
Abstract
Supportive parent–child interactions are critical for facilitating typically developing children's language and social skill development. For children who are late-to-talk, parent–child interactions may be particularly important to address as a means of supporting growth in children's early language abilities. Target Word is one parent-implemented intervention for children who are late-to-talk that teaches parents strategies for facilitating more meaningful communicative interactions with their children, but little is known about the impact of this program on parent–child interactions. The aim of the present study was to determine whether the nature of parent–child interactions changed during the virtual Target Word program and whether changes in parent–child interaction were associated with parents’ participation in the virtual Target Word program. A total of 40 children between 16 and 27 months of age who were identified as late-to-talk and their caregivers were assigned to a treatment or wait-list control group. Parent–child interactions were captured virtually using Zoom at four time points and measured using the Parenting Interactions with Children: Checklist of Observations Linked to Outcomes (PICCOLO). Families completed book reading, pretend, and manipulative play tasks. While 16 of the 20 families in the treatment group completed the study, only 5 of the 20 families in the wait-list control group completed the entire study. Data were analyzed using a constrained longitudinal data analysis approach. Group differences in parent–child interactions were not statistically different at any time point. Further research is necessary to evaluate whether parent–child interactions are in fact impaired in late talkers, the psychometric properties of the PICCOLO for late talkers, and whether parent–child interactions may be assessed differently in virtual versus in-person environments.
Keywords
I Introduction
The importance of supportive parent–child interactions for young children's language development is well-documented in the literature (Adamson et al., 2020; Mathis and Bierman, 2015; Morris et al., 2017). In the early childhood, supportive caregivers provide positive reinforcement, encourage back-and-forth interactions, and employ nonharsh discipline during interactions with their children to facilitate language and social skill development (Raby et al., 2015; Suttora et al., 2021). Conversely, more coercive parent–child interactions, which are often displayed by parents experiencing higher levels of parenting-related stress, have been shown to negatively affect children's language development (Baumrind, 2013; Kucker et al., 2021; Muller et al., 2019; Neece et al., 2012). While supportive parent–child interactions are known to contribute to language development in typically developing children, they may also serve as a protective factor for children with language difficulties by creating a language rich learning environment (Lieneman et al., 2017). Additionally, supportive parent–child interactions foster a connected parent–child relationship, which is associated with stronger language comprehension skills (Jokihaka et al., 2022). One specific population for which supportive parent–child interactions may facilitate language development is children who are late-to-talk (Girolametto et al., 2002; Levickis et al., 2014).
Children who are “late-to-talk” are between 18 and 30 months of age and have delayed expressive language, but no deficits in language comprehension or other areas of development (Rescorla, 2011; Singleton, 2018). The cause of children being late-to-talk remains unknown, but numerous variables have been identified as being associated with late-talking including difficultly with attention, being a biological male, being of lower socioeconomic status, and lower parental responsiveness (Hammer et al., 2017). For children who are late-to-talk, there is a risk of the language difficulty becoming a developmental language disorder which is associated with long-term impacts on language, social, and academic outcomes (Rescorla, 2009; Rice et al., 2008; Singleton, 2018). Previous research on parent–child interactions in the late talker population suggests that parents of late talkers are less likely to follow their child's lead during play, may change topics often in an effort to engage their child in conversation, and verbalize their thoughts less when interacting with their children, which may limit opportunities for engaged language learning (Vigil et al., 2005). This approach to interaction is termed an “idiosyncratic feedback style,” and it has been suggested that parents of children who are late-to-talk engage in idiosyncratic feedback to tailor their communication strategies to their child's limited expressive language skills (e.g. parents respond less often because children initiate less often, parents are more likely to introduce a new topic other than what the child has shown interest in because they want to engage their child in conversation), which unfortunately restricts the language input children receive (Hawa and Spanoudis, 2014; Tannock and Girolametto, 1992). Perhaps due to their more limited interactions, mothers of children who are late-to-talk have reported less functional parent–child interactions (i.e. interactions in which children are more socially withdrawn) than mothers of children with typically developing language on commonly used parent-report measures (e.g. Child Behavior Checklist, Vineland Adaptive Behavior Scales) reflecting the extent to which they felt satisfied with their interactions with their children (Irwin et al., 2002). Moreover, these less functional parent–child interactions create a compounding problem through which children are also more socially withdrawn and less interested in play (Irwin et al., 2002). Parental responsiveness, one component of parent–child interactions, may be particularly important for facilitating communicative interactions in children who are late-to-talk as it has been demonstrated to be proportional to the number of utterances children initiate (Blackwell et al., 2015; Paul and Elwood, 1991). In fact, research has highlighted that increased caregiver responsiveness can increase the frequency of verbal productions, vocabulary size, and improve overall expressive and receptive language skills in children who are late-to-talk (Girolametto et al., 2002; Levickis et al., 2014). Thus, one way of supporting language development in children who are late-to-talk may be by changing the way in which parents and children interact.
Parent-implemented programs that teach parents strategies to facilitate children's language through everyday communicative interactions are commonly used by speech-language pathologists (SLPs) as a first intervention for children who are late-to-talk (Carson et al., 2022). Generally, parent-implemented programs have been shown to improve both child and parent behaviors when offered once per week for more than 8 weeks, even when delivered virtually (Baharav and Reiser, 2010; Camden et al., 2019). For children who are late-to-talk specifically, parent-implemented programs have been shown to positively impact children's language and social communication development (Buschmann et al., 2015; Carson et al., 2022; Cunningham et al., 2019; DeVeney et al., 2017; Girolametto et al., 2001; Heidlage et al., 2020). Programs for parents of late-talkers have also been shown to positively impact parents’ use of specific strategies to support children's language development (e.g. focused stimulation, modeling, and turn-taking), which are key components of responsive parenting and have been associated with gains in children's expressive vocabulary (Girolametto et al., 1996, 2002; Kruythoff-Broekman et al., 2019; Levickis et al., 2014; Wake et al., 2011). For example, one program called Parent-Child Interaction Therapy (PCIT; Falkus et al., 2016) has been used widely with preschoolers with various language difficulties (e.g. children who are late-to-talk, children with more complex language comprehension and/or production difficulties). Research on PCIT has shown that the program improves parent–child interactions, child language outcomes, and that parents feel empowered to facilitate communication with their child after participating (Falkus et al., 2016; O’Toole et al., 2021). Parent-implemented programs may provide an important avenue for studying parent–child interactions in children who are late-to-talk, as in addition to specific language facilitation strategies, parents learn to adjust their interaction style to better support their child's language development during daily activities (Roberts and Kaiser, 2011).
One parent-implemented early language intervention for children who are late-to-talk is Target Word, The Hanen Program for Parents of Children who are Late Talkers (Earle and Lowry, 2015). This program was developed by the Hanen Centre, a nonprofit organization in Toronto, Canada. The Target Word program is run by a Hanen certified SLP who has been trained to implement the program components and focuses on teaching parents to use various strategies to support their children's early language and social communication development (Earle and Lowry, 2015). While the Target Word program focuses on teaching parents to use various language facilitation strategies, it also aims to support and strengthen parent–child interactions to ensure those language facilitation strategies can be applied in meaningful everyday situations. Previous research on the Target Word program has reported gains in children's expressive vocabulary, morphosyntax, receptive language, phonology, and communicative participation, although gains have not always been attributed directly to the program and the long-term benefits of the intervention require further investigation (Cunningham et al., 2019; Hatherly et al., 2023; Kruythoff-Broekman et al., 2019; Kwok et al., 2020).
Most of the available literature has focused on the Target Word program being delivered in-person, although the program can also be delivered virtually. While the in-person and virtual Target Word programs parallel one another, outcomes may differ depending on the context in which the program is delivered. Children's communication outcomes following the virtual Target Word program have only been evaluated recently (Hatherly et al., 2023), and additional evidence is needed to better understand the full impact of the virtual program, which includes understanding whether and how the program may impact the nature of parent–child interactions. The objective of this study was therefore to explore potential changes in the nature of parent–child interactions during parents’ participation in the virtual Target Word program. This study was an exploratory, secondary analysis of parent-responsiveness data collected as part of a broader Pragmatic Waitlist Control Trial exploring children's communication outcomes that was conducted during the COVID-19 pandemic (Hatherly et al., 2023). As such, Target Word programs were run and data were collected remotely via Zoom videoconferencing sessions. The specific research questions for this exploratory study were: (1) does the nature of parent–child interactions change during the virtual Target Word program and (2) are changes in parent–child interaction associated with parents’ participation in the virtual Target Word program?
II Methods
1 Ethics
The Health Sciences Research Ethics Board at the University of Western Ontario provided approval for this study (approval number: 115402).
2 Participants
Two community preschool organizations in Ontario, Canada supported recruitment of families to the study. Both organizations regularly ran the Target Word program and agreed to identify parents of children who were late-to-talk on their caseloads. Parents of 46 children were invited, and 45 agreed to participate. However, only 40 of the 45 families were included in the study, as four children were referred for additional services and one child experienced a significant language burst prior to the study beginning and no longer met the inclusion criteria. Families were assigned to either a wait-list control or treatment group using a 2:1 ratio to account for potential dropouts and natural growth spurts. This means at each community organization, the first two children enrolled were put into a control group, and the third child was put into an experimental group. This process continued until both the control and experimental groups at the organization were filled. Parents at one organization were assigned based on the order in which they received their initial assessment, and those at the second organization were assigned based on their position on a waitlist as they had been recently assessed. Four SLPs (two at each site) ran the Target Word programs, each running a treatment group first (i.e. times 1 to 2) and a wait-list control group second (i.e. times 2 to 3). Each SLP had 4 to 6 families in their programs. Parents of children in the treatment group began Target Word immediately, while those in the control group were placed on a waitlist and began Target Word at time 2. Child demographics are reported in the results section. Parent demographics were not collected as part of the primary study (Hatherly et al., 2023), as the central focus was on children's speech and language outcomes.
3 The Target Word program
To be eligible for the Target Word program children must have a difficulty with expressive language, which is defined by the Hanen Centre as children between 18 and 20 months with less than 24 words, 21 to 24 months with less than 40 words, 24 to 30 months with less than 100 words, and/or no word combinations at 24 months of age. Eligible children must also: (1) be under 30 months of age; (2) have typically developing language comprehension skills or a mild receptive difficulty; (3) have typically developing play, social, motor, and cognitive skills; and (4) present with two or more factors identified by the Hanen Centre as increasing the likelihood of them developing a speech or language disorder (Earle and Lowry, 2015). Example risk factors include limited use of gestures, a restricted speech sound inventory, and a family history of language difficulties.
SLPs who complete the Target Word training program are certified by the Hanen Centre to run the intervention which consists of both group and individual sessions over the course of 10 to 12 weeks. The first two group sessions focus on training parents to use strategies to facilitate communicative interactions with their children (e.g. being face-to-face, letting the chid lead). In the first individual session parents demonstrate their use of the interaction strategies learned to engage in an interactive activity with their child. These interactions are recorded, allowing the SLP and parent to review the videos together to identify areas of strength and areas for improvement. At the end of the first individual session, parents and SLPs collaborate to identify 10 functional target words for the child. The remaining group sessions consist of further training focused on increasing models of the selected target words and supporting language development through the use of questions, expansions, and pretend play. This is followed by a final individual video feedback session at which both the parent's and child's progress are discussed (Earle and Lowry, 2015). Families were free to engage in the intervention in the way that best suited them (i.e. two caregivers attended and one caregiver attended) as is the usual practice of the SLPs who delivered the intervention. The gender of the caregiver who participated in the programs was not collected, but it should be noted that it is typically mothers who participate in these types of interventions (Akemoglu et al., 2020).
4 Procedures
Parent–child interactions were assessed for both groups at four time points (Figure 1): (1) initial assessment (baseline), (2) after the treatment group completed Target Word, (3) after the wait-list control group completed Target Word and the treatment group completed their consolidation period (10–12 weeks during which the parents practice the skills they have learned without direct SLP feedback, and (4) after the wait-list control group's consolidation period. At each assessment point, parent–child interaction data were collected via Zoom where families met with graduate research assistants (RAs) to complete three play tasks. Prior to beginning the Target Word program, families were mailed a standardized set of toys to use during the videoconferencing sessions. The toy sets consisted of three activities: (1) a plush food set in a basket (hotdog, eggplant, pasta, etc.); (2) a “lift-the-flap” book (“Dear Zoo”); and (3) bubbles and wind-up toy. Families were asked to hide the toys until their first assessment session as well as between assessments so they would remain novel for the children.
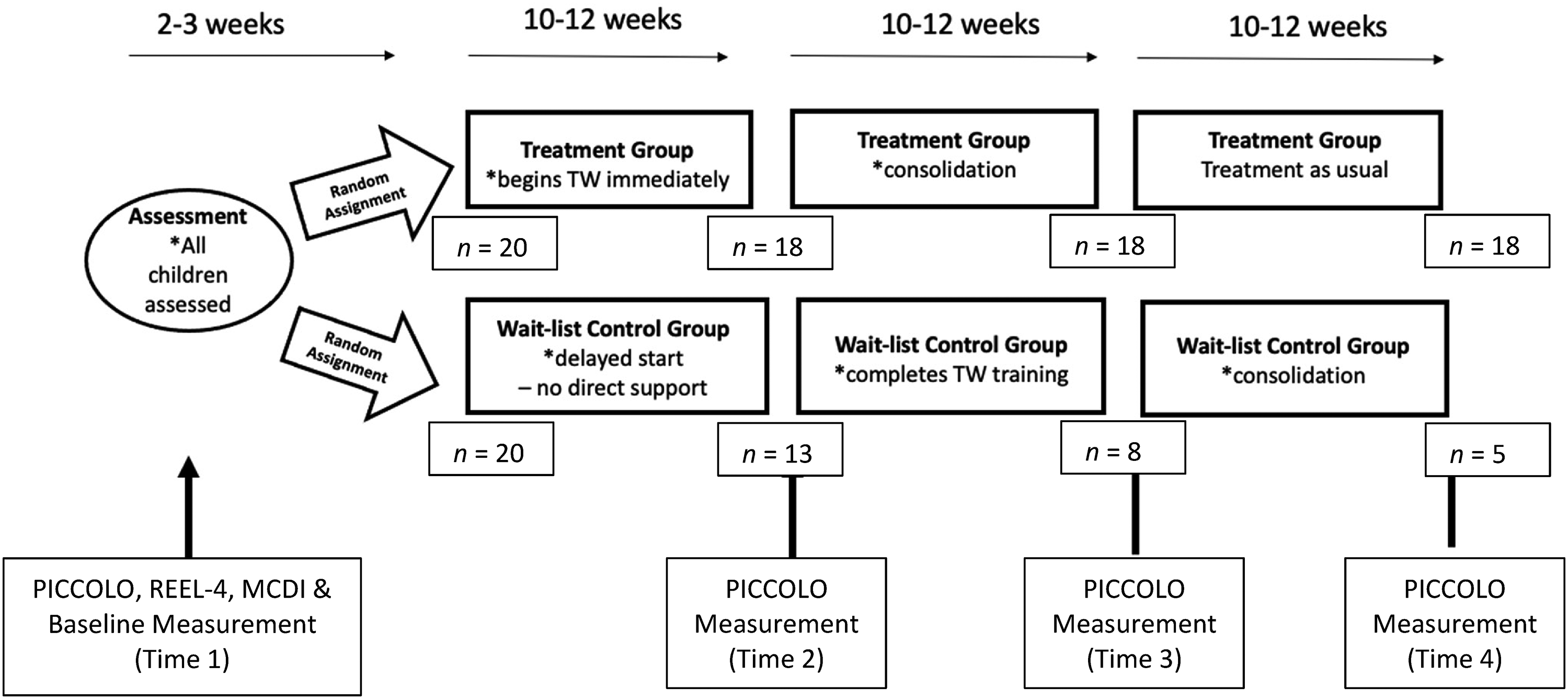
Study design showing each groups progression and measurement point. *Note: “Treatment as usual” refers to other interventions participants in the experimental group may have been receiving based on need following their consolidation period. As per usual care, some children would have received additional services (e.g. individual intervention), while others may have been discharged (e.g. with age-appropriate outcomes).
According to the methods outlined in the Parenting Interactions with Children: Checklist of Observations Linked to Outcomes (PICCOLO) assessment tool (Roggman et al., 2013), families were instructed to engage in three separate play activities: (1) book reading—reading of “Dear Zoo” (Campbell, 2007); (2) pretend play with a plush food set; and (3) manipulative play with bubbles and a wind-up toy. Each play activity lasted between 5 and 10 minutes, and families were asked to do each task for at least 5 minutes. The toys corresponding to each play activity were shipped in separate bags, and parents were asked to take out one bag at a time, engage in play with their child using each toy the way they normally would, and only swap the toys when asked. If a family appeared to be finishing a task early, RAs reminded them of how much time was remaining before the next play activity would begin. If a family was not able to complete a full 5 minutes for an activity (e.g. child was ready to move on to a new task), data were not coded as interactions of less than 5 minutes did not meet the inclusion criteria outlined in the PICCOLO manual. During each play activity, the RA turned off their camera and remained muted to eliminate potential distractions. Interactions were recorded using Zoom videoconferencing software and uploaded to a secure server housed at the University of Western Ontario immediately following each session.
Families had the same SLP at each assessment point, but the graduate RAs completing assessments may have changed over the course of the study. All baseline data (Receptive-Expressive Emergent Language Test (REEL)-4 and MacArthur–Bates Communicative Development Inventories (MCDI)) were collected by the graduate RAs. All other data were collected by both SLPs and graduate RAs who were aware of which group families were assigned to at a given time point. This division of labor was necessary to help reduce the burden on practicing SLPs, who had little time to engage in research. Knowledge of group assignment was required as it impacted which measures were completed at different time points. All study components were completed in English.
5 Baseline measures of language ability
a Receptive-Expressive Emergent Language Test
The REEL-4 (Brown et al., 2020) is a parent-report measure of children's language production and comprehension skills and is validated for children from birth to 36 months of age (Earle and Lowry, 2015). For the purposes of this study, the REEL-4 was used to screen children's receptive language skills to determine whether they met the Target Word program criteria for being classified as late-to-talk (i.e. no or a mild receptive language delay), and to confirm that groups were statistically similar in terms of receptive language at baseline. Children were included in the study if their scores indicated no or a mild difficulty (i.e. within 1.5SD of the mean), aligning with Target Word recommendations (Earle and Lowry, 2015).
b MacArthur-Bates Communicative Development Inventories: Words and sentences
The MacArthur-Bates Communicative Development Inventories is a two-part parent report measure of children's expressive language, that is validated for children aged 16 to 30 months (MCDI; Fenson et al., 2007). In part 1, parents report their child's use of specific vocabulary items to provide a total vocabulary score. In part 2, parents report on their child's morphosyntax skills. From part 2, the complexity (which of two sentences sounds more like the child) and examples (mean length of child's three longest utterances; M3L) sections were used to assess morphosyntax. Both parts of the MCDI were completed to determine if children's expressive language skills were statistically similar at baseline.
6 Longitudinal measurement of parent–child interaction qualities
a Parenting Interactions with Children: Checklist of Observations Linked to Outcomes
The PICCOLO (Roggman et al., 2013) was used to evaluate changes in parent–child interactions over the course of the study. The PICCOLO is a validated 29-item checklist of parental behavior domains, that includes four parts. These four parts describe strengths-based parent–child interaction qualities that consist of: (1) affection—warmth, physical closeness, and positive expressions toward the child; (2) responsiveness—responding to the child's cues, emotions, words, interests, and behaviors; (3) encouragement—active support of exploration, effort, skills, initiative, curiosity, creativity, and play; and (4) teaching—shared conversation and play, cognitive stimulation, explanations, and questions. Affection, responsiveness, and encouragement each have seven items, and teaching has eight items. Each item is scored on a scale from 0 to 2 to describe how frequently each parenting behavior is demonstrated, with 0 being “Absent”—no behavior observed, 1 being “Barely”—brief, minor, or emerging behavior, and 2 being “Clearly”—definite, strong, or frequent behavior. Guidelines for rating each item are provided on the PICCOLO test form as well as in the user manual. For example, item 6 on the Affection subscale states that the parent “is engaged in interacting with child,” and the guidelines state that in order to score this item a 2, it should be observed that the “Parent is actively involved with child, not just with the activity or with another adult.”
The PICCOLO reports good interrater reliability (0.77 across domain scores) and internal consistency (alpha averaged 0.78 across the four domains) (Roggman et al., 2013). Validity and reliability evidence has been collected for children aged 10 to 47 months at both single assessment points and longitudinally, including for children from ethnically diverse backgrounds (Bayoğlu et al., 2013; Roggman et al., 2013). Additionally, the PICCOLO has validity evidence for multiple language versions (e.g. English, Spanish, and Turkish), and for use with parents of children with disabilities (Innocenti et al., 2013; Vilaseca et al., 2019).
Methods for establishing coder reliability outlined in the PICCOLO manual were followed, which involved establishing reliability with practice data prior to coding study data (Roggman et al., 2013). The first author trained four undergraduate RAs and ensured reliability was met. Training consisted of reading the PICCOLO manual, watching PICCOLO training videos and discussing the rationale for recommended scores, followed by independent coding of approximately eight PICCOLO training videos to establish reliability. RAs were required to reach a criterion of ICC = 0.90 on one novel PICCOLO training video, before moving on to coding the dataset. While coding the data, RAs were blinded to which group and time point they were coding to limit potential biases regarding expected outcomes. To further limit biases, each RA coded all videos for one specific time point to ensure they only saw each family once. RAs entered parent–child interaction ratings directly into REDCap (Harris et al., 2009), a secure online data collection system that was housed at the University of Western Ontario.
7 Statistical analyses
Descriptive statistics were used to assess children's demographic data and baseline test scores. For language measures, t-tests were used to analyze group differences at baseline.
Prior to analyzing PICCOLO data, scores were pooled to create an average of the item mean scores for each domain (i.e. affection, responsiveness, encouragement, and teaching) across all three play activities. The average of item mean scores were used per the PICCOLO manual's data on scale stability which indicates that earlier scores predict subsequent scores within each domain with moderate stability (Roggman et al., 2013), while the decision to pool domain scores across play activities was based on similar studies using the PICCOLO (e.g. Montirosso et al., 2023).
Pooled PICCOLO data were analyzed using constrained longitudinal data analysis (cLDA) models, which were used to investigate within group changes between assessment points as well as between group differences between assessment points for each PICCOLO domain. The cLDA method constrains group means at baseline to be equal, which assumes any imbalance is due to chance and ensures independence of the groups (Coffman et al., 2016). cLDA then evaluates differences in group scores at subsequent assessment points using a double-arm design (i.e. treatment and wait-list control groups). The double-arm design allows for the comparison of the variances of estimated group differences across each assessment point (Lu, 2010). The cLDA approach allowed for control of both fixed effects, including time and treatment by time interaction, and random effects, including within-individual correlations across the repeated measure and domains. The model's treatment by time fixed effect evaluated predicted mean scores at each assessment point and their possible corresponding association with group differences. Accounting for within-individual correlations provided the ability to explore scores related to families’ scores at previous assessments and was key for this study as within-family data were highly correlated. The cLDA approach provides a useful method for estimating group differences in longitudinal studies as it has the ability to handle missing data without deleting participants, providing a more precise estimate of treatment differences. cLDA also controls for fixed effects in a way that produces efficient treatment effect estimates, and is an effective approach for smaller sample sizes (Coffman et al., 2016). For the purposes of this study, statistical significance was set using two-sided p-values < 0.05 (i.e. p < 0.025). All analyses were conducted using R Statistical Software (v4.2.2; R Core Team, 2022).
III Results
1 Participants
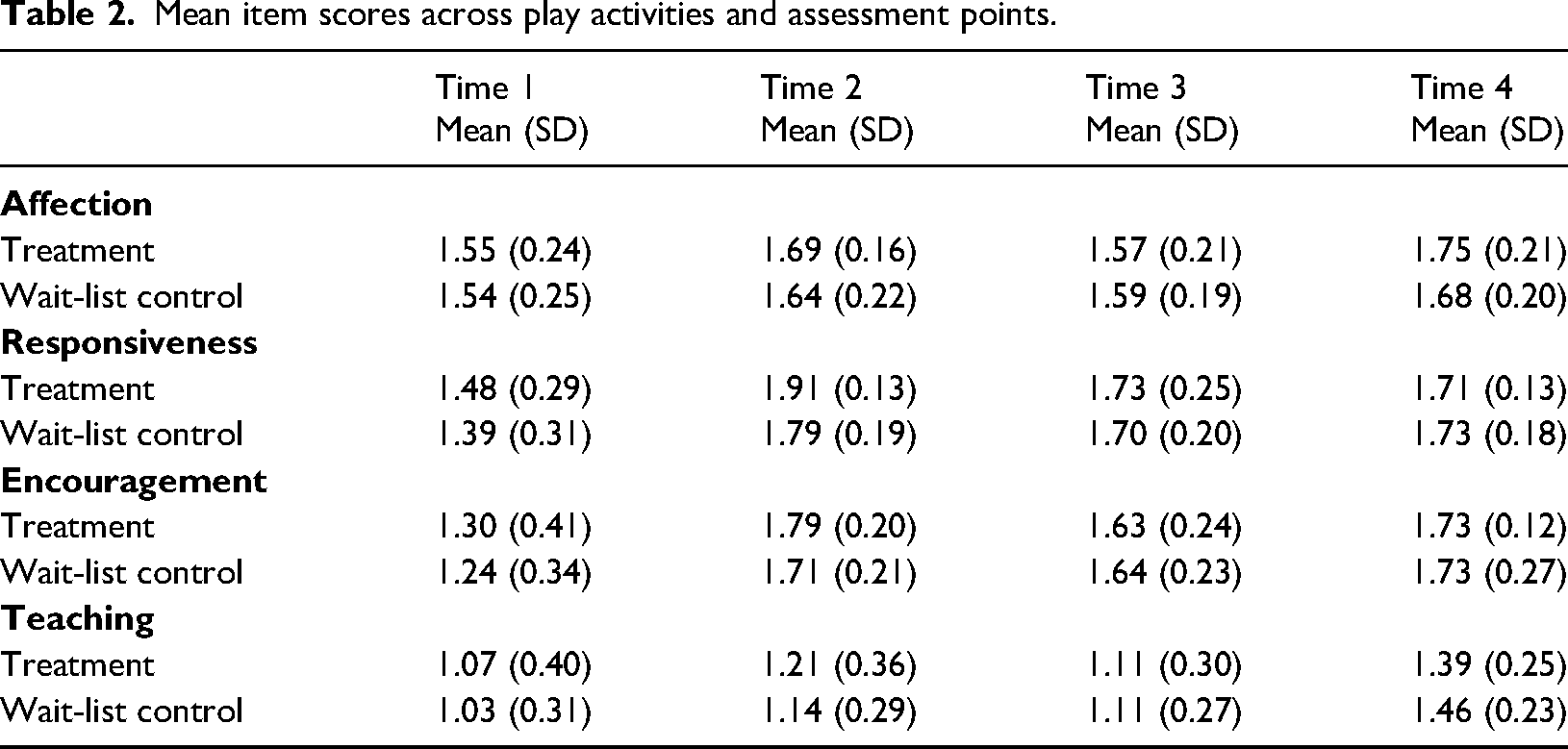
From a total of 40 participants, 20 children were assigned to both the treatment and wait-list control groups. Children in the treatment group were between 16 and 25 months of age (M = 21.0, SD = 2.63), while children in the wait-list control group were between 17 and 27 months of age (M = 21.6, SD = 2.82). A summary of all demographic and baseline data, including REEL-4, MCDI, and PICCOLO scores is presented in Table 1. Several participants in both groups did not complete the study (see Figure 1), however, all available data were included in the cLDA analysis given its ability to handle missing data. A summary of true mean item scores across play activities and assessment points is presented in Table 2. Additional information on children's speech and language outcomes can be found in Hatherly et al. (2023).
Child demographics and baseline measures.
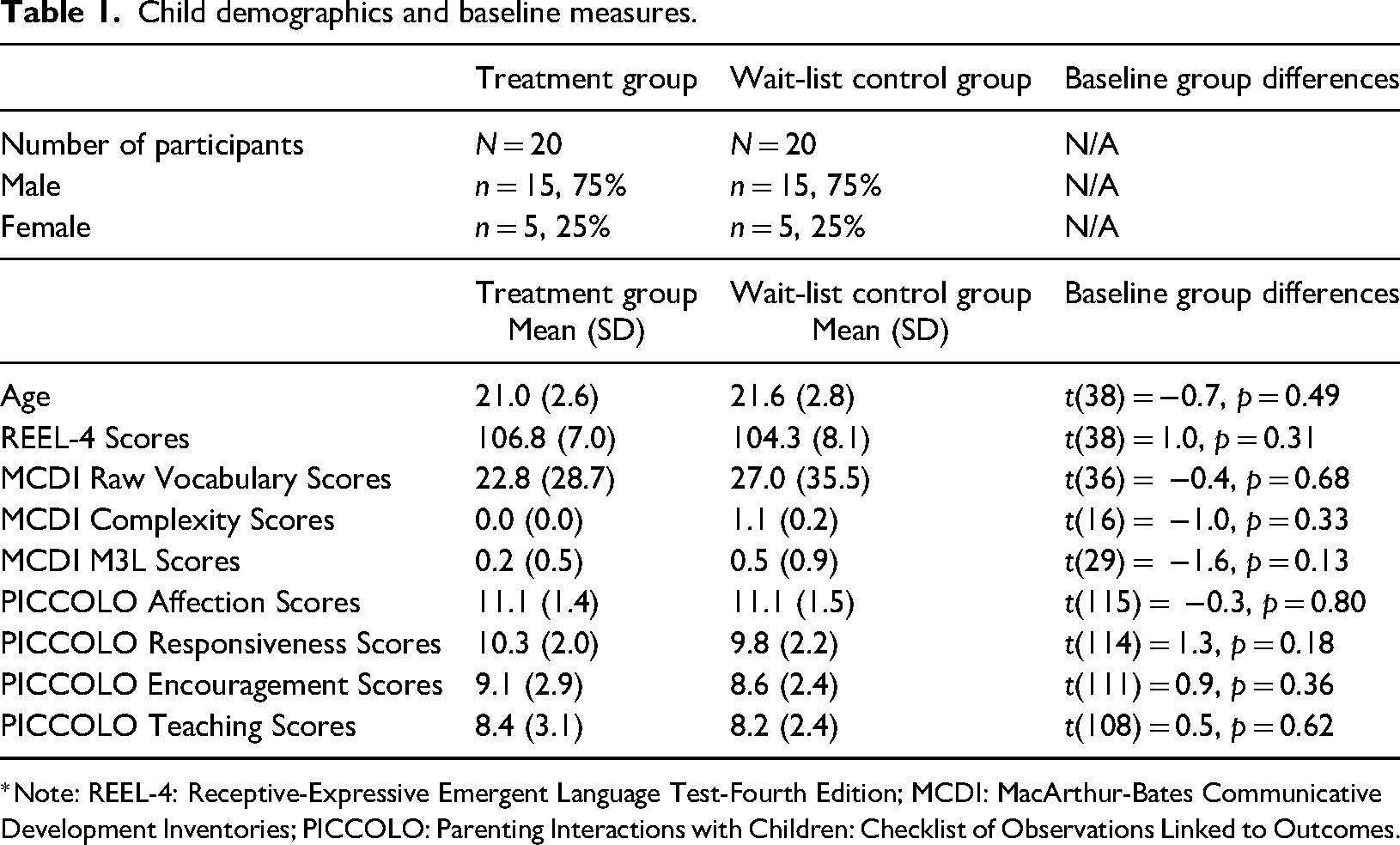
*Note: REEL-4: Receptive-Expressive Emergent Language Test-Fourth Edition; MCDI: MacArthur-Bates Communicative Development Inventories; PICCOLO: Parenting Interactions with Children: Checklist of Observations Linked to Outcomes.
Mean item scores across play activities and assessment points.
2 PICCOLO scores
a Affection
From times 1 to 2, the treatment group had a significant change in scores (0.13; [95% CI: 0.06 to 0.20], p < 0.025*), while the wait-list control group did not have a significant change (0.08; [95% CI: 0.01 to 0.15], p = 0.03). From times 2 to 3, the treatment group had a significant change in scores (−0.11; [95% CI: −0.19 to −0.04], p < 0.025*), while the wait-list control group did not have a significant change (−0.07; [95% CI: −0.17 to 0.01], p = 0.10). From times 3 to 4, the treatment group had a significant change in scores (0.16; [95% CI: 0.09 to 0.24], p < 0.025*), while the wait-list control group did not have a significant change (0.08; [95% CI: −0.02 to 0.19], p = 0.10).
cLDA revealed that group differences on the Affection domain were not statistically significant at time 2 (0.05; [95% CI: −0.04 to 0.15], p = 0.27), time 3, (0.02; [95% CI: −0.09 to 0.12], p = 0.77), or time 4 (0.09; [95% CI: −0.02 to 0.20], p = 0.10), as shown in Figure 2.
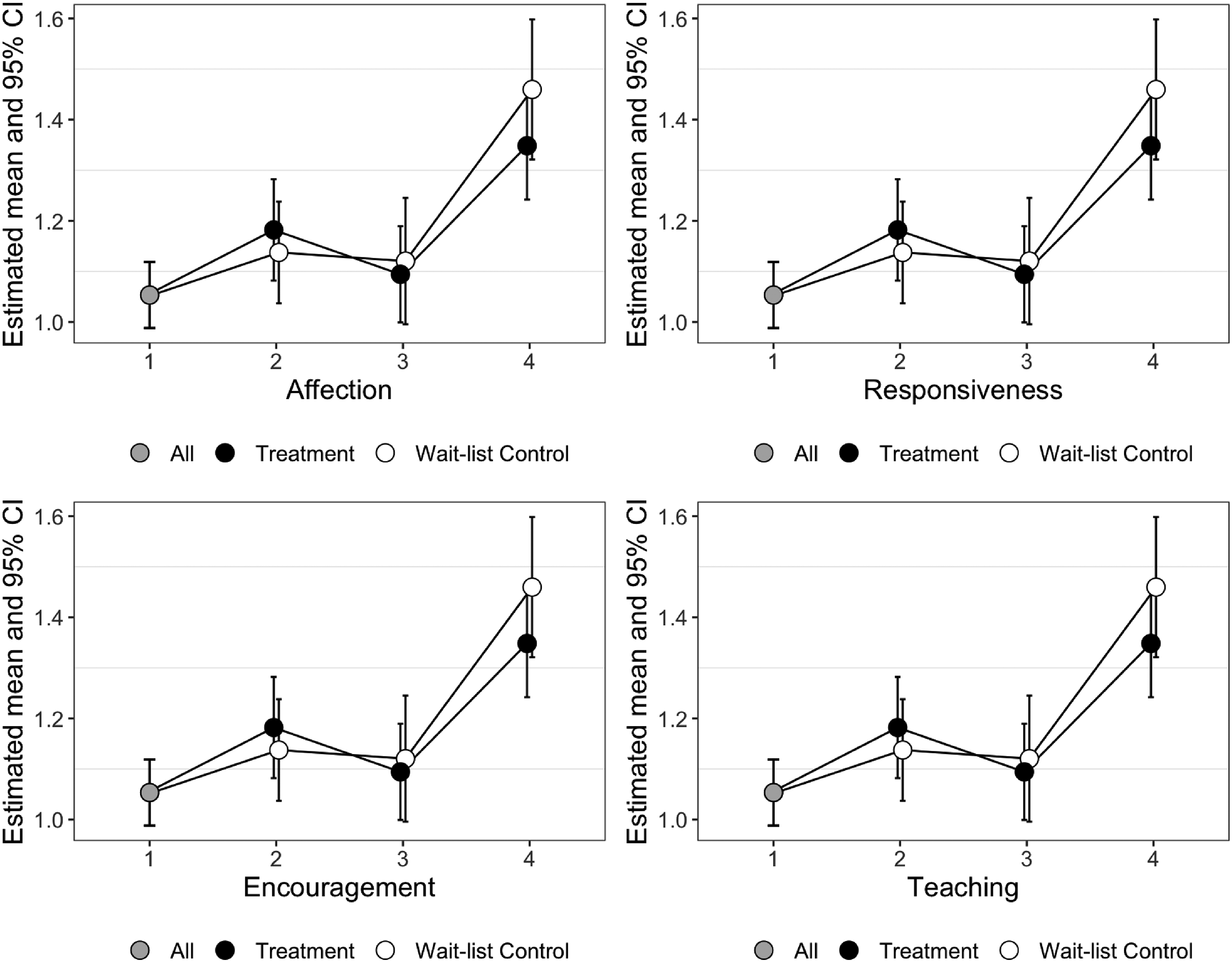
cLDA estimated means and confidence intervals of domain item mean scores across play activities and time points. *Note: Between Time 1 and Time 2, the treatment group received Target Word. Between Time 2 and Time 3, the treatment group had a consolidation period, while the wait-list control group received Target Word. Between Time 3 and Time 4, the treatment group received services as usual, while the wait-list control group had a consolidation period. cLDA: constrained longitudinal data analysis.
b Responsiveness
From times 1 to 2, both the treatment group (0.45; [95% CI: 0.37 to 0.52], p < 0.025*) and the wait-list control group (0.36; [95% CI: 0.29 to 0.43], p < 0.025*) had statistically significant changes in scores. From times 2 to 3, the treatment group had a significant change in scores (−0.18; [95% CI: −0.26 to −0.10], p < 0.025*) while the wait-list control group did not have a significant change (−0.09; [95% CI: −0.18 to 0.01], p = 0.08). From times 3 to 4, the treatment group (−0.06; [95% CI: −0.15 to 0.02], p = 0.12) and the wait-list control group (−0.01; [95% CI: −0.13 to 0.10], p = 0.86) did not have significant changes in scores.
Group differences on the responsiveness domain were not statistically significant at time 2 (0.09; [95% CI: −0.01 to 0.19], p = 0.08), time 3, (−0.01; [95% CI: −0.12 to 0.10], p = 0.89), or time 4 (−0.06; [95% CI: −0.19 to 0.06], p = 0.34), as shown in Figure 2.
c Encouragement
From times 1 to 2, both the treatment group (0.51; [95% CI: 0.42 to 0.61], p < 0.025*) and wait-list control group (0.44; [95% CI: 0.35 to 0.54], p < 0.025*) had significant changes in scores. From times 2 to 3, the treatment group had a significant change in scores (−0.15; [95% CI: −0.26 to −0.05], p < 0.025*) while the wait-list control group did not have a significant change (−0.06; [95% CI: −0.18 to 0.07], p = 0.36). From times 3 to 4, the treatment group (0.07; [95% CI: −0.04 to 0.18], p = 0.22) and the wait-list control group (0.07; [95% CI: −0.08 to 0.22], p = 0.37) did not have significant changes in scores.
Group differences on the encouragement domain were not statistically significant at time 2 (0.07; [95% CI: −0.05 to 0.19], p = 0.24), time 3, (−0.03; [95% CI: −0.16 to 0.11], p = 0.71), or time 4 (−0.03; [95% CI: −0.18 to 0.13], p = 0.72), as shown in Figure 2.
d Teaching
From times 1 to 2, the treatment group had a significant increase in scores (0.13; [95% CI: 0.02 to 0.23], p < 0.025*) while the wait-list control group did not have a significant increase (0.08; [95% CI: −0.02 to 0.19], p = 0.12). From times 2 to 3, the treatment group (−0.09; [95% CI: −0.20 to 0.03], p = 0.14) and wait-list control group (−0.02; [95% CI: −0.16 to 0.12], p = 0.81) did not have significant changes in scores. From times 3 to 4, both the treatment group (0.25; [95% CI: 0.13 to 0.38], p < 0.025*) and wait-list control group had significant changes in scores (0.34; [95% CI: 0.18 to 0.50], p < 0.025*).
Group differences on the Teaching domain were not statistically significant at time 2 (0.04; [95% CI: −0.09 to 0.18], p = 0.52), time 3, (−0.03; [95% CI: −0.18 to 0.12], p = 0.73), or time 4 (−0.11; [95% CI: −0.28 to 0.06], p = 0.19), as shown in Figure 2.
IV Discussion
The primary objectives of the present study were to explore whether the nature of parent–child interactions changed following families’ participation in the virtual Target Word program, and to determine whether changes were associated with families’ involvement in the virtual program. While there were significant changes in PICCOLO scores were observed within-groups at various time points, these changes varied with each domain and at each assessment point, making it difficult to conclude that changes were made during the virtual Target Word program. Additionally, as families in the treatment and wait-list control groups achieved statistically similar scores on the PICCOLO at all time points, it was not possible to conclude that any changes were due to families’ involvement in the virtual Target Word program. There are five potential explanations for the results observed in these data: (1) children who are late to talk perform differently than other populations previously studied using the PICCOLO; (2) the sociodemographic characteristics of the current sample may not have been representative of families with whom the PICCOLO is typically used; (3) changes in parental behavior occurred, but were specific to the Target Word program, transferring to limited differences on the PICCOLO; (4) the PICCOLO may not be sensitive to the types of interaction behaviors observed in parents of children who are late to talk; and (5) the virtual nature of the study may have impacted results. We consider each of these possibilities in detail below.
One possibility is that while children who are late-to-talk have a limited expressive vocabulary, other skills, including their ability to engage meaningfully with caregivers, are more closely aligned with their typically developing peers (Rescorla, 2011; Singleton, 2018). More specifically, it is possible ceiling effects were observed at baseline, preventing the possibility of detecting group differences. For instance, some of our results are discordant with previous research using the PICCOLO. In regard to the affection domain specifically, previous research has demonstrated that PICCOLO scores have significant age effects such that parents of younger children score higher than parents of older children (Montirosso et al., 2023). In our sample, scores on the affection domain fluctuated across the four assessment points as children grew older, suggesting they may perform differently than previously studied populations. While validity evidence has been collected for typically developing populations, to our knowledge the PICCOLO has not yet been validated for use with children who are late to talk. There may be specific differences for children who are late-to-talk on the PICCOLO domains, which could have masked possible treatments effects in the current study. Future research could compare parent–child interactions of children who are late-to-talk and their typically developing peers to explore potential differences.
Alternatively, it is possible that the characteristics of parents participating in the current study may have masked treatment effects. Although sociodemographic data were not collected at part of this study, all families were required to have a device with internet connectivity and the availability to support their child through approximately 20 h of virtual sessions, both with the research team and their community speech-language pathologist. Similar to studies on research during the COVID-19 pandemic, previous research on parent-implemented speech and language programs have documented that the majority of families participating have a household income over $60,000 (Meadan et al., 2014; Roberts et al., 2014). As such, it is possible our sample was not representative of those used in other PICCOLO studies. Moreover, although the cLDA method accounts for missing data, our results should be interpreted with caution due to the high attrition rate which may have impacted the internal validity of the study.
Another possible explanation for the null results of this study is that specific changes in parental behaviors that may be expected following a program like Target Word, could not be captured by the PICCOLO as a measure. For example, perhaps parents learned specific speech and language-focused strategies, rather than overall positive parenting behaviors. A similar study on the Target Word program explored changes in parents’ behaviors during the program and did report some behavior change with respect to parent–child interaction, however those changes were specific to skills taught during the program. Specifically, parents were observed to reduce pressure on their child to communicate and provide more opportunities for their child to take a turn (Kruythoff-Broekman et al., 2019). Kruythoff-Broekman et al. (2019) found that other aspects of parental interaction, such as responsiveness, did not change as a result of participating in the Target Word program. It is possible that parents do learn interaction skills, change behaviors, and that children's engagement improves during the Target Word program, but that those specific skills do not generalize to overall parent–child interaction quality as measured by the PICCOLO.
Relationships have been found with parenting behaviors and children's typically developing early language skills as measured using the PICCOLO (Rivero et al., 2023). However, to our knowledge the PICCOLO has not yet been trialed as a measure with children who are late-to-talk, or in a control trial of parenting behaviors for this population. While the PICCOLO is effective at measuring changes made within groups over time (e.g. Roggman et al., 2013), it is possible it may not be as sensitive to detecting group differences. For example, one recent study utilized the PICCOLO as a component of evaluating a psychosocial intervention for infants and their mothers and found that differences between the experimental and control groups on the PICCOLO were not statistically significant (Alves et al., 2022). Therefore, it is important to acknowledge that there may be some limitations to using the PICCOLO in a study of this design. Another consideration regarding the use of the PICCOLO in this study, is that SLPs who are clinically trained to work with children who are late-to-talk using the Target Word program, may have coded the data differently than the undergraduate RAs who were trained on the PICCOLO only for the purposes of this project. Additional evidence is needed to assess the utility of the PICCOLO for late-talkers and for making group comparisons.
A final possible explanation for the absence of group differences in this study is that the Target Word program and data collection took place virtually, which may have made parent–child interactions more challenging than they might have been in-person, both in terms of teaching the skills and capturing the interactions. As an example, child outcomes in our parallel pragmatic waitlist control trial of the virtual Target Word program (Hatherly et al., 2023) reported limited group differences across speech and language measures, a finding that did not align with past studies on the program when it was conducted in-person (Kruythoff-Broekman et al. 2019), suggesting outcomes could differ for the virtual versus in-person program. One reason outcomes may differ for the program depending on the mode of delivery is that there may have been further distraction in families’ homes during the virtual program, which was conducted during the COVID-19 pandemic when work-from-home conditions and virtual schooling demands may have been an issue (Kwok et al., 2022). These considerable changes to families’ home environments, combined with the Target Word program being conducted virtually, may have contributed to the findings of the present study. Similarly, it should be acknowledged that this study was conducted at the height of the COVID-19 pandemic, at a time when families were experiencing periods of heightened stress and anxiety, which may have impacted parent–child interaction quality (Brown et al., 2020; Roos et al., 2021).
Interpreting the results of this study was challenging as it was difficult to disentangle whether the lack of significant effects was a true null effect or whether results were impacted by factors including the sample, study context, or measurement tools. In addition to exploring the validity of the PICCOLO for children who are late-to-talk, other measures that may be useful in understanding outcomes of interventions for this population, beyond language outcomes, include: the Communication and Symbolic Behavior Scales (CSBS-DP; Wetherby and Prizant, 2002) for addressing child-specific communication skills prior to 24 months, the Emotional Availability Scales (EAS; Biringen et al., 1998) for measurement of both child and parent constructs, and the Early Childhood Home Observation Measurement of the Environment (EC-HOME; Caldwell and Bradley, 1984) for evaluating the dyadic relationship. The Target Word program provides opportunities for clinicians to observe important behaviors thus providing an important opportunity for meaningful feedback for families. In addition to the importance of measuring parent–child interactions from a clinical perspective, families also see observation as a critical way for interventionists to observe their interactions with their child and appreciate that it could provide meaningful opportunities to strategize ways to support their child's learning and development (Keilty et al., 2022). Therefore, a measure that combines evaluation of the parent–child interaction with satisfaction of the parent's experience participating in programs similar to Target Word may be the most useful way to explore outcomes and support overall family wellbeing. In this regard, it may be beneficial to develop and validate a program-specific parent–child interaction measurement tools that focus on the specific skills that are taught in the program to facilitate both feedback and measurement.
In conclusion, while some significant within-group changes in parent–child interactions were found, they were not observed with any predictable pattern, and between-group differences were not statistically significant at any point. These results made it difficult to attribute any changes in parent–child interactions to the virtual Target Word program. As described above, these findings highlight the need to further investigate the nature of parent–child interactions in children who are late-to-talk. Unpacking the relations between parent–child interaction and language skills would lead to more effective supports for children who are late-to-talk and their families. Until there is additional evidence, it is important to stress that clinicians should continue to provide supports surrounding parent–child interaction quality to ensure families have resources and feel supported, particularly considering the additional stressors regarding child development reported by families of children who are late-to-talk (Desmarais et al., 2008).
Footnotes
Declaration of conflicting interests
Cindy Earle is the former Program Director for the Target Word Program. She was not involved in study design, or data analysis/interpretation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this articple: This work was supported by the Ontario Ministry of Research and Innovation (grant number Early Researcher Award (ER16-12-144)).