
Abstract
Children with developmental language disorders (DLDs) may experience barriers to communicative participation. Communicative participation is defined as ‘participation in life situations in which knowledge, information, ideas or feelings are exchanged’. Barriers experienced in communicative participation cannot be explained by language competence alone and are thought to be influenced by contextual factors. A better understanding of these factors will contribute to tailored speech and language therapy services for children with DLD. We conducted a focus group study with 13 speech and language therapists’ (SLTs) to explore their perspectives on contextual (environmental and personal) factors in early childhood that are associated with communicative participation in children with DLD. The personal factor of child well-being, and the environmental factors of familial support and SLT service provision were developed through thematic analysis. The potential mediating role of these factors on communicative participation implies that it is important to address contextual barriers and facilitators in speech and language therapy services.
Keywords
Introduction
Children with developmental language disorder (DLD) have difficulties with understanding and using language. DLD is relatively common, affecting approximately 7.5% of children aged 4 to 5 years (Norbury et al., 2016). Children with DLD often experience severe restrictions in everyday communication (Bishop et al., 2017). Their participation restrictions may vary across contexts and cannot be attributed solely to differences in children's language skills (Dempsey and Skarakis-Doyle, 2010; Eadie et al., 2006).
The ability to engage in everyday communicative situations or communicative participation is an important skill for children with DLD (Jensen de López et al., 2021). Optimising communicative participation is considered as the ultimate goal of speech and language therapy for children with DLD (Hidecker, 2010; Lyford Jones, 2010; Prelock et al., 2008; Roulstone et al., 2012). Communicative participation is defined as ‘participation in life situations in which knowledge, information, ideas or feelings are exchanged’ (Eadie et al., 2006, p.309). This definition has been validated by parents of children with speech and language disorders and professionals, including teachers, speech and language therapists (SLTs) and psychologists, who agreed that communicative participation is ‘understanding and being understood in a social context by applying verbal and/or non-verbal communicative skills’ (Singer et al., 2020, p.9).
The World Health Organisation's (WHO) International Classification of Disability Functioning and Health – Children and Youth version (ICF-CY; WHO, 2007), conceptualises functioning and disability as a dynamic interaction between a person's body functions and structures, activities and participation, and their contextual factors (Figure 1). Contextual factors, that is, personal and environmental factors, influence children's communication in social contexts (Conti-Ramsden and Durkin, 2015; Cunningham et al., 2021; Gerber et al., 2011). Contextual factors may pose a risk or protect against communicative participation restrictions (WHO, 2007). Knowledge of risk factors, such as having low socio-cognitive skills, can help professionals identify children at risk and develop interventions that can remove or neutralise barriers present in their lives (Singer et al., 2022). In contrast, knowledge of protective factors, such as prosociality, can guide the development of interventions for children and young people with DLD that build resilience and facilitate communicative participation (Luthar and Cicchetti, 2000).
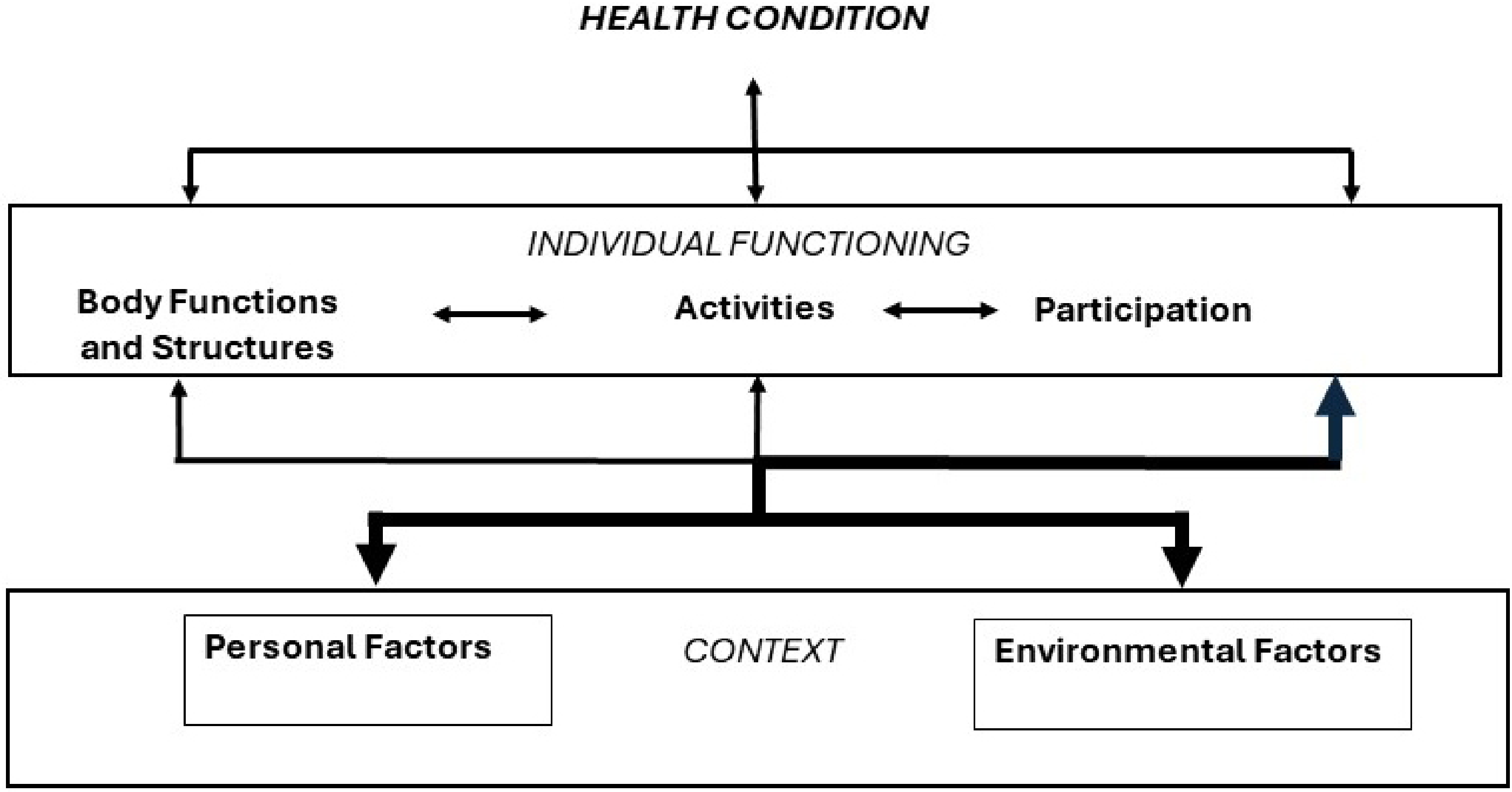
The International Classification of Functioning, Disability, and Health – Children and Youth version (ICF-CY) model of functioning and disability (WHO, 2007) visualises how individual functioning (‘body functions and structures’, ‘activities’ and ‘participation’) emerges from the interaction between the child health condition (‘disorder or disease’) and contextual factors (‘environmental factors’ and ‘personal factors’). The interactions between the components’ contextual factors and participation are highlighted using a thicker line, as they are the central focus of this study. Note. From ‘ICF Beginners Guide’ (WHO, 2002, p. 9), with permission of the World Health Organisation.
In a recent systematic scoping review (Singer et al., 2022), we identified several risk and protective factors for communicative participation in children with DLD. Only studies with a (quasi) experimental design and cohort studies were included. The review found that receiving therapy, a positive early language and communication environment at home, and a higher level of parental education level are protective environmental factors. No environmental risk factors are known. Personal protective factors include being a pre-school girl, reaching school age and being prosocial. Personal risk factors include being an adolescent, having low socio-cognitive skills, and having co-morbid mobility impairments or behavioural problems. However, significant gaps in knowledge were identified, such as the impact of life-satisfaction, motives or motivation, and emotional functioning, as well as the role of interpersonal relationships, and attitudes of other people in the child's environment (Singer et al., 2022).
In order to better understand the many factors and the interplay between them, qualitative research can provide the perspectives of children with language and communication disorders and their parents. Parents have been shown to consider their child's understanding of social situations as a relevant personal factor (Lloyd-Esenkaya et al., 2021; Myers et al., 2011). In addition, parents and children mention several other factors that were not yet identified in the scoping review. These include the child's confidence as a communicator (Markham et al., 2009), their understanding of and ability to regulate emotions (Lloyd-Esenkaya et al., 2021), the development of coping strategies (Lloyd-Esenkaya et al., 2021), practicing communication and putting in an effort (Merrick and Roulstone, 2011), feeling comfortable in the environment, having things in common with others, and feeling accepted by peers (Brinton et al., 2010; Lloyd-Esenkaya et al., 2021; Merrick and Roulstone, 2011; Myers et al., 2011). A protective environmental factor identified by parents, and also found in the scoping review, is the availability of support and therapy (McCormack et al., 2018). In addition, parents mention that informal support at home and in the community has a positive impact on communicative participation (Jensen de López et al., 2021; Markham et al., 2009; McCormack et al., 2018). Focus groups with children with communication difficulties show that a calm and quiet learning environment is helpful for their communicative participation in school (Markham et al., 2009). Finally, other people's attitudes towards the child and their communication problems can have an impact on a child's communicative participation, according to children and their parents (Jensen de López et al., 2021; Merrick and Roulstone, 2011). These insights into the perspectives of children with DLD and their parents highlight what is important to them. Addressing these needs in speech and language therapy is essential to providing family-centred care.
Even when the perspectives of children and parents are known, they may not coincide with those of SLTs. Potential discrepancies may have an impact on the therapeutic process (Marshall et al., 2007). The extent to which SLT perceptions of factors associated with communicative participation align with children's and parents’ perspectives and research evidence, is currently unknown. SLTs provide services to a diverse group of children and families. Exploring SLTs perceptions may broaden insight into contextual factors. Furthermore, their perceptions may be more applicable to practice than evidence from tightly controlled quantitative research studies (Lof, 2011). Therefore, the central research question of this study is, ‘What are SLTs’ perceptions of contextual factors associated with the communicative participation of children with DLD?’
We decided to conduct a focus group study, because focus groups provide opportunities for interaction between participants, which allows SLTs to reflect on each other's contributions from their own experience (Hennink et al., 2010). SLTs insights can complement the research literature and ensure that all relevant barriers and facilitators can be addressed. Ultimately, this may contribute to the optimal communicative participation of children with DLD.
Design
We conducted focus group discussions with SLTs to explore which contextual factors are associated with the communicative participation of individual children with DLD. We used the Hutter-Hennink qualitative research cycle approach (Hennink et al., 2010, p. 5). The cyclical research design is illustrated in Figure 2, and consists of the interrelated design, data collection and analytic cycles. In the design cycle, the ICF-CY was used as a conceptual framework for the development of the research question and the initial topic guide and prompts. In the data collection cycle, we first conducted two pilot focus group discussions to find out which topics were most relevant according to the SLTs and discover how SLTs talked about and reflected on factors that influence children's communicative participation. This cycle is illustrated by the dotted line in Figure 2. The cycle of data collection in the pilot focus groups (circle with the dotted line) is explained in Supplemental appendix A. Following the first pilot discussion, several changes were made to the list of topics and the procedure to improve the natural flow of the conversation. These changes included removing an introductory topic from the list and replacing prompts with more general ones such as ‘Can you tell me more?’ and ‘Can you give me an example?’. The moderator's introduction to the ICF-CY framework was shortened in the second pilot group, allowing for more time for discussion. Talking cards and brainstorming exercises were omitted due to time constraints. Instead, an observer recorded and clustered the factors on a whiteboard. After the second pilot focus group, the SLTs were asked to discuss real cases. These adaptations aimed to gather specific experiential knowledge from SLTs working with children with DLD and their families, as distinct from theoretical knowledge gained from training and literature. Next, we conducted two focus groups in which we specifically asked about SLTs actual experiences. The objective was to delve deeper into SLTs’ perceptions, generate richer data and identify relevant concepts. This cycle is illustrated by the dashed line in Figure 2. Finally, in the analytic cycle, the themes generated during inductive analysis of the focus group data were examined for interconnectedness, and a visual representation of the data was developed. Data analysis of the first and second focus groups resulted in code saturation, and therefore no new focus group discussions were initiated (Hennink et al., 2019). The data collection cycle of the focus groups (outer circle with the dashed line), as well as the analytic cycle will be further explained in the following section.
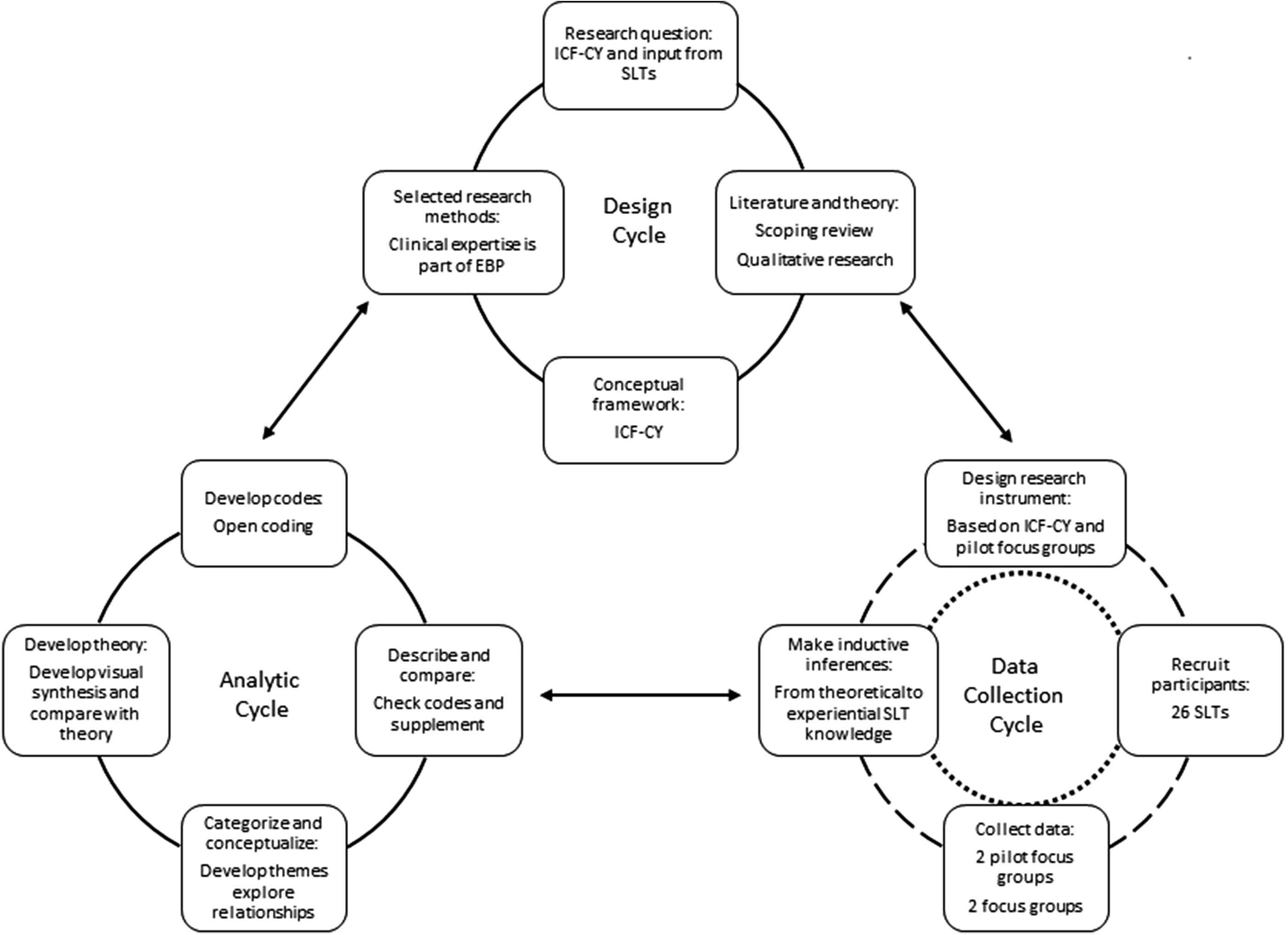
Current study design in the qualitative research cycle (adapted from Hutter-Hennink (2010), in Hennink et al. (2010)). The dotted inner circle in the data collection cycle represents the pilot focus groups, the dashed outer circle represents the focus group discussion for data collection.
The study was approved by the Ethical Review Board of HU University of Applied Science in Utrecht, the Netherlands (reference number 89_000_2019) and was conducted in accordance with the tenets of the Declaration of Helsinki (World Medical Association, 2013).
Research team and reflexivity
The first author, IS, is trained as a developmental psychologist and as an SLT. Her doctoral research is on developing knowledge and tools to support SLTs in shifting their focus from language skills alone to everyday communicative functioning in children with DLD. EG, is an SLT and a senior researcher specialised in research on communicative participation of people with language and communication difficulties. JWG has training in rehabilitation medicine and is a senior researcher on physical health, family empowerment, and cognition in children and youth with disabilities. ML is a senior researcher with expertise in pedagogy and neurolinguistics. She recommended the use of the Hutter-Hennink's qualitative research cycle approach in this study. Two SLTs assisted with data collection: IKW, with over 30 years of experience, and EDW, who has a PhD. in childhood language disorders. ADG assisted with data analysis. She is an experienced SLT with over 25 years of practice.
Data collection cycle main focus groups: Dashed circle
a Design research instrument
The list of topics prompts and materials that were used in the focus groups are shown in Table 1.
List of topics, prompts and materials used in two focus groups.
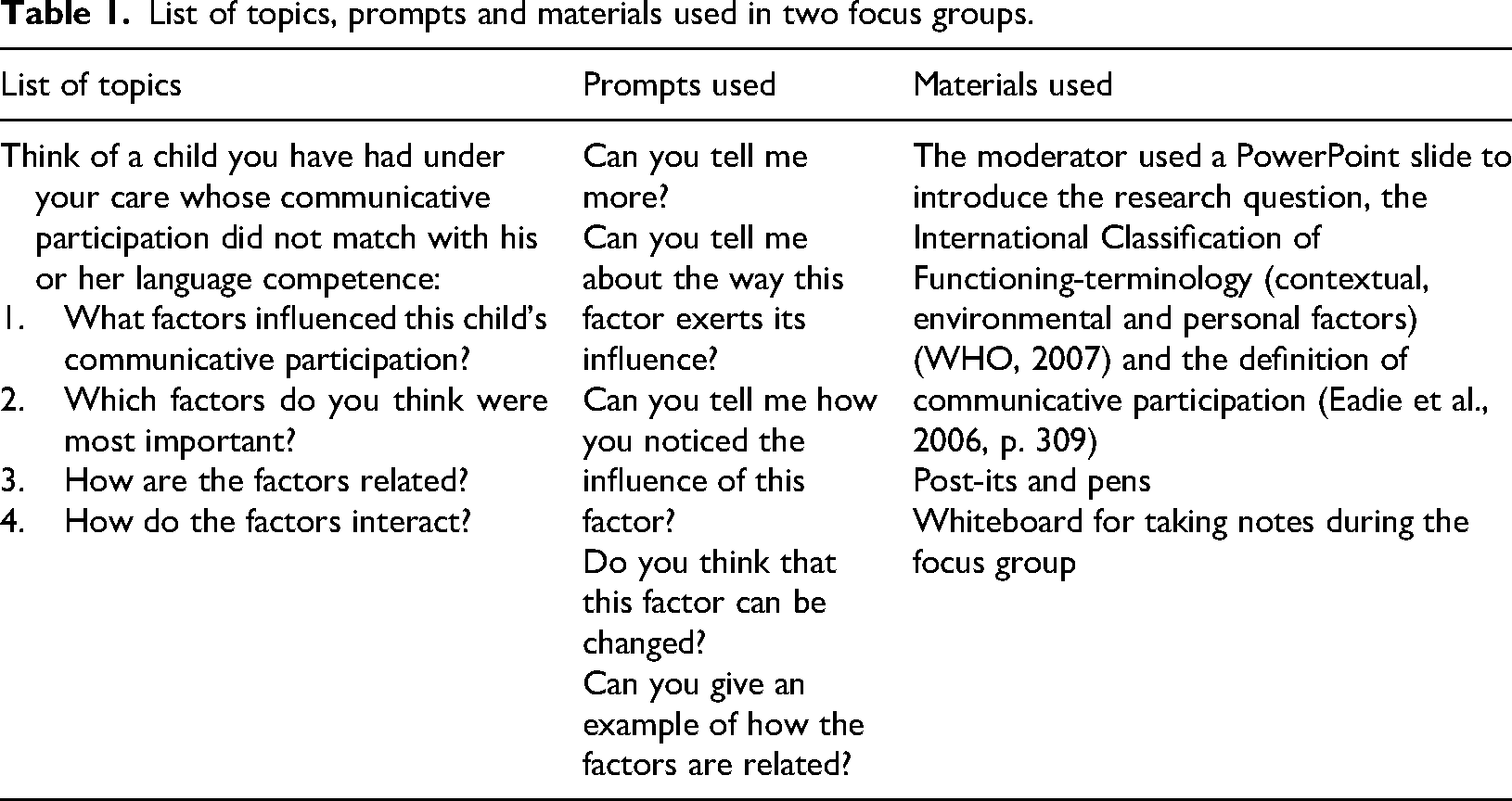
List of topics, prompts and materials used in two focus groups.
b Recruit participants
The focus group participants were SLTs recruited through convenience sampling via social media platforms. They were required to have at least 2 years’ experience of providing services to children aged 3 to 8 years with DLD. The characteristics of participants are shown in Table 2.
Focus group discussion participants.
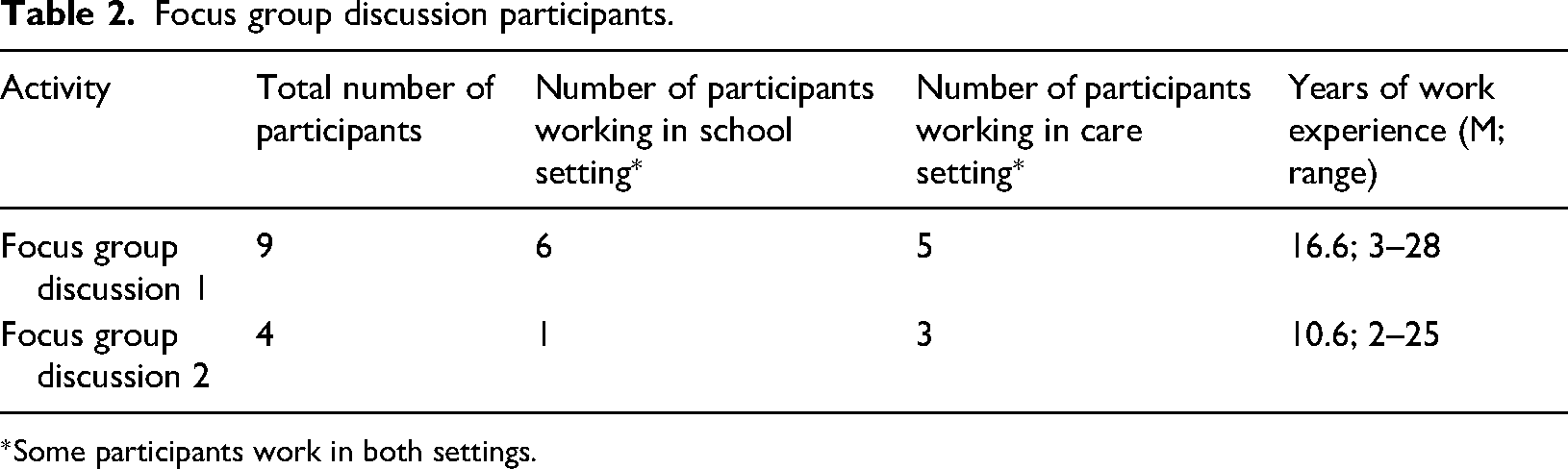
*Some participants work in both settings.
c Collect data
One focus group took place in a school meeting room, and the second focus group was conducted online due to the COVID-19 pandemic restrictions. Both focus groups lasted for 120 minutes. The discussions were video recorded.
a Describe and compare
Data from the focus group discussions were transcribed verbatim. The ICF-CY framework served as the primary lens through which we analysed our data, therefore we organised our data into personal and environmental factors using the ICF framework (deductive) (WHO, 2007). Next, reflexive thematic analysis was used to develop themes relating to communicative participation in children with DLD (inductive) (Braun and Clarke, 2021). The development of codes and themes was driven by the recognition that SLTs’ perceptions are social constructs, and that the way SLTs talk about factors associated with communicative participation is shaped and sustained by training, SLT practices and shared professional beliefs.
b Develop codes
The first author (IS) read the transcript of the focus groups and developed codes through open coding using Atlas.ti (version 22) (ATLAS.ti Scientific Software Development GmbH, 2022). The first deductive step in data analysis was to organise data into two subsets (personal and environmental), followed by an inductive reflective thematic analysis of the fragments falling within each subset. Apart from personal factors (P), environmental factors (E), the outcome of communicative participation (O) was marked in the dataset. Quotes were coded as belonging to personal factors if they described an aspect of the child as a unique individual, whereas quotes were coded as belonging to environmental factors if they described the physical, social and attitudinal environment in which the child lives. If a quote described a positive influence, it was coded with a plus (+) sign, and if it described a negative influence, it was coded with a minus (–) sign. ADG independently coded the transcripts using the same codes. Differences, and additional codes were then discussed and changes were made until consensus was reached.
c Categorise and conceptualise
IS and ADG grouped similar open codes together into second-order open codes in Atlas.ti for Windows version 22 (ATLAS.ti Scientific Software Development GmbH, 2022). This was done separately for open codes relating to personal factors and those relating to environmental factors. No further analysis was conducted on open codes relating to the outcome, as these specified aspects of communicative participation, rather than contextual factors. We used Excel version 2021 (Microsoft Corporation, 2021), to cluster second order open codes into subthemes, and to group subthemes into themes. The results were discussed with all authors until consensus was reached. The subthemes and themes were positioned within the ICF-CY framework. Next, the themes and subthemes were described as closely as possible to the participants’ words. Quotes were extracted from the data to illustrate each subtheme.
In order to explore how factors are related in SLT perception, we identified which open codes were mentioned together in the transcripts. We then aggregated the relationships between open codes at the subtheme level (Hennink et al., 2010, p. 250). Clusters of subthemes that were related in a similar pattern were then categorised into a theme. The last step in data analysis was a visual synthesis of the data, which illustrates how themes and subthemes are related.
Quality measures
In the design phase, we used the ICF-CY framework (WHO, 2007) and stakeholder consultation to inform the research question and the choice of research methods. In the data collection phase, we started with a deductive approach and used the experience of the pilot focus groups to make (inductive) inferences about the line of questioning that would yield the most informative data. Member checks were conducted by sending a summary of the discussion to the participants immediately after each focus group. The majority of the participants confirmed that the summary reflected the discussion well, while some highlighted the importance of particular issues (e.g. responsive caregivers) in their responses. The responses informed the naming of some (sub)themes. Data collection was conducted by two researchers (IS and IWK or EDW). Data analysis was conducted partly jointly and partly independently by two researchers (IS and ADG). The last author (ML) supervised the data analysis. In addition, sensitive issues raised in the focus groups were discussed in meetings with senior members of the research team. The Consolidated criteria for reporting qualitative research (COREQ) checklist (Tong et al., 2007) was used as a framework to ensure comprehensive and transparent reporting of the study design, data collection and analysis processes.
Results
Three themes and nine subthemes were developed. These themes and subthemes are illustrated with SLTs’ quotes. The study positions them in the ICF-CY framework, discusses relationships within and between themes, and provides a visual representation of how contextual factors impact communicative participation in young children with DLD, according to SLTs. All participant names mentioned in this section have been replaced with pseudonyms to protect their privacy and confidentiality.
Personal factor: Child well-being
Child well-being is a crucial theme for communicative participation, according to SLTs. This theme includes the subthemes of ‘mental and physical health’, ‘past experiences with communication’, ‘coping style’ and ‘self-image’. Child well-being is considered a personal factor within the ICF-CY (WHO, 2007), and is not necessarily tied to the child's language problems. The subthemes and their interconnectedness are explained below.
a Mental and physical health
Mental and physical health are both important aspects of overall well-being. Mental health encompasses emotional, psychological and cognitive well-being, while physical health pertains to the body's well-being, including factors such as nutrition, exercise, sleep and overall physical condition. According to SLTs, children's communicative participation can be negatively impacted by physical or mental health issues. When a child is tired, not in good health, or otherwise unwell, that will have an impact on their total functioning. And that includes communicative functioning …Obviously, there will be children with DLD and co-morbid neurobiological disorders, which may already make them less focused on communication. This is an additional barrier to their [gaining] communication skills. Focus group 2, Hannah
b Past experiences with communication
According to SLTs, a child's history of communication experiences significantly influences their interactions with others. Positive experiences can enhance communicative participation, while negative or limited experiences may lead to communication challenges, such as difficulty expressing oneself or understanding others. I also think that due to the DLD, a sort of vicious cycle is created… If you're very verbal and you constantly come up with all sorts of things, and have the ability to ask questions or to express things, and the other person responds to it … the communicative patterns develop very differently compared to those of children who don't know what to say or how to name things, they keep quiet, and then the other person doesn’t respond… Focus group 1, Ellen
c Coping style
Coping style refers to how individuals deal with stress, adversity and challenging communicative situations. Some children will use problem-solving strategies, while others may resort to avoidance or emotional coping. How does the child learn and how does the child cope when things don't go well? What kind of coping response do you get? Does the child get stressed? Will they try again? And what I see a lot with the young children I work with is that when things don't work out, they immediately go ‘boom’ into the red zone …How do you deal with it effectively when a child becomes very upset or very sad when something they're trying doesn't work out? I find that to be important. Focus group 2, Amber
d Self-Image
Self-image refers to an individual's perception of themselves. In the context of speech and language therapy, self-image relates to how a child evaluates their communication skills in relation to their environment. Negative self-perception in this area can have a significant impact on mental health, potentially leading to anxiety, depression or behavioural challenges. If they have a younger sibling who verbally outperforms them, this really has an impact. When they realize this, they might think, ‘Why can't I do that? Why is he or she better than me?’ Those kinds of thoughts could come into play. Of course, you can't look into their minds, but sometimes you can tell from the children's behaviour. This can cause conflicts at home or arguments. Yes, it can. Focus group 2, Julie
SLTs suggest that the subthemes are interconnected. For instance, children who have a negative self-image may experience challenges with their mental health and encounter difficulties in effective communication. Their coping mechanism may involve avoidance or negative behaviour, which can further impact their well-being. Conversely, children who have good mental and physical health may be better equipped to manage communication challenges and maintain a positive self-image. Additionally, positive prior experiences with communication may enhance children's coping abilities and self-image. Understanding these connections can be helpful in addressing communicative participation problems of children with DLD.
Environmental factor: Familial support
SLTs suggest that the communicative participation of children with DLD is significantly affected by the support they receive from their families. This support includes the physical, social and attitudinal environment in which children live and conduct their lives. Therefore, it can be classified as an environmental factor within the ICF-CY (WHO, 2007). The familial support theme can be divided into three subthemes: ‘stimulating and rich environment’, ‘knowledge and acceptance of DLD’ and ‘responsive caregivers’. These factors can either facilitate or hinder progress.
a Stimulating and rich environment
A stimulating and rich environment refers to the surroundings and experiences that provide many opportunities for communicative participation. According to SLTs, this includes access to age-appropriate books and regular dyadic reading sessions, engagement in social interactions and conversations both in one-on-one and in group settings, and participation in play, games and activities with others. SLTs believe that exposing children to a variety of sounds, sights and experiences can enhance their comprehension of the world and encourage communication. It does help if a child has wider experience. Children who do many things with their parents have a much broader world view. They can converse about many different things. Focus group 1, Sara
A stimulating and rich environment also encompasses the network of parents and the level of support they can provide for their child. Early intervention is important. When parents have a small network, children with communication problems may only be identified later on and …then it’s very difficult to do anything. Focus group 1, Petra
b Responsive caregivers
SLTs emphasise the importance of parents or caregivers providing a safe environment and responding positively to a child's attempts at communication. This involves being attuned to the child's needs, emotions and cues, even if the child's verbal communication is limited. SLTs believe that parents should create opportunities for their child to communicate by asking open-ended questions or offering choices. They should also provide positive feedback and reinforcement for the child's attempts to communicate. It is important to maintain an objective and balanced approach to encourage the child's communication development. SLTs acknowledge that progress in communication skills may be slow and requires consistent support from parents without undue pressure. I also know some mothers who are really on top of it. The more speech therapy the better. They are very enthusiastic, but also somewhat one-track. I mean, they are not so much interested in what the child has to say or in talking together, but rather they want them to study hard, do well [in school], learn vocabulary …That is what they consider to be of paramount importance… Focus group 1, Ellen Safety … These kids must feel safe first, otherwise nothing is possible. [Without that] you can't ask anything. Focus group 1, Martha
Stressors such as parental illness, poverty and strong sibling rivalry can adversely affect parental responsivity, especially when multiple problems exist. This can impact how the family relates and communicates. Families where several things are going on, poverty … or another sick sibling in the family… a whole lot of issues can pile up and the child is snowed under. Focus group 1, Jane
c Knowledge and acceptance of DLD
According to SLTs, it is essential for parents and caregivers to have knowledge of and accept DLD. This includes a clear understanding of DLD, including its causes, characteristics and potential impacts on a child's development, as well as accepting the child's diagnosis. SLTs emphasise that it is crucial for parents to understand that the child's language difficulties are real and not due to laziness or lack of effort. The knowledge about DLD that either the parents, teacher, or the entire environment has, plays a really significant role. It affects how the environment treats the child. Focus group 2, Julie
SLTs believe that a stimulating and rich environment for children with DLD involves providing opportunities for language exposure and practice. Informed and supportive caregiving requires knowledge and acceptance of DLD, while parental responsivity involves responding to the child's communication attempts with understanding, encouragement and patience. These aspects of familial support contribute to the child's communicative participation, according to SLTs.
Environmental factor: SLT service provision
SLTs emphasise the importance of timely engagement in therapy services for the development of communicative participation in children with DLD. Two key aspects of intervention in relation to children's communicative participation are highlighted by SLTs: preparation for real-life situations and a child-centred approach.
a Preparing for real-life situations
SLTs emphasise the significance of equipping children with the necessary skills to participate in real-life situations. To achieve this, they suggest integrating social skills training into speech therapy sessions and practising fundamental communication skills, such as asking questions and engaging in discussions. Debate is recognised as an effective method for teaching children how to navigate communication challenges, including enhancing the clarity of their thoughts and resolving misunderstandings. We practise in small groups when possible. For example: How can you ask each other questions? How can you discuss views on a topic? Yes, the really basic skills. Focus group 2, Julie Debating provides a very pleasant structure for children. I notice that children like this structure where one stands up while others sit down, and they have all the time and attention to express their opinion. Focus group 2, Jo
b Child-centred approach
SLTs emphasise the importance of placing the child at the forefront of the learning process. They suggest tailoring communication activities to the unique needs, interests, and developmental stage of each individual child to nurture their individuality and autonomy. I mean that you connect, that you talk to, not over, the child, that you give the child plenty of time and don't talk too fast, that you establish a connection with the child, so that what you say, do, explain, or read, registers with the child. Focus group 1, Ellen For him, it is particularly important that he can suggest a topic, something that he wants to talk about. That suddenly makes him more communicative. Focus group 2, Amber If you show a sincere interest, I think the child will also be able to talk about emotions. Focus group 1, Jo
SLTs believe that therapy should be tailored to the individual needs and interests of the child. This approach enables the child to practice communication skills in real-life situations, leading to meaningful progress in their ability to communicate and participate in everyday interactions.
Themes placed within the ICF-CY
Figure 3 presents an overview of the themes within the ICF-CY framework.
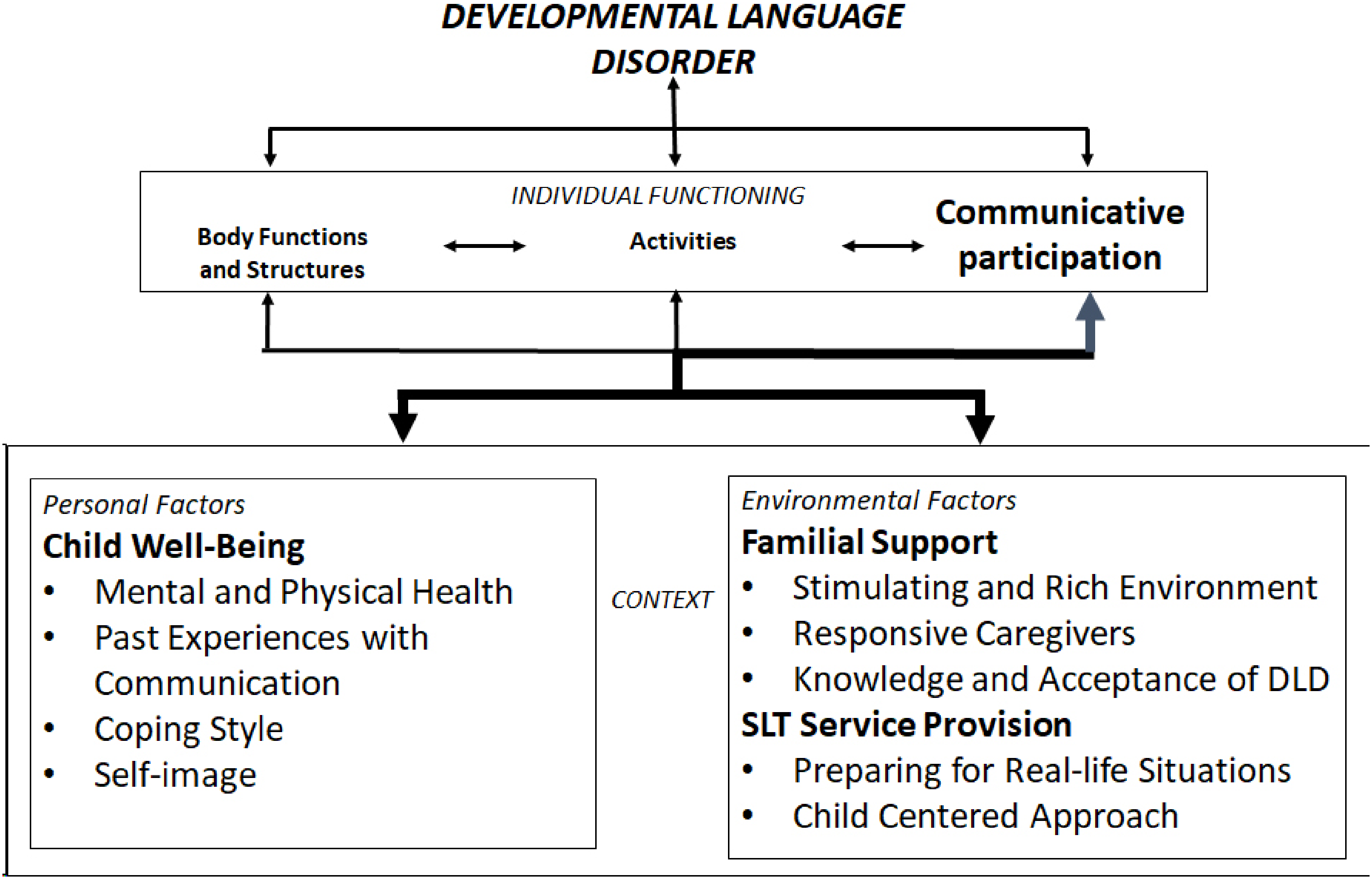
The themes and subthemes identified in this study are positioned within the environmental factors and personal factors components of the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) model (WHO, 2007). Note. From ‘ICF Beginners Guide’ (WHO, 2002, p. 9), with permission of the World Health Organisation.
a Interactions between themes
According to SLTs every theme was found to be related to at least one other theme through codes that were mentioned together. Some associations were described positively. For example, the association between the open code ‘opportunities to communicate’ (subtheme ‘child-centred approach’ and theme ‘SLT service provision’) and the open code ‘taking initiative’ (subtheme ‘coping style’ and theme ‘child well-being’) is framed positively in this fragment: He always brought something to therapy for me. We had to talk about that for about five minutes. It could be a hand puppet, a soccer ball, or a Pokémon. And then you would suddenly see that he could talk quite well about it, that he dared to. But it had to align with his interests. I found it very impressive that he took the initiative, connecting to his experience. And because he took the initiative himself, he gained more confidence to talk about it. Focus group 1, Amber
Other interactions are phrased negatively. For example, the open code ‘parents do not accept DLD’ (theme ‘knowledge and acceptance of DLD’) is negatively associated with the open code ‘child well-being’ (theme ‘self-image’) in the fragment: His parents denying his DLD turned out to be a huge obstacle for his ability to communicate. It gave unrelenting stress. Seeing this one-to-one link between the parents’ lack of acceptance of the problem and their level of stress when communicating with the child has really impressed me. It had a massive impact on how that boy felt about himself and on his communicative participation. Focus group 2, Hannah
The analysis of interactions between themes shows that some have a direct connection with communicative participation, while others are associated indirectly with the outcome, through other themes. In the example above, the theme ‘child well-being’ is directly associated with communicative participation, while the theme ‘familial support’ and ‘SLT service provision’ are associated indirectly with communicative participation through the theme ‘child well-being’. On the level of subthemes, a child's self-image and coping style are associated directly with the child's communicative participation, while an indirect influence was mentioned for mental and physical health and past experiences, as well as the subthemes within the environmental factors’ domain. Finally, SLT service provision is directly associated with the child's self-image and coping style, and indirectly though shaping the child's past experiences with communication, according to SLTs. The interaction between themes is visualised in Figure 4 and illustrated in the following quote: We suspected that it was due to really intense perfectionism, that he only wanted to talk if he was sure he was saying it right. That was a huge barrier for his communication at the time. Everything had to be non-verbal, and that didn’t always go well either. But the great thing was that, once he knew that he could do it, then he immediately talked in full, or almost full, sentences. He seemed to skip all the in-between steps, because he wanted to be able to perform well straightaway. So, perfectionism was important. But I also think that the environment played quite a role because, if you receive a negative response when you make a mistake, you will become more afraid of letting yourself be heard. So that's a trade-off. And once you dare to communicate, even if you make mistakes, and there is a positive response, then that gives positive reinforcement of course. So, I cannot see one separate from the other. Focus group 2, Julie
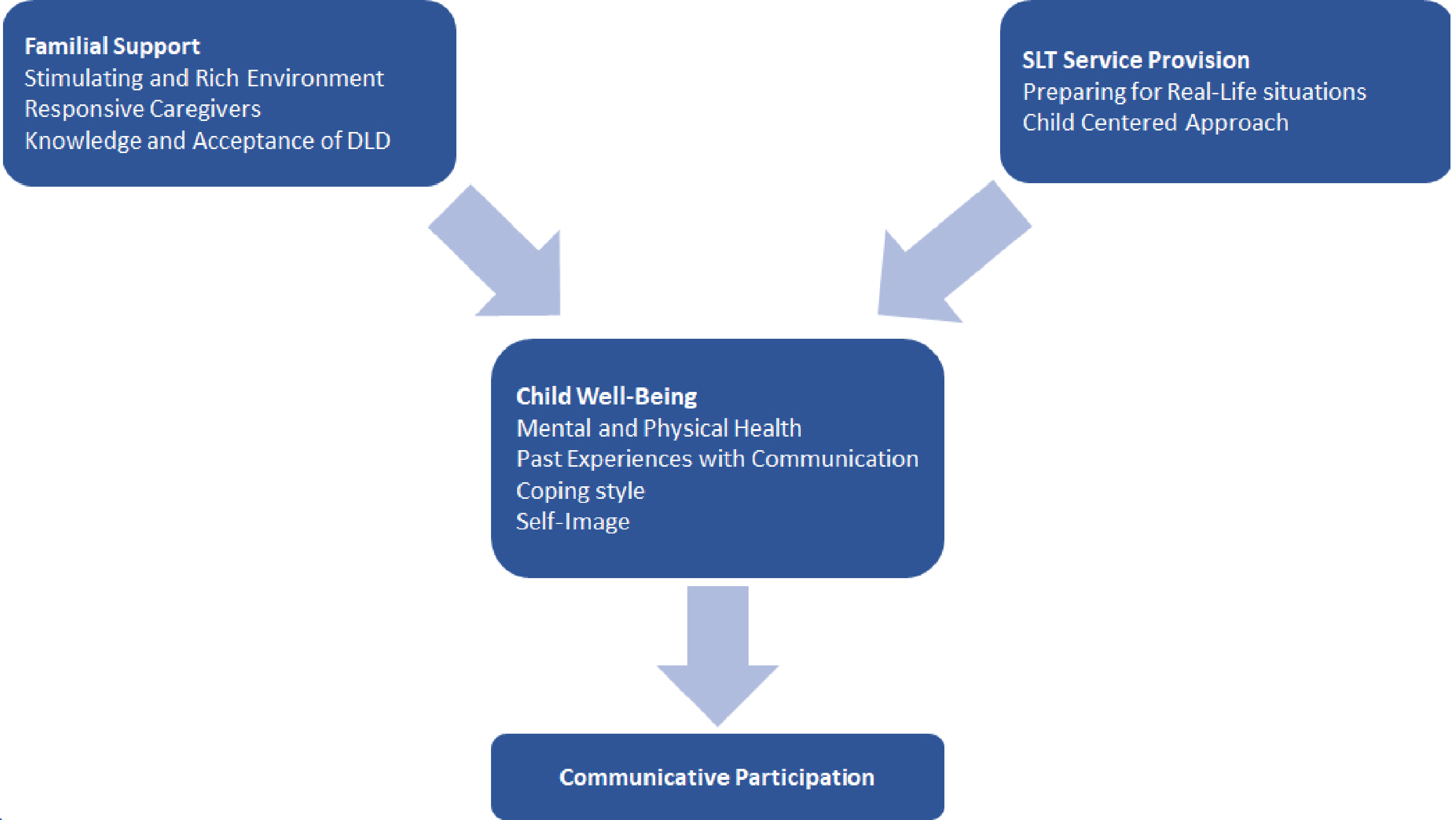
Interrelations between themes, and their relationships with communicative participation according to SLTs. Note. The direction of the arrows in the figure indicates the direction of the relationships between themes as perceived by speech and language therapists.
The study identified three themes and nine subthemes that illustrate personal and environmental factors associated with communicative participation in children with DLD. The analysis of interactions between themes suggests that communicative participation is directly associated with child well-being, which is, in turn, affected by familial support and SLT service provision.
Personal factors
There are many similarities between the theme child well-being identified in the present study with SLTs, and personal factors identified in qualitative studies on the perceptions and experiences of children and parents. These include the child's understanding of, and ability to regulate their emotions (Lloyd-Esenkaya et al., 2021), development of coping strategies (Lloyd-Esenkaya et al., 2021), confidence as a communicator (Markham et al., 2009) and practicing communication (Merrick and Roulstone, 2011). These factors align with the subthemes ‘coping style’, ‘self-image’ and ‘past experiences with communication’ in our study. It is important to note that there are differences in perceptions between SLTs and parents/children. Firstly, the subtheme ‘mental and physical health’ was identified in our study with SLTs but not in studies with parents or children. While parents are likely to be aware of any health problems their child experiences, they may not necessarily associate them with communicative participation. Secondly, parents and children mention that feeling at ease in the environment, having shared interests with others, and feeling accepted by peers (Brinton et al., 2010; Lloyd-Esenkaya et al., 2021; Merrick and Roulstone, 2011; Myers et al., 2011) have an impact on communicative participation. Parents and children consider a child's understanding of social situations as a relevant personal factor (Lloyd-Esenkaya et al., 2021; Myers et al., 2011), but this is not the case for SLTs. This difference may be due to the limited insight that SLTs have into the child's daily life, including their social relationships. This could be because the SLTs who participated in this study primarily work with children in individual sessions.
The subthemes ‘coping style’ and ‘self-image’ identified by SLTs in this study have not yet been linked with communicative participation in quantitative studies (longitudinal and RCT) (Singer et al., 2022). Limited evidence suggests an association between ‘mental and physical health’, and communicative participation, which is consistent with SLT perceptions. Research has established a co-occurrence of emotional difficulties and peer problems in children with DLD (Conti-Ramsden et al., 2019). Furthermore, Singer et al. (2022) found no available data on the influence of other aspects of child health on communicative participation. Lastly, the impact of ‘past experiences with communication’ has not yet been investigated in longitudinal quantitative research (Singer et al., 2022). However, research shows that a positive early language and communication environment at home as an environmental factor, is associated with better communicative participation in children with DLD (Toseeb and St Clair, 2020).
Environmental factors
The environmental factors that emerged from the current study with SLTs are consistent with those identified in previous quantitative and qualitative research with parents and children with DLD. Regarding the theme of ‘SLT service provision’ and the subtheme of ‘preparing for real-life situations’, numerous quantitative studies have shown that engaging in functional therapy has a positive impact on the communicative participation of children with DLD (Cunningham et al., 2018; Singer et al., 2022). The significance of receiving assistance and aid has also been recognised in a qualitative study that sought the opinions of children with communication disorders (McCormack et al., 2018). In contrast, the subtheme ‘child-centred approach’ discovered in this study has not been identified in quantitative studies as a factor that affects communicative participation (Singer et al., 2022), but rather as an approach to stimulate language development (e.g. Rinaldi et al., 2021). This difference may reflect SLTs specialised knowledge and skills in stimulating language and communication development. Furthermore, the theme of ‘familial support’ and its subthemes, including ‘stimulating and rich environment’, ‘knowledge and acceptance of DLD’ and ‘responsive caregivers’, may be linked to the results of a longitudinal study on children with DLD. The study found that a positive language and communication environment at home is crucial for promoting communicative participation (Toseeb and St Clair, 2020). Qualitative research has also mentioned themes related to the early language and learning environment, including children with DLD and their parents. Examples are a calm and quiet learning environment (Markham et al., 2009), other people's attitudes towards the child and their communication problems (Jensen de López et al., 2021; Merrick and Roulstone, 2011), and the positive effect of informal support at home and in the community (Jensen de López et al., 2021; Markham et al., 2009; McCormack et al., 2018). This study's findings suggest that ‘familial support’ and other factors may contribute to a positive early language and communication environment at home. Focusing on these aspects could be a valuable approach in indirect therapy.
Interactions between the child and their environment
Our study found that both familial support and SLT service provision have an impact on child well-being, which is in turn associated with communicative participation. These influences are unidirectional. However, the view of socialisation as a bidirectional process has gained wide acceptance. For instance, in the ICF-CY (WHO, 2007), interactions between personal and environmental factors, and the participation component of functioning are reciprocal. The visual synthesis of our findings does not represent the influence of ‘child well-being’ on ‘familial support’ and ‘SLT service provision’. Only one SLT mentioned that the child's response to communication problems (i.e. ‘coping style’) may influence how parents react (i.e. ‘responsive caregivers’). Furthermore, we did not find any mention of the influence of child or family factors on SLT service provision. Furthermore, the graphical representation of the data indicates a lack of consideration for the impact of SLT service provision on familial support. This may be due to the focus group questions being solely directed towards identifying factors that affect the communicative participation of children themselves. Alternatively, it could suggest that SLTs may not fully recognise the role of the family and community in intervention. To achieve optimal collaboration with parents in therapy, SLTs need to become more aware of parents’ perspectives. This will enable them to adopt a family-centred approach to therapy.
Limitations
Although research suggests that data saturation can be achieved in relatively few focus groups, a minimum of three groups has been suggested instead of the two that we conducted (Hennink et al., 2019). This small number of focus groups means that some themes may have been missed. However, the associations between subthemes within each theme indicate a satisfactory degree of data saturation. In addition, we conducted two pilot focus groups. The pilot focus group participants’ responses aided in the development of a topic list and approach that generated rich narratives on how personal and environmental factors influence communicative participation. These narratives provided valuable insight into the experiences of speech and language therapists.
One limitation of this study is that only four SLTs participated in the second focus group, while the intention was to include six to eight SLTs (Hennink et al., 2010). The COVID-19 pandemic led to the implementation of a lockdown, which resulted in the second focus group being conducted online instead of in person. Conducting a focus group online was a new experience for both the moderators and participants. Therefore, before commencing the focus group, we paid attention to the etiquette for online discussions. In hindsight, the smaller number of participants did not impede group discussion. It is noteworthy that the participants in this online focus group took longer speaking turns than the SLTs in the pilot focus and the first focus group. We now believe that conducting online focus groups with four to five participants may be an appropriate way to include a wider range of experiences and perspectives of professionals with busy schedules.
Clinical implications
To support communicative participation, it is crucial for SLTs working with children with DLD to comprehend that personal and environmental factors can facilitate or hinder communicative participation. Our study on SLTs identified several themes and subthemes that are also perceived as relevant by children with DLD and their parents in qualitative research. These themes and subthemes include: ‘child well-being’, ‘coping style’, ‘self-image’, ‘past experiences with communication’, ‘SLT service provision’, ‘preparing for real-life situations’ and ‘familial support’. The current SLT service delivery in the Netherlands focuses on individual children. The results from this study illustrate that SLTs need to embrace family-centred care and collaborate with both parents and children. Based on our study, we recommend a comprehensive approach to treating children with DLD. This approach should address all relevant contextual barriers and facilitators to achieve optimal communicative participation for children with DLD.
Supplemental Material
sj-docx-1-clt-10.1177_02656590241276693 - Supplemental material for Speech and language therapists’ perceptions of contextual factors associated with communicative participation in children with developmental language disorders
Supplemental material, sj-docx-1-clt-10.1177_02656590241276693 for Speech and language therapists’ perceptions of contextual factors associated with communicative participation in children with developmental language disorders by Ingrid Singer, Ellen Gerrits, Jan Willem Gorter and Margreet Luinge in Child Language Teaching and Therapy
Footnotes
Acknowledgements
We thank the SLTs who generously shared their insights by participating in this study. We also thank Ingrid Wissenburg-Koek MSc and Ellen de Wit PhD for their contributions in the data collection cycle, and Annemieke de Groot MSc for her contributions in the analytic cycle.
Data availability statement
Data available on request due to privacy/ethical restrictions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the HU University of Applied Sciences Utrecht.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.