or decrease myocardial oedema and acts as an oxygen-free radical scavenger. 31 Lastly, lidocaine, previously known as lignocaine, the hallmark of del Nido cardioplegia, is a sodium channel blocker used as a cell membrane stabilizer, which assists in decreasing myocardial excitability and metabolism.7,12,32,34 It is important to ensure careful addition of lidocaine when preparing del Nido cardioplegia, since lidocaine may be toxic at higher concentrations.
Del Nido cardioplegia when compared to other blood-based cardioplegia produces a longer arrest period due to the presence of magnesium and lignocaine which has a longer half-life.7,46 Del Nido cardioplegia contains one part of blood and the apparent benefit of using blood to deliver cardioplegia is that it keeps the heart nourished during arrest and permits renewal of contents upon redosing of the solution. The solution itself precisely corresponds to the components of the blood that are necessary for the best possible reperfusion of the ischemic heart. 57 Del Nido cardioplegia, which contains mostly crystalloid as opposed to blood cardioplegia, supplies modest quantities of calcium ions to prevent excess calcium loading; This trace calcium in cardioplegic solutions is preferable as compared with acalcemic levels. 8
Mechanism of action
Achieving quick onset of isoelectric line and demonstrating adequate myocardial protection, restoration to sinus rhythm, and minimal adverse effects are the ideal characteristics of cardioplegia. 8 Del Nido cardioplegia causes depolarization in phase 0 of the action potential by preventing the voltage activated sodium spike. 7 Hyperkalemic depolarized arrest has negative effects which can be avoided by polarizing the myocytes to a certain extent. 17 It arrests the heart for a period ranging from 45 minutes to almost 180 minutes, on average a good 90 minutes on a single dose.5,17,37,47,58 A dose of 20 mL/kg is administered but it is given at a maximum of 1000 mL (0.001 m3). 32
Cardioplegia is categorized broadly into two; extracellular and intracellular solutions. Del Nido cardioplegia being extracellular, alters the resting membrane potential of the myocytes, inactivating the voltage-dependent sodium channels due to which the sodium entry into the cells does not occur, which inhibits the generation of an action potential, producing an arrest of the myocardium. 6 The cessation of the generation of action potential and resultant contractions also lead to a decrease in the metabolic activity of the heart. 59 Reduced potential difference between the cell’s inner and outer membranes and a rise in potassium content outside the cells are two effects of administering cardioplegia because sodium is unable to pass through the membrane inside, hence the heart is stopped in its diastolic phase. Anomalies in the sodium and calcium ionic gradients and calcium overload within the cells arise from certain sodium currents continuing to function as “window” currents at depolarized potentials and thereby prevent the heart from recovering. Additionally, myocardial cell oedema is countered by the hypertonic nature of mannitol.3,60 All of these collectively are beneficial for the restoration of the heart’s natural rhythm. 9
However, depolarization of the heart cell membrane caused by hyperkalemic arrest prevents the sodium-potassium ATPase from functioning, causing a buildup of intracellular sodium ions. Eventually, the sodium-calcium channel facilitates the intracellular accumulation of calcium leading to myocardial damage. Thus, a high dose of lidocaine counteracts the negative effects of hyperkalemic arrest on myocytes, prolonging the cardiomyocyte’s refractory period and increasing the electrochemical gradient of potassium-induced depolarized state of the membrane. This prevents the intracellular buildup of sodium and calcium ions by suppressing the sodium-calcium channels, which reduces ATP utilization by the cardiomyocytes. The presence of concentrated lidocaine also makes it possible to maintain asystole for an extended period. 35
The use of potassium to arrest the heart is key to preserving intracellular ATP levels. 61 Lidocaine inhibits or blocks the sodium channels that participate in the sodium window current. This helps decrease calcium influx during cardiac arrest, reducing calcium accumulation, and hence provides improved postoperative outcomes in relation to ischemia-reperfusion injury.37,45 Lidocaine blocks the influx of sodium ions thus indirectly inhibiting the sodium-calcium antiporter which allows quick resumption of myocardial function with increased contractility.15,62
The properties of lidocaine combined with magnesium ions provide a distinguished ability to preserve ventricular function, which reduces myocardial oedema. Thus, forming the fundamental mechanism behind del Nido cardioplegia. 37 Deceased myocardial injury in calcium-sensitive immature myocardium with the use of del Nido cardioplegia has been described. In the same way, an aged myocardium is also said to be susceptible to intracellular calcium overload. 59 The mature myocardium post myocardial ischemia is said to be more susceptible to calcium overload and hence myocardial injury. This is due to the weak sodium and calcium channels’ function, which leads to the calcium ions moving into the mitochondria causing mitochondrial damage and energy depletion in the myocytes, leading to contractile dysfunction. 63 The calcium ions, their accumulation, and intracellular overload play a vital role in the negative effects of ischemia-reperfusion injury and therefore myocardial damage. 14 Since we mix crystalloid with 20% blood, myocardial ischemia-reperfusion injury can be reduced in patients undergoing extracorporeal circulation, leading to a reduction of inflammatory mediators released into the systemic microcirculation. 25
Global status of del Nido cardioplegia
Del Nido cardioplegia was introduced in the 1990s, approximately 25 years before the first extensive study was conducted which compared the efficiency of del Nido cardioplegia against cold blood cardioplegia. 12 Since the early 2010s, many institutions transitioned to the use of del Nido cardioplegia in adult cardiac surgery, College of Physicians and Surgeons of Columbia University, New York Presbyterian Hospital being one of the first in 2011. 64 Of the articles we reviewed, four institutions all from different countries, one being India, transitioned to del Nido cardioplegia in 2017 (Figure 1).7,11,48,63
Govindapillai et al. conducted a study on isolated rat hearts to show the effect of del Nido cardioplegia on aged hearts. They noted the following advantages:
62
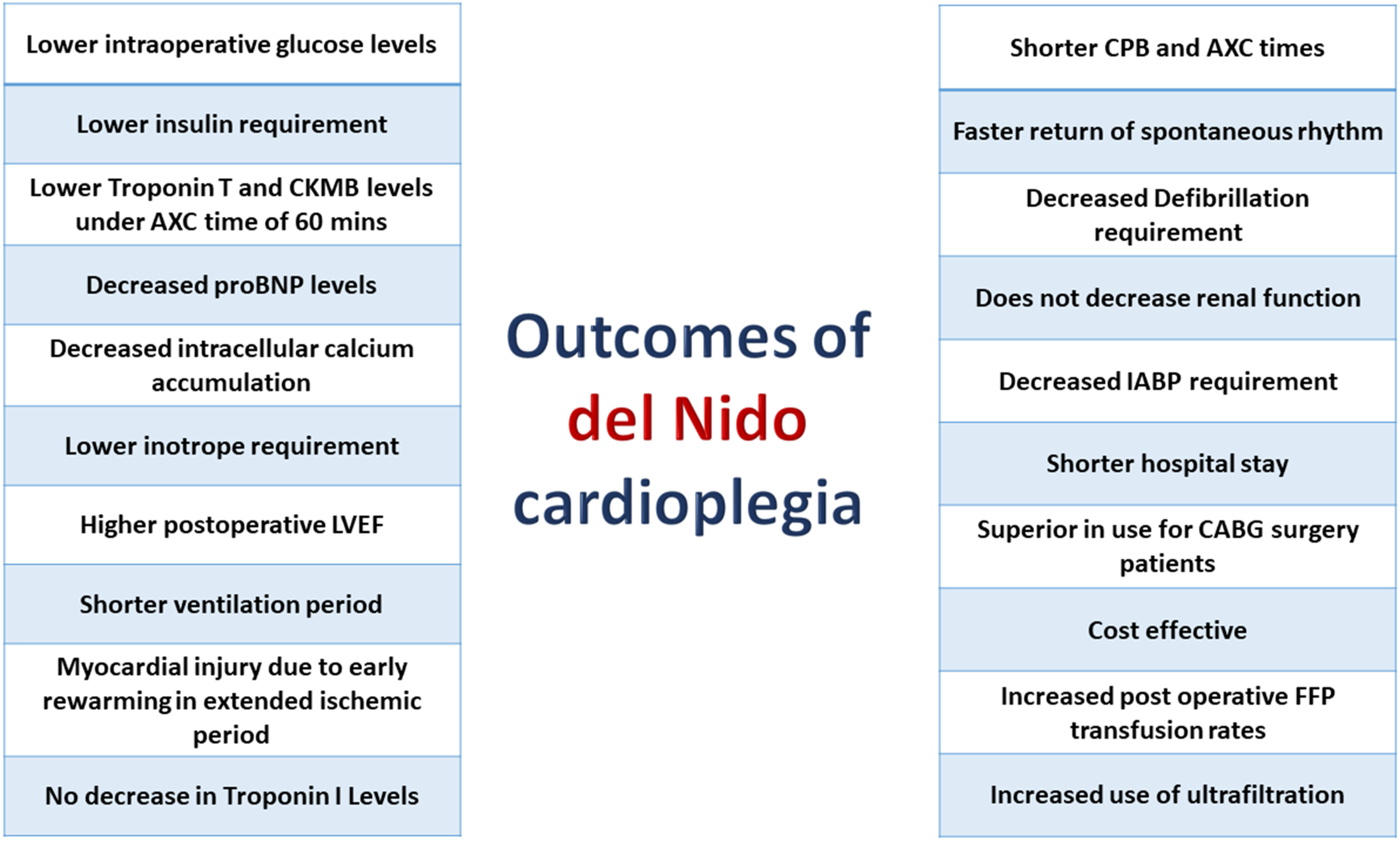
• Lidocaine decreases the negative effect of the sodium window current • Causes reduced spontaneous return of activity during the arrest period • Delays return of activity after cross-clamp removal • Results in decreased coronary vascular resistance • Produces decreased myocardial damage • Can cause better functional recovery after cardioplegic arrest • Myocardial oedema is unaffected by cardioplegia Outcomes of del Nido cardioplegia.
Ischemia-reperfusion injury
The use of del Nido cardioplegia in adult patients was begun based on the hypothesis that the old and the infant population both share similar myocardial characteristics and that the enhanced calcium handling of del Nido cardioplegia is beneficial for the adults through that theory. 5 Del Nido cardioplegia provides long ischemic periods which enables the surgeons to perform uninterrupted work. 4 Ischemia causes myocardial cells to convert from aerobic to anaerobic metabolism causing lactate buildup and acidosis. Myocardial dysfunction occurs due to calcium ion hemostasis alterations. Longer ischemic periods further deteriorate myocardial cellular function and eventually lead to cell death without timely reperfusion. Reperfusion being essential to restore the myocardial function to normality, paradoxically causes ischemia-reperfusion injury which occurs in the post-ischemic period and is caused by the production of reactive oxygen species, calcium, and inflammatory cell accumulation. 12
Even though it was not described in their clinical outcomes, Lenoir et al in their comparative study on adult aortic valve surgery patients, concluded that myocardial injury may occur with del Nido cardioplegia along with prolonged ischemia. 46 One of the reasons may be that much of the solution will have been drained away from the coronaries after an extended ischemic period and the heart will have a warmer environment under bright operating lights. 32
Accumulated calcium during the cardioplegic phase plays an important role in reperfusion injury when the aortic clamp is taken off. 4 To mitigate the risks associated with reperfusion injury, del Nido cardioplegia provides improved tolerance to ischemia, signifying that individuals undergoing complex cardiac procedures may benefit more from del Nido cardioplegia than 4:1 blood cardioplegia due to its greater effect in myocardial protection. 9 Ischemia-reperfusion injury is a potential side effect of cardiopulmonary bypass that might harm overall myocardial function. This damage is brought about by the deterioration of the membrane, the release of free radicals from anaerobic metabolism in the heart due to ischemia, buildup of intracellular calcium levels, and depletion of myocardial ATP. It also comes from excessive calcium load inside the cells, oxidative stress, and neutrophil buildup that occurs when the heart is reperfused with blood. 65 Single dose del Nido cardioplegia solution gets evenly distributed across the heart, thus efficiently safeguarding it from ischemic repercussions. 18
Shorter cardiopulmonary bypass and cross-clamp times
Cardiac surgeons need to ensure that the total operation time is as short as possible and an important contributing factor to that is the bypass and aortic cross-clamp times. 48 By maintaining cardiac arrest for 90 minutes with a single dose, the necessity of recurrent deliveries and intraoperative interventions is decreased.9,58 Also, because it facilitates a more seamless procedure and eliminates the need for a hiatus for redosing del Nido cardioplegia can reduce cross-clamp and bypass times. 35 Shorter cross-clamp and bypass times were noted for del Nido cardioplegia group, which were of significant value.15–17,44,45,54,56,66 This was due to the decreased number of doses and decreased surgical interruptions. 33 It was noted that the decreased bypass and cross-clamp times may also be due to the ‘learning curve effect’ and not only because of the number of doses given and the dosing intervals chosen. 46
The shorter periods of time can be directly related to the number of doses, placement of ostial cannula, or overall volume delivery regarding cardioplegia delivery techniques retrograde or antegrade routes. 17
In one study, they did receive fewer doses of cardioplegia, but it did not significantly affect the cross-clamp and bypass time during the cases. 4 The bypass and cross-clamp times both were reduced in the del Nido cardioplegia group, but the difference was not statistically significant.18,21,41,49,53,67 Quite a few studies did not show a significant difference in both times between del Nido cardioplegia patients and the blood cardioplegia group.5,7,10,13,38,42,44
Single dose use
Sorabella et al. extensively discussed the advantage del Nido cardioplegia provides on decreased intraoperative interruptions caused by its single-dose use, and how the decreased bypass and cross-clamp times show improved outcomes postoperatively. 10 Cagdas et al. demonstrated that with the use of single-dose del Nido cardioplegia in CABG surgeries, significantly shorter bypass and cross-clamp times could be achieved. 48 Most studies report shorter bypass times.50,55 Although one study showed that patients in the del Nido cardioplegia group had more lengthy operation times, bypass times, and cross-clamp times than patients in the St Thomas cardioplegia group. 9
A single shot of Del Nido cardioplegia administered within 90 minutes of cross-clamp following minimally invasive cardiac valve surgery in humans can have the same protective benefits as traditional blood cardioplegia. 35 The simplicity and effectiveness of del Nido cardioplegia’s usage, which enables the operational team to carry out the procedure swiftly, is one of its appealing features. 15
Cardiac biomarkers
Del Nido cardioplegia provides an advantage whereby troponin levels did not rise to the same extent as those in the whole blood cardioplegia group.13,21,38,44,49,53,54,67 In a similar manner creatine-kinase myocardial band (CKMB) levels have also been reported to be significantly lesser with the use of del Nido cardioplegia.42,53,67 Regarding postoperative outcome, there was no significant difference in troponin I levels as seen in a few studies.4,41 G George et al. reported that CKMB did not rise above the normal range on all 3 post-operative days, hence increased myocardial injury was not shown in CABG patients in del Nido cardioplegia group. 7 Patients who had CABG, valve, or aortic surgery had lower or comparable levels of CKMB or troponin when they used del Nido cardioplegia, as reported in another research. 13
On the other hand, Shu et al. mentioned that patients belonging to the del Nido cardioplegia group had significantly greater plasma levels of CKMB and troponin T levels than patients in the St Thomas cardioplegia group. Garg et al. were able to find significantly reduced troponin T levels for del Nido cardioplegia patients in their study. 56 They attributed the cause to lengthy surgery and cross-clamp time which might induce cardiac dysfunction. 9 Del Nido cardioplegia group showed a rise in troponin T and CKMB levels, but the difference was insignificant.16,43 One study could not find any difference for the del Nido cardioplegia group when compared for myocardial biomarkers. 44 In cross-clamp times of more than 180 minutes, del Nido cardioplegia group had increased CKMB levels. 32 Smigla et al reported that del Nido cardioplegia patients undergoing cross-clamp time of less than 60 minutes showed decreased troponin levels as compared to patients with cross-clamp time greater than 60 minutes. 40 When del Nido cardioplegia is compared to cold blood cardioplegia, these results are evident. This can be explained by the viscosity of blood which increases with the decrease in cardioplegia temperature. This inhibits adequate distribution of blood into the microvascular capillary bed of the myocardium especially in patients with coronary artery disease. This decreases the myocardial protection efficacy and preservation. 38
Dose interval
Adult cardiac surgeries on a general basis have less total cross-clamp time and hence with the use of del Nido cardioplegia a 90-min single dose is accepted. In surgeries with cross-clamp time of >90 minutes, a half-dose of 10 mL/kg is widely accepted after 60 to 90 minutes.48,66 Data shows that a subsequent dose is effective and yields comparable results to blood cardioplegia. 32 The average time for first redosing reported by D’Angelo et al. was between 65 and 80 minutes. 58 Elassal AA et al. described that they give an additional dose every 90 minutes for patients with LV hypertrophy and obstructive multivessel CAD. 4 Siddiqi et al. suggested that a single dose of 60 minutes provided adequate myocardial protection in aortic valve replacement patients. 21
Goh S Guim et al. conducted a study in 2020 to investigate the ischemic effects of the time interval between doses of del Nido cardioplegia. They concluded that the use of single-dose del Nido cardioplegia for at least up to 120 minutes can be considered reliable since they were unable to find any significant differences among their patient cohorts divided into different time intervals with the outcomes based on defibrillation requirements, the incidence of arrhythmias and intra-aortic balloon pump (IABP) usage. 68
Transfusion requirement
In one comparative study, they noted that there was no difference in transfusion requirements for patients in the del Nido cardioplegia group and the blood-based St Thomas cardioplegia group. 4 The requirement of transfusion (packed red blood cells) was significantly reduced in del Nido cardioplegia in other studies.16,42,66 The transfusion requirements were similar in a few research.13,54,67 This may be due to more retrograde autologous priming and venous antegrade priming conducted for del Nido cardioplegia group. 7 On the contrary, in another article, increased transfusion rates for plasma were reported in the del Nido cardioplegia group. 67
Hemodilution
Del Nido cardioplegia causes hemodilution but if noted from a different perspective, the two most crucial measurements during the perioperative phase are haemoglobin and hematocrit levels. The deficiency of erythrocytes may exacerbate the oxygenation of bodily tissues and lead to problems after surgery. Conversely, increased concentrations of haemoglobin and hematocrit may affect the efficiency of gas exchange in artificial oxygenator and tissue microcirculation negatively. Utilization of crystalloid cardioplegia has been shown to substantially decrease haemoglobin and hematocrit levels soon after delivery. However, the increased viscosity of cold blood cardioplegia, which suggests a slower flow rate via coronary arteries, may account for a longer duration towards the onset of cardiac arrest achieved with it. 20 It is suggested that del Nido cardioplegia with its 4 parts crystalloid may provide improved microcirculation as compared to whole blood cardioplegia. 5 Even though there is no direct study that has validated this concept, multiple studies have stated that the advantage of the dilution in del Nido cardioplegia may be beneficial in delivering cardioplegia in the microcirculation. Especially since del Nido is delivered at cold temperatures and hypothermia causes blood viscosity to increase.37,69–71
The reported difference in the hemodilution between del Nido cardioplegia and St Thomas cardioplegia was not significant yet both types showed hemodilution occurrence decreased haemoglobin levels, due to the 4 parts of crystalloid in the single-dosed del Nido cardioplegia and the multiple doses of blood cardioplegia with only 1 part of crystalloid. 47 As a result, a few studies showed higher haemoglobin levels post-bypass in del Nido cardioplegia patients.7,53,67 However, this difference may be considered null and void due to the routine use of blood conservation strategies. Gu et al. reported no significant differences in hematocrit and oxygen delivery index between del Nido cardioplegia and cold blood cardioplegia group. 13
Ultrafiltration
Hemoconcentration is required in paediatric or neonatal cardiac surgery alongside del Nido cardioplegia. This is due to the massive hemodilution that occurs. In adult surgeries where the right atrium is opened and bicaval venous cannulation is achieved, the return blood from the coronary sinus can be suctioned into a cell saver and the PRBCs may be salvaged. 27
The use of ultrafiltration has been reported to be significantly higher in del Nido cardioplegia patients.35,42 This is attributed to the larger crystalloid ratio in del Nido cardioplegia. 35 Russell et al noted that the use of ultrafiltration was doubled when crystalloid-based cardioplegia such as del Nido cardioplegia was used. 11 Recommendations for the incorporation of a hemoconcentrator into the cardiopulmonary bypass circuit in all cases where del Nido cardioplegia is used, have been made. 32 One article showed that the volume of ultrafiltration in del Nido cardioplegia group was less than that in the blood cardioplegia group, probably due to the reduced total dose of cardioplegia. 63
Total cardioplegia volume
Urcun et al compared the use of del Nido cardioplegia with microplegia. Microplegia is a type of cardioplegia where a greater blood to crystalloid ratio is administered. In their study, they reported that although the haemoglobin values observed in the blood gases taken at the end of cardiopulmonary bypass of the two groups were higher in the microplegia group as compared to the del Nido cardioplegia group, the difference between them was not statistically significant. 44 The total volume of cardioplegia given was lower in del Nido cardioplegia patients.10,41,49,50,66,67,72 This can be because of the significantly lesser number of doses and repetition of cardioplegia for the del Nido cardioplegia group hence less hemodilution compared to blood cardioplegia.7,16,45 It can also be attributed to its single-dose use. 43 The reduction in dose and elongation of inter-dose timings leads to uninterrupted operations and decreased contamination. 45 Two studies contradicted these findings whereby they found a larger total volume of cardioplegia administered in the del Nido cardioplegia group. 42 Where one of them showed a significant difference. 53
A well-noted input by Dr. del Nido when asked a question on his innovation, if del Nido cardioplegia can indeed be used for CABG alongside valvular cases; His reply was satisfactory saying that his research did not include such a category, but it might as well work only to keep in mind to not give excess volume and that, if possible, deliver cardioplegia retrogradely for adequate distribution. 73
Return of spontaneous rhythm
The antiarrhythmic properties of lidocaine in del Nido cardioplegia may contribute to the higher frequency of swift restoration and increased chance of return of normal heart rhythm in the del Nido cardioplegia group after cross-clamp removal.16,17,21,35,41 An important observation in one research was that even though del Nido cardioplegia was not found to be as effective as St Thomas cardioplegia in matters of the postoperative outcome, return of spontaneous rhythm post cross-clamp removal was increased in the del Nido cardioplegia group. 4 A few studies did not find any significant difference in the restoration of rhythm. 10 On the other side of the same coin, the spontaneous heart rhythm after the restoration of myocardial perfusion was most frequently sinus rhythm when blood cardioplegia was used, consequently, a greater proportion of patients from groups with crystalloid cardioplegia required defibrillation. 20
Defibrillation requirement
Defibrillation is said to damage cardiac myocytes. del Nido cardioplegia patients required lesser defibrillation perioperatively as compared to patients in the blood cardioplegia group, but this difference was not statistically significant.17,21,33,38,39,48,53,54,67,72 This can be attributed to the antiarrhythmic effect of lidocaine present in del Nido cardioplegia solution.21,48 Elassal et al. reported a reduced need for defibrillation in adult patients and they mentioned that defibrillation played a significant risk in postoperative low cardiac output syndrome. 4 Multiple other studies have also mentioned that del Nido cardioplegia required less defibrillation where the difference was significant.15,16 A few studies did not show any difference for intraoperative DC shocks delivered or defibrillation/cardioversion required.10,45
Shane et al. conducted a retrospective analysis to test the efficacy of del Nido cardioplegia on post cross-clamp removal incidence of ventricular fibrillation and defibrillation requirement. They found a significantly decreased requirement of defibrillation in del Nido cardioplegia patients compared to their St Thomas cardioplegia patients. 61 This proved the superiority of del Nido cardioplegia in terms of incidence of ventricular arrhythmias and return of spontaneous rhythm. It is unknown if there is any advantage of this delayed return of activity, but it may be beneficial in myocardial recovery. 62
Cardiac activity
Cardiac arrhythmias such as ventricular tachycardias, ventricular fibrillation, and atrial fibrillation, post-surgery remained far less common in the del Nido cardioplegia group than in the blood cardioplegia group. 9 New onset rhythm disturbance or dysrhythmias were seen significantly less in del Nido cardioplegia comparatively.42,46 Yet, in some findings, the difference was not significant.9,16,18,39,44,58 In other studies, there was no difference in the arrhythmia incidence noted.7,41,72 A greater incidence of atrial fibrillation was found in a pairwise meta-analysis of del Nido cardioplegia in comparison to blood cardioplegia. 8 Still, del Nido cardioplegia is counted as advantageous in terms of lower incidence of ventricular fibrillation with its use because of its effective myocardial protection. 18 Of the 91% of del Nido cardioplegia patients reported by a study by Smigla et al, who spontaneously regained their normal cardiac rhythm, 10% of them required defibrillation later. 40
Pacing requirement
A lower occurrence of pacing requirement and significantly shorter duration of pacing in del Nido cardioplegia was reported alongside a decreased need for permanent pacemaker insertion. 7 One research reported increased use of temporary pacemakers in the del Nido cardioplegia group, but the condition would be better once the patient left the operation theatre; hence they nullified the inferiority of its myocardial safety. 63 Linda Mongero et al. mentioned in her talk on the efficacy of del Nido cardioplegia in 2015 that waiting for the return of cardiac activity was important and that many surgeons would be impatient and not be willing to wait even a mere 30 to 40 seconds. Waiting for a short while instead of directly going for defibrillation or pacing does count as beneficial for the patients. 73
Ventricular ejection fraction
Left ventricular ejection fraction is an indicator of myocardial function and recovery. Studies suggest that patients in the del Nido cardioplegia group had greater LV ejection fraction after discharge, even though the pre-operative levels were similar in both groups.13,45,54,67,72 Low ejection fraction patients had more prevalent neuronal sequelae and cerebrovascular disorders. 39 In another study, right and left ventricular ejection fraction were evaluated separately, and it was shown that del Nido cardioplegia was better in preserving both. 44 Most studies noted ejection fraction of del Nido cardioplegia held no difference with other cardioplegic solutions.41,42
Organ dysfunction
Del Nido cardioplegia can be considered comparably safer due to decreased atrial fibrillation rates, which is a concern for mortality rates and stroke occurrence. 33 Decreased stroke occurrence in del Nido cardioplegia patients undergoing CABG procedure has been shown, but this difference is not statistically significant.41,55 A 2020 study noted that patients suffered more from cerebral disorders in the del Nido cardioplegia category. 39 A comparative study by Kumar et al. showed that postoperative proBNP levels were significantly lower in del Nido cardioplegia patients. 16 Two studies found no difference in the neurological function of del Nido cardioplegia patients.7,13 In individuals without renal problems, patients of del Nido cardioplegia group had higher eGFR when received in the ICU. 13 The blood urea nitrogen levels in the del Nido cardioplegia group were also much lower. In the del Nido cardioplegia group, the kidney function — which is directly linked to cardiac performance, was marginally better. 35 Statistically, no significant difference in postoperative renal insufficiency was reported for del Nido cardioplegia patients, in terms of acute kidney injury occurrence, dialysis usage, or renal impairment.7,13,16,41,67
Mechanical circulatory support requirement
There was a noticeably decreased incidence of intra-aortic balloon pump implantation in the del Nido cardioplegia group and the rates of ECMO requirement and death were comparable.13,44 Two studies did not find any difference in IABP requirement for del Nido cardioplegia patients.16,66 Compared to del Nido cardioplegia, the probability of in-hospital deaths was considerably greater for blood cardioplegia and histidine-tryptophan-ketoglutarate solution. 8 However, two studies were inconclusive in the superiority of del Nido cardioplegia in terms of mortality.7,16
Low cardiac output syndrome
Crystalloid cardioplegia has been linked to myocardial oedema, particularly with multiple doses during lengthy cardiac procedures, which may predispose patients to low cardiac output syndrome after surgery. Research indicates that the development of ventricular wall rigidity caused by myocardial oedema might decrease preload and afterload, ultimately resulting in compromised heart function. 22 Insignificant differences showed decreased low cardiac output syndrome occurrence or development in the del Nido cardioplegia group.41,46,53
Postoperative inotrope usage
The need for inotropes was seen less in del Nido cardioplegia comparatively but the difference was not significant.16,32,49 The difference was seen significantly in a few studies.44,46 This has been described as an indirect indicator of myocardial preservation. 17 Still, few studies could not observe any difference in inotrope requirements.42,43,53,67,72 Lafci et al did publish reduced inotrope use, and even though it was not statistically significant, they reported a 50% decrease in the use of inotropes in del Nido cardioplegia patients comparatively. 18
Ventilation time, icu and hospital stay
Del Nido cardioplegia has been reported to have significantly decreased ventilation time.38,41,42 Yet, other studies were unable to note a difference.7,13,44,54,55 One study reported a significantly longer intubation period in patients in the del Nido cardioplegia group as compared to blood cardioplegia. 67
The del Nido cardioplegia group has been noted to experience a considerably shorter duration of stay in the ICU and fewer cases of cardiac arrhythmia than the St Thomas cardioplegia group, which indicates the myocardial protective efficacy of del Nido cardioplegia.9,38,41 One report did show that the mean intensive care unit (ICU) stay was more in del Nido cardioplegia as compared to blood cardioplegia. 53 Other studies were unable to observe any difference in the length of ICU stay for del Nido cardioplegia patients.7,13,42,54,55,67 Total hospital stay duration was significantly reduced in del Nido cardioplegia patients.10,16,41,53 But when compared to histidine-tryptophan-ketoglutarate solution a meta-analysis revealed that del Nido cardioplegia was linked to longer hospitalizations. 8 Still, few studies were unable to note any difference in hospital stay for del Nido cardioplegia patients.13,54,55,67
Electrolytes
The time needed to wean off from cardiopulmonary bypass was also significantly less for del Nido cardioplegia patients. 16 The del Nido cardioplegia group’s lactate levels were much lower than the cold blood cardioplegia groups in the early stages, lasting from the time the procedure was finished to 9 hours thereafter. At 0 hours postoperatively the lactate level difference was 2.7 mmol/L for del Nido patients and 3.2 mmol/L for blood cardioplegia patients. At 3 hours the differences were 3.2 mmol/L and 4.8 mmol/L. Then after 6 hours the difference was 3.5 mmol/L and 5.8 mmol/L. 13
Del Nido cardioplegia uses a crystalloid base solution that is glucose-free.21,39 This translates to lower intraoperative glucose levels.21,41,72 Ucak and Uncu reported lower peak levels of glucose perioperatively with the difference being 163 ± 24 g/dL for del Nido patients and 193 ± 44 g/dL for blood cardioplegia patients. 41 Similarly, Marzouk et al. reported a significant difference (p = .001) in glucose levels between del Nido cardioplegia patients and cold blood cardioplegia patients. The values were 8.2 ± 2.3 mmol/L in the del Nido cardioplegia patients and 9.0 ± 1.8 mmol/L in the other group. 72
This also links del Nido cardioplegia to reduced infection rates including for diabetic patients.39,72 As compared to blood cardioplegia, del Nido cardioplegia has four times less glucose, as glucose levels are related to the blood ratio of cardioplegia. 41 However, two studies were unable to find any significant difference in glucose levels between del Nido cardioplegia and blood cardioplegia.53,67 del Nido cardioplegia has shown improved postoperative control of glycemia. Hence, it provides decreased insulin requirements39,41 and lower frequency of insulin administration.42,43
Cost-effectiveness
The cost-effectiveness of del Nido cardioplegia has been mentioned as a part of its pre-eminence. 17 The production and usage of it has been found to be economic.15,52,53 Even though this link has been made to its use, a translation to the Indian healthcare and economy has not been notable. 48
Tepid modified del Nido cardioplegia
Utkan Sevuk et al demonstrated the use of tepid modified del Nido cardioplegia which contained 30 mEq/L of potassium which is relatively more than that of normal del Nido cardioplegia. The temperature was 28oC and lidocaine, magnesium sulphate, and mannitol were used in lesser amounts. In their comparative study they noted no significant difference between the two groups regarding the following measurements; Postoperative inotropic scores, postoperative troponin T levels, IABP requirement, defibrillation requirements, postoperative LV ejection fraction, transfusion requirements, or any postoperative atrial fibrillation development. A significant difference was found for cross-clamp and bypass times, where the tepid group had a shorter time period. 24 The left shift of the oxy-haemoglobin curve caused by hypothermia increases haemoglobin affinity for oxygen which consequently leads to reduced oxygen delivery in cold blood cardioplegia. 22 The increased ratio of blood and its advantage apart from oxygen delivery has not been extensively defined. Cleveland Clinic has recommended the use of del Nido cardioplegia in adults in only valvular surgeries at least until its efficacy is definitively proven for CABG patients. 37
In coronary artery bypass grafting surgery
It appears that del Nido cardioplegia offers low-risk patients an affordable and effective technique while undergoing on-pump CABG surgery. 9 del Nido cardioplegia use in acute myocardial infarction patients undergoing CABG procedures was not documented until 2014 when Yerebekan et al. reported the first study that showed the benefits of del Nido cardioplegia in coronary revascularization. Bypass and cross-clamp times were reported to be significantly shorter for del Nido cardioplegia. In their patient population low cardiac output syndrome prevalence, IABP requirement, use of inotropes postoperatively, sepsis, atrial fibrillation, acute kidney injury, and occurrence of stroke were not significantly different between the del Nido cardioplegia group and whole blood cardioplegia group. Due to the decreased value of blood transfusion requirement, the reduced numbers showed secondary advantage of del Nido cardioplegia regarding ICU stay duration, ventilator use duration, and total hospital stay duration. Their study discussed the improved effectiveness of del Nido cardioplegia regarding its mechanism of action, mainly contributed by lidocaine and magnesium. The combined effect of these two leads to better cytoprotection. 64
Guajardo Salinas et al. in their study on the use of del Nido cardioplegia in low-risk CABG patients, were unable to find any significant difference in terms of length of stay, complications, or short-term mortality. 52 According to one current study, del Nido cardioplegia is a reliable and useful cardioplegia for valve or CABG procedures performed on patients older than 70 years of age. 13 Sorabella et al. had 14 patients who came in with a patent LIMA graft which posed a challenge for myocardial perfusion. The LIMA graft was left unclamped and continuous retrograde cardioplegia was used and was reported to be well-tolerated, between del Nido cardioplegia and whole blood cardioplegia. 10 Also, current evidence suggests that del Nido cardioplegia given through retrograde coupled with antegrade fashion is fruitful. Although, acute heart block can be one problem that may occur due to retrograde delivery and lidocaine overdose. 32
Del Nido cardioplegia used as a single-shot cardioplegia may be inadequate for CABG patients with obstructive multi-vessel disease and LV hypertrophy. This may necessitate multiple doses to achieve better myocardial protection and to alleviate damage, with heterogeneous distribution of cardioplegia. 21 The use of del Nido cardioplegia in minimally invasive valvular surgery as compared to St Thomas cardioplegia was summarized by Russel S et al, they reviewed that there was not much significant difference between the postoperative outcomes between both groups, but del Nido cardioplegia is favouring when it came to CKMB levels directly after the surgery, and with regards to a decrease in bypass time. This indicates improved efficiency in surgery yet no significant changes in the postoperative myocardial damage. 11
Ringer’s lactate as the base solution
Kantathut N et al reported the use of Ringer’s lactate as the base solution for del Nido cardioplegia in adult cardiac surgery. They then compared its efficacy and performance based on clinical outcomes against blood cardioplegia. They measured troponin T levels as an indicator of myocardial injury which favoured the use of del Nido cardioplegia, alongside duration of inotrope usage and incidence of ventricular and atrial fibrillation. It was also associated with a shorter length of ICU and hospital stay and decreased total cardioplegia volume. They also measured CKMB levels which were similar for both study groups. They noted that troponin T measurement had a higher correlation with clinical outcomes when compared with postoperative CKMB levels. The decrease in total volume directly correlates to the reduction in hemodilution, hence the reduction in RBC transfusion. They were concerned with the calcium levels and its effect on postoperative outcomes, but even with ringer’s lactate as the base solution, the total calcium concentration was twice the amount in the original solution. They theorized that the addition of lidocaine and magnesium sulphate countered the increased calcium level. 36
Heart transplantation
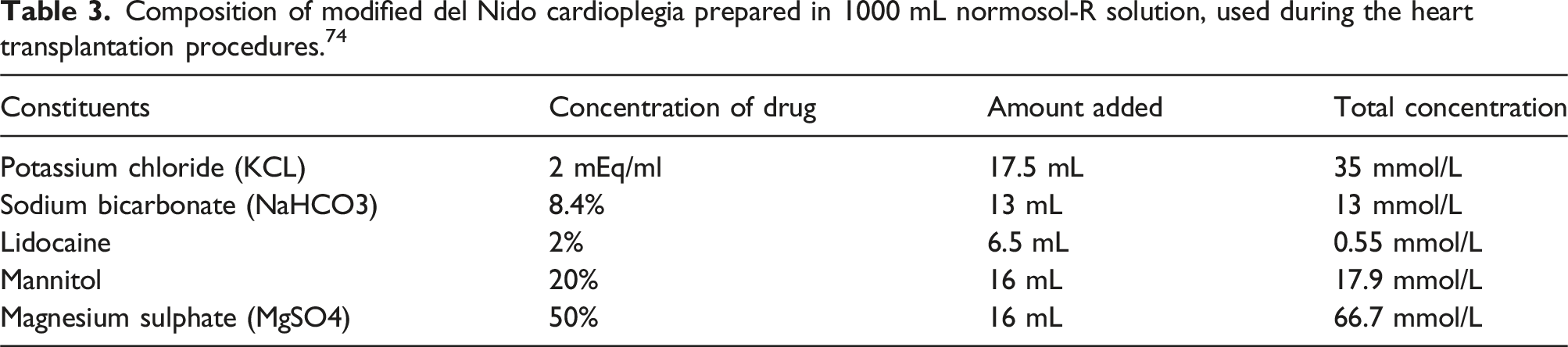
Composition of modified del Nido cardioplegia prepared in 1000 mL normosol-R solution, used during the heart transplantation procedures. 74
Asanguinous del Nido cardioplegia
In 2018, a case report was published by Rosenbloom et al. on the utilization of asanguinous del Nido cardioplegia for an aortic valve replacement on a patient diagnosed with cold agglutinins. The case was uneventful, and they successfully used del Nido cardioplegia without blood in the surgery for a cross-clamp time of 52 minutes. Procedure and patient outcomes such as ventricular function, return of spontaneous rhythm, and weaning off bypass were normal. 75
Del Nido cardioplegia versus microplegia & warm blood cardioplegia
Table summarizing the reviewed studies incorporating and evaluating the use of del Nido cardioplegia in adult cardiac surgery (DNC – del Nido cardioplegia, STH – St. Thomas cardioplegia).
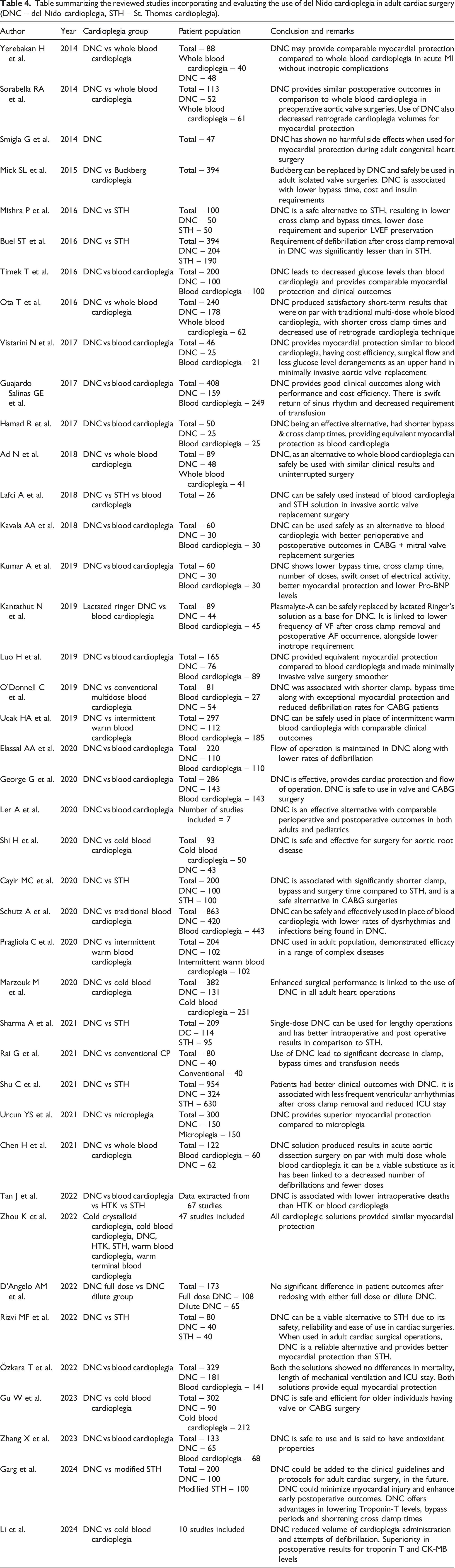
In recent years, it has become increasingly clear that del Nido cardioplegia is indeed advantageous and can be used as an alternative to traditional cardioplegia. 58 Garg et al. predicted the incorporation of del Nido cardioplegia in standard protocol for adult cardiac surgery in the near future. 56 del Nido cardioplegia may be used in adult cardiac surgery, but the selection should be patient-specific until a proper criterion is established. 51 The most recent meta-analysis by Li et al. concluded that del Nido cardioplegia provides better myocardial protection in adult cardiac surgery (Table 4). 77
Conclusion
Various studies highlight the importance of cardioplegia in myocardial protection during cardiac surgeries. Factors like delivery method, route of administration, and composition of the solution are crucial in choosing the right cardioplegia for each patient and procedure. Preferences of surgeons and medical centres heavily influence this selection. Del Nido cardioplegia emerges as an alternative to standard blood cardioplegia, offering efficacy in reducing hemodilution, transfusion needs, and bypass times. Indeed, del Nido cardioplegia has the potential to provide better myocardial protection, especially in elderly patients, with improved early outcomes. There is still no certainty in the choice of cardioplegia and it is still fully dependent on the cardiac team’s choice; Myocardial protection under those terms has reached a plateau phase until the next big breakthrough is made.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.