
Abstract
Parental differential treatment (PDT) is an important aspect of children’s unique experiences within the family environment, with well-established links to lower-quality sibling relationships. Existing literature often assumes that PDT fosters anger and rivalry. However, the reverse association may also be true, with poor sibling relationships disrupting parental attitudes and behaviors that exacerbate differential parenting. The directionality of the observed relationship is important to address for understanding the internal workings of family dynamics and the particular role of sibling relationships. Thus, the current study explored directional associations between PDT and sibling relationship quality using a longitudinal, repeated-measures design. Data were from an international sample of caregivers (n = 497; 43.46% female) with two children each (n = 994) between the ages of 5–17. Random-intercept cross-lagged panel models examined the longitudinal associations between PDT and sibling relationship quality, while partitioning between- and within-families variance. Irrespective of time, findings suggested that higher overall PDT and differential negativity specifically were related to poorer-quality sibling relationships between families. Furthermore, within families, more differential negativity predicted better sibling relationship quality at a later time point, and poorer sibling relationship quality led to subsequent decreases in differential negativity. Interpreted through the lens of homeostatic effects and feedback loops within family systems, the findings illustrate the dynamic ways in which families achieve stability, in addition to underscoring sibling relationship quality as a potential protective factor against differential parenting.
The family is an important shared developmental context for siblings. Yet, children in the same home often have different experiences (Daniels & Plomin, 1985). One important aspect of these distinct experiences is parental differential treatment (PDT). This occurs when parents and caregivers exhibit differing levels of affection, warmth, sensitivity, and support (i.e., differential positivity) or control, reactivity, harshness, and punishment (i.e., differential negativity) toward siblings (Daniels & Plomin, 1985; Jensen & Thomsen, 2024; Meunier et al., 2012). Since Daniels and Plomin (1985) first brought attention to this issue, PDT has been shown to have implications for not only individual child well-being, but also sibling relational well-being (Meunier et al., 2012). However, robust testing of the magnitude and bidirectionality of this association has yet to be established. Thus, it remains unclear whether sibling relationship quality influences PDT, if PDT affects sibling relationship quality, or if these have bidirectional associations. Moreover, clarifying the extent to which these associations may be attributable to shared family environments is essential for elucidating potential causal effects. Hence, the present study examined longitudinal associations between PDT and sibling relationship quality in a multilevel analytical framework, focusing on both within-family associations and family-wide environmental factors.
Sibling relationships persist across the lifespan, and siblings often spend more time with each other in their childhood and adolescence, compared to any other relationship (Gilligan et al., 2020; Kluger, 2011). Notwithstanding, sibling relationships remain understudied relative to other aspects of family units (Kluger, 2011), and more research is needed to identify the predictors of sibling relationship quality and associated outcomes. Positive sibling relationships—those characterized by kindness, affection, and care—facilitate healthy social and cognitive development by providing early socialization and opportunities for learning skills such as conflict resolution and cooperation (Howe & Recchia, 2014; Jensen et al., 2023; Kramer, 2014; Whiteman et al., 2011). Sibling relationships can further protect against psychosocial risk and mental health challenges (Buist et al., 2013; Davies et al., 2019; Gass et al., 2006). Conversely, strained or conflict-laden sibling relationships predict both internalizing and externalizing behavior in children (Buist et al., 2013; Jensen et al., 2023; Waid et al., 2020). Moreover, the outcomes associated with sibling relationship quality are not isolated to individual children but may interact with other family processes, particularly parenting practices.
PDT is typically conceptualized as either a measure of the direction of differential treatment (i.e., relative PDT) or a measure of the magnitude of differential treatment experienced by siblings (i.e., absolute PDT; Jensen et al., 2013). In this study, we focus on absolute PDT, which captures the magnitude of PDT, allowing for a focus on the family unit as an interconnected system. Meta-analytic evidence suggests that PDT is detrimental to well-being, with links to internalizing and externalizing symptomatology in children and youth (Jensen & Thomsen, 2024; Jiang et al., 2025). Specifically, children from families where siblings face higher levels of PDT display greater internalizing difficulties such as depression and anxiety, as well as externalizing behaviors (e.g., aggression, delinquency, and risk-taking; Jensen & Thomsen, 2024; Jiang et al., 2025). These findings collectively illustrate that PDT is a key family process with important implications for child and youth well-being.
As both sibling relationship quality and PDT are family-based factors linked to psychosocial outcomes, research has focused on understanding their interactions. Previous work has revealed that children who receive unequal treatment from their parents experience poorer quality sibling relationships, characterized by behaviors such as competition and physical aggression, and less affection and support (Brody, 1998; McClellan et al., 2024; Meunier et al., 2012; Shanahan et al., 2008). Parental differential warmth is linked to less positive sibling relationships, while sibling differences in parent-child conflict are related to more sibling conflict (Meunier et al., 2012; Shanahan et al., 2008). Shanahan et al. (2008) observed these links both cross-sectionally and longitudinally. However, this relationship is often assumed to be unidirectional, whereby PDT causally affects sibling relationship quality. In line with the spillover hypothesis, which posits that affect within one relationship in the family system transfers to additional familial relationships (Nelson et al., 2009), greater negativity in one parent-child relationship may transfer to the sibling relationship. For instance, PDT could instill feelings of anger and rivalry among siblings, which manifest as hostile behaviors and ultimately lead to poorer-quality relationships (Ansbacher & Ansbacher, 1956; Brody, 1998; Jensen et al., 2013; Jensen & Thomsen, 2024; McClellan et al., 2024).
However, the observed association between PDT and sibling relationship quality may operate in the reverse direction, such that the quality of the sibling relationship predicts parenting practices and PDT. Previous findings suggest that positive sibling relationships predict more positive parenting styles and later increases in parental support, whereas siblings’ negativity is associated with the opposite (Derkman et al., 2011; Yu & Gamble, 2008). Higher-conflict sibling relationships may spill over into parent-child dyads by disrupting parent-child interactions and fostering parents’ negative attitudes toward at least one of their children (Derkman et al., 2011; Yu & Gamble, 2008). These disruptions and attitudes may, in turn, lessen parental support and affection and increase the differential treatment of siblings (Yu & Gamble, 2008). This literature base affirms the presence of associations between PDT and sibling relationship quality, with some evidence for potential bidirectional and synergistic effects. Indeed, the association between PDT and sibling relationship quality may be understood more clearly through a bidirectional perspective. That is, transactional effects could account for the observed relationship as a product of continuous interactions between PDT and sibling relationship quality. The transactional model theorizes that developmental processes and outcomes depend on the co-shaping of children and their environments over time (Sameroff, 2010). Thus, environmental influences alter childhood development trajectories, which concurrently or subsequently shape those very environments and experiences. In keeping with a transactional framework, PDT may shape children’s relationships with their siblings, which may also predict PDT.
In addition to a need to clarify the strength and direction of associations, it is also possible that the associations between PDT and sibling relationship quality are not causal or directional in nature but emerge as a result of other shared family factors such as genetic influences or shared risks (e.g., socioeconomic vulnerability; psychosocial adversity). Not only do sibling relationships experience strain among families facing adversity, but PDT is more prevalent in these families (Kretschmer & Pike, 2009; Meunier et al., 2013). Given this, it is important to isolate potential family-wide, time-independent influences from temporal mechanisms that are putatively causal (Hamaker et al., 2015), allowing for an understanding of how siblings and multiple parent-child dyads shape each other over time.
The Present Study
Despite literature illustrating associations between PDT and sibling relationship quality, the directionality of this association remains understudied. Addressing this gap is important for understanding potential causal pathways and the extent to which associations operate at within- or between-family levels of analysis. Thus, we explored the longitudinal (bi)directional associations between PDT and sibling relationship quality via random-intercept cross-lagged panel models (RI-CLPMs). We first hypothesized that there would be significant links between PDT and sibling relationship quality at the between-family level of analysis, irrespective of time (H1). That is, families exhibiting higher levels of PDT, on average, will also report lower-quality sibling relationships. We further hypothesized that, within families, higher levels of PDT at previous timepoints will predict lower sibling relationship quality at subsequent timepoints (H2a) and that poorer sibling relationship quality will reciprocally predict higher levels of PDT at the next time point (H2b). If supported, H2 would suggest the presence of transactional processes.
Method
Participants and Procedure
We employed data from the Child Resilience and Managing Pandemic Emotional Distress in Families (CRAMPED Families) Study, an international, longitudinal project that explored family functioning and well-being during the COVID-19 pandemic. Participants were recruited through the Prolific® research panel. Those who previously disclosed to Prolific® that they have children were invited to complete a screening questionnaire of the study inclusion criteria, and those deemed eligible received an invitation to participate. Participants were caregivers over age 18 with at least two children aged 5–17 who resided in the same household. Caregivers completed questionnaires about their own and their family’s well-being, including parenting practices and sibling relationship quality. Child-specific measures were collected for two children in the family—the child closest to (but not younger than) five years old, and the next oldest sibling in the household. Informed consent for the future use of data was collected from caregivers at study baseline.
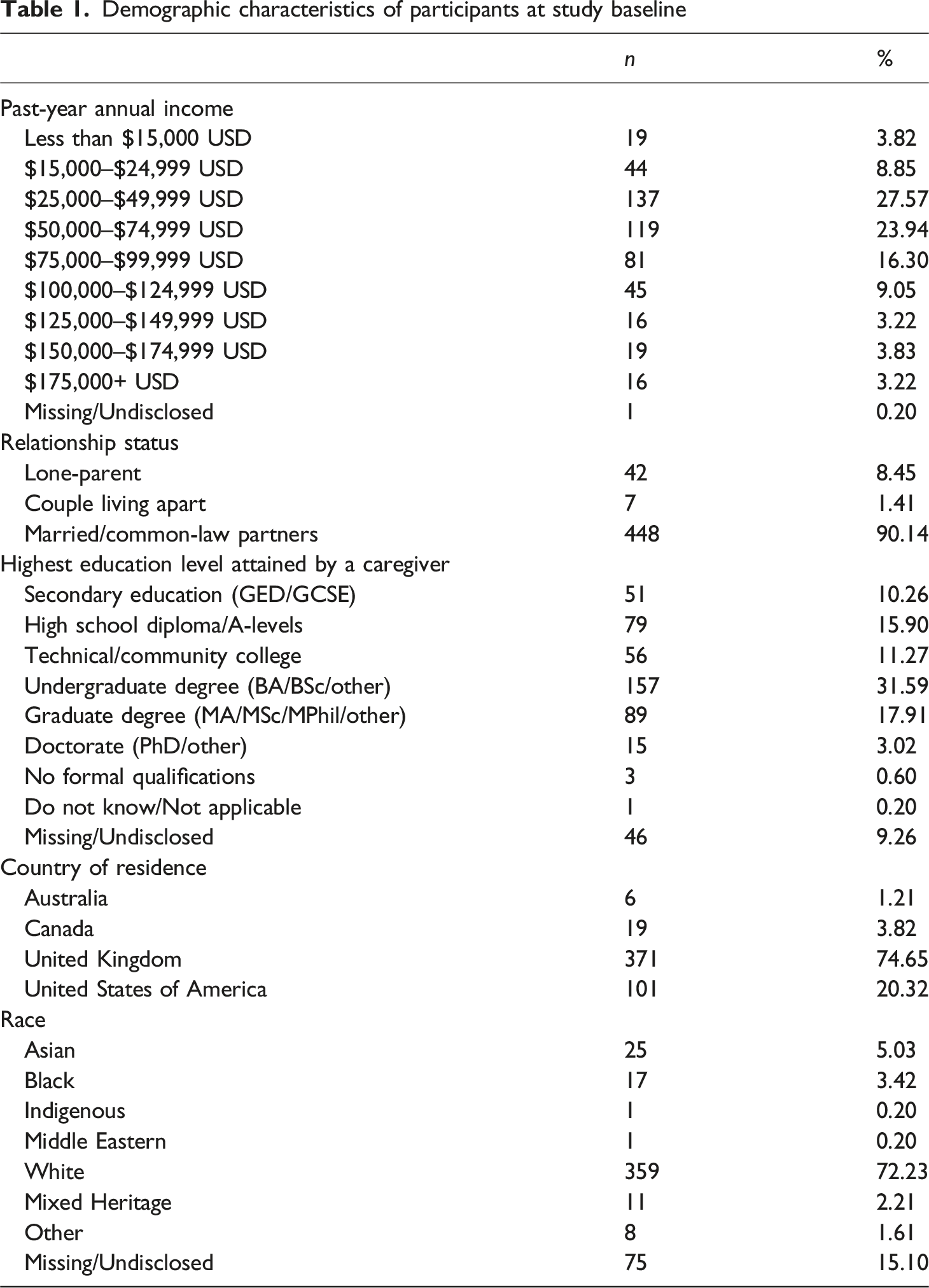
Demographic characteristics of participants at study baseline
Measures
Parental Differential Treatment
Descriptive Statistics of Study Variables
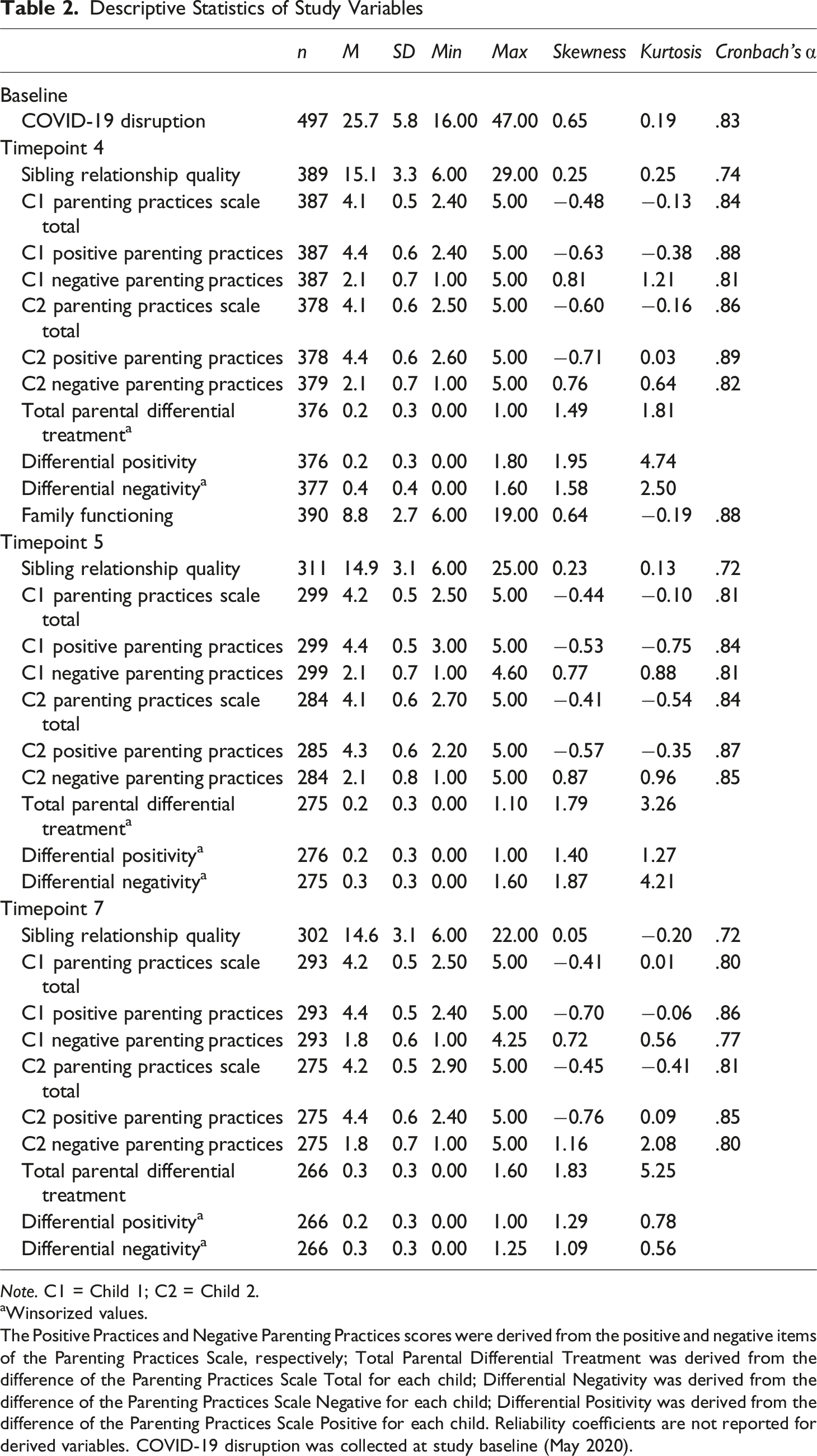
Note. C1 = Child 1; C2 = Child 2.
aWinsorized values.
The Positive Practices and Negative Parenting Practices scores were derived from the positive and negative items of the Parenting Practices Scale, respectively; Total Parental Differential Treatment was derived from the difference of the Parenting Practices Scale Total for each child; Differential Negativity was derived from the difference of the Parenting Practices Scale Negative for each child; Differential Positivity was derived from the difference of the Parenting Practices Scale Positive for each child. Reliability coefficients are not reported for derived variables. COVID-19 disruption was collected at study baseline (May 2020).
Total PDT was operationalized as the absolute difference score between each sibling’s mean total parenting practices score. As such, higher values represented greater degrees of differential treatment toward siblings. In post hoc analyses, absolute difference scores were calculated for each child’s average positive parenting practices and average negative parenting practices. These represented differential positivity (i.e., the extent to which one sibling experienced more positive parenting than the other sibling) and differential negativity (i.e., the extent to which one sibling experienced more negative parenting than the other sibling), respectively.
Sibling Relationship Quality
The sibling relationship quality was assessed over all seven waves of the study and measured using the Parental Expectations and Perceptions of Children’s Sibling Relationships Questionnaire (PEPC-SRQ; Kramer & Baron, 1995). Caregivers reported on six items via a 5-point Likert scale (1 = Never, 5 = Always), which examined how frequently siblings engaged in both positive and negative behaviors with each other over the past two weeks. For example, items included examining how frequently siblings engaged in sharing and physical aggression over the past two weeks. The items assessing positive behaviors were reverse-coded, and all items were summed to create a total sibling relationship quality score, such that higher scores indicated poorer quality. The PEPC-SRQ demonstrates adequate internal consistency (Kramer & Baron, 1995), and several studies have successfully used the questionnaire to measure relationship quality in siblings from several countries and across age ranges (López-Fernández et al., 2022). As shown in Table 2, Cronbach’s α suggested adequate but not excellent internal consistency (Howitt & Cramer, 2007).
Covariates
The covariates included in the model were the caregiver’s age and gender, the sibling age difference, sibling gender composition (dummy coded such that same gender = 1, and different gender = 0), family annual income (at baseline), family functioning, and COVID-19 disruption. These variables were controlled because aspects of the sibling relationship vary based on the sibling age difference and gender composition, particularly in younger generations (Tanskanen & Rotkirch, 2019), and PDT may be exacerbated in adverse settings, including amongst lower socioeconomic status and heightened family stress (Meunier et al., 2013). Family functioning was measured using the six positively-valenced items from the Family Assessment Device General Functioning scale (Epstein et al., 1983), while COVID-19 disruption was measured with 16 items of the COVID-19 Family Stressor Scale (Prime et al., 2021). In particular, the COVID-19 pandemic could influence the relationship between PDT and sibling relationship quality as it introduced unique challenges for parents and families to navigate, including lockdown protocols and school closures. These disruptions are associated with adverse outcomes for the family environment, negatively influencing parenting practices and both parent-child and sibling relationships (Cassinat et al., 2021; Griffith et al., 2022; Menter et al., 2022; Prime et al., 2020).
Statistical Analyses
Data were analyzed using RStudio (version 4.2.2; R Core Team, 2022). Descriptive statistics were calculated, and the distribution of study variables was examined graphically via histograms and boxplots. Non-normality was further evaluated via skewness and kurtosis according to recommended criteria of <2.0 and <7.0, respectively (Niemand & Mai, 2018). Bivariate correlations between study variables were examined for descriptive purposes.
We employed the lavaan R package (Rosseel, 2012) to construct RI-CLPMs (Mulder & Hamaker, 2020) that assessed the associations between PDT and sibling relationship quality over time. The RI-CLPM expands upon the traditional cross-lagged panel model and partitions time-independent variance by creating a stable trait-like component (i.e., a random intercept) from the observed variables at all time points, with the factor loadings fixed to 1. The within-family variables thus represent the difference between the observed measure and the expected score (i.e., the family average) at each time point, respectively, equating to the time-dependent variance. The cross-lagged and autoregressive paths model the time-dependent, within-family variability, or the departures from the family mean at a particular point in time. In other words, it becomes possible to observe if PDT at earlier timepoints predicts later sibling relationship quality, or vice versa, compared to what is typical in each family (i.e., controlling for stable differences).
We initially sought to only examine total PDT in association with sibling relationship quality. However, previous literature has documented that the links between sibling relationship quality and PDT may operate differently across the domains of parental positivity and negativity (Meunier et al., 2013; Shanahan et al., 2008). Understanding these specific aspects could provide more meaningful insights into the specific kinds of parenting practices most closely related to sibling relationship outcomes (Jensen et al., 2013). We therefore conducted post hoc analyses that examined differential positivity and differential negativity in separate models.
We constructed three RI-CLPMs. Model 1, which involves the originally planned analyses to test the study hypotheses, assessed associations between total PDT and sibling relationship quality. Thereafter, we constructed two post-hoc models that decomposed total PDT into differential positivity (Model 2) and differential negativity (Model 3). Model fit was evaluated using the chi-square test, as well as the following fit indices: The Standardized Root Mean Square Residual (SRMR; Byrne, 2001), the comparative fit index (CFI; Byrne, 2001), the Tucker-Lewis Index (TLI; Hu & Bentler, 1999) and the root mean square error of approximation (RMSEA; Hu & Bentler, 1999). Small and statistically non-significant chi-square measures are suggestive of good fit, though this can be impacted by sample size (Tucker & Lewis, 1973). Additionally, for adequate fit, the values of the fit indexes should be as follows: SRMR ≤0.05, CFI ≥0.90, TLI ≥0.95, and RMSEA ≤0.06. Models were estimated with robust maximum likelihood (MLR) estimation, which adjusts the chi-square test statistic and standard errors for non-normality (Lai, 2018).
Missing Data
Of the participants who accessed the survey at baseline (n = 551), n = 54 (9.80%) were removed as they reported on at least one child who was not between the ages of 5 and 17, which was an inclusion criterion to ensure measurement validity. This resulted in a final sample of n = 497. Of the final sample, n = 435 (87.53%) were retained at T4, n = 342 (68.81%) were retained at T5, and n = 336 (67.61%) were retained by T7. Regarding data completion, 86.44% (n = 376) at T4, 80.41% (n = 275) at T5, and 79.17% (n = 266) at T7 provided complete responses to the present study’s variables. Little’s Missing Completely at Random test (Little, 1988) reached statistical significance (χ2(1620) = 2074.72, p < .001), suggesting that missingness in the data was associated with study variables and the missing completely at random assumption was violated. To examine this in more detail, we created binary variables indicating whether participants dropped out at each timepoint included in the study and evaluated the extent to which drop-out was associated with demographic characteristics (caregiver and child age, caregiver and child gender, and family income) via logistic regression models. The results indicated that dropout likelihood was not associated with any of the covariates assessed in the study at T4 or T5. However, older caregivers were less likely to drop out of the study by T7 (OR = 0.92 [95% CI = 0.87–0.98]). Families reporting higher levels of COVID-19 disruption were more likely to drop out at the final time point as well (OR = 1.08 [95% CI = 1.02–1.14]). Independent samples t-tests showed that participants who dropped out at T4 reported slightly higher levels of positive parenting toward the older sibling in the study (t(375) = −20.50, p < .001). Given these results, all models were estimated using full information maximum likelihood with covariates added as auxiliary variables to account for missingness bias (Enders & Bandalos, 2001).
Results
Descriptive Statistics
Bivariate Correlations Between Model Variables
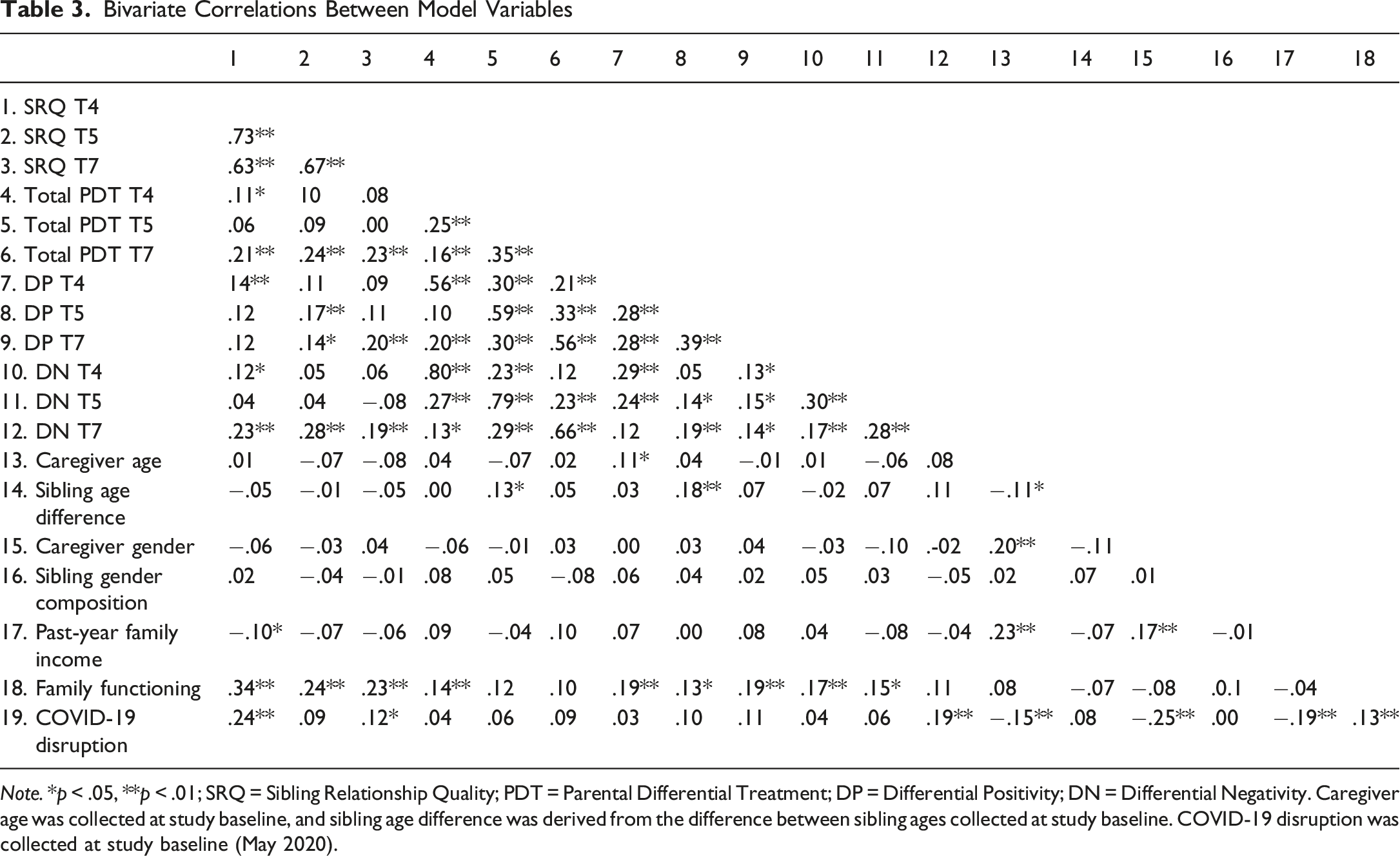
Note. *p < .05, **p < .01; SRQ = Sibling Relationship Quality; PDT = Parental Differential Treatment; DP = Differential Positivity; DN = Differential Negativity. Caregiver age was collected at study baseline, and sibling age difference was derived from the difference between sibling ages collected at study baseline. COVID-19 disruption was collected at study baseline (May 2020).
Random-Intercept Cross-Lagged Panel Models
Total PDT and Sibling Relationship Quality
Model 1 examined the links between overall PDT and sibling relationship quality. Fit indices suggested that the model was a good fit to the data: χ2(33) = 47.21, p = .052; CFI = .97, TLI = 0.95, RMSEA = 0.03 [90% CI = 0.004–0.05], SRMR = 0.03. The full model is graphically depicted in Figure 1. As hypothesized (H1), at the between-family level, there was a significant positive association between PDT and sibling relationship quality, whereby greater PDT was associated with poorer sibling relationship quality (σ2 = .73, p = .020). The within-families covariances were not significant, suggesting PDT and sibling relationship quality were not associated within timepoints once accounting for stable time-independent variance. Longitudinally, lower sibling relationship quality at T4 predicted ongoing lower quality at T5 (β = .40, p = .007). Higher PDT at T5 was also associated with higher PDT at T7 (β = .28, p = .036). Model 1 suggested the potential presence of a transactional association, though the observed pattern ran counter to Hypothesis 2. The association between lower-quality sibling relationships at T4 and PDT at T5 approached statistical significance (β = −.24, p = .058), and from T5 to T7, higher PDT was associated with better parent-reported sibling relationship quality (β = −.29, p = .018). Time-invariant covariates were regressed onto the between-families component of the model. These indicated that higher family dysfunction was associated with poorer sibling relationship quality (β = .38, p <.001) and greater parental differential treatment (β = .35, p = .002). COVID-19-related disruption was also associated with lower-quality sibling relationships (β = .18, p = .002). RI-CLPM of sibling relationship quality and total parental differential treatment. Note. *p < .05, **p < .01; Solid lines indicate statistically significant associations, while dashed lines indicate insignificant associations. PDT = Parental differential treatment; SRQ = Sibling relationship quality; parameters starting with “b” refer to the between-families variance components, and parameters starting with “w” refer to variance at the within-family level.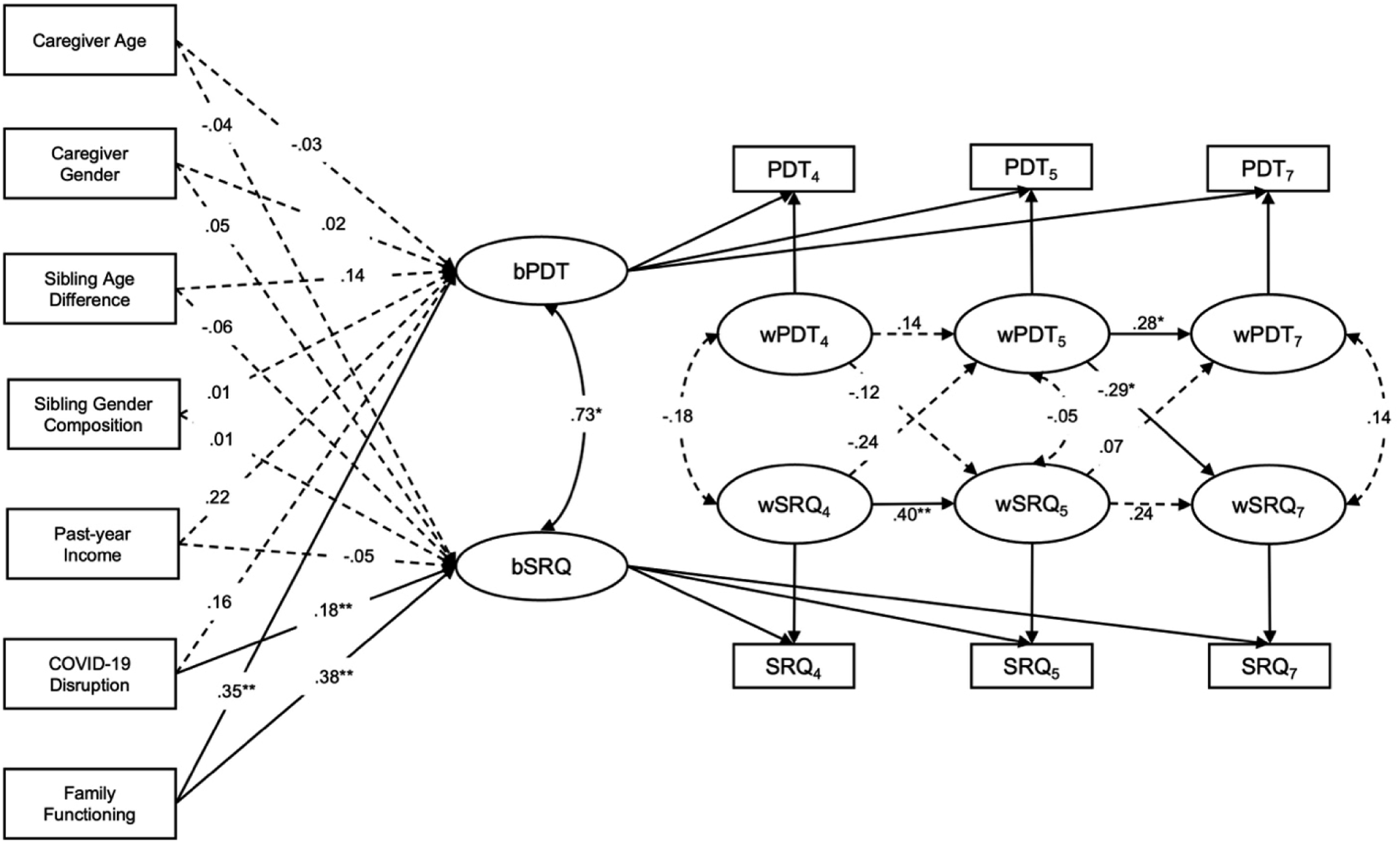
Differential Positivity and Sibling Relationship Quality
We further conducted post-hoc analyses to examine whether specific aspects of differential parenting may be associated with sibling relationship quality over time. Model 2, the differential positivity model, showed good fit to the data: χ2(33) = 44.89, p = .081; CFI = .98, TLI = 0.96, RMSEA = 0.03 [90% CI = 0.00–0.045], SRMR = 0.03. As shown in Figure 2, no significant covariances emerged at the within- or between-family levels of analysis. Sibling relationship quality at T4 positively predicted sibling relationship quality at T5 (β = .34, p = .025). There were no other significant autoregressive effects, nor any significant cross-lagged associations in Model 2. Of the time-invariant covariates, greater sibling age difference (β = .21, p = .029) and family functioning challenges (β = .37, p < .001) were associated with higher differential positivity, and the effect of COVID-19 disruption (β = .17, p = .050) neared significance. Higher COVID-19 disruption (β = .18, p = .001) and family functioning difficulties (β = .36, p < .001) were also associated with lower-quality sibling relationships. RI-CLPM of sibling relationship quality and differential positivity. Note. *p < .05, **p < .01; Solid lines indicate statistically significant associations, while dashed lines indicate insignificant associations. DP = Differential positivity; SRQ = Sibling relationship quality; parameters starting with “b” refer to the between-families variance components, and parameters starting with “w” refer to variance at the within-family level.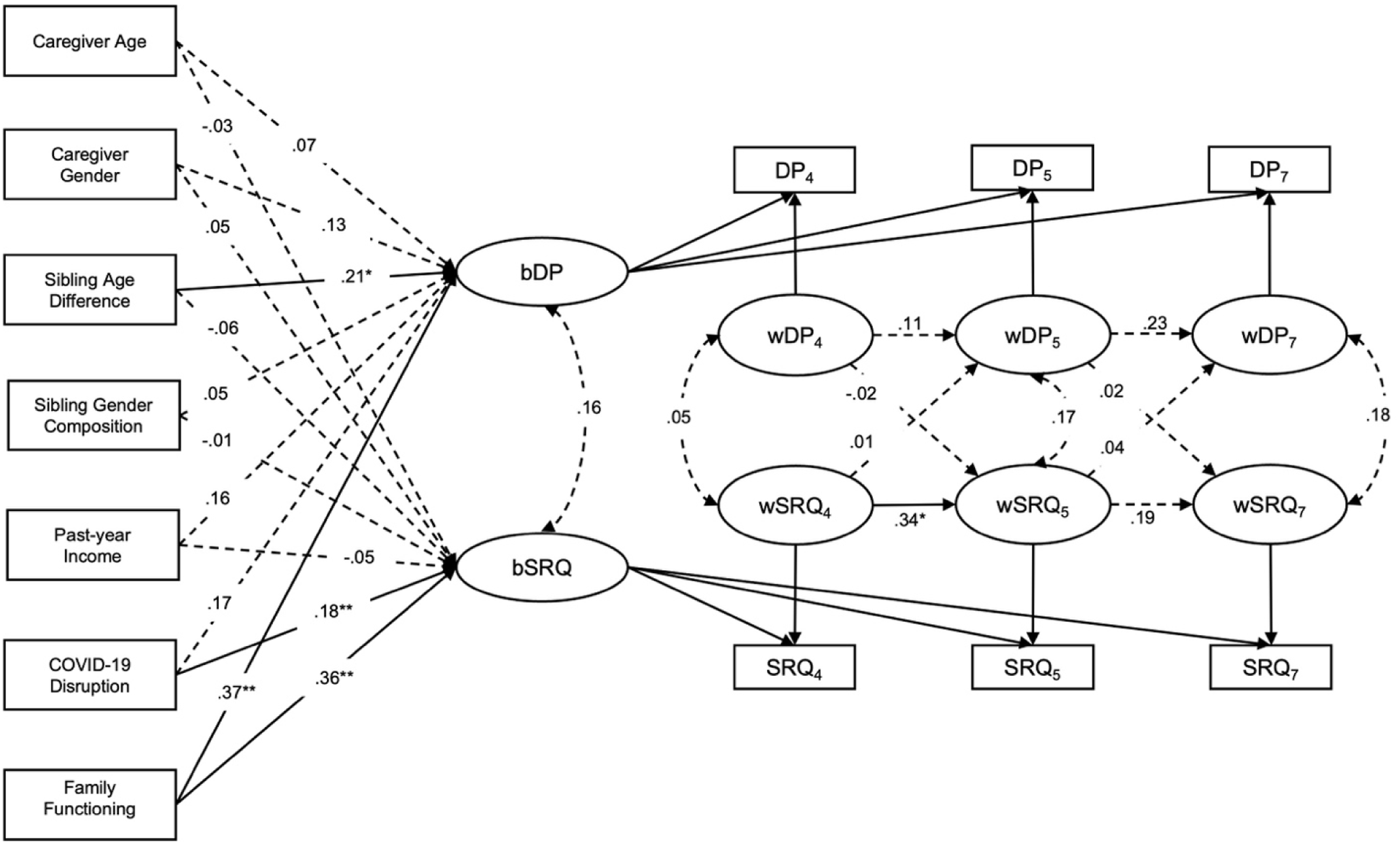
Differential Negativity and Sibling Relationship Quality
The differential negativity model, Model 3, also offered a good fit to the data: χ2(33) = 56.36, p = .007; CFI = .95, TLI = 0.92, RMSEA = 0.04 [90% CI = 0.02–0.05], SRMR = 0.03. Figure 3 shows the full model. The covariance linking the random intercepts was significant (σ2 = .59, p = .014), suggesting differential negativity is associated with poorer sibling relationship quality, overall and independent of time, at the between-family level of analysis. A significant autoregressive effect emerged for sibling relationship quality, such that lower quality at T4 predicted similar patterns at T5 (β = .42, p = .002). Two significant within-families cross-lag effects emerged in Model 3. First, lower-quality sibling relationships (compared to the family average) at T4 predicted less differential negativity (than the family average) at T5 (β = −.27, p = .013). Thereafter, higher differential negativity led to higher-quality sibling relationships than is typical for the family at T7 (β = −.33, p = .005). This pattern is similar to that observed in Model 1 and affirms the potential presence of transactional associations. As with the other models, higher family dysfunction predicted both differential negativity (β = .34, p = .001) and poorer sibling relationship quality (β = .39, p < .001). COVID-19 disruption was also linked to poorer sibling relationship quality (β = .17, p = .004). RI-CLPM of sibling relationship quality and differential negativity. Note. *p < .05, **p < .01; Solid lines indicate statistically significant associations, while dashed lines indicate insignificant associations. DN = Differential Negativity; SRQ = Sibling relationship quality; parameters starting with “b” refer to the between-families variance components, and parameters starting with “w” refer to variance at the within-family level.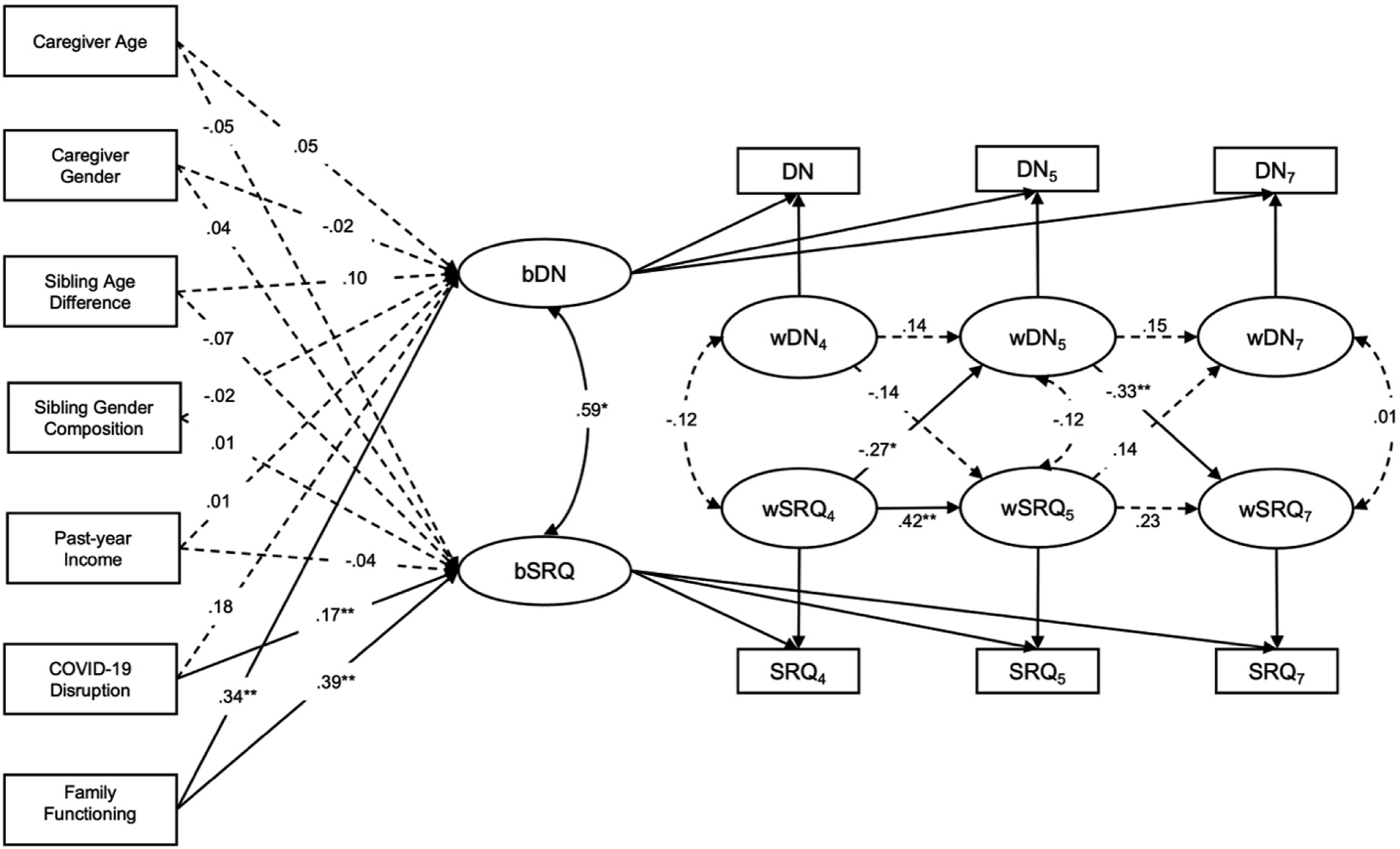
Discussion
The present study explored associations between the magnitude of PDT and sibling relationship quality using RI-CLPMs, isolating the time-varying and time-invariant components of this association. Consistent with our hypotheses, greater overall PDT and differential negativity specifically corresponded to poorer sibling relationship quality, overall and irrespective of time, at the between-family level. In other words, when families demonstrate more differential negativity, siblings have poorer quality relationships. Within families, the association between differential negativity and sibling relationship quality is transactional, though the pattern of association runs counter to initial hypotheses. Compared to the family norm, poorer sibling relationship quality at a particular time predicted less differential negativity at a subsequent time point, which corresponded to poorer sibling relationship quality thereafter. Though inconsistent with initial hypotheses, such within-family patterns appear to align with the family systems principle of homeostasis, whereby families actively maintain a predictable pattern of interacting (for better or for worse), through dynamic negative feedback loops.
Between-Family Spillover: Sibling Relationships and Parenting Quality
Between-family results indicated that total PDT and differential negativity, overall and irrespective of time, were associated with poorer quality sibling relationships. These findings support existing literature suggesting that families with a greater magnitude of differential treatment experience sibling relationships with more challenges and negativity. Previous studies on this relationship have proposed theories in line with the spillover hypothesis, which suggests that affect in familial relationships transfers to other relationships in the family system, with the same affective valence (Nelson et al., 2009). Specifically, it is suggested that when parents are more controlling, harsh, and reactive toward one child than another, negativity may transfer to sibling dyads and result in poorer quality relationships through fostering anger and rivalry. Additionally, poor sibling relationship quality may spillover and disrupt parent-child interactions and foster negative parental attitudes toward children (Derkman et al., 2011; Yu & Gamble, 2008). These disruptions and attitudes may solidify as a stable family dynamic and further manifest as negative behaviors directed toward one child, thus producing, maintaining, or exacerbating differential negativity.
It is possible that a family-wide shared third variable process may be responsible for the between-family association between PDT and sibling relationship quality. Substantial evidence suggests that PDT and poor sibling relationship quality are more prevalent among families facing adversity, including cumulative psychosocial risk (Kretschmer & Pike, 2009; Meunier et al., 2013). This may be because, under conditions of stress, parents’ psychological resources are taxed, and they may have greater difficulty regulating their parenting (Meunier et al., 2013). Relatedly, it may be simpler to allocate more attention, love, and support to a child who exhibits fewer challenges and who is easier to parent, while becoming harsh and reactive to a child who displays more challenging behaviors, including poor emotional regulation (Meunier et al., 2012, 2013). Similarly, children may struggle with behavior in a more disorganized or chaotic home environment, leading to conflict and tension between siblings (Kretschmer & Pike, 2009). Notably, some environmental factors previously observed to influence PDT and sibling relationship quality were controlled for in the models, including family dysfunction, though we cannot rule out other unaccounted-for environmental factors, nor can we rule out shared genetic effects explaining associations between PDT and sibling relationship quality.
Within-Family Effects: Homeostasis and Negative Feedback
The cross-lagged effects of Model 3 support a transactional relationship, whereby parents appear to adjust their magnitude of differential negative treatment in response to poorer sibling relationships, and siblings may then compensate for negativity in the parent-child relationship by increasing warmth in the sibling relationship. These results contradict the spillover hypothesis, which informed the present study, and instead suggest a homeostatic process within the family system—that is, the process of maintaining stable conditions through a dynamic steady state (Kim & Rose, 2014). Family systems theory suggests that when families observe conflict and fall out of a state of equilibrium, they adopt homeostatic mechanisms to counteract the tension and return to a stable condition (Messer, 1971). Parents may be reacting to a worsened sibling relationship by treating their children more equally (e.g., being firm with both) to offset sibling conflict and return the family to a predictable or familiar state. Further models of family homeostasis suggest that when families deviate from their homeostatic level, a mechanism for maintaining stability within the family is the formation of defensive alliances (Messer, 1971; Persram et al., 2017). These alliances are temporary, as dyads come together as a means of support, maintaining equilibrium amidst conflict (Messer, 1971; Persram et al., 2017). Following this model, when the magnitude of differential negativity becomes greater than what is average for the family, children could display more prosocial behaviors in the sibling relationship, forming a defensive alliance to counteract the increased negativity from parents (i.e., “teaming up”). This temporary increase in positivity within the sibling relationship may serve to maintain stability within the entire family, counteracting the heightened differential negativity in the parent-child relationships. Alternatively, sibling relationships serve as a coping mechanism for children, observed to protect against family stressors, including family conflict, and the resulting adverse outcomes (Davies et al., 2019; Gass et al., 2006). In situations of heightened differential negativity, siblings may turn toward each other for warmth as a coping mechanism against the increased parent-child conflict. Thus, sibling relationship quality may show increases in positivity in the context of greater differential negativity, as this may buffer against family conflict and/or maintain stability within the family environment. These findings highlight the importance of homeostatic mechanisms within families, as parents and siblings respond to volatility and departures from “the norm” in the family environment to stabilize the family unit.
Limitations
The results of the current study should be interpreted with several limitations in mind. First, study variables were measured via parent reports, which could deviate from child-report data, as parents and children often hold different perspectives. For instance, children tend to report more positive behaviors and fewer negative behaviors than their parents on measures of sibling relationship quality, and parents and children may report differently on parenting practices (Braconnier et al., 2018; Jensen & Thomsen, 2024; Meunier et al., 2012). Additionally, parents may have been influenced by a social desirability bias when reporting on parenting practices toward their children. Future studies may consider using both child and parent reports, in addition to observational data, to examine the relationship between PDT and sibling relationship quality.
Other limitations relate to the external validity of the study. As the CRAMPED Families Study was conducted throughout the COVID-19 pandemic, caution must be exercised in generalizing these findings to other time periods. While COVID-19 disruption was controlled for in the study models as a covariate, it is possible that the observed familial relationships and parenting practices could be influenced by the unique stressors and demands of the pandemic (i.e., parents being more controlling in line with lockdown protocols). Our measures also took place over longer intervals of one year. While this allowed adequate time for change, it is possible that smaller fluctuations were not detected, especially as PDT measures were generally small in magnitude. Moreover, our sample primarily comprised white, well-educated, employed, two-parent households from the United Kingdom. This raises questions about the generalizability of the findings to other demographic populations, as PDT is greater amongst contextual risk factors, and sibling relationship quality is influenced by family functioning and divorce (Brody, 1998; Meunier et al., 2013; Sheehan et al., 2004). Additionally, the children in the study spanned a wide age range, making it difficult to ascertain differences related to developmental stages. Going forward, examining the longitudinal relationship between PDT and sibling relationship quality in the context of different familial and contextual risk factors, and considering developmental stages, may bolster the generalizability concerns of the present study.
Implications
The unique findings across domains of PDT highlight the importance of considering negative and positive parenting practices separately. When examining PDT, future studies should consider unique processes that may differ within and between families, rather than using broad metrics of overall parenting behavior. Moreover, existing literature has often theorized that PDT is the causal factor in the relationship between PDT and sibling relationship quality; however, the present study presents evidence for sibling relationships influencing parenting behaviors. Research should expand upon these findings, examining the impact of sibling relationships on parenting practices and the homeostatic mechanisms that may be at play. Additional research avenues may also explore the sibling relationship as a protective factor against negative parenting practices and dyadic conflict in the family. Recognizing how familial dyads influence other familial relationships has important implications for clinical practice. The present findings provide support for programs that focus on improving family dynamics by targeting select familial dyads and strengthening these relationships to offset negativity in other dyads. Additionally, programs intended to bolster sibling relationships are of importance, given the implication that these relationships may protect against negative parenting practices.
Conclusion
The present study extends existing literature by exploring the directional relationship between PDT and sibling relationship quality using longitudinal panel methodology. Findings suggest an overall relationship whereby greater PDT generally, and greater differential negativity specifically, are associated with poorer sibling relationship quality. Moreover, lower quality sibling relationships are associated with lower differential negativity over time, while greater differential negativity (greater than the family average) is associated with more positivity in the sibling relationship over time. This novel finding implicates homeostatic processes and the importance of maintaining social stability within the family environment. Potentially, parents respond to increased conflict in the sibling relationship by treating siblings more equally, and children recognize changes in parental treatment and react by forming stronger and more cohesive bonds in order to maintain stability within the family unit. Similarly, children may be turning toward their siblings as a coping mechanism against the increased parent-child conflict, using the sibling relationship as a protective factor. The findings of the present study have implications for future avenues of research and the potential to inform programs that improve family dynamics.
Supplemental material
Supplemental Material - Parental Differential Treatment and Sibling Relationship Quality: A Longitudinal Study
Supplemental Material for Parental Differential Treatment and Sibling Relationship Quality: A Longitudinal Study by Lillian M. Eckert, Jasmine Zhang, Mark Wade, and Dillon T. Browne in Journal of Social and Personal Relationships
Footnotes
Author Contributions
Conceptualization: Lillian M. Eckert, Dillon T. Browne; Formal analysis: Lillian M. Eckert, Jasmine Zhang; Funding acquisition: Dillon T. Browne, Mark Wade; Investigation: Dillon T. Browne, Mark Wade; Writing – original draft: Lillian M. Eckert; Writing – reviewing and editing: Lillian M. Eckert, Jasmine Zhang, Dillon T. Browne, Mark Wade.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study included the Society for Research in Child Development (SRCD) Small Grants Award [NA], Canada Research Chairs Program [950-232347], Ontario Early Researcher Award [ER19-15-224], and a Canada Graduate Scholarship – Doctoral [767-2022-1583].
Open science statement
As part of IARR's encouragement of open research practices, the authors have provided the following information: The research was pre-registered. The aspects of the research that were pre-registered were the study’s hypotheses and analysis plan. The registration was submitted to the Open Science Framework. The data used in the research cannot be shared with any person because we do not have ethics approval for data sharing. There are no materials used in the research to be shared.
Ethical Considerations
Ethics approval was obtained from the Human Research Ethics Board of the University of Waterloo (approval: 46079) on January 29, 2024.
Consent to Participate
Informed written consent was obtained from all caregiver participants included in the study.
Data Availability Statement
The dataset used is not publicly available because ethics approval was not obtained for data sharing.
Supplemental material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.