
Abstract
This article presents findings from an in-depth qualitative study focused exclusively on the first-hand experiences of small and micro businesses managers who have responded to employees with mental health difficulties. Despite growing policy focus on workplace mental health, empirical research evidence on management experiences of responding to mental health issues in a small or micro business context is rare. Drawing on in-depth interviews with 21 UK-based small and micro business managers who described 45 individual employee cases, we examine how managers traverse a support-performance continuum, and use a tension-based lens to analyse the tensions that managers experienced. We examine three key tensions for small and micro business managers that surfaced when responding to employees with mental health problems: (1) Individual vs Collective; (2) Confidence vs Caution; (3) Informal vs Formal. Our analysis exposes how managers handle tensions when managing at the nexus of support and performance and contributes a deeper understanding of the dynamics and challenges of managing mental health problems in small and micro businesses.
Keywords
Introduction
Management of mental health in the workplace is of significant social and economic concern (Goetzel et al., 2018; OECD, 2015; Vos et al., 2016); it is high on western public health agendas. Common mental health problems, including stress, anxiety and depression, affect around one-fifth of the working age population (Steel et al., 2014) and are a leading cause of workplace absence and productivity loss, with annual estimated global costs of over USD$1 trillion (Chisholm et al., 2016). Academic research from a range of disciplines has focussed on how workplaces shape mental health both in terms of harmful effects and in supporting and enhancing mental health (Woods et al., 2019). Drawing on empirical evidence from 45 employee cases recounted by 21 UK-based small and microbusiness managers with first-hand experience of managing employees with a mental health problem, we examine how managers navigate support and performance practices. Through this, we illustrate how the management of employee mental health problems in a small and microbusiness context reveals multiple tensions that have to be negotiated. We define small businesses as those with fewer than 50 employees and microbusinesses as 1–9 employees (European Commission, 2005).
Research on manager experiences of managing employees with mental health problems is concentrated in large organisations (250+ employees), and studies incorporating a range of business sizes rarely disaggregate findings on the experiences of small employers (Gignac et al., 2020; Jansson and Gunnarsson, 2018; Ladegaard et al., 2019; Martin et al., 2018; Porter et al., 2019). Moreover, empirical research which aggregates small and medium enterprises (SME) in the same category is unhelpfully homogenizing (Mallett and Wapshott, 2017), particularly when examining the challenges and constraints shaping the management of mental health and related occupational health (OH) strategies and interventions in small and microbusinesses. Consideration of small and microbusinesses as distinct from medium-sized firms (50–249 employees) is required, as the latter display different characteristics that are likely to be significant in managing employee mental health. For example, medium-sized firms are more likely to have more resources and more formalised Human Resource Management (HRM) (Wapshott and Mallett, 2015), with greater scope to redesign jobs, all of which will shape approaches to managing workplace mental health.
Workplace mental health has been subject to growing policy attention in recent decades in the UK (Department for Work and Pensions, 2009; Stevenson and Farmer, 2017) and workplace mental health initiatives proliferate 1 . The UK legislative framework for supporting mental health at work is in the 2010 Equality Act; this requires employers to make ‘reasonable adjustments’ for employees who have mental or physical disabilities, although what constitutes ‘reasonable’ is open to interpretation. Other factors such as a supportive culture, employee assistance programme or stigma reduction interventions are not legally mandated; moreover, employees with a mental illness might not seek reasonable adjustments if they are unaware of their rights (Follmer and Jones, 2018). Even where employees do not consider their mental health problem to constitute a disability in legal terms, the UK professional people management body (Chartered Institute of Personnel and Development – CIPD) advocates appropriate changes to work or working patterns to support employees with poor mental health (CIPD, 2021). Similar legal frameworks are in place in the USA (the Americans with Disabilities Act), and in Australia (the Equal Opportunity Act, 2010). UK employers have, in a broad sense, been imbued in recent years with heightened awareness of mental health at work, the more so in the contemporary era as Covid-19 has triggered heightened anxiety for workers (Department of Health and Social Care, 2021; Hamouche, 2020).
The economic impact of the Covid-19 pandemic is likely to affect many small and microbusiness managers and their employees, with emerging evidence pointing to significant impact of uncertainties about financial stability, job security and business continuity (Brown and Cowling, 2021; Cowling et al., 2020; Eggers, 2020; Hurley et al., 2021; Morgan, 2020). Concern for owner-manager mental health due to financial distress has also been highlighted (Lathabhavan et al., 2021). This precarious situation is likely to increase stress and anxiety among small and microbusiness employees. It is therefore, vital that small and microbusinesses are equipped to respond to mental health problems amongst their workforce. However, there is a paucity of evidence upon which to base mental health intervention strategies for the small business sector (Martin et al., 2019).
While we note the body of work focused on managing physical health and safety in small firms (Eakin, 1992; 2010; Eakin et al., 2003; Eakin and MacEachen, 1998; MacEachen et al., 2010), a parallel strand on psychological health has yet to fully emerge. A review of psychological distress and related work attendance in SMEs by Cocker et al. (2012) found limited research on workplace mental health risks, prevalence or responses. A decade on, and evidence remains limited. Whilst guidance on mental health at work proliferates, a recent international systematic review of workplace mental health guidelines (Memish et al., 2017: 220) concluded ‘recommendations were often not appropriate for small-medium businesses that do not have the time, money, or confidence to implement resource-intensive interventions, or the staff with expertise and roles intended for this purpose’. Yet, despite this growing acknowledgement of their differing context, few in-depth empirical studies have focused exclusively on the first-hand experiences of managers navigating mental health problems among employees in small and microbusinesses. This absence of empirical evidence base is noteworthy, when considered against the growing number of guides and interventions offering targeted advice for small businesses.
A central theme emerging from this research was the challenge inherent in implementing an appropriate balance between support, performance management and assessment of capability. Ipsen et al. (2020) call for research to better understand the mechanisms and intersections between how leaders can integrate the management of mental health with performance. We identify three key tensions for small and microbusiness managers that emerged when traversing a continuum of support-performance interventions: (1) Individual versus Collective; (2) Confidence versus Caution; (3) Informal versus Formal. Drawing on the work of paradox theory scholars (Fairhurst et al., 2016; Lewis and Smith, 2014; Miron-Spektor et al., 2018; Poole and Van De Ven, 1989; Putnam et al., 2016; Smith and Lewis, 2011) we use a tension-based lens to analyse how tensions are experienced by managers and their response strategies. By directing attention to the tensions shaping how managers balance support and performance, we provide a deeper understanding of the dynamics and challenges of managing mental health problems in small and microbusinesses. Importantly, manager experiences indicate that tensions are rarely ‘resolved’ in any conclusive sense, but reflect an ongoing and dynamic balancing act. Our analysis exposes how small and microbusiness managers handle tensions when managing at the nexus of mental health support and performance and thus makes an important and timely contribution to the scant empirical evidence base on managing mental health problems in small business.
In the following section, we review the literature that informs our study. We begin with the extant evidence base on manager experiences of responding to employee mental health problems, which emanates predominantly from larger workplaces. Drawing on wider HRM and OH literature, we then extrapolate how the particular context of small and microbusinesses might shape management responses to an employee presenting with a mental health issue. The theoretical framework for our analysis is then introduced, namely a tension-based lens. Following this, we describe the research method, then present our findings, and conclude by discussing the implications for theory and practice.
Background
Managing mental health in the workplace
Extant research on manager experiences of supporting employees with mental health problems, emanating from studies of larger organisations or mixed-size samples that do not disaggregate findings by organisation size, reveals some common themes. Open two-way communication between managers and employees is fundamental to effective support (Jansson and Gunnarsson, 2018; Thisted et al., 2020) but navigating disclosure can be complex for both parties. Managerial tensions can arise where employees lack awareness of their mental health difficulties and are unable or unwilling to recognise the effects of their symptoms (e.g. lowered productivity, poor timekeeping, withdrawal, interpersonal conflict), hence, problems are framed as poor performance or challenging conduct and become disciplinary matters (Gignac et al., 2020; Porter et al., 2019). Not all situations bring challenges, and where employees find work a respite from their mental distress, productivity can be unaffected (Jansson and Gunnarsson, 2018). Standard workplace flexibilities and ‘natural supports’ (Secker and Membrey, 2003) such as flexitime, working from home and positive co-worker relationships can mean the need for specific managerial intervention is minimal in some cases (Jansson and Gunnarsson, 2018; Peterson et al., 2017). Successfully supporting an employee to regain function in the workplace can also be a source of pride and satisfaction for managers (Jansson and Gunnarsson, 2018; Lexén et al., 2016; Martin et al., 2018; Mizzoni and Kirsh, 2006; Peterson et al., 2017; Tse, 2004) and can increase manager skills and competencies (Martin et al., 2018).
Research identifies cross pressures and a difficult ‘balancing act’ in managing employees with mental health difficulties, in which the needs of the employee, co-workers, business, and manager’s values, feelings and interests are weighed against one another (Bramwell et al., 2016; Kirsh et al., 2018; Ladegaard et al., 2019; Martin et al., 2018). Managers are conscious of impacts on co-workers, including increased workload and time consumed in supporting the unwell employee, either practically or emotionally, which in turn affect overall productivity (Porter et al., 2019). Managers encounter tensions in maintaining confidentiality, where co-workers ask questions about the employee or query the rationale for adjustments (Gignac et al., 2020; Hauck and Chard, 2009; Kirsh et al., 2018). Over time, empathy and accommodation shown by co-workers can decline, being replaced by stress, frustration and resentment (Gignac et al., 2020; Jansson and Gunnarsson, 2018; Ladegaard et al., 2019; Martin et al., 2018; Porter et al., 2019). Managers may be placed in the role of mediator, and relationships between employee, manager and co-workers might be irreparably damaged where sustained attempts at support prove unsuccessful (Gignac et al., 2020; Lexén et al., 2016). This complex and demanding task may take its toll on the mental wellbeing of managers themselves (Kirsh et al., 2018; Ladegaard et al., 2019; Martin et al., 2018).
How this balancing act is negotiated within the specific context of small and microbusiness, has received little attention. We argue that the small and microbusiness context, characterised by ‘high degrees of informality, close spatial and social proximity and resource poverty’ (Wapshott and Mallett, 2015:14), may exacerbate managerial tensions. Approaches to HRM and workplace health and safety in smaller firms tend to be informal (Marlow, 2002; Nguyen and Bryant, 2004) with informal approaches to health and wellbeing perceived as in keeping with organisational size and culture, as well as more cost effective (Tu et al., 2021). Financial survival of the business is typically the most pressing issue, with OH matters taking lower priority (Bramwell et al., 2016; Hasle and Limborg 2006; Martin and LaMontagne, 2018). Small and microbusinesses are less likely to have access to OH provision, dedicated HR support, or to develop policies in advance of problems arising (Fullick et al., 2019; Harrison et al., 2013; Steadman et al., 2015; Tu et al., 2021). Because mental, and other health issues, are encountered less often than in large organisations (Barnes et al., 2009; Brohan et al., 2010), and resources are limited, small firms tend not to inform or equip themselves in a pre-emptive or proactive way (De Kok, 2005; Martin et al., 2020; Tu et al., 2021).
Rigid absence management policies and external intervention may conflict with the more flexible and personal workplace culture in small firms (Andersen et al., 2007; Bevan et al., 2004; Eakin et al., 2010; Fullick et al., 2019). Resolutions to OH issues are found through dialogue and negotiation, rather than fixed policies and procedures (Adams et al., 2015; Andersen et al., 2007; Eakin et al., 2003; Gunnarsson et al., 2014). UK evidence suggests that small businesses are more likely to exercise discretion with sickness absence policies and sick pay, including going over and above statutory requirements (Adams et al., 2015; Tu et al., 2021). Engagement with external sources of support and guidance, for example, HRM consultants or OH specialists, when managing a sick employee is unlikely (Andersen et al., 2007); hence, responses to employee health issues are also reliant on the attitudes and skills of business owners (Martin et al., 2015).
Informality and close spatial and social proximity in small and micro businesses create both opportunities and constraints for effective management, creating challenges and tensions for managers. This physical and social environment might facilitate more personal approaches to managing mental health and encourage employee disclosure of health problems (Jones and King, 2014; Wilson et al., 2012), but conversely could increase an employee’s sense of duty to attend work despite illness, resulting in higher levels of presenteeism (Holt and Powell, 2015; Knani et al., 2021). For small businesses with little experience of employing people with disabilities, underpinning drivers of goodwill and social conscience may be constrained by (mis)perceptions that supporting employees with mental health problems will bring additional cost (Ju et al., 2013; Lexén et al., 2016). Looking at health problems more broadly, Barnes et al. (2009) found sickness absence in the context of a small workforce and tight profit margins expedited a move towards performance-related dismissal or early retirement options amongst some microbusinesses. However, close working relationships helped small employers to respond flexibly to illness and close personal bonds motivated employers to move beyond basic legal requirements when making adjustments.
Paradox theory and a tension-based lens
Drawing on paradox theory, we use a tension-based framework to interrogate the circumstances and contexts shaping how small and microbusinesses managers balance support and performance, and in so doing, provide a deeper understanding of the dynamics and challenges of managing mental health problems in small and microbusinesses. Paradox theory is a meta-theory, which focuses on how organisations or individuals experience and cope with tensions arising from contradictory elements. Smith and Lewis (2011: 382) define paradox as ‘contradictory yet interrelated elements that exist simultaneously and persist over time’. Managing mental health problems in the workplace inherently involves tensions through negotiating competing demands, goals, interests and perspectives that persist over time. Tensions manifest as ‘stress, anxiety, discomfort, or tightness in making choices, responding to, and moving forward in organisational situations’ (Putnam et al., 2016: 68). What constitutes a paradox depends on what managers perceive as contradictory, yet interrelated, within their environment (Putnam et al., 2016), meaning a paradox perspective can be usefully applied to numerous scholarly fields and across a broad range of tensions (Keegan et al., 2018; Lewis and Smith, 2014).
Paradox theory specifies that tensions become salient when situations are difficult. Latent tensions can become salient with environmental factors (plurality, scarcity and change) and an actor’s paradoxical cognition (Fairhurst et al., 2016; Smith and Lewis, 2011). Resource scarcity can intensify an individual’s experience and recognition of tensions (Miron-Spektor et al., 2018; Smith and Lewis, 2011). Thus, limited time and financial resources in small and microbusinesses can elevate the awareness of tensions amongst managers when attempting the difficult task of managing employee’s mental ill-health. Small and microbusiness managers are likely to be faced with intensive plurality when managing ill-health as managers navigate the pressures regarding balancing the needs of an ill employee with others in a small workforce, particularly in a context with close spatial and social proximity.
Management responses to tensions can be proactive or defensive (Lê and Jarzabkowski, 2015) and trigger different handling strategies. Individuals might react defensively to competing tensions, treating them as an ‘either-or’ choice, with managers simplifying the paradoxical tension and negating one side of the tension. This is similar to a contingency perspective that emphasises how effective responses depend on immediate circumstances and offer a pragmatic trade-off (Qiu and Chreim, 2021). Although, Smith and Lewis (2011: 391) argue that ‘either-or’ responses are embedded in ‘forces for consistency, emotional anxiety and defensiveness’. Conversely, individuals might engage actively with tensions, working through them in constructive and self-reinforcing ways, accepting a ‘both-and’ response rather than attempting to resolve the tension (Smith and Lewis, 2011). This recognises how phenomena can fit opposing categories simultaneously. How managers respond to tensions can affect their own wellbeing. Embracing contradictions and dualities can promote good mental health (Gaim and Wahalin, 2016), whereas defensive responses can be counterproductive and result in anxiety (Ashford and Reingen, 2014; Lewis, 2000). Orientation towards proactive coping strategies helps actors anticipate dynamic effects, creating a broader perspective that aims at using tensions for creativity and innovative development (Smith, 2014). Thus, applying a tension-based lens can help us think about how managers work through and balance tensions in a given context rather than trying to solve the grand challenge of managing mental-ill health in the workplace and so is a lens with both theoretical and practical relevance.
Categorisations of response strategies.
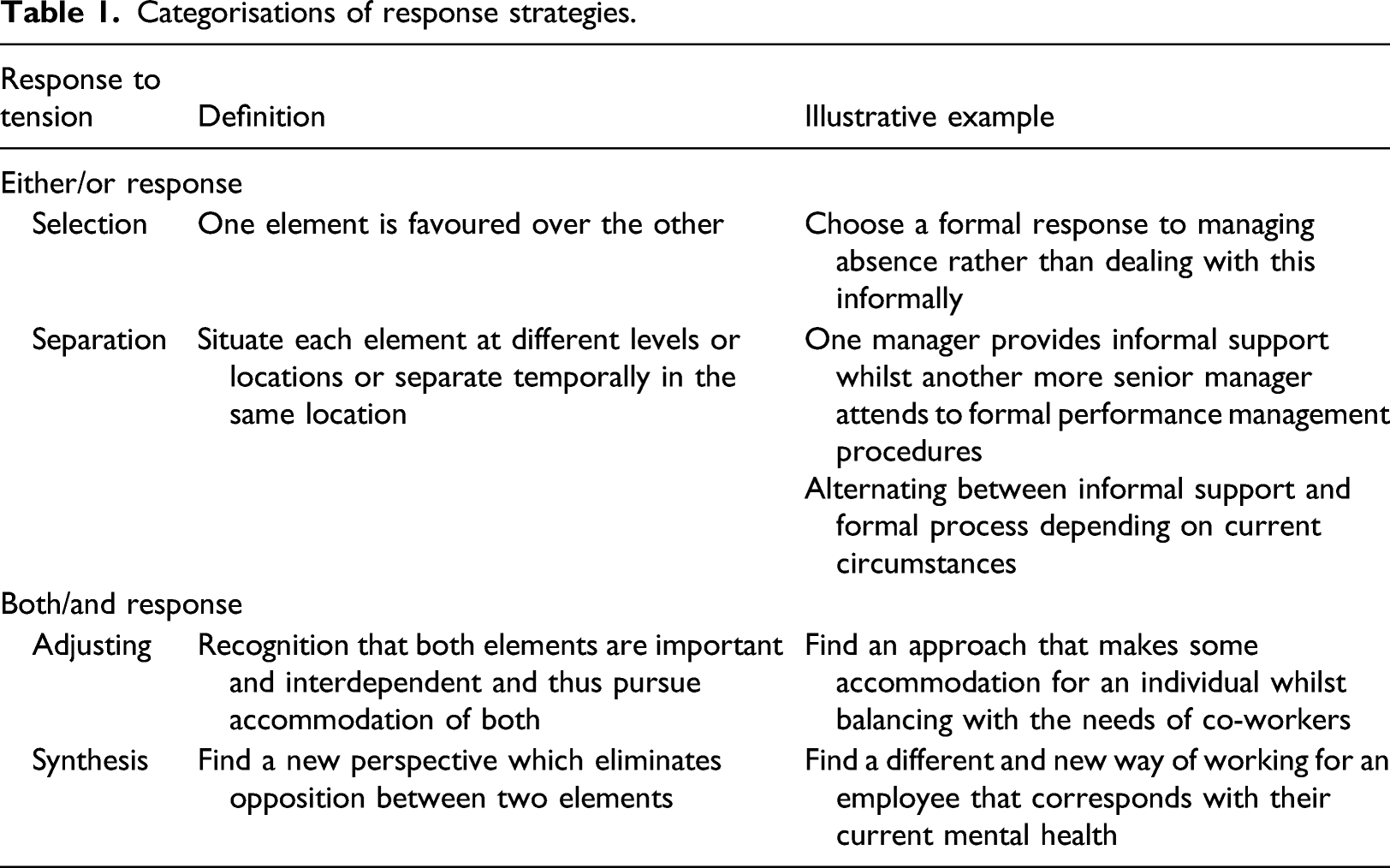
The two ‘either-or’ strategies include selection where one element is favoured over the other (Putnam et al., 2014; Seo et al., 2004), and separation where managers hold each element separate in time, location or context (Poole and Van De Ven, 1989; Seo et al., 2004). The first of our ‘both-and’ strategies is adjusting where managers view both elements as important and interdependent and thus pursue accommodation of both (Jarzabkowski et al., 2013). Our second ‘both-and’ response strategy is synthesis where managers identify a novel solution taking both elements into account (Poole and Van De Ven, 1989; Schad et al., 2016).
Methodology, method and data
A qualitative methodology was employed to explore the experiences of managers of small and microbusinesses who had encountered and responded to mental health problems among their employees. Our focus on manager experiences, and their interpretations of the meaning of those accounts of events, contextualised in specific workplaces and social relationships, demands a social constructionist ontology (Berger and Luckman, 1966). Yet, our attempts to draw policy and practice implications from our findings reflect the influence of a critical realist paradigm to the extent that workplaces as institutions, and the actors within them, are real in their capacities to shape, enable or constrain social action (Bhaskar, 2016; Pilgrim, 2022). A weak social constructionism thus, underpins our approach.
Sample and recruitment
Interview sample and case characteristics.
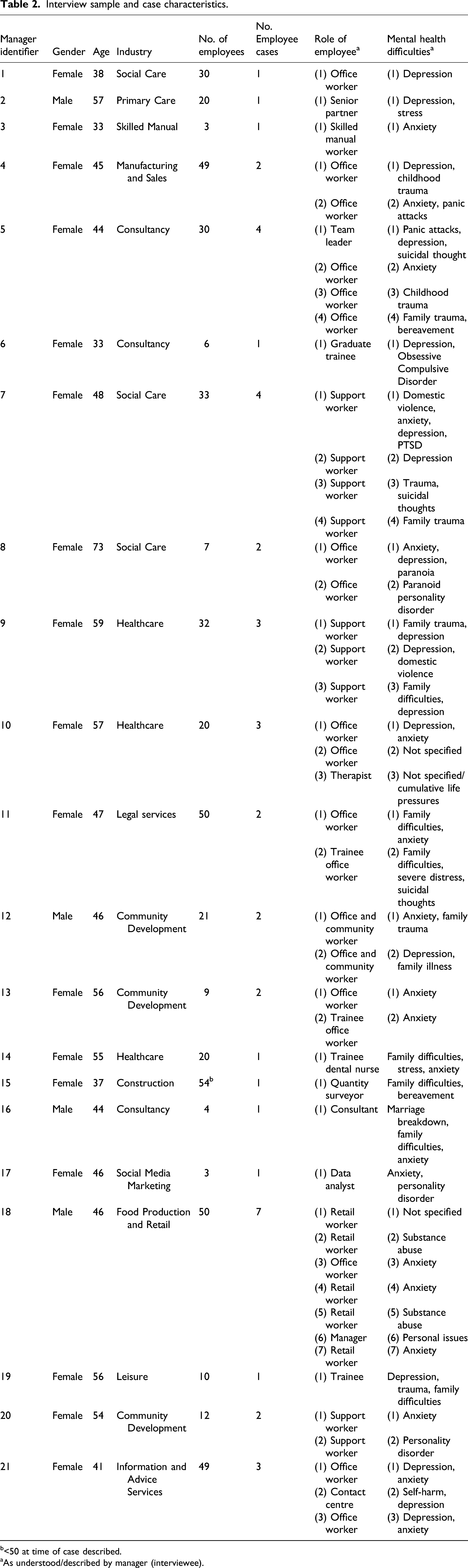
b<50 at time of case described.
aAs understood/described by manager (interviewee).
To elicit direct insights, rather than attitudes or perceptions, recruitment was restricted to managers with first-hand experience of managing employees through times of mental health difficulties. Whilst job titles varied, including CEO, managing director, practice manager, operations manager and talent manager, all held some responsibility for personnel management issues. For simplicity, henceforth, we refer to all research participants as managers. Businesses ranged in size from three to 542 staff members, including the managers/directors. Around one-third were microbusinesses (1–9 employees). Employees were contracted directly, with the exception of one firm who employed staff on a freelance basis. The employees in cases described by managers had been recruited through a competitive application process, with the exception of one recruited via a scheme targeted at individuals with long-term health problems. Thus, this study represents a context of open, rather than supported, employment (Lexén et al., 2016; Mizzoni and Kirsh, 2006). Fourteen firms were private companies and seven were charities with paid employees. Sectors included healthcare, social care, skilled manual trades, manufacturing, retail and sales, consultancy, law, digital media and community development. Businesses were located in urban and rural locations across England and Scotland. Nine managers had personal experience of mental health problems, and five mentioned close family experience. Around a third of organisations had mental wellbeing as a core or significant part of their service remit, for example, voluntary sector mental health support, welfare advice and guidance and six managers had professional training/qualification in mental health such as psychotherapy, psychology. We therefore, note the relatively ‘engaged’ character of this self-selecting sample.
Interview method
Interviews took place between November 2019 and February 2020 and were conducted by the first and second authors, either face-to-face (n = 4) or by telephone (n = 17) according to interviewee preference. Interviews averaged 71 min (range 37–110 min), and were recorded with consent and transcribed verbatim. Interviews used a combination of narrative and semi-structured approaches (Jovchelovitch and Bauer, 2000; Scheibelhofer, 2008; Ziebland, 2013). Managers were first invited to tell their story of their experience of supporting an employee with mental health problems. This was done using a narrative interviewing approach, that is, minimal prompting, following the interviewee’s lead. We explored what happened (experience) and what they did (response). Our opening question was ‘Starting from wherever you think is relevant, and in your own time, please could you tell me about the experience that prompted you to take part in this project’. Researcher-directed questioning followed, focused around experience of managing and supporting employees with mental health problems. Interviews explored specific employee cases, rather than broader perspectives on promoting mental wellbeing at work. We focused on eliciting detail on: how managers discovered the employee’s mental health difficulties; the stage an employee disclosed a mental health issue; steps taken to support/retain the employee; and the actors involved. We explored short-term and longer-term impacts including: personal impact on interviewee (e.g. own wellbeing, work-life balance, personal finances), impact on colleagues/team (e.g. interpersonal relationships, workload, disclosure), impact on business operations (e.g. productivity/service delivery), and financial, legal, future plans/business strategy (e.g. growth/reduction of business/staffing; hiring decisions). Other discussion points included organisation mental health policies; the nature/duration and impact of any absences (e.g. short term, long term, repeated, predictable/unpredictable); presenteeism; how any return to work was managed; the influence of formal/legal obligations; and sources of information, advice, and guidance. We probed for how the situation progressed, resolved or concluded. Finally we discussed the manager’s reflections on what they feel they did well, what they feel they would have done differently, and if and how they changed any of their approaches going forward.
Data analysis
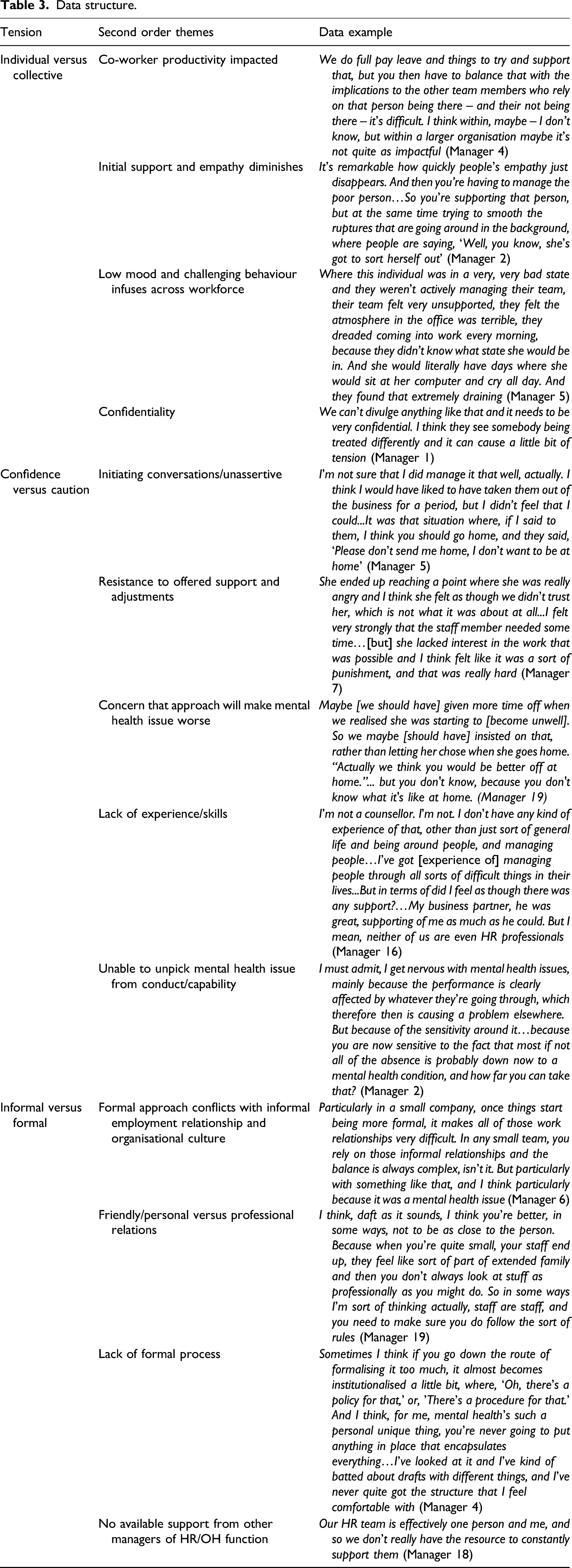
Data structure.
Matrix example.
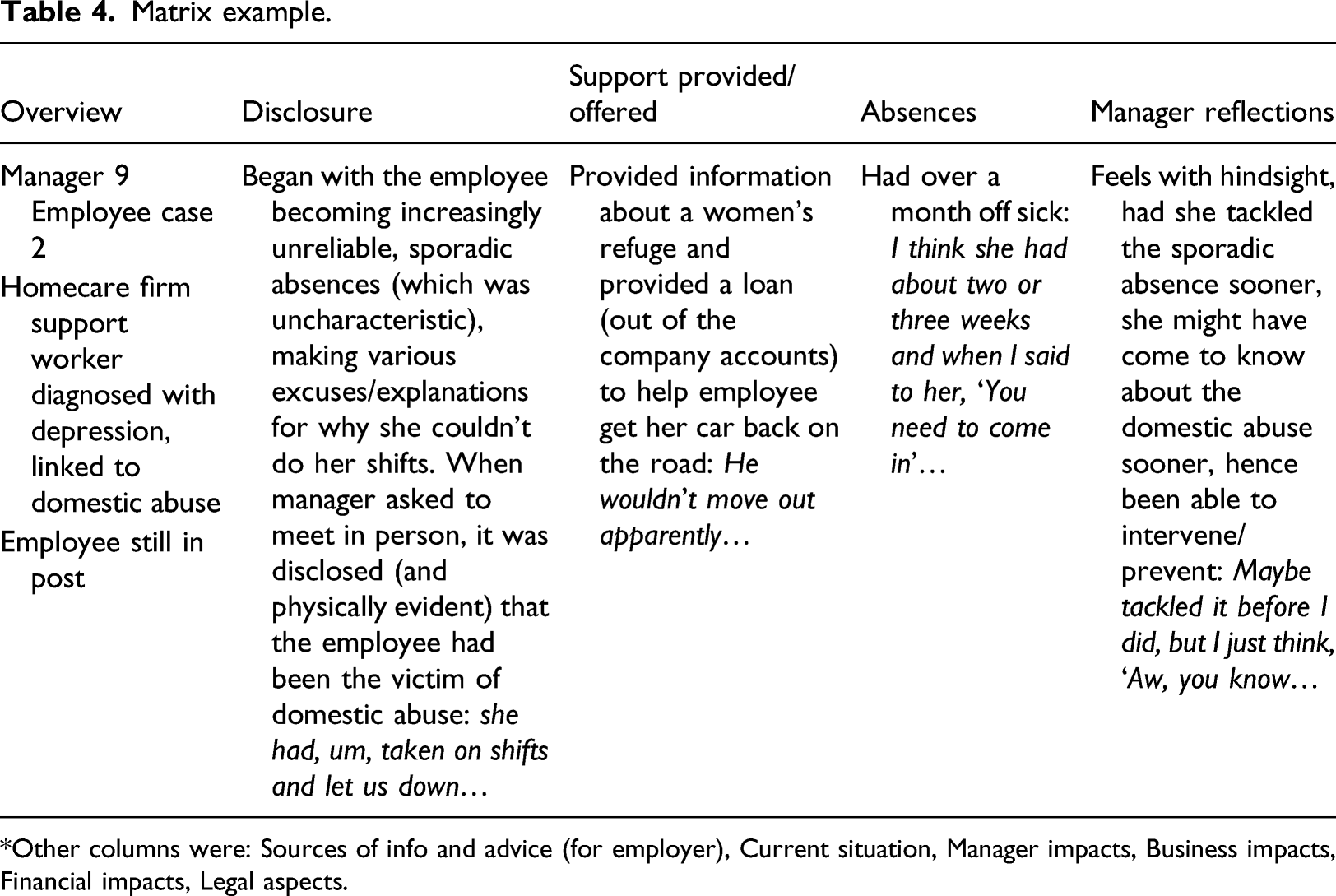
*Other columns were: Sources of info and advice (for employer), Current situation, Manager impacts, Business impacts, Financial impacts, Legal aspects.
Employee cases
Forty-five employee cases were described (see Table 2). These were not evenly distributed amongst the sample; experiences ranged from a single case, to managers who frequently encountered mental health problems among staff. The employees whose mental health problems were described held a range of roles and positions within companies, from trainee through to senior partner. Of the 45 cases described, 25 employees remained in post at the time of the research and 20 were no longer with the firm.
In recruiting to the study, we did not use any predetermined definition of mental health; rather, we adopted a broad conceptualisation encompassing the spectrum of psychological distress. Over two-thirds of cases involved common mental health problems, including anxiety, depression and stress. A smaller proportion were severe mental illnesses such as bipolar disorder. Some employees had engaged in self-harm or disclosed suicidal thoughts. A minority of cases involved substance use and addiction. Several cases represented ‘emergent’ mental health issues (Martin et al., 2018), where the effects of one or more stressful or traumatic life events such as work-related stress, physical illness, relationship breakdown, family pressures, abuse or assault, caring for seriously ill relatives, or suicide of a close family member culminated in the experience of depression and/or anxiety. Managers recognised the fluctuating and episodic nature of mental health (Gignac et al., 2020), describing employees whose mental health problems manifested differently, and sometimes unpredictably, over time.
Findings
We present our findings in two parts. First, we examine how managers navigate a continuum of support and performance practices in response to employee mental health problems. We then identify three key tensions for small and microbusiness managers that arose when traversing this continuum, and analyse how tensions are experienced by managers and how they use ‘either-or’ and ‘both-and’ strategies to respond to these tensions.
Navigating support and performance
Accounts of supporting employees through episodes of mental ill-health revealed a spectrum of management actions, from informal support through more formalised and structured support, to approaches closer to performance management (see Figure 1). This spectrum of actions demonstrate how managers needed to find an appropriate balance between, support that accommodated the employee’s symptoms and reduced capacities, and performance management actions that sought to catalyse the employee into improving and restoring required levels of productivity and conduct. In the course of supporting an employee, managers could move dynamically through this continuum, in either direction, and could implement a combination of actions. This was not a linear process for managers but rather it was iterative, bidirectional, and negotiated in light of tensions, which we identify and analyse in the subsequent section. The Support-performance continuum.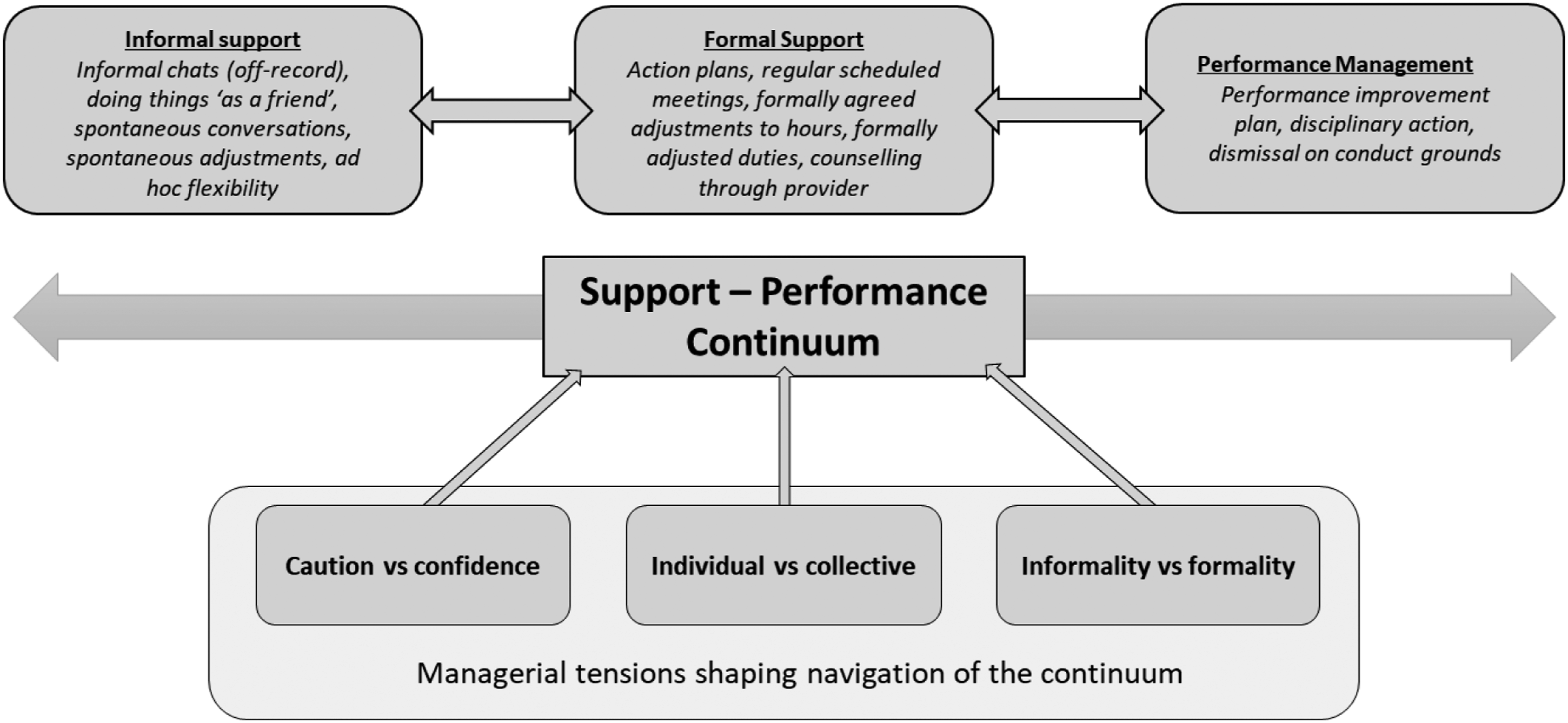
Three employee case examples illustrate dynamic ways managers traversed this support-performance continuum and demonstrate a difficult balancing act. As a first example, a manager of a homecare business with 30 employees (Manager 1) described the case of an employee with fluctuating depression. The manager first became aware of the employee’s mental health problems via concerns about their performance. Issues of concern included negative interactions with colleagues and their attitude and disposition more generally. This case involved a dynamic response. Initially a formal performance management approach was used, but the manager quickly modified this in light of disclosure of mental health issues during a performance improvement meeting. The manager utilised semi-formal support in the form of a written plan and a standing, yet ad hoc, arrangement to work from home. The arrangements appeared to be working well for the employee but retained some tensions for the manager in terms of resentment from co-workers who were not aware of the employee’s mental health issues and did not understand the differential treatment offered (i.e. flexibility to work from home on an ad-hoc basis). The manager also reflected that she was sometimes too cautious in responding to the employee. The manager remained aware of the need to be agile within the support-performance continuum, in response to potential future fluctuations in the employee’s mental health: ‘At the moment we're going through quite a good phase, but that can all change quite quickly’.
In a second example, a manager of a community development organisation with 21 employees (Manager 12) recounted a case of an employee with depression. After several months of poor attendance, the employee’s absence was broached as a performance issue: It wasn’t declared that they had depression when they started with us…The first six months were pretty good, in fact without any absences, and since then it’s been significant. And you just have to start saying, ‘Well look, you know, it’s having a proper impact on our ability to deliver and certainly reputation as well’ (Manager 12, Male: Community Development, 21 Employees)
In this case, a ‘capability’ approach was taken to managing the employee’s performance, involving a wellness action plan, disclosure of medical records, and a performance improvement plan focused on attendance. This manager was initially cautious, as he was concerned about how his actions might exacerbate distress if perceived as unsympathetic. The performance improvement plan initially led to improvements in the employee’s ‘attitude and behaviour’, but things had subsequently taken a downturn and a second phase of performance management was implemented. At this stage, the manager quickly took a formalised approach to support and whilst mindful of the risks of exacerbating distress through performance management, interventions remained in the performance management segment of the support-performance continuum. Tensions emerged in relation to the impact on service delivery and the effects of the employee returning to work when not fully productive. At the time of the research, this manager was still in an active stage of performance management, rather than a steady state of ‘successful’ resolution.
In a third example, a manager at a welfare support charity, with 33 employees (Manager 7) described a case of an employee experiencing PTSD, anxiety and depression, following a history of trauma and more recent domestic assault. This case exemplified a movement from informal support in the immediate aftermath of the assault, including practical and financial support to move to safe accommodation and an extended period of compassionate leave, significantly over and above standard allowances, through formalised action planning and role adjustment, to disciplinary proceedings when workplace conduct became unacceptable. The manager described the tensions inherent in balancing support and performance management, stemming from concerns of underperformance and the potential impact on co-workers: It does cross the border into performance management. It can’t not sometimes, because you end up with presenteeism then...and so that also has to be recognised and carried, and you have to ask yourself how much of that you can allow, you know. When would you be expecting to see people really kind of start to come back to performing at a better level? You don’t want to add to the pressures that people are under, but equally you do have minimum standards of behaviour, of performance and it’s how you manage all of that and, and I don’t think there’s a clear kind of straightforward answer (Manager 7, Female: Social Care, 33 employees).
This manager emphasised the emotional toil of traversing the support-performance continuum and navigating the tensions this entailed: ‘That whole conundrum of it, I find really challenging and really emotionally draining myself’.
Tensions in navigating support and performance
Tensions tended to arise when performance or conduct became an issue and/or where the employee did not engage with workplace adjustments offered. Managers variously referred to tensions as ‘very difficult to sort of walk that tightrope’; a ‘juggling act’; ‘spinning a lot of plates’; ‘always on the back foot’. Data revealed the emotional and cognitive demands of responding to these tensions. Often these emotions were negative where managers felt conflicted and torn. In other cases, emotions were more positive, particularly where managers felt they had successfully worked through the tensions. For example, a manager recounted the case of an employee she perceived as having supported successfully through mental ill-health whilst holding the needs of the wider business in balance: I think I actually felt better that I held the balance, I felt like I held the balance of the organisation a bit better – all the times we were discussing with her what she needed to do, I kind of felt like I was really holding in mind what we needed the business to achieve as well and making, just checking in with myself that I wasn’t going over the top because I wanted so, so much for it to work and be a nice person (Manager 13, Female: Community Development, 9 employees).
We identify three tensions that emerged in the small and microbusiness context as managers traversed the support-performance continuum: individual versus collective; confidence versus caution; informal versus formal. We illustrate in the following sections how these tensions give rise to ambiguity as managers attempt to navigate support and performance, and in our analysis we draw out the specificity to the small business context. We then examine the ‘either-or’ and ‘both-and’ response strategies used by managers, as categorised in Table 1, and, expose the emotional struggles revealed in manager accounts.
Individual versus collective
Several managers spoke about how close and caring relationships within small organisations could be conducive to supporting an employee with disclosed mental health problems, who needed periodic workplace accommodations. Data indicated that for disclosed mental health problems, many managers initially focussed on supporting the individual rather than problematising their performance and resultant impact on co-workers. However, this was sometimes temporary, as tensions between individual and collective needs arose: I think it’s still reminding myself that I need to bear in mind the impact on other people and the organisation, and not just the individual who’s struggling with the issue, whatever. I think that’s still something I need to develop a bit more, and I think I’d have done that differently in the first case, probably, particularly if I’d have thought about it more (Manager 13, Female: Community Development, 9 employees).
Over time the unwell employee could become an encumbrance on both the time and energy – and hence productivity – of co-workers. This could have an emotional impact on managers as they pursued simultaneous contradictory demands from both the individual and co-workers: It’s exhausting from all angles, because you’re trying to sort of balance everything… We were as open and honest as we could be with everybody [but] they don’t all know the full story (Manager 4, Female: Manufacturing and Sales, 49 employees). You’re putting those [co-worker] staff under pressure, which will then affect their mental health, and it just becomes a really challenging cycle to manage, and we are good at emotional well-being, support for our team, but even so, I think we have to be realistic that it doesn’t mean it’s an easy thing to do, and it’s a constant juggling and a constant managing things (Manager 7, Female: Social Care Provider, 33 employees).
Close social relationships within small workplaces meant that co-workers wanted to help, but could find their own mental wellbeing was affected by the emotional burden and build-up of work pressure. These issues were more apparent in organisations where staff worked in close proximity, a common feature of many small and microbusinesses. In some cases, all staff worked within one open-plan space or across just two or three rooms. We’ve got a very supportive team, and I think people do genuinely want to support each other, but that means that if somebody is feeling a bit down, somebody will take the time to talk to them – which is a positive thing, from a support side, but it takes time away from both people doing their work, and it also leaves people feeling a bit fed up, a bit sad maybe, or a bit worried about their colleagues. It doesn’t keep morale high (Manager 5, Female: Consultancy services, 30 Employees).
Over time, this could lead to a reduction in support and sympathy from co-workers, leaving the manager with challenging personnel issues to negotiate and smooth over: It’s remarkable how quickly people’s empathy just disappears. And then you’re having to manage the poor person…but at the same time, trying to smooth the ruptures that are going around in the background, where people are saying, ‘Well, you know, she’s got to sort herself out’ (Manager 2, Male: Primary Care, 20 Employees). Tolerance was very low with the rest of the team, because you can take so much for so long, and then every time she was off sick…So it does impact, and it does impact them because they’re trying to keep to time, [clients] don’t want to be running late, so the impact is everywhere, and the strain is everywhere for everybody (Manager 14, Female: Healthcare, 20 Employees).
Therefore, whilst a focus on the individual was initially successful, managers sometimes moved towards a selection strategy when the tension became salient, favouring the collective element and often taking a capability approach even when it was unclear this would benefit an individual. Some managers described the discomfort in making choices deemed necessary to move the situation forward. In the following excerpt, the manager describes the emotional and cognitive demands of responding to this tension: I suppose what I find hard is if I’m having to give tough messages...the hardest thing for me is feeling a little bit like a hypocrite, and that balance between genuinely caring deeply about the individual staff member and their issues and having to juggle and manage the impact of that on other members of the team [and] on the client group…[but co-workers] can’t keep carrying more and more and more and more, and working stupid hours every week, with no sign of it reducing, so you have no choice, as an employer…either they’ll be performance-managed back to a decent standard of work or they’ll be performance managed out of a job, and that’s shit. I don’t want that to be what has to happen at all, not ever for anybody (Manager 7, Female: Social Care provider, 33 employees).
Data also revealed that many managers attempted an adjusting response strategy that integrated and balanced the needs of individuals with that of co-workers through supporting individual needs whilst simultaneously smoothing ruptures and appeasing frustrations amongst co-workers: I found it quite stressful, to be fair. At the start of each day you could be quite apprehensive because you didn’t know just what was going to throw up out of that day, and what sort of- because you’ve not only got to manage the person who’s struggling, you’ve got to manage the other staff’s attitude towards them. And some others would be going, ‘Oh God, she’s skiving’ or ‘I’ve done all this and she’s only done that.’ So you’ve got that side of it to manage, as well as the actual person that is struggling (Manager 19, Female: Leisure, 10 employees). That lack of empathy really does start to be a problem. And yet, in my position, if you’re on as the manager, it’s then trying to sort of, you know, trying to smooth it over, because, you know, ‘Yes I know it’s a pain, but actually, you know, she has real issues here, and we have to be supportive’. (Manager 2, Male: Primary Care, 20 Employees).
However, in small, spatially proximate teams, the issue of employee confidentiality magnifies the individual-collective tension and so constrains the use of ‘both-and’ response strategies. Recall the manager at a homecare business with 30 employees (Manager 1), recounting the case of an employee with fluctuating depression. She described a personal support plan where the main provision was the employee working from home on days she found it difficult to be around people. Whilst working from home had been unproblematic for the employee’s duties, the manager described how this caused tensions with co-workers, who were unaware of the employee’s mental health issues and were discontented by this differential treatment: There’s quite a lot of resentment actually, from some members of the team. Because we can’t share the reasons behind, you know, the mental health. We can’t divulge anything like that, and it needs to be very confidential. I think they see somebody being treated differently and it can cause a little bit of tension sometimes (Manager 1, Female: Social Care provider, 30 Employees).
This inability to be open with co-workers, especially when the employee’s difficulties were obvious, could further exacerbate a sense of lowered mood or morale across the workforce. Some managers emphasised how this could be felt more acutely in small workplaces, where the usual climate was one of open and inclusive communication.
Co-workers were sometimes required to absorb the workload of an employee with mental health difficulties, when absent or less productive. In response, some managers described another adjusting strategy whereby they or senior managers absorbed the majority of the absent/unwell employee’s workload themselves to mitigate pressure on co-workers: If we do fall short, what ends up happening is that the senior team usually step in because it’s just easier to try and manage that, because the challenge is that some of these staff are quite fragile. So whilst we may be allowing one some time off to give them some freedom to go and get their support or time off for recovery, by asking somebody else in, you could actually end up impacting them and creating further stress for them. So we tend to try to avoid that just by the more kind of senior staff, and I guess some of the senior staff are quite resilient so they just step in if required (Manager 18, Male: Food production, 50 Employees).
This illustrates a context specific challenge as the impact of reduced productivity migrates upwards to senior colleagues. Indeed this tension may not become salient in larger organisations with more resources for workload to be absorbed into the wider workforce.
Confidence versus caution
A number of managers reported confidence in managing mental health problems, particularly where they had personal experience of mental health problems, or among close family members. Confidence also came with experience, both in terms of mental health expertise, but also with management experience. Yet, many also reported tension between a cautious and confident response. Disclosure of mental health problems was often indirect, with managers becoming aware of difficulties through observations of changes in employee performance, behaviour or presentation. There were instances where a manager’s initial enquiries were met with defensiveness or denial from the employee. This ambiguity and antagonism could foster caution from managers and undermine confidence, with some questioning their competence. Moreover, managers often found performance-related conversations difficult and emphasised how this was additionally challenging when issues of mental health were intertwined. Managers were often concerned their approach might exacerbate the employee’s difficulties, further undermining their confidence.
A manager of a small consultancy firm (Manager 5) described a case of a team leader experiencing panic disorder, depression and suicidal thoughts alongside a marriage breakdown. This case was ongoing for 18 months and the manager described a long period favouring a cautious approach. In the following excerpt, the manager expresses her regret at her cautious management approach and emphasises a greater willingness to risk any implications of a more confident approach in future: I wish, in hindsight, I’d have taken more decisive action earlier. I don’t know what that would be, but I think I should have tried harder to find a way to perhaps take them out of the business for a period of time. Because I think the toll that it took on those around them was too much...I think I should, in hindsight, I could have, I should have found a way, even if it put us at risk of legal action...So in hindsight, that is one that I wish I’d managed better, or more firmly (Manager 5, Female: Consultancy services, 30 Employees).
Even managers who were confident in addressing performance matters recognised the inherent tensions at the nexus of mental health and performance; they struggled to ascertain when it was reasonable to have a performance-focused conversation with a mentally unwell employee. Others expressed trepidation and fear of potential consequences if employees took the organisation to a tribunal on the grounds of discrimination, unfair or constructive dismissal. A microbusiness manager recounted a case of an employee with a combination of issues that initially was not recognised by the employee or manager as mental health related, but culminated in a diagnosis of depression and Obsessive Compulsive Disorder. The employee was ultimately dismissed on capability grounds after a year of workplace difficulties. The manager emphasised the challenge of disentangling symptoms and effects of mental ill-health, from unacceptable conduct that could reasonably be dealt with as such: In terms of a lot of the performance management, it felt quite murky, the relationship between behaviour and mental health. And what we were seeing and what was being said to us was often quite conflicting. And I found that, I think, probably particularly for a small business, I didn’t feel there was a lot of guidance in helping unpick that (Manager 6, Female: Consultancy services, 6 employees).
This manager used a selection strategy, again favouring the caution element. She also reflected on how she might be more directive about attendance and productivity at an early stage, however remained cautious as this conflicted with the informal employment relations climate: There’s maybe a few things we would have done differently, but they would have made quite significant changes to how we work, so I still don’t know whether – when it came down to it – we would be prepared to do it...I think, in terms of the earlier stages and the working from home and then not [actually] working and things, I mean, we could have forced that. We could have said, ‘You’re not working. You need to get signed off sick or you need to get on – do your work.'...but that’s not really commonly the way that we manage and work generally...I know what we should have done is challenge that behaviour...But, as I say, we chose not to (Manager 6, Female: Consultancy services, 6 employees).
Some managers had little or no experience of managing employees with mental health problems, as there had been few instances in their organisation’s history. The microbusiness manager recounting the case above described an absence of process experience and associated caution: We were particularly nervous. Because it’s a small business we’d never in the history of the business given anyone a formal warning at that point, so then to do that and then there also be [mental health factors], you know, we were very conscious that we didn’t want to be doing anything that was not the appropriate thing to do or that was out of line with guidance or that could be seen as constructive dismissal (Manager 6, Female: Consultancy services, 6 employees).
Informal versus formal
Managers described workplace contexts characterised by close informal employee-manager relations and so often took an informal approach to managing employee mental ill-health. However, some described a tension between their desire to support the employee informally as a ‘friend and colleague’, set against business requirements and a more professional formal approach: Where do you go from here? How do you help your employee? How do you help your friend? Because in small businesses, the people that work for you tend to get close…How do you protect yourself from not doing something completely insane and actually putting yourself and your business in danger because you’re trying to do something right but you’re actually doing something wrong? (Manager 16, Male: Consultancy services, 4 employees)
Moreover, a more formalised approach could sit in tension with the informal relationships within small and microbusinesses. Taking what was deemed a harsh line on performance management could negatively affect goodwill and morale across the wider workforce: In a small company, once things start being more formal, it makes all of those work relationships very difficult. In any small team, you rely on those informal relationships and the balance is always complex, isn’t it. But particularly with something like that [mental health] (Manager 6, Female: Consultancy services, 6 employees).
This manager described how it had been difficult to balance performance management and pastoral support, because – being a microbusiness with only herself in an employee relations role – both aspects of support had fallen to her, leading to a sense of inner conflict: I was the only one effectively that she was talking to about it and I was her, you know, her ultimate boss really in terms of how the business so it was a, yeah, it was a quite a conflicting thing to have to sort of manage...if there’d been an ability for someone else to take over one or other side of that I would have done that (Manager 6, Female: Consultancy services, 6 employees).
This illustrates how a separation strategy, where informal and formal elements are located with different managers or an HR function, is usually unavailable to managers in microbusinesses and some small firms. Managers lack the option of creating independent distance between support and more formalised performance management procedures, thus exacerbating the tensions felt.
Some managers separated the informal and formal elements temporally. Recall the case of Manager 7, with an employee experiencing PTSD, anxiety and depression. The manager initially responded with informal support in the aftermath of an assault and then responded with formalised action planning and role adjustment, and disciplinary proceedings when workplace conduct became unacceptable. Yet, this manager highlights her nervousness and being unsure how the employee would react to a formal approach: I don’t know if sometimes a formal process helps to put some boundaries in place, but you’ve got to really balance: would that formal process add weight to the trauma and the mental illness and the suffering, or would it actually redirect somebody down a healthy path…That was really hard because I’d spent months supporting her and through a horrific situation, and then I had to say, you know, ‘This is not okay, and it’s so not okay that this becomes a disciplinary issue...And that’s a very difficult conversation to have with somebody when you know that they’re already struggling (Manager 7, Female: Social Care provider, 33 employees).
However, as the manager described, clarity and direct addressing of inappropriate conduct was in this case an effective way to achieve the necessary performance longer term: We supported her hugely, immediately, on a practical level. We gave her emotional support. We’ve paid for her to have counselling, all the things we would normally do. But the minute she behaved inappropriately, we dealt with it formally. And I was nervous about it, because I didn’t know how she’d react, but actually I think it was fairer to her, and we were really clear that, ‘Actually, if this happens again, this is what will happen, and then this is the ultimate potential outcome, which is that you could lose your job’…She was clearly quite upset at the time, but her attitude has changed, and things have been better (Manager 7, Female: Social Care provider, 33 employees).
Data also revealed examples of a synergising strategy in response to the informal-formal tension, particularly with consideration of the unique value of the employee to the organisation. This is illustrated by a manager at an information and advice charity, with a remit that included provision of mental health support to clients, who recounted a case of an employee with long-term depression and anxiety: If [employee] most of the time was off work, or was hardly answering the phone, then yeah we would have to move down capability on the grounds of ill health. But that has to be severe…having her in the workforce, at times, if she’s unwell, she might answer less calls, which means that there’s less clients...but actually, having her in the workforce and what she brings in terms of her empathy of people and her understanding of many of the clients that come through our organisation, because she herself experiences things, balances that out (Manager 21, Female: Information and Advice Services, 49 employees).
This manager tried to minimise formal sickness absence and the impact for the employee of statutory sick pay by taking an informal flexible approach to where the employee worked, such as ad-hoc writing up case notes at home or working a flexible week with short and extended days with little or no notice: I was just like right, so is there any way that we can get you to still do your job and therefore we don’t class you as off sick? And that is part of the support plan as well. So if we have agreed with people, because of the types of roles that they hold, that they can work in a different way...then we say well, then that’s fine. If there’s no impact, then you do the work at the end of the week and therefore we don’t have to class it as sick. We only want you to be off sick when you can’t do the job. Um, whereas if you can do it, and you have mental health needs, in a different way (Manager 21, Female: Information and Advice Services, 49 employees).
Discussion
Through applying a tension-based lens, we analysed how small and microbusiness managers responded to tensions associated with traversing a support-performance continuum when managing employees with mental health problems. Our analysis revealed three tensions that arose within the small business context at the nexus of managing support and performance: individual versus collective; confidence versus caution; informal versus formal. These tensions emerged when managers were faced with performance or conduct issues, and when the close-knit social and physical proximity of small workplaces exaggerated impacts on co-workers. Tensions were evident even for managers with personal experience of mental health issues or working in sectors more literate in mental health.
The experience of managerial tensions when supporting employees with health problems is not exclusive to the small business context. However, our findings address an important gap in the literature: extending the current evidence base in highlighting how the intensity of these tensions, and their more immediate interpersonal consequences, distinguish the small business experience, constrained as they are within smaller social and more co-dependent social and managerial structures. In a large firm, there is greater staff resource to take up any shortfall, more opportunities to redeploy or redesign roles, and larger, multi-layered management infrastructures that can dilute the pressures felt by any given individual. Conversely, our findings illustrate how – in small businesses – attempts to balance tensions fall predominantly to one individual, and the emotional and cognitive toll this takes. The absence of discrete or specialist HRM and OH functions limits the extent to which expert parties are available to provide guidance and share the burden of support. Limited histories of managing mental health difficulties, alongside flattened structures, mean managers cannot draw on experience nor gain support or advice from peers. Moreover, findings demonstrate how, in a small business, the impact of one employee’s mental ill-health was felt more immediately, often quickly permeating the entire workforce. For small firms, finite resources and capacities meant there came a point where the limits of ‘reasonable’ adjustment were reached, and managers felt there was justification in taking a performance management or capability approach in the wider interests of the business. Together these contextual features shaped responses to tensions in these small and microbusinesses, all of which contributed to the complexity of managing mental health in these small workplaces.
Consistent with previous research (Gignac et al., 2020; Jansson and Gunnarsson, 2018; Ladegaard et al., 2019; Martin et al., 2018; Porter et al., 2019) our analysis reveals how the performance or conduct of an employee with mental health problems could affect co-worker workloads, and have a socio-emotional impact on morale and workplace relations. Whilst this may occur in any small team, the close social and spatial proximity characterising many small and microbusinesses, particularly where all staff are situated in one location, heightens this risk – permeating the psychosocial climate of the entire organisation. For small and microbusinesses, although a range of workplace adjustments and accommodations are feasible as illustrated by the support-performance continuum traversed by managers in this sample, it is the speed with which these become unsustainable which might be faster than in larger firms. The risk of overwhelming co-workers may be less likely in larger organisations with more capacity to redistribute work across multiple members of the workforce or with greater resources to recruit temporary cover. Indeed, managers often initially focused on individualised support without consideration of the wider collective. However, in cases where situations became unsustainable an individual-collective tension became salient and managers moved towards a selection strategy favouring the collective element, focussing on performance management and capability approaches, even in the awareness that this could be detrimental to individuals and potentially risk a tribunal. Some managers sought to balance the needs of the individual whilst smoothing ruptures and appeasing frustrations. Over time, this could result in managers having significant personnel issues to negotiate. This adjusting response strategy could be successful but was constrained by confidentiality and finite goodwill of co-workers.
Managers found performance-related conversations difficult and so often took a cautious approach. Limited experience of managing mental ill-health, as is the case for many small and microbusinesses (Barnes et al., 2009; Brohan et al., 2010; De Kok, 2005; Martin et al., 2020; Tu et al., 2021), impeded a more confident approach with managers reflecting that they would have acted with confidence earlier in hindsight. In the absence of prior experience, managers can feel under-confident and concerned about the employee’s emotional reaction (Martin et al., 2018). This is consistent with paradox theory, which suggests individuals vary in ability and resources needed to constructively react to salient tensions (Shao et al., 2019). We suggest the confidence-caution tension is difficult to synthesise or adjust in a small or microbusiness context where managers lack experience of dealing with mental health issues and have limited OH or HRM support. Some managers reflected that they might be more confident following their initial experience, yet were hesitant out of concern that a more proactive, confident approach might conflict with an informal employment relations climate. This implies that confidence building alone might not be sufficient to help small business owners navigate a support-performance continuum, as at times a cautious approach might be more appropriate.
An informal response was often favoured by managers, at least initially. A formal structured approach was useful in some cases, and managers reflected that in future they might be quicker to take up a formal strategy despite recognition of an informal-formal tension. More structured approaches can help employers to recognise and intervene in emergent issues at an earlier stage, and provide greater transparency and accountability for managers and the employee in the event performance management and capability matters are broached (Martin et al., 2018). However, managers in this study were concerned that a formal approach could damage close-knit relationships and conflict with an informal organisation climate. Kirsh et al. (2018) highlight the challenges of engaging employees in conversations that address both personal and workplace effects of mental health issues. As was evident in our study, managers can experience role conflict in reconciling personal relationships against maintaining professional distance (Martin et al., 2018). A separation strategy was used occasionally with an informal element held during one period and the formal at another. Managers in these small and microbusinesses were often solely responsible for employment relations, whilst also holding front line and line manager roles, leaving limited scope to delegate formal elements of performance management to a less closely involved party. This limits the possibility of a separation response strategy whereby the HR function might shoulder a formal performance management process. This was the only tension where data revealed a synthesis response strategy whereby managers developed new ways of managing situations when they valued individual strengths; for example, informal and flexible work schedules to mitigate need for formal absence. This reflects research indicating managers provide high performers with more flexible work conditions (Kossek et al., 2016; Remnant, 2019).
Our findings demonstrate how managers require agility and constant renegotiation of support and performance in light of tensions that become salient over time and according to context. We contribute to theory by taking a tension-based lens to bring into focus how managers work dynamically through tensions as employee mental health problems emerge and impacts become evident, striving to balance individual and collective needs and modifying the formality and assertiveness of their intervention. Paradox theory suggests that managers can deal with tensions in constructive ways, learning from the situation, emphasising the value of a ‘both-and’ perspective in complex situations. Conversely, dealing with tensions in defensive ways can lead to anxiety and paralysis. At the time of the research interviews, managers in the study were all able to reflect on learning points, but their accounts often suggested they had been through phases of anxiety and inertia. The ability of small and microbusiness managers to respond proactively to tensions were constrained by context. ‘Either-or’ strategies were found for all tensions and often resulted in pragmatic yet temporary solutions. These tensions were not solved by managers when they used an ‘either-or’ strategies as over time situations often broke down and managers remained conflicted and anxious. Research, policy and guidance on supporting employees with mental health problems typically seek to establish what works and what effective practice looks like. Our study has demonstrated that success is rarely, if ever, complete. Managing employees with mental health problems engenders inescapable tensions, continually negotiating a balance between support and performance. What works for one party in this equation may work less well for another, and what is working at one time may be less effective at another.
The study signals a number of policy implications. First, policy and guidance for small and microbusiness should recognise tensions arising in the small business context that shape management of employee mental ill-health at the nexus of support and performance, and the emotional and cognitive challenges these create. Ignoring this undermines the utility of that guidance, even when it purports to be tailored to a small business context. Second, mental health training as originally conceived, focuses on stigma reduction, symptom recognition and workplace adjustments (Tsutsumi, 2011). Our findings support calls for training to additionally focus on increasing manager confidence to broach emergent concerns, practical skills training on conducting difficult conversations and the time and space to practise these (Bryan et al., 2018). This would be especially beneficial for non-specialist managers in smaller firms. However, as noted above, this needs to be contextualised with an appreciation of how informal social relations might make a cautious approach more appropriate. Third, an important implication of our analysis is recognition of the significant psychosocial demand on small and microbusiness managers, when dealing with the complex array of practical and emotional impacts and dynamic processes involved in managing an employee through mental health difficulties. Small business owner-managers are already at high risk of occupational stress, burnout and depression (Cocker et al., 2013) exacerbated by the Covid-19 pandemic. We support calls for research and intervention to support manager wellbeing when faced with the cross-pressures of supporting employee mental health in parallel with attending to co-workers, productivity and profit (Ladegaard et al., 2019; Martin et al., 2020).
Limitations and future research
Due to the recruitment channels used in this study, the participating managers were, overall, relatively more engaged in the mental health at work agenda hence, unrepresentative of the wider population of small businesses. Whilst some managers had never proactively considered mental health in the workplace until confronted with their first employee case, we recognise that businesses in a lesser state of engagement and readiness to respond were underrepresented. Echoing Kristman et al. (2016), future research needs to examine experiences of small businesses that are not predisposed to engaging with employee mental health. However, the balance within the data of positive and challenging experiences reassures us against self-selection bias. We also acknowledge that our focus on manager experiences means we have only one side of these stories. We wish to recognise the employees whose lived experiences were relayed via their managerial’ perspectives, and are conscious that their own version of events may be different. The UK focus of this study is also a limitation to wider applicability of findings, for example, in relation to countries where legislative frameworks and employer healthcare/insurance responsibilities differ, or where small business guidance and intervention on mental health is more extensively embedded.
Data reflected the heterogeneity of both small businesses and mental health experiences. Within the sample, firm resources, and so, manager experiences, differed markedly within the small categorisation. Formality increases with business size, with influential changes occurring at around 20 employees (Storey et al., 2010). Larger-scale qualitative research is necessary, including sectoral segmentation and finer gradation of business size. This research paves the way for further research in the creation, and evaluation, of more context specific guidance to better support small to microbusinesses as they navigate challenging circumstances, not only for the unwell employee, but also for managers, co-workers and the business itself. Specifically, our study highlighted the role of and impact on co-workers within a small workplace, when employees experience mental ill-health. Co-workers have been described as important, but often invisible, players in the workplace support and accommodation process (Tjulin et al., 2010). Their efforts and ongoing willingness to be flexible and accommodating around the needs of an unwell colleague can be critical to the sustainability of their work productivity (Dunstan and MacEachen, 2014); future research should further illuminate this dynamic in the small and microbusiness context. Finally, the manager accounts reveal the significant impact that supporting employees through mental health problems may have on their own sense of psychological wellbeing, signposting another avenue for future research.
Conclusion
This study illuminates the first-hand experiences of small and microbusiness managers who supported employees through mental health difficulties, an area lacking in empirical evidence within the workplace mental health agenda. Using a tension-centred lens to frame our findings, we revealed a picture of small and microbusiness managers ‘juggling on a tightrope’ as they navigated a delicate balancing act between support and performance management. We identified three key tensions: individual versus collective interests, confidence versus caution in approach, and informal versus formal management strategies – all of which were intensified by close psychosocial and spatial proximities of the small business environment. We conclude that these tensions are perhaps irresolvable, but point to implications for more tailored and context-sensitive policy and practice in the area of workplace mental health.
Footnotes
Acknowledgements
We are grateful to the 21 study participants who shared their experiences, and to the organisations and individuals who assisted with recruitment by promoting the study among professional networks. Grateful acknowledgement of three academic reviewers who provided constructive criticism that improved earlier drafts of this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of York Research Priming Fund (2019–20).