
Abstract
Syphilis, a resurgent sexually transmitted infection caused by Treponema pallidum, poses significant public health challenges globally. Its varied clinical presentations, especially oral manifestations, position dental professionals uniquely for early detection and intervention. This review synthesizes current epidemiological trends, clinical features, diagnostic approaches, prevention strategies, and management guidelines with an emphasis on the role of dental professionals. A literature review was conducted to assess the clinical presentation of syphilis, prevention and management by dental professionals. Key topics included epidemiology, risk factors, transmission, diagnosis and treatment. A systematic search was conducted across PubMed, Ovid MEDLINE, EMBASE, Scopus, and Google Scholar for studies published in English from 2010 to 2024, supplemented by public health and media reports. A notable increase in syphilis cases was reported globally, including Canada and the United States, with disproportionate impacts on vulnerable populations. Oral lesions, including chancres and mucosal patches, frequently present in early stages, underscoring the importance of dental examination. Rapid point-of-care testing offers opportunities for timely diagnosis in dental settings. Prevention relies on education, routine screening, and structural interventions, while management centres on penicillin-based treatment and coordinated referrals. Dental professionals can play a critical role in mitigating syphilis transmission through early identification, patient education, and referral. Strengthening interdisciplinary collaboration and provider training is essential for improving syphilis outcomes and population health.
Keywords
Introduction
Syphilis is a sexually transmitted infection (STI) caused by the bacterium Treponema Pallidum (Smith et al., 2021). It is known as the “great imitator” since its signs, symptoms, and even histopathological characteristics look like many other diseases (Tudor et al., 2024). Globally, syphilis prevalence has been increasing, with a 60% increase from 1990 to 2019 (Chen et al., 2023). In North America, Canada experienced a 109% rise in syphilis cases between 2018 and 2022, while the United States reported a 79% increase during the same period (Global Biodefense, 2024; Public Health Agency of Canada, 2024a). This growing incidence represents a significant public health concern. Syphilis progresses through primary, secondary, latent, and tertiary stages, with the possibility of oral lesions appearing at any of the stages except the latent phase, which lacks clinical manifestations (Smith et al., 2021). Despite being a treatable condition (Public Health Agency of Canada, 2024b), syphilis is often asymptomatic. When symptoms do occur, individuals may not seek care, and even if they do, it is sometimes misdiagnosed resulting in delays in diagnosis, continued transmission, and potential complications.
An overlooked point of contact with the health care system in the diagnosis of syphilis is dental clinics. Dental professionals represent a largely underutilized but critical point of contact for syphilis detection. Oral manifestations occur in up to 12% of syphilis cases (Smith et al., 2021), positioning dental professionals as key frontline providers capable of recognizing suspicious lesions, initiating timely referrals, and supporting STI prevention efforts, especially among high-risk populations. With the expansion of the Canadian Dental Care Plan, a federal program for low- and middle-income Canadians (Government of Canada, 2025), more individuals are expected to receive routine oral health services. This expansion provides an important opportunity to incorporate syphilis screening and awareness within dental practices, aligning oral health care with broader public health goals.
The aim of this narrative review is to examine the role of dental professionals in the early recognition, prevention, and management of syphilis. By synthesizing current evidence on epidemiology, transmission, risk factors, and oral manifestations, this review highlights how dental settings can serve as important points of detection and referral. In doing so, it emphasizes the opportunity to align routine dental care with broader public health initiatives, particularly within the expanding landscape of publicly funded dental services in Canada.
Methodology
This narrative review followed a structured approach to identify and synthesize literature. A comprehensive search of the medical and dental literature in the English language was conducted across the following electronic databases: PubMed, Ovid MEDLINE, EMBASE, Scopus, and Google Scholar. In addition, grey literature, including relevant reports from governmental and non-governmental organizations, as well as media sources, were reviewed to capture broader public health perspectives and emerging evidence. Five reviewers (MA, AZ, AG, RD, and TB) independently used Boolean operators to combine search terms and screen titles and abstracts for relevance. Keywords included: “syphilis,” “oral syphilis,” “Treponema pallidum,” “sexually transmitted infections,” “dentistry,” “oral health,” “Canada,” “diagnosis,” and “transmission.” Any conflicts and uncertainties related to study selection were resolved through discussion among reviewers.
The search was restricted to publications from January 2010 to June 2025 to ensure relevance to current clinical and public health contexts. Eligible studies included primary research articles, reviews, case reports and policy documents addressing any aspect of syphilis relevant to dental practice or oral health. Reference lists of the included sources were manually searched to identify additional sources not captured in the database search. In addition to dental-specific content, broader background information on syphilis was included to provide a comprehensive and accessible overview for dental professionals. As this is a narrative review, no formal quality assessment tools were applied to evaluate the included studies. The review aimed to provide an overarching synthesis of the available literature, rather than assess the methodological rigor of each study.
Results
In total, 39 research articles and reports were included in this review. The findings of this review are organized into four key areas: (1) syphilis as a public health concern and its epidemiology; (2) detection and diagnosis, including oral manifestations across stages and congenital syphilis; (3) transmission and prevention, with emphasis on the role of dental professionals in education and risk mitigation; and (4) management of syphilis, including treatment protocols and follow-up care to ensure optimal outcomes.
Epidemiology of syphilis
In 2022, the World Health Organization (WHO) estimated that 8 million adults aged 15–49 acquired syphilis globally (World Health Organization, 2025). Among them were pregnant women, whose untreated infections led to an estimated 700,000 cases of congenital syphilis (World Health Organization, 2025), a serious but preventable condition. Figure 1 illustrates the number of infectious and congenital syphilis cases in Canada, the United States, the United Kingdom, and Australia in 2022. Number of infectious and congenital syphilis cases, in 2022, across Canada, the USA, the United Kingdom and Australia (Australian Government, 2023; Global Biodefence, 2024; Public Health agency of Canada, 2024a; UK Health Security Agency, 2024).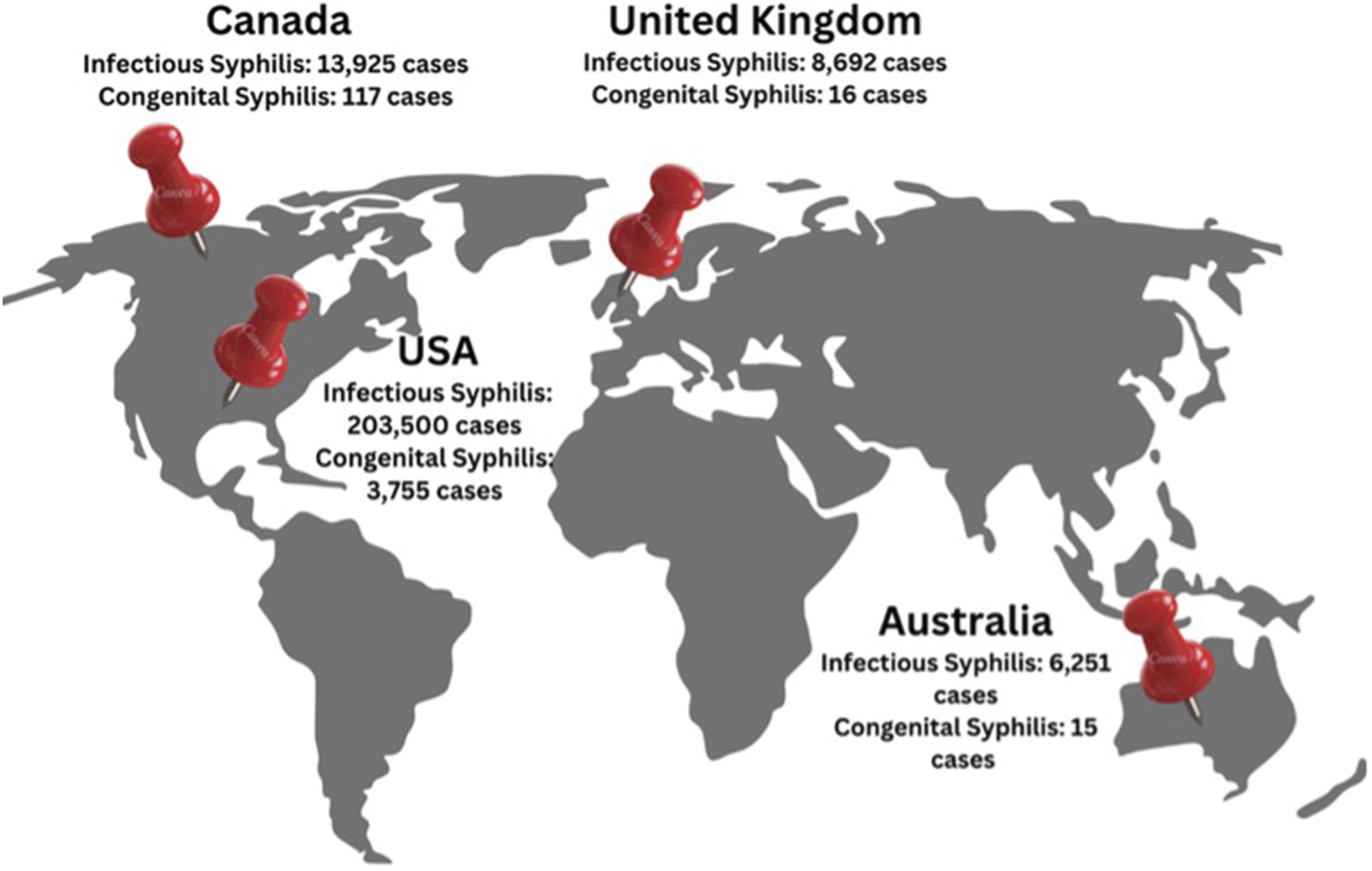
In Canada, syphilis has been a nationally notifiable disease since 1924. Reported case rates were historically high until the 1940s, after which they declined steadily through the 1990s. A resurgence began in the early 2000s and accelerated significantly after 2017 (Aho et al., 2022; Public Health Agency of Canada, 2020). The United States, where syphilis became notifiable in 1944, has followed a similar trajectory, with reported cases beginning to rise again around 2000 and increasing sharply after 2016 (Centers for Disease Control and Prevention, 2024). As illustrated in Figure 2, syphilis rates in both countries have now surpassed levels recorded in the late 1970s. Syphilis is currently the third most commonly reported notifiable STI in Canada, following chlamydia and gonorrhea (Public Health Agency of Canada, 2024b). Rate of reported cases of syphilis per 100,000 population in Canada and the United States (Aho et al., 2022; Centers for Disease Control and Prevention, 2024; Public Health Agency of Canada, 2020).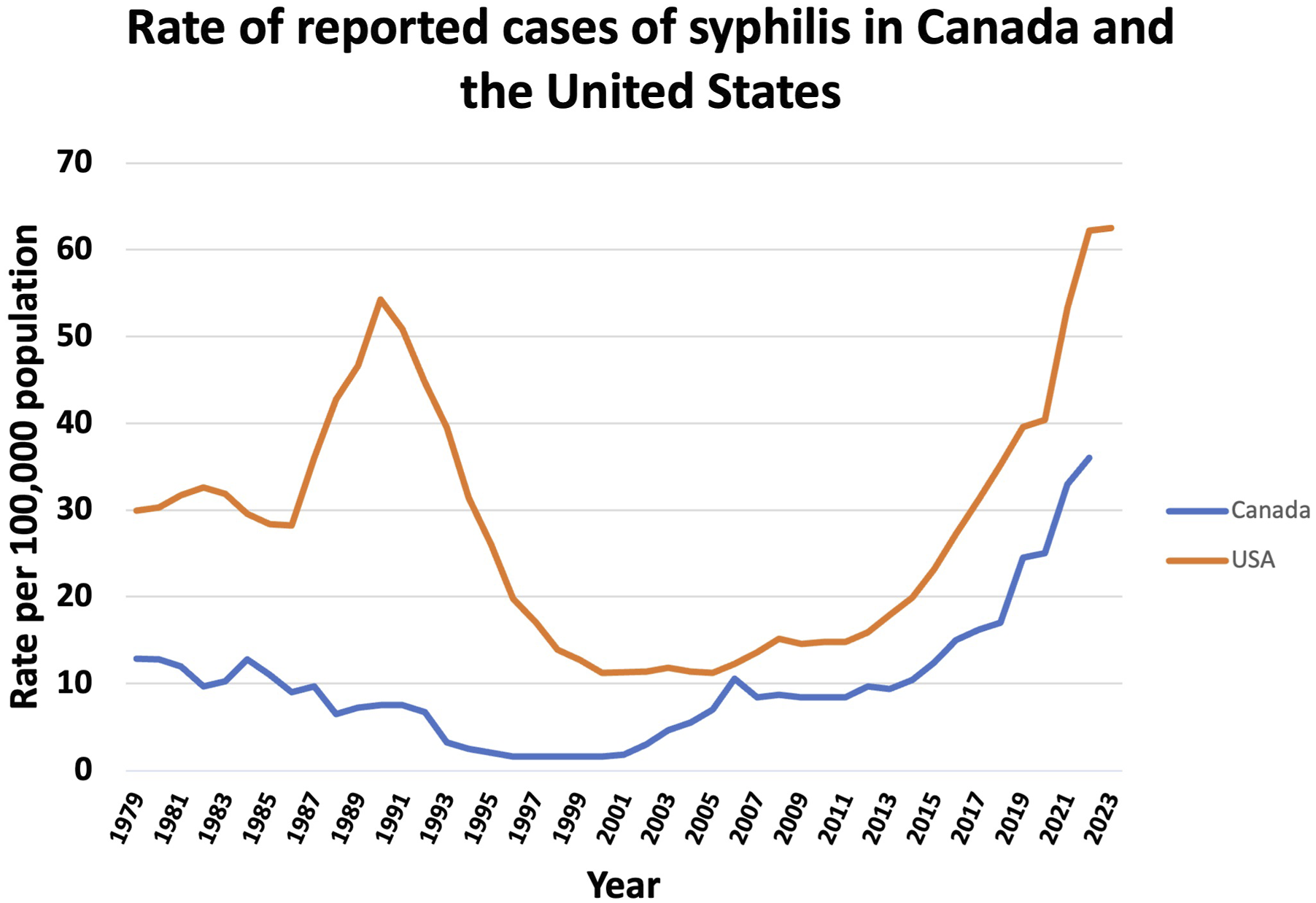
In both Canada and the U.S., the increase in syphilis has been especially pronounced among females of reproductive age (15–39 years), contributing to a parallel rise in congenital syphilis. In Canada, syphilis rates among women in this age group were 256% higher in 2022 than in 2018 (Public Health Agency of Canada, 2024a). Although the U.S. does not report rates by this specific age group, it has recorded a 111% increase in syphilis cases among females since 2019 (Centers for Disease Control and Prevention, 2024). As a result, congenital syphilis has surged. In 2022, Canada recorded 246 cases—up 7% from the previous year and a staggering 599% increase from 2018. Of these, 117 were classified as early congenital syphilis (Public Health Agency of Canada, 2024a). The United States reported 3755 congenital syphilis cases in the same year, reflecting a 31% year-over-year increase and a 183% rise since 2018 (Global Biodefense, 2024).
Indigenous communities in Canada face further higher rates of syphilis compared to non-Indigenous populations. Between 2017 and 2021, syphilis infection rates among First Nations people were 13 times higher than the national average (Native Women’s Association of Canada, 2025). While the exact reason remains uncertain, this disproportionate burden is likely influenced by multiple intersecting factors, including limited access to healthcare, poverty, unstable housing, stigma, and intergenerational trauma. The COVID-19 pandemic further disrupted screening and care efforts (Global News, 2022). Mistrust in the healthcare system remains a significant barrier to timely diagnosis and treatment, underscoring the importance of culturally safe, community-driven interventions. In 2022, the province of Saskatchewan, with 17% of the population being Indigenous, reported the highest rate of infectious syphilis per 100,000 population (Figure 3). Over the past 5 years, cases have risen dramatically in the province, prompting public health officials to declare a syphilis epidemic (Global News, 2022). Number of infectious cases of syphilis and rate of syphilis per 100,000 population across the Canadian provinces and territories, in 2022 (Public Health Agency of Canada, 2024a).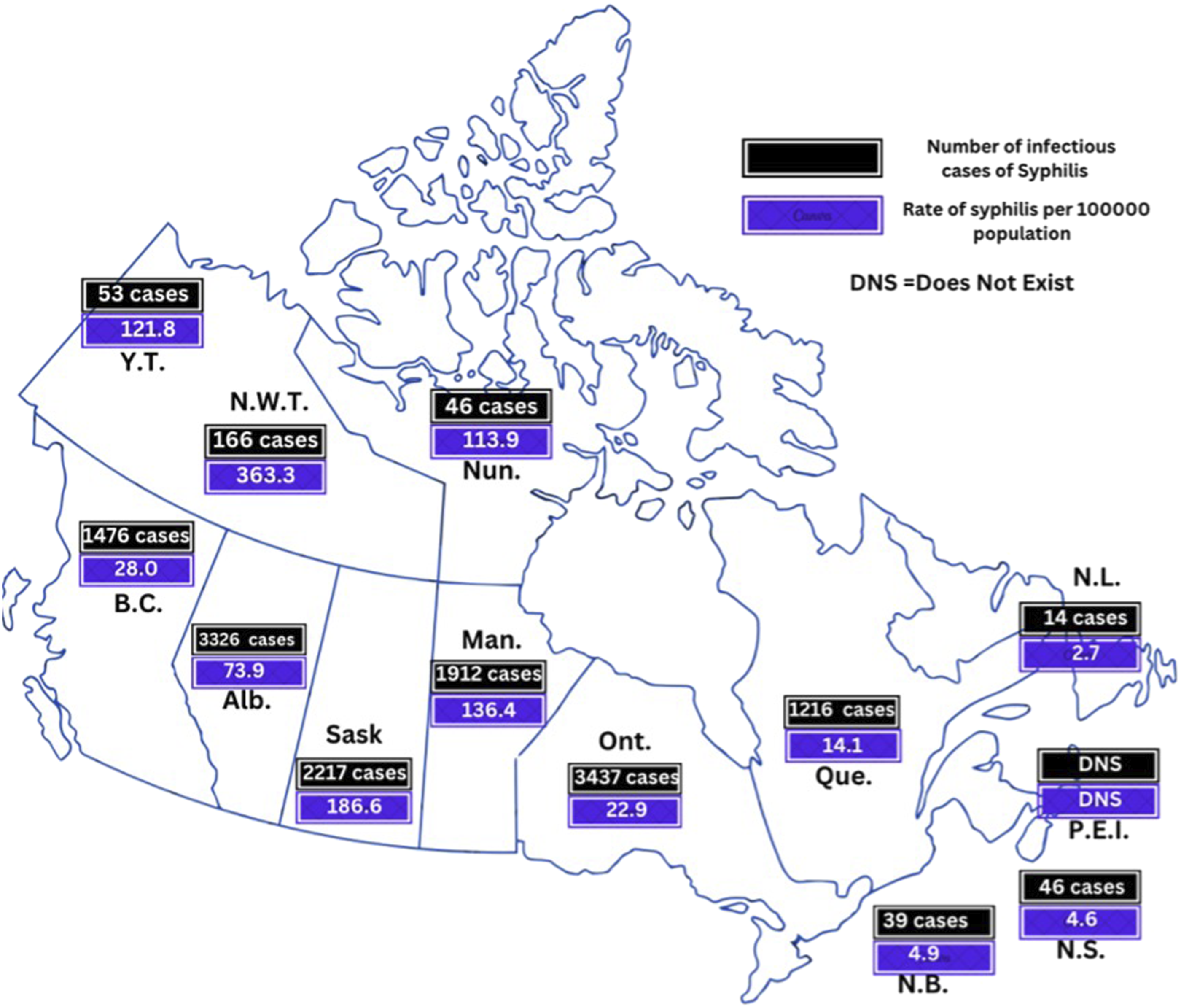
Detection of syphilis
Signs and symptoms
Syphilis presents with a wide range of clinical manifestations that vary in location, duration, and severity depending on the mode of transmission and stage of disease. It may be either acquired or congenital, with the latter resulting from transplacental transmission. Many cases remain asymptomatic and are only detected through serologic testing (Begum et al., 2024). In symptomatic individuals, clinical features are stage-dependent and guide both diagnosis and management. Syphilis progresses through four stages, outlined in Figure 4, each associated with distinct systemic and oral features. This review focuses on oral manifestations relevant to dental professionals. Stages of syphilis.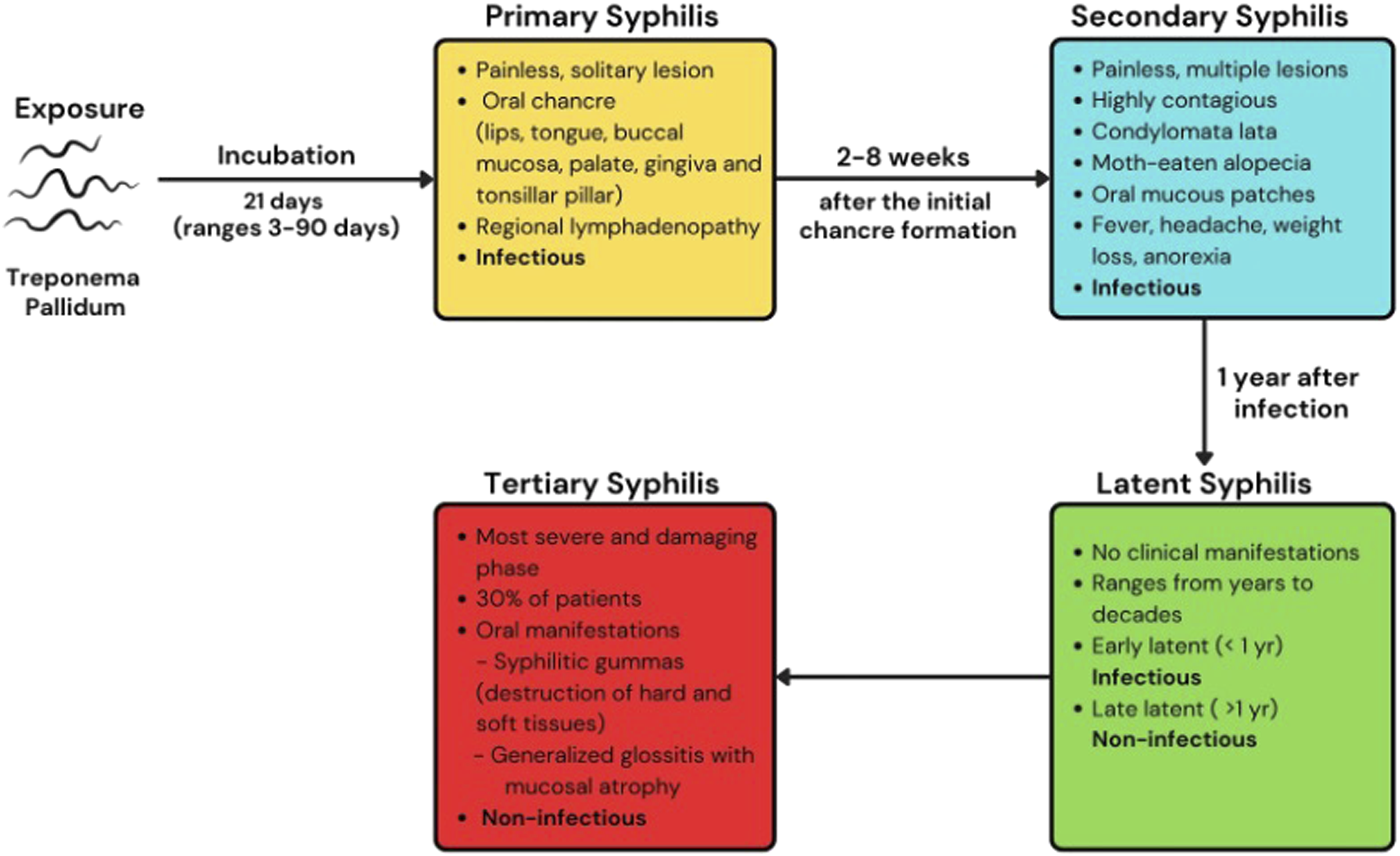
Primary stage
The primary stage, also known as the chancre stage, typically begins around 21 days (range: 3 to 90 days) after exposure to Treponema pallidum (Public Health Agency of Canada, 2024b). It is characterized by the appearance of a small, solitary, painless papule at the site of inoculation. This lesion later ulcerates to form a chancre—a firm, non-suppurative ulcer with raised, indurated borders (Smith et al., 2021).
Given that the chancre arises at the point of bacterial entry, the genital mucosa is most frequently affected, 40–75% of extra-genital lesions occur in the oral region, and approximately 4–12% of primary syphilis cases present with oral chancres (Smith et al., 2021). Common intraoral sites include the lips, tongue, buccal mucosa, gingiva, hard palate, and tonsillar pillars (Figure 5). Regional lymphadenopathy may also occur and can be tender or non-tender. Oral manifestations of primary syphilis, “oral chancre” (Jones et al., 2012; Ramoni et al., 2009; Smith et al., 2021).
Even without treatment, chancres typically resolve within 3 to 6 weeks (Tudor et al., 2024). However, spontaneous resolution does not indicate eradication of infection. Without treatment, T. pallidum disseminates hematogenously and lymphatically, leading to secondary syphilis. Only 30–40% of patients are diagnosed during the primary stage (Smith et al., 2021).
Secondary stage
In approximately 25% of untreated cases, secondary syphilis develops 2 to 8 weeks after the primary lesion appears (Tudor et al., 2024). This stage is highly infectious and marked by systemic and mucocutaneous involvement.
Patients in this stage may present with multiple painless, contagious lesions, including A) condylomata lata, which are raised, grayish-white papillary lesions that develop in warm, moist areas such as the groin, underarms, and oral cavity; B) moth-eaten alopecia, a form of patchy, non-scarring hair loss; and C) oral mucosal patches, which are painless grayish-white or yellowish ulcers on the lips, tongue, buccal mucosa, and palate (Carbone et al., 2016; Schuch et al., 2019) (Figure 6). Oral manifestations of secondary syphilis (De Paulo et al., 2015; Smith et al., 2021).
Systemic symptoms may include fever, headache, weight loss, myalgia, and anorexia. While symptoms may resolve spontaneously, about 25% of untreated individuals experience recurrence within the first 12 months (Tudor et al., 2024).
Latent stage
Without treatment, the infected individual progresses to the latent phase that can last for years, even decades, and has no clinical manifestations, relying on serological testing for diagnosis. Early latent syphilis (within 1 year of infection) is infectious, while late latent syphilis (more than 1 year) is not. In this stage, there are typically no outward signs or symptoms, including in the oral cavity.
Tertiary stage
Tertiary syphilis is the most severe and damaging phase, which occurs in approximately 30% of patients (Smith et al., 2021). It includes cardiovascular syphilis, gummatous syphilis, and neurosyphilis forms. Symptoms might appear months, years, or even decades after the initial infection. Oral syphilitic gummas are large, irregular ulcers with a necrotic base, often leading to significant destruction of both hard and soft tissues, sometimes causing palatal perforation (Mulder Van Staden et al., 2022) (Figure 7). Less common oral symptoms may include generalized glossitis with mucosal atrophy (Mulder Van Staden et al., 2022). Oral manifestations of tertiary syphilis, “oral gumma” (Jones et al., 2012; Sharma and Sharma 2016; Titinchi et al., 2020).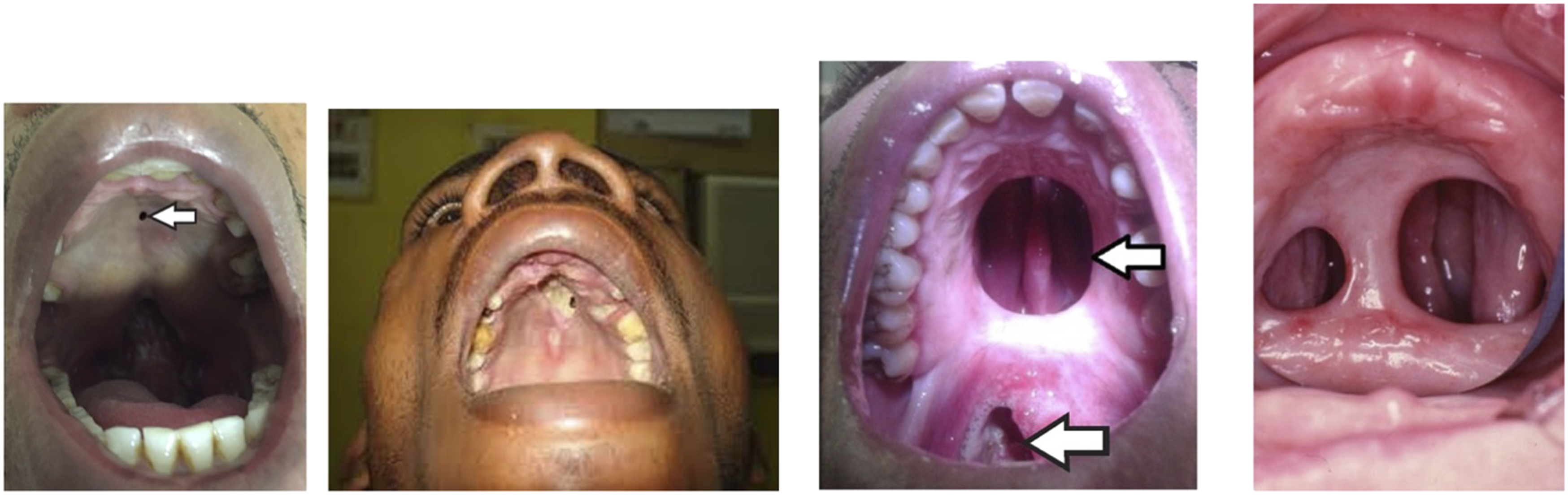
Congenital syphilis
When syphilis is transmitted from a pregnant woman to her fetus, the child develops “congenital syphilis.” The likelihood of vertical transmission of syphilis depends on the stage of maternal infection, with the risk exceeding 70% in cases of untreated primary or secondary syphilis during pregnancy (Canadian Paediatric Society, 2024). Consequences include stillbirth, neonatal death, premature birth and low birth weight.
Early congenital syphilis typically presents within the first 2 years of life and may cause rhagades, radial scarring around the mouth, atrophic glossitis, yellow discoloration of the lips, and a high-narrow palatal vault (Leão et al., 2006; Mulder Van Staden et al., 2022). If symptoms appear after 2 years, it is classified as late congenital syphilis. It is rare because most of affected infants do not survive beyond the first few weeks of life. Hutchinson’s triad may be present: interstitial keratitis, eighth nerve deafness, and Hutchinson’s teeth (Pessoa and Galvão, 2011) (Figure 8). Dental defects, such as peg-shaped incisors and malformed first molars, become apparent with the eruption of permanent teeth. These defects are caused by an inflammatory reaction from Treponema pallidum that inhibits ameloblasts. Other manifestations include premature loss of primary teeth and palatal perforation. Interstitial keratitis can result in visual impairment or blindness, while eighth nerve deafness typically begins with high-frequency hearing loss between 8 and 10 years of age (Pessoa and Galvão, 2011). Hutchinson’s teeth, congenital syphilis (Healthline, 2019; Medeiros et al., 2023; Pessoa and Galvão, 2011).
Diagnosis of syphilis
Syphilis testing is recommended for individuals presenting with signs or symptoms of infection, as well as asymptomatic individuals at an elevated risk of acquiring or transmitting the disease. Diagnosis relies primarily on serologic testing, which is typically conducted using two types of tests—non-treponemal and treponemal assays. Interpretation can be complex, and diagnosis should not be based on a single test result (Public Health Agency of Canada, 2024b). Testing algorithms may vary across jurisdictions in Canada, with provinces and territories employing different approaches depending on available resources and public health strategies (Public Health Agency of Canada, 2024b).
Rapid tests offer a timely and accessible alternative to standard laboratory-based diagnostics, which can take 48 hours or more for results. These tests typically use a small amount of blood obtained via fingerstick and can deliver results in as little as 60 seconds to 15 minutes, depending on the device. Rapid testing allows for same-visit clinical decision-making, including patient counselling and initiation of treatment (Tudor et al., 2024). Rapid tests are especially valuable in community-based and resource-limited settings (Clark and Grobelna, 2022). Some multiplex rapid tests can also detect HIV antibodies, enabling simultaneous screening for co-infections. This integration is particularly beneficial for outreach programs and populations with limited access to laboratory services (BioLytical Laboratories Inc., 2025). Moreover, rapid testing helps reduce loss to follow-up, which remains a major barrier to syphilis care. By improving immediate linkage to care, these tests support public health goals of preventing onward transmission and reducing congenital syphilis cases (Clark and Grobelna, 2022).
It is important to distinguish between point-of-care tests (POCT) and over the counter (OTC) self-tests. POCTs are conducted by trained health care providers in clinical or community settings, such as dental clinics, outreach programs or mobile testing units. These tests allow immediate counselling, linkage to confirmatory testing and prompt referral or treatment withing the same setting. In contrast, OTC self-tests are designed for individual use without professional supervision and rely on self-collection and interpretation of results. Positive OTC must be followed by confirmatory laboratory testing (World Health Organization, 2024).
In Canada, Health Canada has approved only two rapid POCT for syphilis: the INSTI® Multiplex HIV-1/HIV-2/Syphilis Antibody Test (approved in 2023) and Multiplo® TP/HIV Test (approved in December 2024) (BioLytical Laboratories Inc., 2025; MedMira Inc., 2025). Both are approved for use by trained health care professionals only. In the United States, the FDA approved the Syphilis Health Check in 2014 and the DPP® HIV-syphilis system in 2020 (VedaLab., 2024; U.S. Food and Drug Administration 2023a). These POCT are also intended for use by trained professionals. Notably, in August 2024, the FDA approved the first OTC at-home syphilis test, First To Know®, which can be self-administered at home and delivers results in only 15 minutes. It is available for purchase online, offering a discreet, convenient option for individuals who may face barriers to clinical testing (U.S. Food and Drug Administration, 2023b). However, positive results will require confirmatory testing and linkage to care.
Transmission of syphilis
Syphilis is primarily transmitted through direct contact with an infectious lesion, most commonly during sexual activity. Vertical transmission from an infected mother to her fetus can also occur via the placenta during pregnancy, leading to congenital syphilis—a serious and preventable outcome. Although rare, non-sexual transmission may occur through skin contact with infectious sores, needle sharing, blood transfusions, or accidental inoculation, such as needlestick injuries (Manitoba Public Health Branch, 2024; Public Health Agency of Canada, 2024b).
Dental professionals may be at occupational risk through contact with syphilitic chancres, blood, or saliva, particularly if infection control practices are inadequate (Mulder Van Staden et al., 2022). While the risk of transmission from needlestick injuries is low, it depends on factors such as the injury’s severity, the stage of the source patient’s infection, and the presence of fresh blood in the needle (Bowden, 2001). Notably, blood contamination is found in up to 39% of needle lumens following local anesthetic injections, reinforcing the need for safe injection and disposal protocols (Kotze and Labuschagne, 2014).
Prevention of syphilis
There is currently no vaccine for syphilis. Vaccine development is challenging due to the need for cross-strain protection, durable immunity, and safety across diverse populations, including pregnant individuals and people with HIV. Despite these hurdles, a vaccine remains a critical goal for long-term disease control (Cameron, 2018).
Syphilis risk is shaped by a combination of behavioural, epidemiological, and structural factors. Behavioural risk factors include unprotected sex, multiple sexual partners, men who have sex with men (MSM), and contact with known cases or other sexually transmitted and blood-borne infections (STBBIs). Epidemiological risks include previous syphilis or STBBIs, HIV infection, residence in high-prevalence areas, homelessness, limited prenatal care, and poor socioeconomic conditions (Public Health Agency of Canada, 2024b).
Structural determinants such as limited access to healthcare, lower education levels, and poverty also play a significant role in syphilis transmission. For instance, congenital syphilis often results from inadequate or absent prenatal care, underscoring the importance of routine antenatal screening, especially in high-risk populations (Macêdo et al., 2017; Tetteh and Moore, 2025).
In clinical and dental settings, administering local anesthesia is the leading cause of needlestick injuries, followed by the improper disposal of needles (Gaballah et al., 2012). Preventing occupational exposure requires comprehensive training on the safe handling of sharps, the use of safety-engineered devices, and access to effective disposal systems. Ongoing staff education, surveillance, and prompt reporting of incidents are also essential to mitigate risk (Canadian Centre for Occupational Health and Safety, 2024).
In the event of a needlestick injury, healthcare providers should immediately halt the procedure, remove gloves, and wash the affected area thoroughly with soap and water. If the eyes or oral mucosa are exposed, the area should be flushed with running water (Canadian Centre for Occupational Health and Safety, 2024). Every reasonable effort should be made to obtain the patient’s informed consent for testing. Providers are advised to consult with public health authorities, a family physician, or an infectious disease specialist for further counselling and follow-up (Royal College of Dental surgeons of Ontario, 2024). If the patient is known to have syphilis at any stage, a single dose of benzathine penicillin is recommended for post-exposure prophylaxis (Bowden, 2001; Franco et al., 2007).
For patients diagnosed with syphilis, standard precautions are critical to prevent further transmission. The Centers for Disease Control and Prevention (CDC) recommends strict adherence to hand hygiene, appropriate use of personal protective equipment (PPE), and safe injection practices (Centers for Disease Control and Prevention, 2016). Equipment and surfaces that may have been contaminated should be properly sterilized or safely discarded before use with another patient.
Management of syphilis
Penicillin remains the gold standard for the treatment of syphilis, with the therapeutic regimen tailored according to the stage of infection and individual patient factors. Both the Public Health Agency of Canada (PHAC) and the CDC recommend a single intramuscular injection of 2.4 million units of long-acting benzathine penicillin G for the treatment of infectious syphilis, which includes primary, secondary, and early latent stage (Centers for Disease Control and Prevention, 2021b; Public Health Agency of Canada, 2024b). Late latent and tertiary syphilis require three weekly intramuscular injections of the same dosage (Centers for Disease Control and Prevention, 2021b; Public Health Agency of Canada, 2024b). For pregnant and lactating individuals, a single dose of benzathine penicillin G-LA is effective in most cases of early syphilis. Some experts suggest administering two doses, 1 week apart, particularly in the third trimester, to reduce the risk of vertical transmission (Public Health Agency of Canada, 2024b). Patients allergic to penicillin may be treated with doxycycline, tetracycline, ceftriaxone, or azithromycin, though these alternatives are not preferred during pregnancy (Public Health Agency of Canada, 2024b). Management becomes more complex in individuals co-infected with HIV, particularly those with advanced or untreated disease. Close monitoring and strict adherence to antiretroviral therapy are critical in such cases to ensure optimal immune function and treatment efficacy.
Post-treatment follow-up is essential to evaluate treatment response and detect potential reinfection. PHAC guidelines recommend serologic testing at 3, 6, and 12 months for cases of primary, secondary, and early latent syphilis. For late latent and tertiary stages, testing is advised at 12- and 24-month post-treatment (Public Health Agency of Canada, 2024b). Similarly, the CDC recommends that clinical and serologic evaluations should be performed at 6- and 12-month post-treatment for primary, secondary, and early latent syphilis (Centers for Disease Control and Prevention, 2021b). In cases where follow-up may be uncertain or there is concern for reinfection, more frequent evaluations might be warranted. For late latent and tertiary syphilis, serologic tests should be repeated at 6, 12, and 24 months (Centers for Disease Control and Prevention, 2021b).
Given its public health implications, infectious syphilis is a reportable condition across all provinces and territories in Canada, with mandatory notification to PHAC. While non-infectious forms such as late latent and tertiary syphilis may also be reportable, depending on provincial or territorial regulations (Public Health Agency of Canada, 2024b). In the United States, syphilis is nationally notifiable at all stages. Healthcare providers and laboratories are required to report confirmed cases to local or state health departments, which then forward the data to the CDC for national surveillance (Centers for Disease Control and Prevention, 2021a).
Discussion
This discussion highlights the evolving role of dental professionals in the detection, prevention, and management of syphilis—a responsibility that is growing in importance amid rising case rates and the expanding reach of public dental programs such as the CDCP. These findings underscore how dental professionals can play a critical role in advancing public health goals related to STBBIs. Effective integration of detection, prevention and management efforts requires not only clinical awareness but also interprofessional collaboration and supportive policy frameworks.
Detection of syphilis in dental settings
Given that syphilis can present with oral manifestations, including chancres, mucous patches, and gummas, dental professionals are well-positioned to identify early signs of infection, particularly in individuals who may not routinely access medical care. As syphilis becomes increasingly prevalent, oral lesions are more frequently observed in clinical practice, reinforcing the dental provider’s role in early recognition and timely referral. This proactive approach not only benefits individual patients but also contributes to broader efforts to interrupt disease transmission.
Dental professionals often interact with underserved populations, such as those seen in public dental clinics, shelters, and outreach programs. With the expansion of the CDCP, these interactions are likely to increase, further emphasizing the importance of awareness and early intervention. Integration of rapid POCTs into dental settings could enhance early detection, particularly in high-risk populations. However, implementing such innovations requires the careful evaluation of the feasibility, acceptability, and training needs of dental providers in this context (Brondani and Chang, 2014).
In cases of persistent or unexplained oral lesions, biopsy may be used to assist in diagnosis or rule out other conditions (Smith et al., 2021). Although not a primary diagnostic tool for syphilis, biopsy remains a valuable adjunct in complex cases.
Prevention of syphilis through dental practices
Syphilis prevention requires a comprehensive, multidisciplinary approach that includes education, awareness, and behavioural interventions. Dental professionals can contribute by providing educational materials in waiting rooms or operatories, such as pamphlets and posters detailing signs, symptoms, modes of transmission, and the importance of regular testing. These resources support public health messaging and may prompt patients to engage in conversations about sexual health and testing.
Routine screening discussions during medical and dental history intake, particularly with at-risk patients, can also aid in early detection. However, these initiatives are most effective when supported by institutional and policy level action. For example, regulatory bodies can support this effort by updating standard forms to include relevant sexual history questions, thereby normalizing conversations around STBBIs within dental care settings. This policy-level endorsement could help shift the profession’s norms toward more holistic, preventive care models.
Continued professional development is essential. Workshops, seminars, and continuing education modules focused on the oral manifestations of systemic diseases, such as syphilis, can enhance diagnostic accuracy and referral practices. Incorporating interactive formats and collaboration with infectious disease experts can bridge the gap between theory and clinical application, equipping dental teams with the confidence to respond effectively to suspected infections.
As the CDCP increases access to care for underserved populations, the opportunity for targeted prevention also expands. Integrating syphilis education and awareness into dental visits may help reduce disease burden in high-prevalence groups.
Management of syphilis by dental professionals through interprofessional collaboration
While dentists do not treat syphilis directly, they are essential in facilitating access to appropriate care. Establishing referral pathways is critical. Providing dental practitioners with directories of local clinics and infectious disease specialists can streamline the referral process for patients who present with signs suggestive of syphilis.
Clear referral protocols, including documentation templates and communication guidelines, can help standardize the process across practices and ensure consistency in care transitions as well as prevent patients from being lost in the health care system. Equipping dental professionals with training on how to approach sensitive discussions around sexual health may further enhance patient engagement and reduce stigma. Interprofessional collaboration is central to this model. Collaborative training sessions and shared electronic health records could strengthen the process and improve outcomes.
Follow-up after referral is another important component of care. Dentists should encourage patients to seek medical evaluation and, where appropriate, monitor the resolution of any oral manifestations. This reinforces a patient-centred, integrated approach to care that supports both oral and systemic health.
Collectively, efforts to enhance the detection, prevention, and management of syphilis in dental settings highlight the significant role that dental professionals can play in public health surveillance and response. The integration of these domains, supported by training, policy, and interprofessional collaboration, has the potential to position dental practice as an active partner in infectious disease control. Realizing this potential will require future research to explore practical models for integrating point-of-care testing and assess provider readiness for implementation. Ultimately, engaging the dental workforce in syphilis detection and prevention aligns with broader health equity goals, including improving access to underserved populations, reducing barriers to care, and strengthening the public health infrastructure through interdisciplinary collaboration.
While this review highlights important opportunities for dental professionals in syphilis detection, prevention, and management, some limitations should be acknowledged. As a narrative review, it may be subject to selection and interpretation bias, and the included evidence varies in scope and quality. In addition, the focus on English-language studies published within the last 15 years might have excluded relevant findings from older or non-English research.
Conclusion
As syphilis rates continue to rise, the role of dental professionals in early detection, prevention, and interprofessional collaboration is increasingly vital. Oral manifestations may be among the first visible signs of infection, positioning dental providers as key contributors to timely diagnosis and referral. With growing access to dental care through initiatives like the CDCP, dental settings are uniquely positioned to engage underserved populations in public health efforts. Incorporating syphilis education, screening awareness, and structured referral protocols into routine dental care can enhance patient outcomes and reduce transmission. Continued professional development and system-level support are essential to empowering dental teams to recognize and respond to syphilis. Future research should evaluate the feasibility of point-of-care testing, assess provider readiness, and explore patient perspectives on discussing sexual health in dental settings. Strengthening the connection between dentistry and public health is critical in addressing this preventable disease and improving health equity across vulnerable communities.
Footnotes
Acknowledgments
We acknowledge the generous support of Green Shield Canada.
Authors contributions
All authors have contributed to the conceptualization, literature search, analysis, writing, and revision of the manuscript. All authors have read and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data in this manuscript are publicly available and have been cited.