
Abstract
Interventions designed to improve communication environments and the quality of adult–child interactions in early years (EY) settings are an important part of facilitating children’s communication skills both for children with identified Speech, Language and Communication Needs (SLCN) and children without SLCN. One such intervention devised and delivered by speech and language therapists (SLTs) in Nottinghamshire is the Language Lead Approach (LLA), where SLTs deliver a formalized but flexible package of support and training to EY practitioners who go on to become Language Leads (LLs) for their setting. Nine SLTs delivering the LLA were interviewed to explore their perspectives on the implementation and impacts of the LLA. Interviews were analysed thematically. Three key themes were identified, the first of which related to factors internal to the setting and included aspects relating to the nature of initial and sustained engagement with an LL and the setting manager, time pressures and the impact of different setting organizational cultures. The second theme which emerged related to the individual qualities and characteristics of the LL, as SLTs noted that the response of LLs to the role varied considerably and was influenced by their confidence, experience and leadership capacity, as well as the degree of autonomy in the role. The final theme, external influences on implementation, reflected the SLTs own working practices and workload. Overall, SLTs felt the LLA was effective and could be implemented alongside their daily workload. SLTs reflected on their lack of training to implement such interventions, the challenges to sustaining the LLA at the setting and County level, and the challenges of evidencing effectiveness. This research has implications for those designing and evaluating training and mentoring approaches as well as for those SLTs who are seeking to develop the effectiveness of their consultative working with Early Years Educators (EYEs).
I Introduction
Children’s Speech, Language and Communication (SLC) is a public health concern (Public Health England, 2016), and with high proportions of children in England starting school with SLC below expected levels (Law et al., 2017), training for early years (EY) staff around Speech, Language and Communication Needs (SLCN) is crucial (McLeod, 2011). There have been many early years programmes implemented at local and national levels aimed at supporting the SLCN of children through developing the knowledge and skills of staff in the sector. In response to the Bercow Review (2008) of SLT services which highlighted the need for skills development in the area of SLC for the whole EY workforce, Every Child A Talker (ECAT) was launched in the UK to attempt to address this training deficit. This was closely followed by the Early Language Development Programme (ELDP) from 2011 to 2015. In her evaluation of the ECAT programme, McLeod (2011) suggests that this cascade model of training did not necessarily support EYEs to progress from the initial training and that the quality of the training itself was diluted by the cascade model.
Research continues to suggest that language promoting strategies may not be well understood by EYEs (Gooch and Powell, 2013) and that, within EY settings, the communication environment may continue to constrain children’s optimal SLC development (Degotardi and Gill, 2017). Bercow’s 10-year review stresses that ‘understanding of speech, language and communication should be embedded in initial qualifications and continuing professional development for all relevant practitioners’ (ICAN, 2018: 3). Furthermore, greater effort needs to be made in identifying and supporting SLCN at the earliest opportunity, hence there is an imperative for EYEs to develop their knowledge and skills in this area (Lee and Pring, 2016).
In the study of early language interventions, there has been little research into implementation processes, with the focus tending to be on efficacy of the intervention, often in controlled studies (Law et al., 2017). Exploring the relationships between practitioners and examining the skills required for collaborative working helps to identify key factors in implementing and sustaining an intervention (Nilsen, 2015). An implementation science approach, examining how intervention programmes are executed, can support the investment in the ongoing development and value of these interventions and enhance the evidence-base for their effectiveness.
Moir et al. (2018) suggest that the field of implementation science can support the success and sustainability of interventions in their examination of the way the systems involved in cross-service interventions impact on early years interventions in settings. Evidence suggests that the training and development in a setting of an individual language ‘champion’ to develop the work around SLC can be part of an effective intervention (Law and Pagnamenta, 2017).
1 The context
Since October 2015, the responsibility for community SLT services has been held by Local Authorities (LAs) within their public health remit. LA commissioners must liaise with SLT services and meet population needs effectively. In Nottinghamshire in 2008, the Nottinghamshire Child and Families Partnership Speech and Language Therapy (NCFP SLT) service developed a structured response to local needs and demands called the Language Lead Approach (LLA) as a delivery model for community SLT provision across the county. The package was intended to suit each context, based on the combined knowledge of SLTs, EY settings and commissioners, which, using additional evidence from research findings (McDonald et al., 2015). The content and framework of the LLA was designed by the NCFP SLT service, but the implementation in each setting is a collaborative effort between SLTs and the EY setting staff.
In the LLA, a practitioner in an EY setting volunteers or is selected to be the Language Lead (LL) for the setting. An SLT meets with the LL to present the framework and both parties discuss ideas for improving communication environments and skills in the setting. Training courses are provided by the SLT but the rest of the plan is delivered by the LL. The role is not formally recognized or remunerated; different settings will provide more or less time and resources for the LL. For a detailed description of the LLA, resources for practitioners and training packages, please see: https://www.nottinghamshirehealthcare.nhs.uk/language-lead-role?smbfolder=603 (accessed November 2020).
This way of working, with the LLA as the interface between health and education, is locally viewed as highly beneficial in managing children’s SLCN. The overall philosophy behind the LLA is that of a key practitioner with a passion for communication and language being supported and empowered to develop a language-rich and nurturing environment in their settings. With training and mentoring from a named SLT, the LL will also act as a source of information and guidance for parents and colleagues as a result of their enhanced skills and knowledge in this area.
There has been a gradual roll out of the LLA and there are now more than 150 LLs in early years settings across Nottinghamshire, supported by a named SLT. The key concept of a language ‘champion’ was a central theme in the development, promotion and application of the LLA (Law and Pagnamenta, 2017). There is evidence which suggests that SLTs place high value on collaborative working (Jago and Radford, 2017), although some research suggests that interprofessional working is not always easy to negotiate and there may be structural and relational difficulties in cross-boundary working (Payler and Georgeson, 2013), including staff feeling under-supported (Baxter et al., 2009). Understanding contextual issues is likely to be crucial for successful collaboration.
Gorozidis and Papaioannou (2014) discuss the relevance of the motivation and learning dispositions of staff on the receiving end of this type of training and development package where rewards are generally intrinsic and not related remuneration or progression. This is echoed by Miech et al.’s 2018 research into the ‘champion’ role. There are implications for the SLTs involved in the implementation of the LLA as they are continually tasked with fostering enthusiasm and maintaining practitioner engagement with the Approach within the constraints of their relationship with the LLs which is not that of a line manager or appraiser/supervisor.
The LLA has been successfully developed and maintained for over a decade. The NHCT SLT service has continued to review and develop the Approach in a number of ways in response to the regular cycle of feedback received from the LLs (McDonald et al., 2015). They have recently undertaken their own assessment of the effectiveness of the LLA (Dillon and Marr, 2019). Feuerstein et al. (2018) present a robust case for the involvement of practitioners in the design, development as well as the delivery of collaborative approaches for successful implementation. As researchers we were interested specifically in the SLT perspective on how the Approach is implemented to help inform other SLT service providers and commissioners of these services.
2 Aims
The aims of this research were to consider what SLTs believe helps the implementation of the LLA and what barriers exist to effective implementation. Through the perceptions of the SLTs involved in working with this model of service delivery, the research aimed to identify the factors which SLTs perceived as having an impact on the successful implementation of this training and mentoring model of practitioner development. Two aspects of implementation were of interest: the way that the training approach was implemented and what affected this, and the way that the LLA itself was then implemented by practitioners to support SLT delivery and improve outcomes for children in EY settings in Nottinghamshire.
3 Methodology
This qualitative research was founded on an interpretivist stance assuming that there are individual interpretations of similar experiences (Darlaston-Jones, 2007). Preservation of the subjective point of view was key as we sought to understand SLTs’ social realities, discovered through an interpretivist lens (Fereday and Muir-Cochrane, 2006).
The primary researcher had a previous professional background in SLT practice. Her practitioner background might have influenced her perception of public health interventions in SLCN. The second researcher was aware of the LLA as she was related to a piloting participating SLT in the service. However, we had no bias towards a positive outcome for the LLA.
II Method
1 Research design
Semi-structured interviews were considered to be an effective method of collecting data, giving each individual the opportunity to respond freely to open questions about their own experience of the implementation of the LLA. Interview questions were designed around the Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2009). The CFIR is a cross-disciplinary implementation assessment framework designed to allow researchers to investigate and evaluate the implementation of services, strategies or interventions in a variety of settings and from a variety of viewpoints. The CFIR consists of five main categories: the outer setting or wider context of the intervention, the inner setting or organization and local context in which the intervention is being implemented, the intervention itself, the characteristics of the individual being interviewed and their reciprocal relationship with the intervention, and a reflection on the implementation process.
2 Sample
Participants were recruited purposively via an invitation email to all twelve SLTs currently working to support LLs in settings across the County. Ten SLTs responded to the email and gave their consent to participate; two did not respond to the email invitation, which could have been for a number of reasons, including workload. Of those who responded, interviews were successfully arranged with nine of them between April–June 2017. The level of post-qualification experience of the SLTs was varied, as were their ages and their experience of working using the LLA, thus providing a range of professional insights into the LLA.
Seven interviews were conducted in the SLT’s workplace; one interview was conducted in the researcher’s workplace and another in the participant’s home. Interviews were audio-recorded and transcribed verbatim; each interview lasted for an average of forty minutes (for interview questions, see Appendix 1).
3 Piloting
Pilot interviews were conducted with 2 SLTs involved in the original design and roll-out of the LLA. The pilot participants endorsed the questions and interview process and questions were revised, to address areas of duplication, misinterpretation or lack of clarity. Following the pilot, small changes were made to the wording of the questions in relation to the way the LLA approach fitted with other aspects of the SLT caseload.
4 Ethics
This evaluation was granted ethical approval from Nottingham Trent University and Nottinghamshire NHS Trust. An ethical approach to data collection and storage was maintained at all times following the BERA ethical guidelines (BERA, 2018). Participants completed a signed consent form and were given full details about their right to withdraw from the study. Issues of anonymity and confidentiality were addressed through recordings and anonymized transcriptions being saved and password protected, and references to specific named individuals being removed from the transcripts.
III Analysis
The interviews were analysed using thematic analysis (Braun and Clarke, 2006), a method for analysing interview data from a variety of epistemological and ontological stances. As a researcher with clinical experience who holds views on both implementation approaches and childhood language development, the stance within the analysis was characterized by an interpretivist approach to the data. This method of analysis also enabled the researcher to handle the large amount of data gathered in the study.
Familiarity with the data was essential (Fereday and Muir-Cochrane, 2006) therefore multiple stages of reading and coding of the transcripts were employed. JK, who had conducted and recorded all the interviews, was the main analyst. SM familiarized herself with the full data set and contributed to discussions and decisions around coding throughout the coding process. The research approach to analysis was mainly inductive, aiming to elucidate the core elements of the intervention by capturing statements which linked to the themes from the CFIR but also other related or novel themes. Each transcript was read through initially with pertinent points and quotations highlighted. Then the first transcript was read again with additional notes being made alongside the text, noting elements related to themes as they developed. A second reading of the transcript enabled coding by theme and a thematic template to be developed in discussion with the second researcher. Emergent themes tended to be linked to original question themes generated from the CFIR categories, allowing the thematic framework to be developed with themes aligned to elements from the CFIR as well as to the additional or novel codes. Specific participant responses within these themes were then examined by the main researcher to appraise the goodness-of fit of the overall theme. Each subsequent transcript was read and re-read in the same way and additional themes were added as a result of extensive discussion to support coding of data and to construct a thematic template (below). Hence, there was an iterative approach to coding, revisiting and recoding data in the light of shared researcher discussion and reflection on codes, supporting the joint development and final identification of themes and sub-themes.
1 Findings and analysis
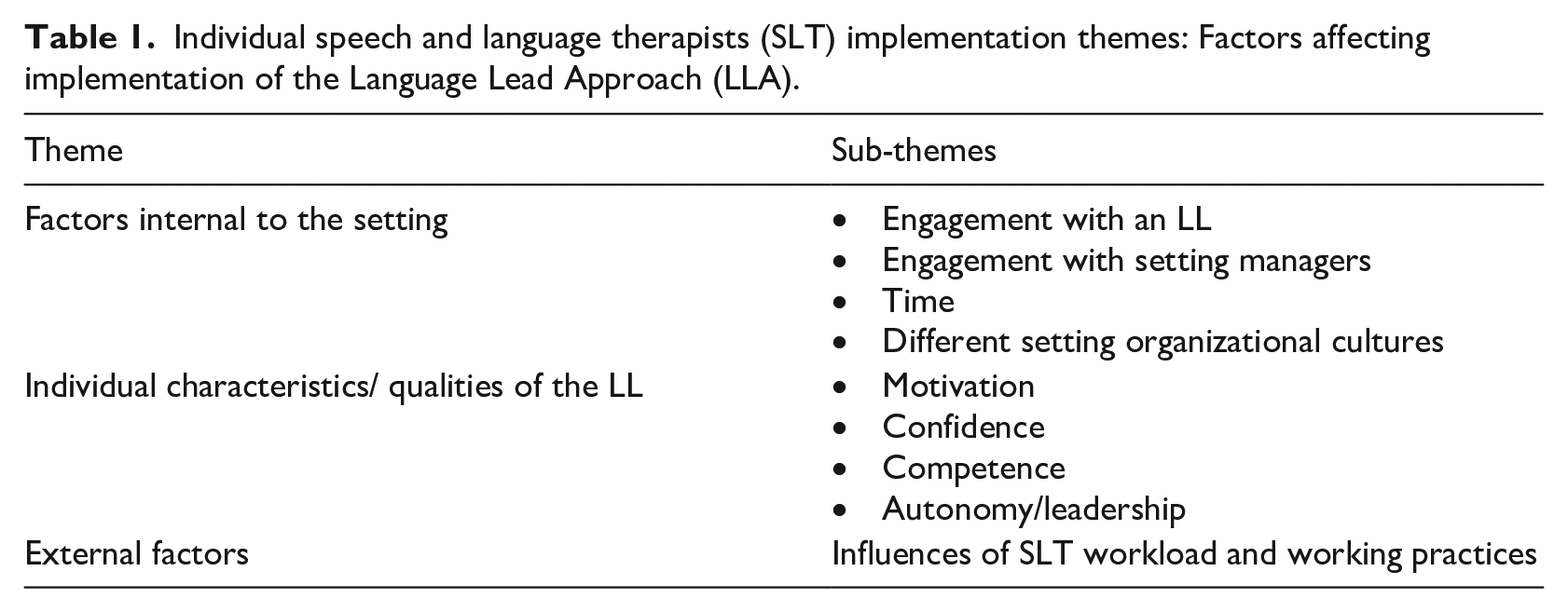
As described above, our analysis concerned coding into all five categories of the CFIR. However, issues around the wider context and the intervention itself are not discussed in further detail here due to the constraints of space and our decision to focus more specifically on aspects of setting practice, inter-professional working and practitioner characteristics. These three categories are more likely to be of use to practitioners designing or offering a similar intervention and are more amenable to action than outer context factors which are largely locality-specific. Table 1 shows the relevant themes which emerged from our thematic analysis and these are then discussed in detail, theme by theme, supported by excerpts of the participants’ voice.
Individual speech and language therapists (SLT) implementation themes: Factors affecting implementation of the Language Lead Approach (LLA).
2 Factors internal to the setting
a Engagement with an LL
The SLTs we spoke with believed that a key part of their role with the LLA was linked to getting the LL on board, and it was apparent from the responses that this took up varying amounts of time depending on how receptive the setting was. Dedicated time and effort at the start of implementation was acknowledged to generally result in an effective process from the SLT perspective, with several participants noting the relational aspect of the LLA. Nearly every SLT spoke of the value they placed on personal passion, engagement and on working over a period of time to build confidence in the identified LL practitioner.
b Engagement with setting managers
All the SLTs interviewed identified the role of the setting manager as being highly influential to the successful implementation of the LLA. Managers were characterized by SLTs as gatekeepers and the degree to which the manager enabled the SLT to work with the setting was felt by SLTs to influence the implementation, along with how much the manager prioritized the approach. SLT01 sums this up:
It comes down to managers and how much they value it. . . if the manager’s really on board with it and they’ve got time, often that’s better but if it’s not highly valued and they’re trying to do it around everything else they’ve got to do sometimes. . . you’re working on the same action plan for 6 months.
This quotation reflects the perceived extent of a manager’s influence on the LLA and highlights how the SLT felt that a setting manager could prevent the Approach from moving forward. A number of managers had designated either themselves or the school Special Educational needs Co-ordinator (SENCo) to the role of LL. Whilst this indicated prioritization and commitment to the LLA, SLTs felt these individuals were often busy or not best placed to implement the LLA.
c Time
Many SLTs suggested that the time which the LL was allocated to implement the LLA within the setting was significant in effective implementation. SLTs recognized that, for LLs, the LL role was an additional, often unrecognized, time pressure alongside their work duties. SLT03’s comments, like those of several others, were sympathetic:
The main thing I keep coming across is that they don’t feel like they’ve got time to do it. . . so some are a little bit nervous about it or a bit sort of stressed and thinking I don’t know if I’ve got time to do this on top of everything else I’ve got to do. . . we discuss that time is in the agreement and things but a couple of people have said ‘it’s been thrown upon me.’ (SLT03)
In parallel, SLTs seemed to experience a degree of stress in giving implementation of the LLA enough of their own time. Several SLTs noted that they would like to have more time allocated to spend in supporting each LL and SLTs were clearly heavily invested in the relational approach which the LLA involves. However, maintenance of this collaborative model, despite being introduced in part to relieve demands on the service, created its own new set of demands on the SLT as coach, mentor and co-worker, causing some stress and frustration for a number of SLTs.
d Different setting organizational cultures
A suggestion widely made was that it was the ‘culture’ of the organization and how well it was managed rather than the type of organization that had the most impact on effective implementation. One of the first places cultural influences were noticed was in the selection process for the LL, with SLTs suggesting that the process was not consistent across settings, depending heavily on the pool of staff available as well as the manager’s oversight in identifying a relevant practitioner for the role.
Further links were made between the organizational context and effectiveness of implementation, with different types of settings being identified as being more or less consistent in their implementation of the LLA and how this worked in practice. Schools were often identified as having a more consistent staff team, with nurseries and Children’s Centres in some areas being noted as having a higher staff turnover and a smaller staff pool.
SLTs also noted difficulties that private or voluntary (PVI) nursery settings might have in consistent implementation of the LLA due to the wide age range of children in the setting and the lower levels of staff qualifications. They made comparisons with the more developed support structures and organized hierarchy within the Foundation Unit of a school setting with a greater maturity, authority and experience of teaching staff.
Several SLTs noted that their own level of involvement in the selection of the LL had evolved over time and was dependent on the nature of the relationship with the setting, their own level of confidence as well as their knowledge of setting staff. Along with the selection element was the concept of empowerment and whether the LL was given the authority to implement and develop the role. This had implications about who is in charge of the LLA and who the SLTs feel holds the ultimate power in its implementation:
It depends on the relationship with. . . the setting. If I feel confident enough to say ‘so and so would be really good’ especially in a PVI setting. In a school we would say either the F1 or F2 teacher because they have the power to change things. . . . It’s often the teacher who’s had a bit more experience and they’ve got a degree. . . who is maybe a Foundation Stage co-ordinator who’s got a leadership and management role within the school. (SLT09)
Whilst getting services engaged is crucial to the LLA, further comments about the motivation and culture in a setting indicate that the SLTs were aware of indirect factors influencing implementation, also suggesting a level of strategic engagement as setting priorities fluctuated. It was clear that SLTs felt some settings valued the LLA whereas for others it was a ‘tick box exercise’ or it was being used as a response to a challenge from Ofsted around communication and language.
However, most SLTs felt that the effectiveness of the LLA and its implementation in the setting depended less on the type of setting and more on the qualities of the individual LL coupled with the authority that they were given by the manager of the setting.
IV Individual characteristics/qualities of the LL
SLTs reported wide disparities in the LL’s levels of competence and confidence in leading on SLC within their settings. Whilst there was no one ideal set of LL characteristics described by the SLTs, they did endorse several key characteristics of more successful LLs which supported their ability to lead on language including (1) motivation, (2) confidence, (3) leadership and (4) learning capacity.
Motivation and enthusiasm were seen as valuable attributes for new and experienced LLs; passion was named as both an internal motivator to meet the demands of the role but also as a quality that could motivate and inspire other staff in the setting around communication and language.
It was clear that the level of confidence of the LL varied from person to person and that this affected the way the SLTs role as mentor operated. SLTs described how confidence in being the LL was particularly linked age and experience:
When they’re told you’re the Language Lead they kind of go, whoa, that sounds like a lot of pressure and sometimes. it’s the younger girls that get given it and they’re kind of panicking a little bit. (SLT04)
Confidence was also linked to whether the practitioner had a clear understanding of the LLA with some SLTs suggesting that some LLs were overconfident or had an unrealistic view of what the LL role entailed which made the mentoring relationship more difficult and highlights the importance of providing clarity about the role and the expectations at the start of the process. However, motivation and confidence alone were not considered enough for someone to become a successful LL. They needed to have the abilities to develop their skills and to lead on the implementation.
The effect of different LL competency levels was clearly noted to have an impact on the implementation of training and mentoring. Low levels of competence were seen as limiting the effectiveness of the LLA, as were levels of personal responsibility to maintain knowledge and capacity to follow through. On the other hand, there was a consensus that a competent LL made implementation, and the SLT role within it, a good deal easier and more rewarding.
The fact that the role is as a lead for language was noted to be a relevant point by a majority of the SLTs who expressed how they perceived the success of the LLA to be contingent on the LL’s assertiveness and ability to lead on and promote the LL agenda. The leadership qualities of the LL were identified as being essential to the successful embedding of the LLA in a setting, such that SLTs actively promoted the ideas of becoming a language ‘champion’:
I think that a lot of times it depends on the individual staff, how keen they are, how assertive they are within their team to promote the LL role and the LL strategies. (SLT06)
V External factors
It was noted by a number of the SLTs that this way of working was a contrast to, and had to be balanced with, their usual clinical practice. Some suggested that they kept their clinical roles separate from their LL mentoring role and needed to prioritize their caseload children, whereas others suggested there were good connections between their clinical work and the LLA.
Other SLTs noted that if a child from their caseload was attending a setting with a good LL it would make their clinical job easier. Linked to this, caseload children were also noted to be a way into settings who were reluctant to engage with the LLA.
Several participants, including more recently qualified SLTs, noted that SLT training did not prepare them for this model or focus of service delivery. This was surprising considering that the consultative model of working has been common practice for a number of decades. The expectations on their mentoring skills within the LL model was daunting for some newer SLTs and this was reflected in how SLTs commented on their own knowledge and skills in the implementation of the LL approach and their confidence in holding LLs accountable for agreed tasks. Several suggested that the traditional model of clinical delivery was more within their ‘comfort zone’:
I don’t think we learn that when we train, that kind of advisory capacity that we’re all being encouraged to go into. (SLT07)
1 Discussion
In this study we interviewed nine SLTs from a department of twelve about their experience of the implementation of a specific SLC mentoring and support approach to staff development and universal SLT service delivery in order to understand the factors which affected effective implementation from an individual perspective. The aims of this study were to consider what SLTs believe helps the implementation of the LLA and what barriers exist to effective implementation. Consequently, the research had a very specific focus on what is required to ‘make things work’ in relation to the LLA and the interaction between the professionals involved. Two aspects of implementation were of interest; the way that the training and mentoring approach was implemented by SLTs and what affected this and, the way that the LLA itself was subsequently implemented by practitioners.
Three key themes emerged identifying factors related to the success or otherwise of the implementation of the LLA.
a Internal factors within each setting including culture and management
The investment of time and energy by SLTs is often thwarted by a setting’s own different priorities and the fact that some individual LLs do not necessarily support the ongoing embedding of good practice. Jago and Radford (2017) identify the individual practitioner as a potential barrier or enabler to this type of collaborative working and Baxter et al. (2009) note the influence of power and hierarchy within teams in implementing collaborative working. Payler and Georgeson (2013) also note the historical disparity in resourcing issues within different types of setting, affecting the potential ability of practitioners to collaborate effectively.
The dissemination of skills needs to be considered as a workforce development issue within the EY where research has shown that mentoring approaches and following areas of specialist practice knowledge support retention (Jovanovic, 2013). This finding also supports the view expressed in the Bercow review (2018) which highlights the role of local leaders in embedding SLC support systems.
The setting leadership and the amount of devolved leadership was central to the perceived success of the Approach and a key learning point was in relation to the role of leadership in the EY context. Hence, managerial support was seen as crucial alongside the leadership of the LLA by the individual LL. Edbrooke-Childs et al. (2019) identify the relevance of careful, transparent planning and leadership in enabling collaborative working processes for facilitating implementation and embedding effective change. The pedagogical approach of the training is critical to its effectiveness and SLTs need to tailor training to individual contexts and to ensure learners are given time to reflect on and assimilate their learning. McLeod (2011) suggests that time is crucial for continued professional ownership and implementation of these collaborative training programmes.
b Individual characteristics of the LL
Personal characteristics were material to the effective implementation, including capacity to lead, motivation and confidence levels (Gorozidis and Papaioannou, 2014). SLTs need to develop an awareness of the range of knowledge and skills which practitioners bring to their roles and to adapt their approaches to training and mentoring accordingly. This echoes Payler and Georgeson’s (2013) research into the wide variation in confidence and competence encountered in inter-professional working which is dependent on both practitioner experience and type of setting, requiring educator awareness at each stage of training. The view of personal leadership qualities as being central to the dissemination and ongoing maintenance of the LLA echoes Miech et al.’s (2018) review which indicates that a champion who is enthusiastic and invested in a programme from the start is a strong factor in successful implementation.
c Factors external to the setting, including the influence of the SLTs own confidence and availability as a trainer and mentor
SLTs expressed frustrations at the lack of time they had to invest in the LLA and their own lack of training, although the evidence suggests that SLTs place a high value on collaborative working. This theme corroborates the findings from a number of other studies which have been conducted over many years without any apparent resolution of this issue which is surprising, particularly considering that consultative approaches to SLT service delivery have been implemented, in part, as a way of addressing the demands on the SLT service (Baxter et al., 2009; White and Spencer, 2018).This appears to be a successful intervention, and therefore warrants adequate time to make it effective. The NCFP SLT service have considered improvements based on these findings.
SLTs reflected on their own knowledge and skills which affected their effectiveness as implementers of the intervention. Specifically, they expressed that their clinical training had not prepared them for the way a collaborative role would operate within the LLA (Jago and Radford, 2017). If this type of approach is going to continue to be used as an intervention model, then SLTs should receive pre-qualification training in this way of working.
Therapists expressed a number of different views about how working using the LL approach fitted with their clinical role. There are implications for higher education institutions if the training of future SLT practitioners is to prepare them for the demands of the ‘new’ collaborative working environment.
2 Limitations
Although participants gave their views on the value of the LLA, we did not specifically seek to research the effectiveness of the Approach itself. Further research, beyond implementation to determine the impacts of the LLA for children in the settings where it is implemented would be a relevant next step from this initial piece of research in order to judge whether the SLT’s perceptions of practitioner competence correlate with any specific improvements in children’s SLC outcomes.
As a result of our findings, the NCFP SLT service actioned a number of changes to their implementation of the LLA which are elaborated further in the discussion. It would have been valuable to have had the opportunity to follow up the study with participants and to be able to discuss improvements and developments in implementation as part of this research. However, due to service priorities, our approaches to revisit some of these changes were not able to be followed up, which was a frustration for the researchers. In relation to limitations in the research process, the addition of a third party might have supported the data coding and analysis, however, the dialogic discussion between the two researchers was robust throughout, resulting in full agreement at each point in the coding and analysis process.
A parallel study was carried out by the researchers with the LL practitioners themselves. These findings, which provide additional insights into the LLA from a practitioner perspective, are documented elsewhere in publications by the authors (Kent and McDonald in Kent and Moran, 2019; Kent and McDonald, 2019).
3 Impacts
Although this research was designed to explore the implementation of the LLA rather than its effectiveness, it has supported insight into wider SLT service delivery issues, and it is possible to provide some preliminary evidence of impacts. Research findings were shared with participants and with the NCFP SLT team in order to inform service planning for ongoing implementation. The team have actioned a number of changes to their implementation of this service delivery model, including reviewing the recruitment process of LLs at the start of implementation. There has been consultation with experienced LLs to develop the training offered to practitioners new to the role, and buddying relationships have been set up. SLTs have provided differentiated network meetings for new LLs and have updated all LL resources, in particular providing a fully updated guide for setting owners/managers.
Footnotes
Appendix 1
Interview schedule for speech and language therapists (SLTs).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.