
Abstract
Communication partners are instrumental in the successful use and implementation of augmentative and alternative communication systems (AAC), especially in schools, but stakeholder views from low- and middle-income countries (LMICs) are not well represented in the literature. Focus group interviews with seven professionals and three caregivers from South Africa were conducted to understand their perceptions and experiences of AAC use and implementation. The results highlighted additional issues which practitioners in LMICs need to consider when implementing AAC in under-resourced schools for learners with special education needs. Although some challenges overlap with those experienced in high-income countries, such as support and training, high staff turnover and burnout, large caseloads and language and codeswitching differences, these challenges present differently in low-income contexts, requiring alternative solutions. High-income countries do not often need to consider the risk a high-tech AAC device places on the child and their family due to the risk of crime in low-income contexts, the device affordability, the device features and the range of accents available when introducing an AAC system. This exploratory study suggests that LMICs, like South Africa, could make great strides towards providing appropriate AAC technology for all if i) strategic partnerships between governmental and non-governmental groups were put in place, ii) appropriate communication, training and support systems were established, and iii) evidence-based core-language AAC systems were created.
Keywords
Introduction
Effective augmentative and alternative communication (AAC) depends on both the AAC user and their communication partners (National Academies of Sciences, Engineering and Medicine, 2017; Kent-Walsh et al., 2015; Moorcroft et al., 2019b). AAC is an important option for children with complex communication needs (CCN), reducing barriers to communication, increasing opportunities for language and literacy development, and ultimately improving their quality of life (Leonet et al., 2022). Children with CCN may not develop typical speech, language, and communication skills due to motor, language, cognitive and/or sensory perceptual impairments. AAC is divided into three categories: no-tech, low-tech, and high-tech. No-tech AAC uses facial expressions and motor movements, such as manual sign. Low-tech AAC involves basic communication devices, such as paper-based communication boards and books, whereas high-tech AAC includes speech generating devices and other computer and tablet-based technologies to send a verbal message (Leonet et al., 2022). Equipping schools with the tools they need to provide inclusive education, not only assists children with CCN but also helps children at risk for difficulties with learning and literacy (Kathard et al., 2011). When schools train teachers on the importance and relevance of AAC, whilst providing them with resources to adequately support the children, the children thrive (Moorcroft et al., 2019a). Moreover, peer scaffolding, when peers demonstrate a skill and offer support, assists the child using AAC and their peers. Peers develop language, social and academic leadership skills, whilst also increasing awareness and acceptance of AAC use (Finke et al., 2009).
Traditionally, AAC support has focused solely on individuals with CCN whilst neglecting the needs of caregivers, service providers, peers and other communication partners (Light et al., 2019). Early AAC intervention is paramount for early communicative success, and intervention effectiveness ultimately relies on acceptance and modelling of AAC by communication partners (Moorcroft et al., 2019b). Despite the need for AAC, challenges often occur which result in the rejection or abandonment of AAC systems by children with CCN and their families. To understand why AAC systems are underutilised, Baxter et al., (2012) conducted a systematic review of barriers and facilitators to the provision and use of high-tech AAC systems between 2000 and 2010. Moorcroft et al. (2019a) undertook a similar review, considering the barriers and facilitators to the use of low-tech and unaided AAC between 2000 and 2016. These reviews found that rejection rates dramatically increase if communication partners are not familiar, or do not fully accept the AAC device. The perceptions of speech and language therapists (SLTs), teachers, caregivers and peers about factors that contribute to the acceptance, rejection or abandonment of AAC systems – and their attitudes towards users of such systems – has been discussed (Baxter et al., 2012; Dada et al., 2016; Moorcroft et al., 2019a, 2019b; Tönsing and Dada, 2016; van Niekerk et al., 2019). However, less is known about the specific challenges encountered by stakeholders when introducing AAC systems within special education settings in low- and middle-income countries (LMICs), and potential ways to overcome these challenges.
Despite the evidence indicating that communication partners play a crucial role in the successful use and implementation of AAC systems (National Academies of Sciences, Engineering and Medicine, 2017; Kent-Walsh et al., 2015; Moorcroft et al., 2019b), there are limited studies considering the perspectives of stakeholders from LMICs (Mukhopadhyay and Nwaogu, 2009; Tönsing and Dada, 2016; Tönsing et al., 2019; van Niekerk et al., 2019; Wormnaes and Malek, 2004). Research from high-income countries often serves as the gold standard for AAC intervention. However, additional challenges are experienced when implementing AAC in under-resourced and low-income contexts (van Niekerk et al., 2019). For instance, there is a lack of AAC knowledge and skills amongst teachers and SLTs in many African countries, such as Botswana, Egypt and South Africa (Mukhopadhyay and Nwaogu, 2009; Tönsing et al., 2018; Wormnaes and Malek, 2004). Less than 50% of the Egyptian participants in Wormnaes and Malek's (2004) study felt that they were sufficiently qualified in the field of AAC, despite working with individuals with little or no functional speech, and the majority of the participants in Mukhopadhyay and Nwaogu's (2009) study in Botswana displayed negative attitudes towards AAC. Tönsing et al., (2018) discussed how the skills of AAC service providers in South Africa are often limited when designing and implementing AAC systems and techniques in multiple languages. In order to provide some background to this study, the South African context will be further described.
The South African context
South Africa's official language policy allows schools to select any of the 12 official languages as the language for learning and teaching. However, multilingualism, multiculturalism and the diverse range of social issues can make it difficult to ensure equality in all educational spheres (Pascoe and Norman, 2011). Speakers of indigenous languages are often under-served due to the lack of contextually relevant resources in African languages, including AAC, and the language mismatch between professionals and the children/families they serve (Kathard et al., 2011; Pascoe and Norman, 2011). It is estimated that approximately 63% of children in South Africa come from poor households (Statistics SA, 2020), many of whom face a higher level of crime, overcrowded living situations, generational illiteracy and increased trauma and violence (van Niekerk et al., 2019). These environmental barriers have a negative impact on children's access to education and many of South African children from poor households do not obtain the exit requirements from secondary school which would allow them to make use of tertiary educational opportunities.
In addition, the South African Department of Health (responsible for the implementation of early intervention) is only able to meet 25%–65% of the total assistive products required, despite providing healthcare services to over 80% of the country (Visagie et al., 2020). Once children requiring AAC reach school-going age, they are referred to the Department of Education for continued intervention (van Niekerk et al., 2019). Unfortunately, many children are lost in the system due to limited resourcing and poor coordination at these transition points (van Niekerk et al., 2019). In addition, up to 70% of school-going age children with disabilities do not even attend school in South Africa. Of those who do attend, most are still in separate special schools for learners with disabilities (Donohue and Bornman, 2014) where both rehabilitation personnel, and suitable assistive technology are not always available (van Niekerk et al., 2019). Although South Africa is moving towards an inclusive education system (South African Department of Education, 2001), the implementation has been slow, largely due to poor policy directives, the large number of students in mainstream classrooms, lack of funding and a lack of support for schools and teachers (Donohue and Bornman, 2014).
With this in mind, strategies used in high-income countries, to provide learners with appropriate AAC technology, may not be applicable in LMICs. Considering stakeholders’ roles in the acceptance of AAC, the aim of this exploratory study was to document multiple stakeholders’ experiences, perceptions of implementing AAC in their context, and their ideas for overcoming the challenges surrounding the use of AAC within schools for Learners with Special Education Needs (LSEN) in South Africa. The research question was therefore: What are the perspectives of teachers, SLTs and caregivers on the implementation of AAC systems for children with CCN in South African education settings, and how do these perspectives reflect the challenges and opportunities of AAC implementation in LMICs, such as South Africa? There were three research objectives: (1) To examine the perspectives of teachers, SLTs, and caregivers regarding the current accessibility and effectiveness of AAC systems when faced with varying levels of resources, (2) To explore the challenges faced by these professionals and caregivers in implementing AAC systems in a LMIC, such as South Africa, and (3) To identify the support needed for professionals and caregivers in LMICs, such as South Africa, to improve AAC implementation.
Method
Qualitative approach
This project is part of a larger study where naturalistic synthetic child speech was created for three children with CCN, in three languages, namely South African English, Afrikaans and isiXhosa. Prior to the participants hearing the synthetic voices, face-to-face focus groups were conducted to determine AAC implementation challenges currently faced by participants. Thus, a descriptive qualitative design was used during this exploratory project as it allowed the researchers to obtain detailed descriptions from several stakeholders (Terre blanche et al., 2006). We anticipated that participants’ perspectives would highlight key challenges, resource limitations, and varying views on the accessibility and effectiveness of AAC systems in the context of a LMIC, such as South Africa. This exploratory focus group study does not seek to confirm predefined predictions or reach consensus on specific points, but rather to gather rich insights into the issues at hand, which will extend our understanding of the topic (Liamputtong, 2011). For this study we used purposive sampling as the participants were selected based on their relationship to the three children for whom the synthetic child speech was created. Participant selection criteria included familiarity with at least one of the three child participants, including their specific needs and difficulties; and the ability to participate in focus groups conducted in English. In this study, two focus groups were conducted after working hours, in a school setting. One focus group included caregivers of the three children with CCN whilst the other included teachers and SLTs who work with children with CCN. Two focus groups were conducted to ensure that power imbalances did not occur between participants.
Ethical approval for this study was obtained from the Human Research Ethics committee (HREC no. 765/2021) at a South African university and followed the guidelines outlined in the Helsinki Declaration of 2013 (World Medical Association, 2013). The appropriate provincial education department and the relevant school principals gave permission to access the schools. All participants were asked to maintain confidentiality, and each participant had to be legally competent and informed before they were invited voluntarily to sign a consent form.
Participants
Purposive sampling was used, with researchers primarily recruiting participants within three LSEN schools in Cape Town. Figure 1 shows how participants were selected. Once the three children were selected for the larger study, the adult participants (professionals and caregivers), were selected by moving outwards in concentric circles. Therefore, the participants were familiar with at least one of the child participants, including their specific needs and difficulties. Participants with different linguistic backgrounds were selected to reflect the multilingual context. Most participants were recruited from three LSEN schools, with the exception two professionals who were recruited via social media.
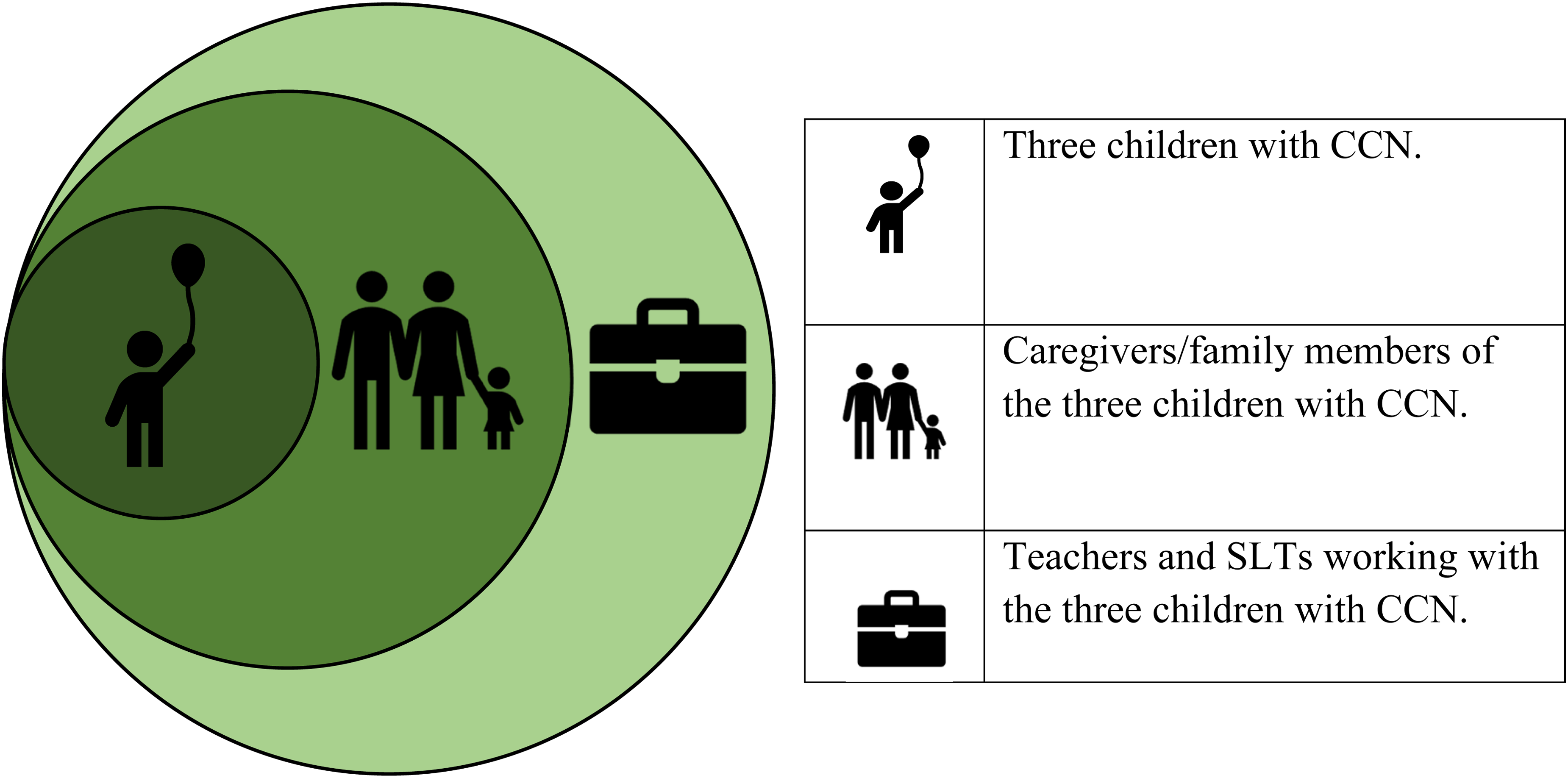
Participant selection process.
Six caregivers gave written consent to participate, but three were unable to attend on the day. Thus, only three adult caregivers participated in the focus group (x̄ age = 47 years old). Two participants were mothers of children with CCN whilst another was a grandmother of a child with CCN. Although the children were encouraged to use AAC at school, the caregivers were not yet exposed to AAC, as the children were not allowed to take their school AAC devices home. The children's diagnoses included autism spectrum disorder, significant intellectual disability and cerebral palsy (x̄ child age = 10 years old).
Professionals
Twelve teachers and SLTs gave written consent, but only seven were available to participate (x̄ age = 37 years old). Participant A consults with LSEN schools, trains SLTs in the area, and has extensive experience with both high- and low-tech AAC systems. Similarly, Participant B previously worked at a company specialising in assistive technology, where she trained caregivers and implemented various AAC systems, and currently works in a LSEN school, where high- and low-tech AAC are available. Participant C has access to both high- and low-tech AAC at her LSEN school but reports that she mainly incorporates low-tech AAC into her sessions. Participant D has experience implementing low-tech AAC in both private and public practice and has previous LSEN experience. Participant E mainly incorporates low-tech AAC into her sessions as there is currently only one child in her LSEN school who has access to a high-tech device. Participant F has had high-tech AAC in her LSEN classroom for the last 3 years, following a donation of high-tech AAC systems to her school. Lastly, Participant G has limited experience implementing low-tech or high-tech AAC, although it is available in the LSEN school, as they rely primarily on manual sign. Table 1 outlines the participants’ key sociodemographic characteristics.
Professional focus group participant demographics (n = 7).
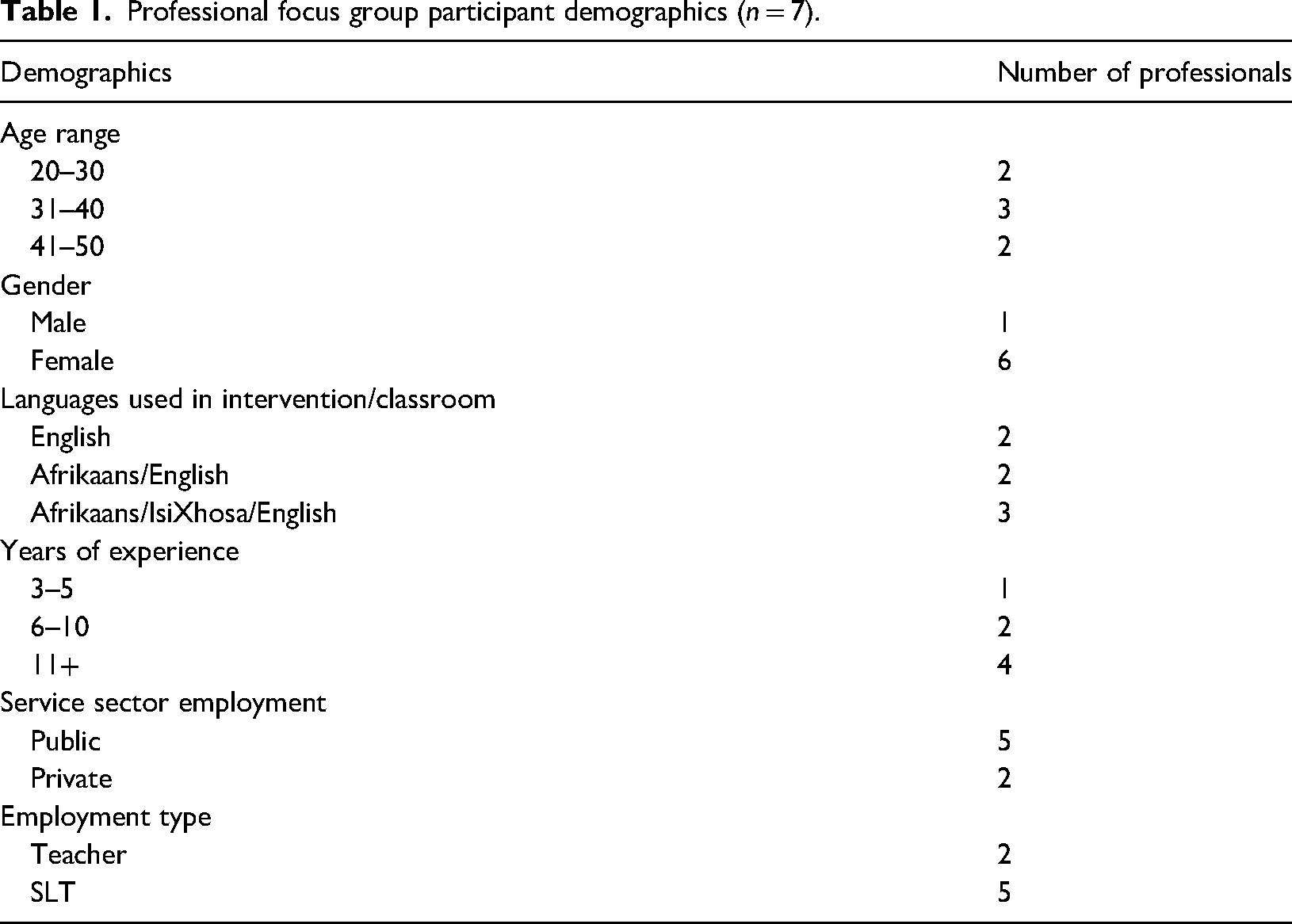
Professional focus group participant demographics (n = 7).
The data were collected during two focus group sessions, lasting approximately 1.5 h each. Separate interview schedules were devised. The facilitator asked topic-related descriptive questions to guide the discussion, starting with general questions (e.g. ‘What is it like communicating with your clients/children?’) and proceeding to the research questions (e.g. ‘What challenges have you experienced, implementing/using AAC in South Africa?’) (Terre blanche et al., 2006). To ensure credible data, focus groups were audio recorded and immediately following each group, typed transcripts were prepared. To maintain anonymity, no identifying information was recorded in the transcripts. Transcripts were provided to the participants for member checking, and none indicated they required changes.
Data analysis
Verbatim transcripts of the discussions were analysed via thematic analysis in a five-stage framework approach, using NVivo (QSR International, 1998). According to Braun and Clarke (2006), thematic analysis identifies and analyses patterns of meaning in a dataset. In stage one, data familiarisation, the transcripts were reviewed, and patterns were identified. Initial codes were generated in stage two. Codes identify interesting features of the data (semantic content or latent) and refer to the most basic element of the raw data that can be assessed in a meaningful way. In stage three, themes were identified and all relevant extracts from the transcripts were collated and categorised. The themes were refined and reviewed in stage four, for example, some themes were merged. In stage five, defining and naming the themes, the themes were divided into sub-themes, and the data were analysed and further refined. Two judges independently applied the coding framework to the interview data. Discrepancies were discussed until consensus was reached and 100% agreement between the two judges occurred, ensuring validity and reliability of the analysis and the identification of key information.
Results
Caregiver focus group
Themes and subthemes that emerged after analysing the caregiver focus group are presented in Table 2. Two themes emerged from the data, namely, device suitability and benefits.
Identified themes, subthemes and examples discussed by caregivers.
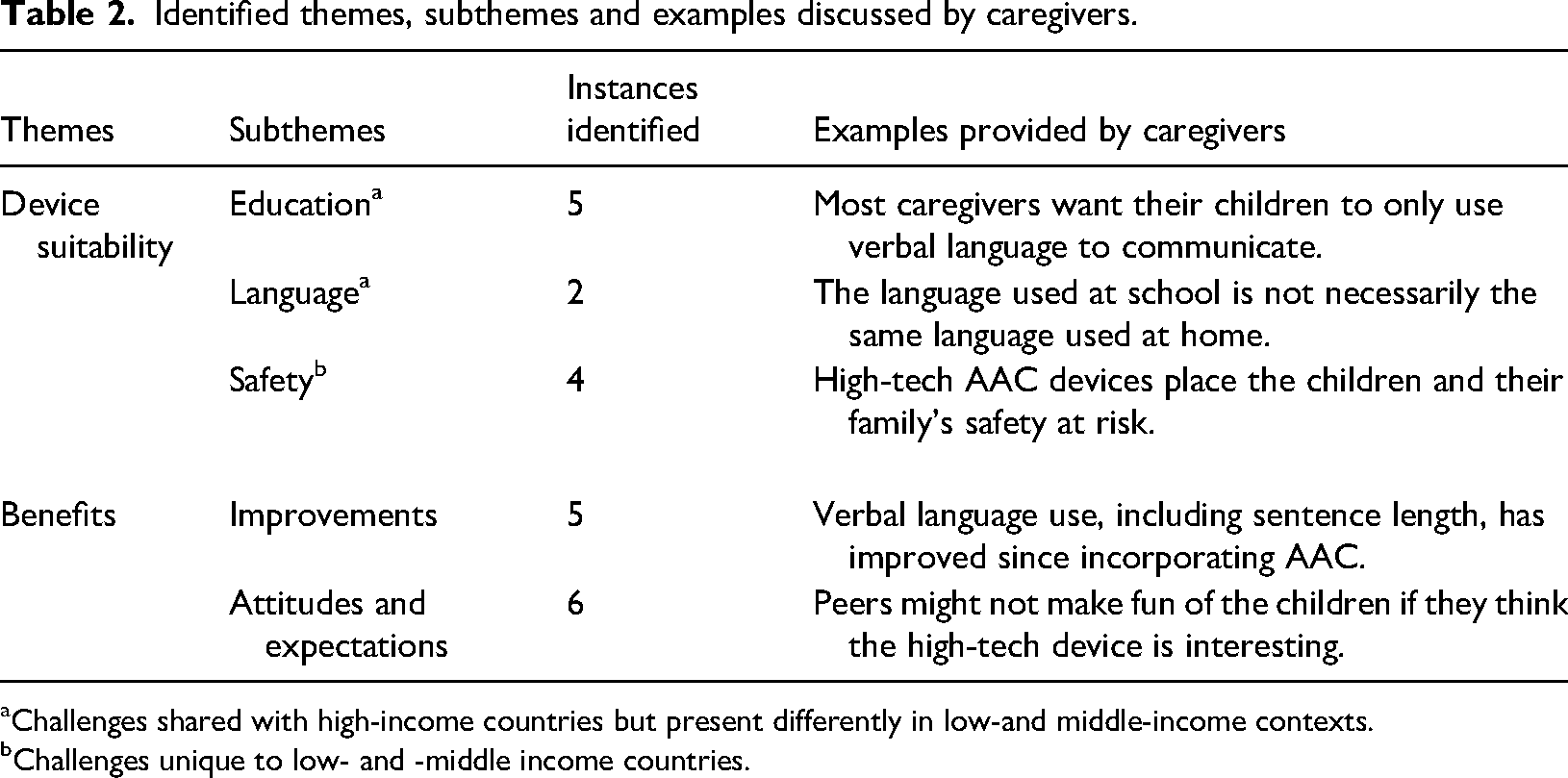
Identified themes, subthemes and examples discussed by caregivers.
Challenges shared with high-income countries but present differently in low-and middle-income contexts.
Challenges unique to low- and -middle income countries.
The device suitability theme encompasses the appropriateness of using high-tech devices for particular families, and situations. Three subthemes were identified, including education, safety and language.
Caregivers reported feeling ill-informed about alternative forms of communication. During discussions surrounding AAC knowledge, one caregiver stated, ‘we have a lot to learn.’ In addition, some caregivers acknowledge that they have never learnt how to communicate with their children who have CCN: ‘He cannot speak at all, so he uses [manual] sign … I don’t know [manual] sign at all’. Another caregiver highlighted a preference for spoken language, ‘because we [family] don’t actually want him to use [AAC]. We want him to speak’. This was echoed by another caregiver who said ‘we also prefer talking to [manual] sign … Otherwise, when are they going to learn to talk?’ Caregivers also indicated that AAC devices should only be used at school, where children are safe and supported, ‘he will sit with that [AAC device] at school because [the SLT] is there to help him…’
With this in mind, if caregivers don’t feel comfortable using AAC at home, then the child's AAC exposure and interaction is limited to the classroom. However, the language used at school is not necessarily the language used at home, which further hinders AAC use at home as one caregiver pointed out, ‘his teacher mentioned that he speaks English with her [but he] speaks Afrikaans at home’. Although many children become multilingual over time due to the variety of languages spoken at home and at school, ‘they want to [teach] him isiXhosa at school’, and ‘he is Afrikaans … [but] when he is cross, he complains in English’, AAC devices are often not representative of this diversity.
Additionally, caregivers raised concerns for their child's safety while using high-tech AAC devices and would prefer the devices stay at school. They are concerned that theft of the device may occur from their home or while on public transport, placing the child and family at risk. One caregiver stated ‘because outside, they will break the [AAC device]. They will either take it from him or break it … and he can’t come back and say that [person] took it or what happened to the [device]’. Caregivers were also concerned about the safety of the device software. Typically, passwords are required before updating AAC software, but they believe their children will bypass these safety precautions and delete important components by mistake, ‘We will be worried [about the AAC software] because [child] is always deleting games and stuff [on our phones]’. Finally, due to the broader community's lack of understanding about AAC use, caregivers expressed concern that their children may be bullied, ‘I think they will make fun of him if he [goes] outside with the [AAC device]’. One caregiver mentioned that due to this ‘he doesn’t speak or play with [neighbourhood children] anymore’. The caregiver explained that the child only plays ‘at school with his new friends’ where peers are more exposed to different forms of communication.
Benefits
This theme encompasses the benefits experienced by caregivers who have children that use AAC. It has two subthemes, including improvements, as well as attitudes and expectations.
Although some caregivers were hesitant about using the device, one caregiver stated that they noticed improvements in their child's verbal vocabulary and sentence length after using the device at school, ‘he is catching up nicely now’, while another mentioned that ‘he couldn’t speak at first, but he is starting [after AAC]’.
One caregiver shared her concerns about the expected poor attitudes of children as ‘kids might make fun of him’ for using the device, but another suggested that having a high-tech device would likely encourage ‘other children to play on it or do the same thing’ and this would be ‘exciting.’ They expressed that children's attitudes might change over time as the AAC technology ‘would be interesting’ for them.
Professional focus group
Themes and subthemes that emerged after analysing the professional focus group are presented in Table 3. Five themes emerged from the data, namely, support and training, device and software, education system, language and code-switching, and AAC benefits. The lack of support and training was the greatest challenge described by professionals.
Identified themes, subthemes, and examples discussed by professionals.
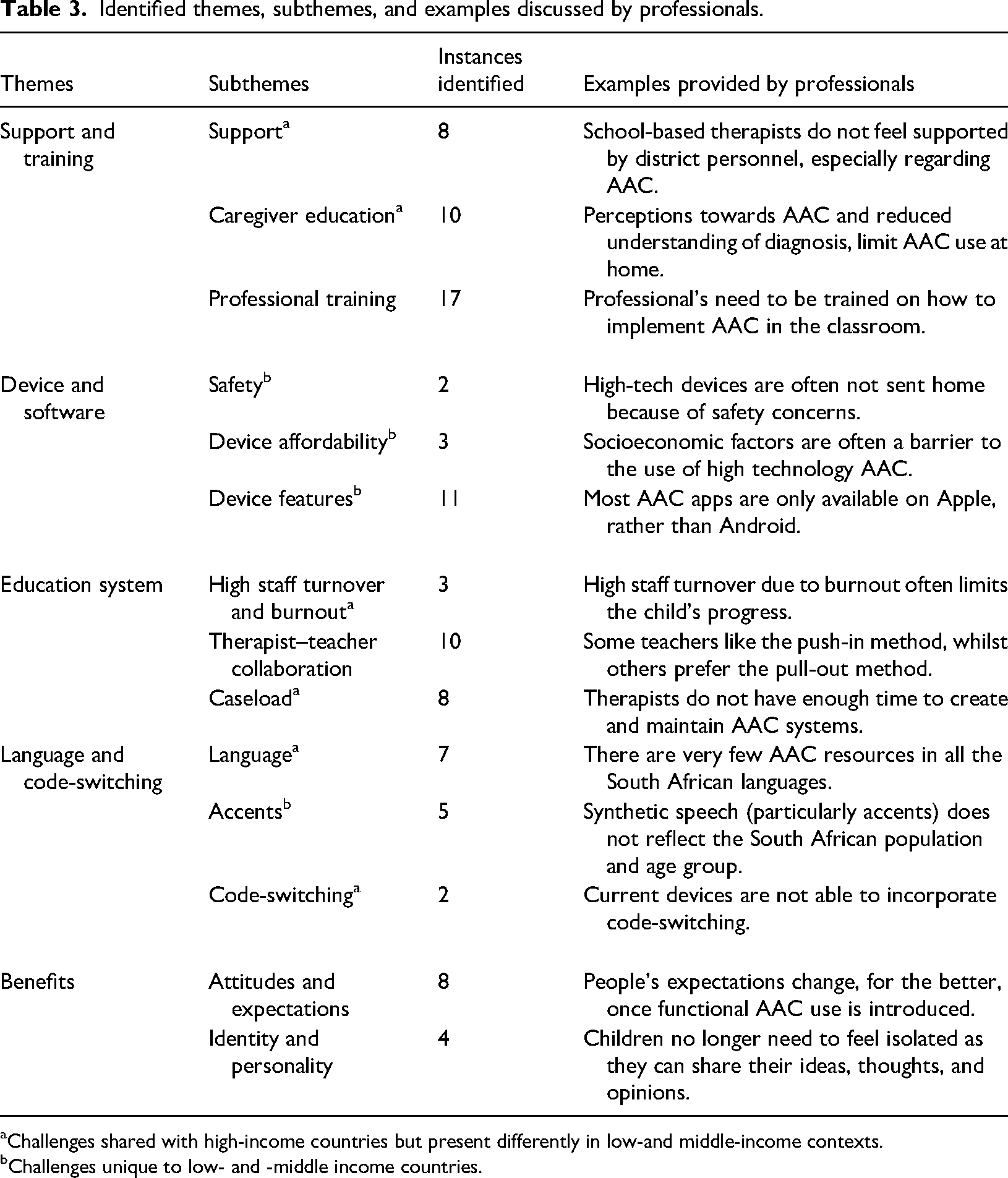
Identified themes, subthemes, and examples discussed by professionals.
Challenges shared with high-income countries but present differently in low-and middle-income contexts.
Challenges unique to low- and -middle income countries.
This theme outlines the imperfect support structures and limited training opportunities often experienced by professionals. Three subthemes were identified, including support, caregiver education and professional training.
SLTs reported feeling unsupported by the district level support staff within the education system. One therapist shared her experience as a senior SLT in a LSEN school: The school didn't employ me; the Department of Education employed me. I had a district therapist, who did not support me in the way that I needed, who did not allow me to support others in the way that I wanted. When I started, all the schools met [at an AAC forum] …. And as soon as funding became involved, the district therapist said, ‘you're out of line, this is now district level, we’re taking over’ and it stopped. The school [was] lovely, amazing, incredible; beyond the walls of the school? Lack of support, like you can't believe.
This lack of support is sometimes also felt at a school level as many have ‘never had a senior therapist’ who could assist with AAC decision making. The few SLTs who could speak to a senior SLT indicated that it felt like ‘a weight off [their] shoulders’. One SLT expressed: ‘We did our best with what we had but with very little support or anything that came with the AAC. There were probably six kids that would have definitely benefited [from AAC] so it was a shame that there was nothing that we could do’. Another SLT described the impact of this lack of support on the sustainability of AAC use: Until everyone's not working in individual schools and individual silos trying to make something happen … And the people who employ us, the people who support us, don't start putting systems/support/training in place – It's always going to be individual teachers, individual therapists, trying their level best for years until the next person comes and tries their level best for years.
Educating caregivers about their child's diagnosis and AAC system was another important subtheme. Professionals feel that it may be unrealistic to expect them to start incorporating AAC immediately after receiving a diagnosis. One SLT shared their perspective: But in my experience, 90% of people are in survival mode, before disability even hits your family in [South Africa]. We are all trying to be safe, people are all trying to make money … And then you get a child with a disability that adds so much, that most of us in privileged situations will never understand.
The professionals revealed that sometimes caregivers do not fully understand the implications of their child's diagnosis and ‘the parents don't come into the schooling environment’. SLTs feel that helping caregivers understand the purpose of AAC could improve their perception of AAC use. One SLT said: When I say the parents don't get it, I put that on us and myself … because I haven't done the right job. If they're not getting it, it's because I haven't found the right way to help them get it or I haven't identified what's important for them and I'm not addressing their needs, which is key.
The participants also mentioned limited professional training as a concern. Some teachers working in LSEN schools are not given enough training at an undergraduate level to educate children with special needs. This is further compounded by that fact that, Those kids who look, sound, act more severely disabled, who, for the most part are our AAC kids, are the ones who are left with less trained staff … it's not always the case- it is changing- but that legacy, [still] exists in a lot of our schools.
Furthermore, SLTs mention that AAC resources are often underused in the classroom, ‘my low-tech stuff is hidden away somewhere’. One teacher indicated that ‘if you want [school-based AAC] to work, you have to invest in the teachers and empower them …’ It was discussed that teacher training should focus on giving teachers ‘the tools’ necessary for using AAC in the classroom, rather than training teachers on how to teach the vocabulary. Some teachers have stated that they learn best when SLTs share resources and model how to use AAC. One teacher said, ‘a lot of their things I imitate, and I ask them to email me this resource and that…’
Similarly, the SLT's revealed that they are also given limited undergraduate AAC training before they are expected to train others to use AAC. One SLT said: ‘You look online and there's lots of lovely, very long, convoluted articles about AAC, that's very helpful, but show me actually how to do it because in [university], I didn't do it’. One SLT shared that ‘it fell on me as a therapist to programme the devices’, which wasn’t prioritised in undergraduate training. SLTs expressed: ‘I’m learning [about AAC] as I go’ and indicated that they want a ‘step-by-step guide’ that they can work from towards sustainable AAC implementation.
Device and software
The device and software theme encompasses professionals’ perceptions of the limitations of high-tech devices in under-resourced settings, with three subthemes: safety, device affordability and device features.
Professionals mentioned that taking public transport can be dangerous when children have high-tech devices. SLTs also reiterated caregivers’ concerns, ‘if mom says, “I'm really not comfortable, our home's not safe. Having [a high-tech device] in our home is going to put us at risk”. I don't want that for any of my [clients]. Okay, then the low-tech goes home’.
Professionals highlighted device affordability as a barrier to high technology AAC implementation. The professionals would like learners to have assistive devices. However, they reported that schools do not have the financial resources to provide assistive devices, and most of the families ‘can't afford that technology’. One SLT shared their experience, ‘some of my [clients] use low-tech picture-based systems, but I'm trying to move them on to high-tech, but because they are so expensive, we've had to do a lot of fundraising. So that has been a challenge’. Many schools are not comfortable sending high-tech devices home because of the excessive replacement cost. One SLT mentioned: ‘But the iPad breaks, the charger doesn't come in, we have [extended periods with no electricity], the screen gets smashed, it just freezes …’ Access barriers limit AAC use in LMICs, although there are clear benefits for children's communication. For example, some families do not have access to electricity, and professionals do not necessarily have the resources to implement a functional AAC system: ‘I only used low-tech because there was no high-tech … And we didn't even have internet … So, it was whatever I [could] find at home.’
Device features must also be considered in LMICs. One SLT mentioned that ‘the majority of AAC apps, and particularly the [evidence-based] ones, are actually on Apple, not Android …’ but Apple iPads are more expensive than Android devices. AAC software has a limited number of South African voices. Thus, to differentiate the different speakers in the classroom, one needs to ‘modulate the frequency’ of the voices. Speech generation devices, such as Go-Talks by Attainment Company (2011), have been offered to some schools, but consensus was that SLTs did not like these devices. One SLT said: I can’t stand [Go-Talks]” while another SLT said, “I do have some kids that use Go-Talks. They're not my favourite … for some kids, [Go-Talks] are helpful, but really, it's just about, do the teachers implement it in the classroom? And the answer is largely no.
Education system
This theme considered the challenges that professionals regularly face, working with school-aged children who need AAC to communicate. Three subthemes were identified, including high staff turnover and burnout, therapist-teacher collaboration, and caseload.
According to the SLTs, ‘there's high staff turnover in schools, you're training all the time’. The AAC system that one SLT implements may not be the preference for the next SLT or welcomed by the next teacher. One SLT said, It's like pick your battles. The same as you're speaking about teachers coming in, therapists coming in, and the high turnover of staff … the ball almost stops rolling, rolls back a bit and then a new therapist spends two years just getting the ball to where you left it. And then she's probably burnt out and needs to take a break. I mean, that ball never makes momentum.
SLTs shared that AAC intervention may not be prioritised because SLTs may feel ‘uncomfortable with [AAC] systems … [SLTs] just don't know where to start’ and new therapists may focus on other areas of communication instead.
Therapist-teacher collaboration was another subtheme mentioned by the professionals. The most common way for therapists to see children during school time is to use the ‘pull-out’ method (children taken out of class for therapy). One SLT explored some of the disadvantages of this method, ‘the teacher doesn't get to see [AAC] working. The child doesn't get to see the teacher use it; the teacher doesn't see the therapist use it. The therapist doesn't see what goes on in the class …’
However, another SLT mentioned that sitting in the LSEN class is only possible if ‘there is space in the classroom’. Even so, participants made it clear that the collaboration between therapist and teacher is essential for a positive outcome for the child. Some teachers are accommodating and eager: ‘a lot of times we [teachers] observe the therapist in the class and then you see certain techniques, certain resources that they use … then you actually learn a lot of the things you can apply with other kids in the classroom’, while others stated ‘you're not sitting in my class, this is my time with my children’. Some teachers feel that SLTs make better progress when they see the children outside of the classroom: ‘[SLTs] … do some magic there [intervention in SLT room] and when they come back, I’m able to teach this child successfully and assess everything’. It was evident from the discussion that teachers had different preferences for levels of assistance in the classroom.
Large caseloads were acknowledged as a great challenge for SLTs in LSEN schools. One therapist spoke about her experience: We were two SLTs in a school of 200. I had a caseload of about 70, of which at least 10 were children who couldn't speak and needed AAC, but I didn't have enough time to implement systems with them, or train everybody.
SLTs reported that they do not have enough time to conduct intensive therapy with the children, ‘that means that for that whole week, my other 35 kids don't get seen’. SLTs also mentioned that aside from the large caseloads, all their extra time was filled with other school responsibilities, such as ‘break duty’, sport and ‘finance committee’ work, and they had little time to personalise AAC devices. Additionally, as staff numbers are limited at public schools, one SLT said, ‘the OTs also have 70–90 [children on their caseload], and there are also wheelchairs that are broken and there isn't someone to fix the wheelchairs. So, then the physios become the wheelchair repair people, or the teachers join’. It was acknowledged that assistants would be valuable for the entire multidisciplinary team, ‘so that you can take your expertise and maybe manage the 70 [cases] but have multiple assistants on the ground in the classroom’. However, school budget constraints meant that assistants are seldom hired.
Language and code-switching
This theme highlights the difficulties experienced by professionals who work with children using AAC in a multilingual country. It has three subthemes, including language, accents and code-switching.
SLTs shared the language challenges experienced, specifically that there are few synthetic voices in some of the South African languages. In addition, most of these AAC systems are text-to-speech systems, which illiterate children cannot access. One SLT stated, Over the years, we never really had a child successfully using a speech output device, largely because of language barriers and accents … They're all isiXhosa speaking children [in the school], and to create an entire vocabulary in a different language, when it's not available, would take years.
This highlights the challenges faced in multilingual contexts. If an AAC system is set up for English, it typically cannot be translated into an African language such as isiXhosa. For example, in isiXhosa, ‘you can’t use one word with a picture, because words aren’t words, they’re root words’. For example, ndiyam
The professionals noted that American, British and Australian English accents are generally used with speech-generating devices. An SLT noted how pronunciation was often problematic for users in South Africa whose English pronunciation of words was very different. Discussing a Zimbabwean child who used a speech generating device, SLTs said, He had this American computer voice … I was like, this is such a lovely story, but I cannot focus because it sounds ridiculous … an adult male American voice, but the child had a Zimbabwean name. So even his own [device] couldn't pronounce his own name.
On the other hand, another SLT mentioned: ‘I've had people who, when the kids speak with an American or … what is to be considered a “posh” accent, then people actually expect more of them.’ It seems that when a child uses a high-tech device, the accent of the synthetic speech plays a role in how the child is perceived by others.
Code switching is another aspect of growing up in a multilingual society. Participants believed that almost every family in South Africa alternates between two or more languages during conversation, even if the child has special needs. One SLT described the code-switching situation well by saying: I’m not aware of a high-tech device that does [code-switching] in a functional manner, anywhere in the world … most devices still require a significant shut down to get the second language. And so, you can’t code-switch, because you can either be in one language or the other … [South Africa's] got such a mix [of languages], that code-switching is a real challenge when it comes to AAC.
Benefits
This theme encompasses the benefits experienced by professionals who work with children that use AAC. It has two subthemes, including attitudes and expectations, and identity and personality. A teacher shared, I can see it assists with communication, social interaction and with learning. [Often] you sit in a classroom and a child wouldn’t have been able to tell you what they like, what they dislike, their emotions- and I can see the iPad even assists with speech now.
One of the teachers mentioned that having assistive devices for some of the children in their class would reduce the learners’ frustration. An SLT summed it up as follows, ‘in the core of all the … hecticness of trying to get a child to speak, we need to remember the value of that child speaking, of that little personality sharing with you’. According to the participants, AAC could change people's attitudes, expectations, and perceptions of children with CCN: ‘People expect so much less of [children who use AAC] and then you’re changing the perception of them, again’. Another SLT said: ‘Having a voice, especially in a classroom can be really great. Because kids who are hidden suddenly are not anymore’. Professionals agree that ‘getting [children with CCN] as independent and as excited as possible, will give hope to their parents, will give hope to the teacher, will give hope to the therapist to push a little bit harder’.
The professionals expressed how children can share more of their personality and identity when they are given a voice: If this voice does give them their identity, their excitement for sharing, for communicating, I mean, the world's their oyster. In comparison to this child that may be like- ‘what I have to say, doesn’t really matter, because what's going to come out? That's not me’.
As age plays a role in identity, SLTs shared that having a voice that ages with the child is an equally important identity component to consider but, ‘sometimes we neglect [aging the voice] for the … population’. Lastly, the professionals acknowledged that AAC has the potential to give children the ability to share their thoughts, helping them feel less isolated. One SLT shared, ‘the discussions I’ve had with young teens to adults, who have no speech and who have to use these voices has been very much that when they find their voice, it's like that moment of finding who they are’.
Discussion
Literature acknowledges that communication partners are crucial to the successful use and implementation of AAC systems (National Academies of Sciences, Engineering and Medicine, 2017; Kent-Walsh et al., 2015; Moorcroft et al., 2019b). However, published literature from AAC stakeholders is not representative of LMICs. For example, in Baxter et al.'s (2012) systematic review, stakeholders from 27 studies resided in high-income countries such as the UK, USA, Australia, Canada and Israel, but only one study included perspectives from a middle-income country, Egypt. Although Baxter et al.'s (2012) research was conducted over 10 years ago, recent literature focusing on LMICs is still less common than research from high-income countries, and often lacks input from multi-perspective stakeholders (Mukhopadhyay and Nwaogu, 2009; Tönsing and Dada, 2016; Tönsing et al., 2019; van Niekerk et al., 2019). This exploratory study presented perspectives from teachers, SLTs and caregivers in South Africa, an LMIC. This study was conducted to highlight additional issues for AAC implementation in this context as little information is available, but further work will be needed before generalisation can occur.
Findings indicate that reduced support and training is the most commonly experienced challenge that professionals face when implementing AAC. Although a lack of support and training is not unique to LMICs (Moorcroft et al., 2019a), when combined with limited personnel, training and resources (Pascoe and Norman, 2011), the problem is exacerbated. Our study highlights that without adequate support and training, AAC service delivery in LMICs may remain unsustainable. Other South African studies (Tönsing and Dada, 2016; Tönsing et al., 2019; van Niekerk et al., 2019) echo the need for training when introducing assistive products. Similarly, results from our caregiver focus group suggest that misunderstandings surrounding the purpose of AAC are experienced with caregivers, often brought about by a lack of AAC-related training and education, as supported by van Niekerk et al. (2019). Training caregivers from LMICs is challenging as they often cannot attend meetings due to a lack of transport and limited time off work. They may also have limited access to technology and/or basic resources. This was clear in our study and research from other developing countries, such as Kenya (Gona et al., 2014). Professionals highlighted the need for therapist and teacher empowerment to implement change, and support from the education system. Providing training and support to stakeholders so that they may be agents of change for AAC provision and intervention could pivot the burden of disease for children who need AAC, and their families.
Although South Africa has a progressive disability policy, the accessibility of assistive devices, particularly high-tech AAC devices, is limited (van Niekerk et al., 2019). When high-tech devices are available, our study shows that practitioners from LMICs need to consider the high risk of crime and the risk that using such an expensive device places on the child and their family. Communication difficulties, along with the attached stigma and cultural beliefs surrounding children with special needs in LMICs, may act as a catalyst for bullying and crime. These findings are supported by studies in other LMICs (Gona et al., 2014; Mukhopadhyay and Nwaogu, 2009). However, even if the family's safety is not at risk from having a high-tech device in the home, many families, even those in high-income countries, prefer that their children only use high-tech devices at school (Tegler et al., 2019). If the language used at school differs from the language used at home, high-tech devices become less useful (Tönsing et al., 2018). It is recommended that children receive a low-tech device that matches the layout of the high-tech device. This low-tech device could be used in situations where having a high-tech system puts the family at risk, as a back-up in case the high-tech system fails, or in circumstances where the high-tech system is impractical or unfeasible.
Additionally, our study highlights that practitioners need to consider high-tech AAC device affordability and device features. Although much of Africa's AAC development work has been conducted in South Africa (Gona et al., 2014), the country is limited by financial resource constraints (Tönsing and Dada, 2016; van Niekerk et al., 2019; Visagie et al., 2020). There is great variation in resourcing and the provision of assistive technology between the different provinces (regions), with more rural provinces often experiencing the greatest challenges (van Niekerk et al., 2019; Visagie et al., 2020). People who provide and use assistive technology in low-resourced contexts often support imported products over local ones (Visagie et al., 2020). Imported products are usually more expensive, and the design features may not be suited to the environmental, cultural and language needs of the country (Visagie et al., 2020). If local companies were incentivised with governmental tenders, production costs may decrease, and the availability of affordable local technology and culturally appropriate software would increase. It would be beneficial if collaborative and strategic partnerships and communication channels between the Departments of Health and Education, non-governmental organisations, disabled persons’ organisations, local manufacturers and donors, were created and formalised to ensure affordable and accessible AAC solutions.
Local research into culturally appropriate synthetic voices and other AAC systems should be ongoing, and current best practice should not simply rely on research from high-income countries. Our study showed that practitioners need to consider the range of languages and accents available when introducing AAC systems. Many LMICs are multilingual, and may lack access to minority languages on their AAC devices (Terblanche et al., 2022). Moreover, professionals are not always sufficiently competent in all the languages to meet the language demands of a multilingual society (Kathard et al., 2011). Despite ethical guidelines stating that individuals should not be denied intervention because of a language mismatch (Pascoe and Norman, 2011), our study shows that evidence-based core language AAC systems are not widely available for SLTs and teachers, especially when finances are limited. Simple translation of a graphic symbol-based system into two or more spoken languages is not appropriate because different languages require different representation methods (Tönsing et al., 2018). However, even if systems were developed, they would need to allow code-switching, and make use of culturally and linguistically appropriate AAC symbols, paired with the correct orthography (Tönsing et al., 2018). We need to advocate for government-supplied culturally appropriate core language AAC systems. In multilingual countries, the cross-cultural readability of graphic symbols, and the development of AAC systems in different African languages, would assist AAC users and those who support them.
The development of culturally appropriate core language AAC systems may ease the burden on professionals. Large caseloads, a lack of human resources and related support services in LMICs, mean that professionals in LSEN schools feel overworked, leading to periods of burnout. Similar experiences were shared by professionals in Botswana (Mukhopadhyay and Nwaogu, 2009) and Egypt (Wormnaes and Malek, 2004). As assistants are not always available in LMICs, SLTs report that classroom-based intervention for each child on their caseload is not necessarily practical. Our study highlights that if LSEN schools do not prioritise and advocate for AAC use, AAC development for children with CCN will remain limited.
Despite these challenges, there are numerous benefits to using AAC systems. AAC gives children with CCN a functional way to initiate and respond to conversation, which reduces social isolation and encourages active participation. Children with CCN have opportunities to showcase their personality, interests and ideas. When using a high-tech AAC device, having a synthetic voice that mirrors the language, gender, age and natural voice capabilities of a child with CCN, provides that child with an identity, and strengthens their communication partners’ expectations and perceptions of them.
Limitations and future directions
This is an exploratory study and therefore the small sample size and methodology selected means that the findings cannot be generalised to all AAC stakeholders in LMICs. The caregiver group was particularly limited. Although the focus groups were conducted after working hours and transport fees were covered by the study, the caregivers informed the research team that the loss of income, the transport cost which had to be paid upfront, and lack of childcare for the other children in the home, were all reasons that made participation difficult. These challenges indicate clearly why similar participants from low-income backgrounds often go underrepresented in research. Future research should consider gathering the views of stakeholders at other ecological levels and mapping the process of change through theory of change workshops. Users of AAC themselves should also be included as stakeholders in future projects. Researchers need to develop multilingual AAC systems and AAC intervention guides, along with appropriate synthetic child speech in under-resourced languages.
Conclusion
Communication partners are vital to the successful use and implementation of AAC systems. This study presented the perspectives of SLTs, teachers and caregivers of children using AAC in South Africa, highlighting practical issues professionals need to consider when implementing AAC in under-resourced contexts. The safety risk associated with using high-tech AAC devices, device affordability, device features, and the range of languages and accents available when introducing an AAC system are all aspects that are important to consider in this context. Strategies that may advance the implementation and use of AAC in South Africa, and other similar settings, include development of strategic partnerships between governmental and non-governmental groups, establishing appropriate communication, training, and support systems, and creating evidence-based core-language AAC systems.
Footnotes
Acknowledgements
The authors would like to thank the participants for their valuable contribution. The financial assistance of the National Research Foundation (NRF) of South Africa (DSINRF Reference Number: MND200619533947) is also gratefully acknowledged. However, the conclusions are the authors own and are not attributed to the NRF.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation (NRF) of South Africa (DSINRF Reference Number: MND200619533947).