
Abstract
Sexual communication is integral for many interpersonal relationships’ success, with both relational and individual health affected by the quality of sexual communication between partners. In polyamorous relationships, partners make agreements regarding their engagement in concurrent romantic and/or sexual relationships. The objective of this project was to examine how safer-sex practices are discussed within polyamorous relationships through the lens of sexual scripts theory. Participants (n = 26) were individuals self-identifying as polyamorous who reported their discussions of safer-sex practices, as well as their relational and health implications resulting from such conversations. The prevailing cultural script of having discussions about safer-sex practices, which participants learned from other poly community members and partners, was key to successfully establishing multiple intimate relationships. Interpsychic scripts were illustrated in participants’ desire to have recurrent open and honest discussions, including when a potential new partner was coming into the picture. Interpersonal scripts were seen in the topics of these discussions participants reported having, which included using condoms, sharing sexually transmitted infection (STI) results, understanding risk tolerance, and knowledge of other partners and their sexual practices. Having these discussions successfully not only allowed participants to pursue new sexual relationships but also helped build relational trust and intimacy. Refusal by potential partners to discuss safer-sex practices was perceived as a red flag and resulted in either cooling off relational interest or avoiding sexual activity. This study’s findings suggest health and relational implications for individuals in polyamorous relationships. Healthcare practitioners and relationship counselors should offer STI testing to all individuals regardless of marital status, allowing for destigmatization of STI testing.
Keywords
Sexual script theory (Simon & Gagnon, 1986) proposes that sexual behavior follows a set of scripts around which we organize, interpret, and understand sexual encounters (Garcia et al., 2012). In the U.S., monogamy has historically been the acceptable sexual script (Gupta et al., 2025) and scripts are gendered (Frith & Kitzinger, 2001; Garcia et al., 2012), raced (Stephens & Phillips, 2003, 2005), and reinforced by media representations (Garcia et al., 2012). The monogamous sexual script has led to mononormativity, or the belief that monogamy “is the natural, common, and morally superior way” of engaging in romantic or sexual relationships (Gupta et al., 2025, p. 1906), that dyadic relationships are meant to be marital and reproductive in addition to monogamous (Montali et al., 2023).
Contrasting mononormativity, consensual nonmonogamy (CNM) or ethical nonmonogamy comprises relationships in which more than two people are involved romantically and/or sexually (Hamilton & Winward, 2022). CNM encompasses a wide range of relationship styles, which includes swinging (e.g., exchanging partners with other couples for sexual purposes), open relationships (e.g., where couples allow their partner to have sexual experiences aside from their own relationship), and polyamory (e.g., distinctive from adultery, in which secrecy is key) (Alarie et al., 2024; Moors et al., 2021; Sheff & Hammers, 2011). In this study, we focus on polyamory in which there is acceptance of developing multiple romantic and/or sexual relationships simultaneously (Alarie et al., 2024; Dixon, 2016). A recent United States Census-based national sample of 3,438 single adults suggested 1 out of 6 people desire to engage in polyamory, and 1 out of 9 people have engaged in polyamory at some point during their life (Moors et al., 2021). In existing research, the people who engage in CNM are typically white, straight, cisgendered, and between 28–45 in age (O’Byrne & Haines, 2021), even as people of a variety of identities engage in CNM (Balzarini & Muise, 2020). Although outside the bounds of predominant monogamous relationships between two people, polyamorous relationships still contend with some of the same issues and scholars have articulated the need to understand communication behaviors of genders and sexualities, which includes polyamorous relationships (Balzarini et al., 2017; Rubinsky, 2018). Communicating about safer sex practices is imperative for maintaining healthy relational and health outcomes (Horan, 2016) regardless of the relational makeup. Yet, there remains a gap in the literature on (1) how adults in polyamorous relationships discuss safer sex, (2) the relational implications of such conversations, and (3) the health implications of such conversations. Guided by sexual scripts theory (Simon & Gagnon, 1986), this project aims to investigate safer-sex discussions in polyamorous relationships and argues that ongoing, meta-communication regarding sexual scripts and personal and health boundaries are vital aspects of polyamorous relationships.
Literature review
Understanding CNM in relation to sexual health
As mentioned above, CNM encompasses a variety of relationships such as swinging or polyamory (Alarie et al., 2024; Moors et al., 2021; Sheff & Hammers, 2011). While these types are considered ethical by those within the community and even some outside of the community, CNM relationships in general often bear stigma as they “represent major transgressions of the norm of monogamy” (Andersson, 2022, p. 1918). In fact Balzarini and Muise (2020) report that 26–43% of people in polyamorous relationships report feeling stigmatized and Vaughan et al. (2019) highlight the stigma within healthcare experiences. By being stigmatized, CNMs are misunderstood and mischaracterized, resulting in research grounded in the premise that behaviors in CNMs are akin to infidelity and upsetting to their partner(s) (Hamilton & Winward, 2022; Séguin, 2019). In polyamory specifically, the emotional and interpersonal aspects of building meaningful relationships are often highlighted despite being outside traditional understandings of time spent together or sexual or romantic exclusivity (Cardoso et al., 2021). Given this context, it is important to investigate specific perceptions and attitudes related to CNMs as related to safer-sex behaviors. Therefore, in this study, we will focus exclusively on individuals in polyamorous relationships.
Even beyond defining CNM, defining polyamorous relationships is complex and contested (Klesse, 2006), with several variables affecting a polyamorous relationship, including investment, acceptance, secrecy, and time spent having sex (Balzarini et al., 2019). To navigate such a relationship, all partners make agreements regarding their engagement in concurrent romantic and/or sexual relationships (Balzarini et al., 2019). Polyamorous relationships can take many structures, including “primary” and “secondary” partners (e.g., hierarchical polyamory), triads, quads, “Vs,” and “mono-poly” relationships where some partners are monogamous and others engage in relationships with other people (Mercer et al., 2018; Moors et al., 2021). The participants in this study added to these labels explaining a nesting partner as a partner with whom they live, a polycule to denote all members connected through polyamorous relationships with one another, and a “hinge,” which, similar to a V, is one person who dates two other people who are not dating one another, thereby acting as a hinge between two metamours. Regardless of the terms used, a primary concern facing individuals in any sexual relationship is that of sexual health.
For individuals in any sexual relationship, sexually transmitted infections (STIs) are often a point of concern. STIs are among the most common infectious diseases in the United States; nearly 2.5 million new cases were diagnosed in 2023 (CDC, 2024b). If left untreated, STIs can cause several types of cancer, infertility, and other health issues with short-term and long-term implications (World Health Organization, 2024). For individuals with multiple sexual partners, associated risks of STIs may increase if proper safe sex practices are not adhered to (e.g., using condoms and regular sexually transmitted infection [STI] testing (Johns Hopkins Medicine, 2024). Even in cases where one individual is monogamous but another is polyamorous, the risk of STI transmission and infection is increased (Mercer et al., 2018). Yet, some research suggests that CNM partners report greater condom use during intercourse than monogamous partners (Lehmiller, 2015). Therefore, it is imperative for research to investigate how safer-sex practices are discussed in polyamorous relationship structures. In the present study, we used sexual scripts theory as the theoretical lens to examine how individuals in polyamorous relationships discuss safer sex.
Sexual scripts theory
Sexual scripts theory suggests that three interrelated levels of reality exist and guide the development of conversations about sex-related topics (Simon & Gagnon, 1986). This theory goes beyond the existence of the scripts themselves (e.g., which inform perceptions of sex or sex-related constructs) to examine the underlying processes (O’Byrne & Haines, 2021; Romaniuk & Terán, 2022). This theory poses the idea that individuals adhere to specific sexual scripts if two conditions are fulfilled: (1) that a script is socially acceptable, and (2) that favorable outcomes are produced as a result of behaving in accordance with a specific script (Romaniuk & Terán, 2022). Three factors, or levels, affect the social acceptability of the script. These levels include intrapsychic, where an individual develops personalized scripts based on evaluations of existing cultural scripts; interpersonal, where interaction with others is evaluated; and cultural, which describe the societal norms regarding sexual behaviors (Machette & Montgomery-Vestecka, 2023). Essentially, intrapsychic scripts are based on a person’s expectations of sexual communication within the relationship(s), while interpersonal scripts focus on which sexual topics are discussed and at what points in the relationship (Machette & Montgomery-Vestecka, 2023). Individuals can acquire (i.e., learn) a new script, activate (i.e., cue retrieval of) a script, and apply (i.e., utilize in their own life) a script (Wright, 2011).
Several sexual scripts are identified in literature, albeit with few explicitly focused on polyamorous relationships. Cultural sexual scripts are primarily driven through media exposure (e.g., television); for individuals who have little or no first-hand experience with sex or dating, these cultural scripts are a primary mechanism of how one will understand social acceptability of behaviors (Romaniuk & Terán, 2022). Garcia et al.’s (2012) study identified the influence of mediated representations of scripts to be formative in college hookup culture. Stinson (2010) suggested, however, that hookup culture was quite different from dating culture and was a departure from mononormativity. As mentioned above, monogamy has a clear cultural script, or template, with which individuals can choose to model sexually or romantically (Wosick-Correa, 2010). Intrapsychic scripts draw upon the cultural, or socially accepted, scripts. They also arise to meet the needs of particular interactions while fulfilling individual “desires, memories, and plans” (Gagnon, 1990, p. 10). Interpsychic scripts, therefore, provide the wherewithal by which people realize their sexual identities (La France, 2010). They influence interpersonal scripts, which occur during social interactions (Gagnon, 1990; La France, 2010).
Interpersonal sexual scripts are typically developed out of family relationships and adjusted later in life through peer relationships. For example, having more open and diverse conversations about sex in one’s family of origin predicted increased direct sexual communication for women (Wu & Pask, 2024). While research has developed and some of the thoughts surrounding polyamory have shifted over time, research indicates that therapists have perceived nonmonogamous individuals as fearing commitment or intimacy (Hymer & Rubin, 1982) or even as having a personality disorder (Knapp, 1975). These positive or negative interpersonal interactions can create or reinforce ideas of what it means to be in a polyamorous relationship.
Given that individuals are more likely to have experience interacting with individuals who are in monogamous relationships (e.g., having one consistent romantic or sexual partner) in comparison with those who are in polyamorous relationships, these scripts may be particularly powerful. Extant literature has long explored recommendations for monogamous individuals related to safe-sex practices, specifically related to communication. For example, Troth and Peterson (2000) explored antecedents and consequences of young adults’ beliefs about safe-sex communication in their early couple relationships, finding that positive attitudes to safe-sex discussion predicted having talked about AIDS and condoms with a dating partner as well as actual condom use. However, less is known about how sexual minorities navigate similar but arguably more complex conversations.
What literature exists around scripts and CNM looks at script theory broadly and in specific relation to alternative scripting. Some research focuses on scripts from a different perspective, naming them rules or agreements (Wosick-Correa, 2010) or norms (Rodrigues et al., 2024), but often in opposition to hegemonic sexual scripts. O’Byrne and Haines (2021) found that CNM relationships are not unbound by scripts but follow “alternative rules” in establishing scripts. Haupert et al. (2017) posited that people in CNM relationships also have explicit rules about STI testing and barrier methods in sexual encounters. Lamont’s (2017) study described polyamorous participants’ emphasis on equal power among relationship partners and the importance of non-gendered relationship rules as being crucial scripts. Tiidenberg (2014) claimed that when discovering or creating scripts that diverge from the mainstream, a sense of community is particularly important. In Rittenhour and Sauder’s (2024) study, participants shifted away from hegemonic scripts when exposed to “a new sexual experience, sex education, or an alternative sex community” (e.g., polyamorous communities, p. 463). One recent work identified ideals of consent, honesty, and communication reproduced and renegotiated in CNM relationships broadly, finding that negotiation itself is key for their relationships, with renegotiation likely (Andersson, 2022). We build on the existing research to ask,
How do adults in polyamorous relationships use sexual scripts to discuss safer sex?
Initiating or participating in a conversation with a sexual partner can pose risks to the relationship itself (Brannon & Rauscher, 2019). Many adults feel that providing sexual information, including information about their sexual history, will negatively affect their partner’s perceptions of them (Xiao et al., 2015). In monogamous relationships, sexual self-disclosure leads to greater partner understanding of sexual likes and dislikes, which in turn leads to a more favorable balance of sexual rewards and costs and thus to higher sexual satisfaction (MacNeil & Byers, 2005). Of note, research shows a bidirectional relationship between sexual satisfaction and relationship satisfaction among long-term couples (Beaulieu et al., 2023), and CNMs have higher sexual satisfaction and relational intimacy than monogamous couples (Montali et al., 2023). Self and partner communication variables, such as willingness to engage in such conversations necessitating openness and honesty, predicted relationship satisfaction in monogamous dating couples (Jubran et al., 2025; Meeks et al., 1998). Sexual scripts theory has been applied in the context of sexual communication discrepancies, finding that these discrepancies are related to sexual satisfaction (Machette & Montgomery-Vestecka, 2023). Yet, these processes are less investigated among those in polyamorous relationships. Therefore, we present our second research question:
What are the immediate and subsequent relational implications or consequences of these discussions?
Expanding beyond relational implications, health is also important for individuals in polyamorous relationships. As mentioned previously, undiagnosed STIs can result in several short-term and long-term health issues (Johns Hopkins Medicine, 2024). Given that having multiple partners may increase someone’s risk of STI exposure (CDC, 2024a), despite evidence that STIs are no more prevalent in CNM relationships than in monogamous ones (Lehmiller, 2015), it is important to understand how safer sex is negotiated in polyamorous relationships. Previous research found that higher levels of self-efficacy related to condom usage and an increased willingness to communicate about health positively predicts open conversations about STIs (Brannon, 2019). Based on existing sexual scripts, an individual may choose to disclose or withhold information that may be relevant to their own, or their partner’s/partners’, health, thereby affecting health decision-making processes (Brannon & Rauscher, 2019). Therefore, we ask,
What are the health implications or consequences of these discussions?
Method
Author positionality
In the spirit of reflexivity, we report that each author identifies as a married woman living and operating within U.S. understandings of sexual scripts and stigma around CNM relationships. Our PhD programs in the U.S. either did not cover CNMs or only covered them briefly. The first and third authors regularly publish health communication-related research, and the second author focuses on how particular groups use discourse. Although none of the authors identify currently as consensually nonmonogamous, we were careful not to claim otherwise with participants while recognizing the need for research related to how polyamorous-identified people negotiate safer-sex conversations.
Procedures
After receiving IRB approval, we posted our call on a national communication listserv (COMMNotes) to begin recruiting. Additionally, we used snowball sampling to solicit participation from adults at least 18 years of age who self-report engaging in polyamorous relationships. Initially, we struggled to find participants willing to be interviewed, necessitating a hiatus in data collection until new leads could be secured. We were able to repost our call on the national listserv later and collected enough interviews after this second round to reach data saturation in our transcripts (Glaser & Strauss, 2009). Duplication of participants was not allowed. We conducted and recorded 26 in-depth interviews through Microsoft Teams, which auto-transcribes data. We manually verified the transcripts, resulting in 523 pages of data. Interviews ranged from 15-45 min with an average length of 28 min.
Participants
Participant demographics.
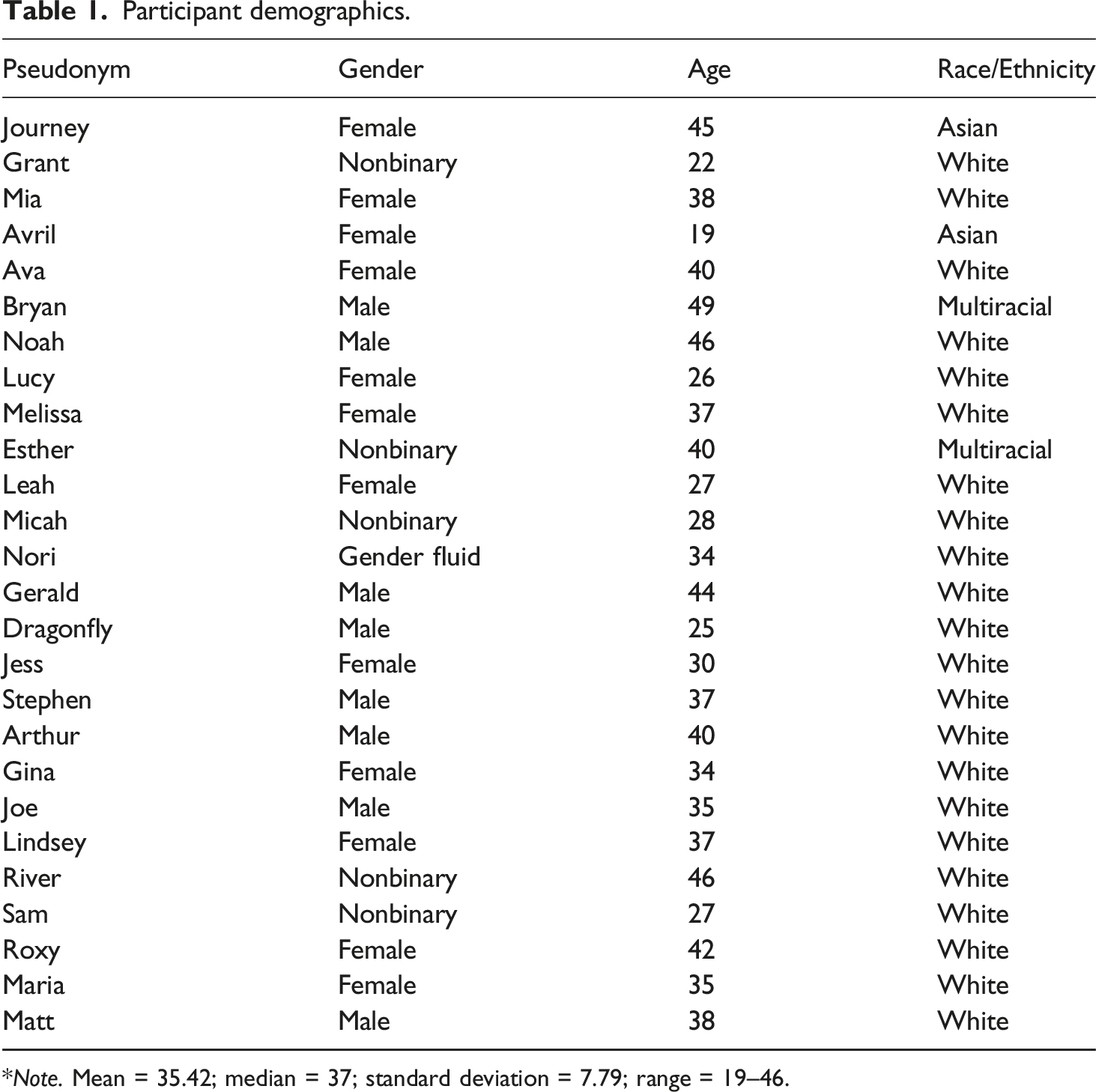
*Note. Mean = 35.42; median = 37; standard deviation = 7.79; range = 19–46.
Data analysis
The interview recordings were auto-transcribed, manually verified, and analyzed by emphasizing the researchers’ active roles (Braun & Clarke, 2013, 2022). We based our understanding of reflexive thematic analysis (RTA) on elements of reflexivity, integrating meaning-based interpretive stories, and considering our analytic practice by ensuring our methodological procedures and concepts were coherent with our research values (Braun & Clarke, 2022). We recognize that RTA is inherently subjective and that coding is an inherently interpretative practice, with our understanding and lived experiences affecting how we describe exemplar quotes (Braun & Clarke, 2023) (see Author Positionality, earlier). We used sexual scripts theory as the guide for our RTA to inform the development and interpretation of codes and themes by orienting us to patterns of meaning related to scripts, expectations, and normative understandings of sexuality within the narratives described in the interviews. We selected RTA given its theoretical flexibility, as well as recommendations related to sample size and analytic focus, specifically as we were interested in how personal experiences are situated within wider socio-cultural contexts (Braun & Clarke, 2021).
Prior to coding and theme development, we immersed ourselves in the data by reading transcripts multiple times. Since each of us conducted interviews, we first started with our own interviews before reviewing other interview transcripts. We took notes throughout the interviews and reviewed these as part of the data immersion process as well. Codes were generated manually, throughout which our team met multiple times during the data analysis process to discuss our individual interpretations of the data, the theory, and development of themes. We used sexual scripts theory through a constructionist paradigm, in which we understood the themes through social and context-bound constructions. Our reflexive process involved regular weekly meetings with shared notes and peer discussion as we reviewed and refined.
Participants meta-communicated that open, clear, and on-going communication with their partners is essential to navigating their relationships. This metacommunication was present when participants described cultural scripts (RQ1). The themes of protection and boundaries were prevalent in the data. Some of the codes such as STIs, STI testing, condoms, and pregnancy led to the creation of the protection theme. Consent, safety, and type of sex were codes that led to the boundaries theme. Both themes were prevalent in intrapsychic and interpersonal scripts (RQ1).
We ensured rigor through validation strategies like prolonged engagement with the data over several months’ time, continuing reflexive dialogue in our peer discussions, selection of illustrative exemplars, and member checks in which we sent the draft of our manuscript to five participants who had indicated interest in reviewing the manuscript (Creswell, 2007). Three of the five responded with comments, such as suggesting we further clarify certain parts of their interviews (e.g., Gina offering more insight into the issues with a partner who did not want to use condoms despite her insistence on their use), which we integrated into the present version of the manuscript.
Results
Presence of scripts in safer-sex discussions
In this section, per RQ1, we identify the sexual scripts participants used to navigate safer-sex conversations between themselves and their partner(s). As discussed above, sexual scripts theory proposes that there are three levels affecting the social acceptability of scripts. These three levels—intrapsychic, interpersonal, and cultural—do not work in a linear fashion but overlap and reinforce one another. For instance, an intrapsychic script may be reinforced if the person sees it play out at the cultural level just as it may be adapted or abandoned if it is not seen as socially acceptable interpersonally.
Intrapsychic scripts
RQ1 focused on how adults in polyamorous relationships use sexual scripts to talk about safer sex. At the intrapsychic level, participants explained the importance of communicating the boundaries of the relationship and protection as central themes. One participant, Joe, said that discussing polyamory preceded conversations about safer sex because partners had to discuss what polyamory means to each of them first, “You know, do you consider yourself polyamorous? What are the sort of parameters for the relationship that you’re expecting?” For Joe, partners must know and be able to communicate their own ideas around the boundaries of the relationship before further talk about safer sex can commence.
Communicating about intrapersonal understandings of the relationship and safer-sex talk also occurs whenever a new dating partner comes into the picture, according to Melissa. These talks occur early in the relationships and are context dependent, including how often partners meet and the intensity of the relationship. For some participants, communicating boundaries and testing needs is imperative before a new partner is added. Participants noted they must also contend with who should initiate these conversations. When asked whether it is he or his partners who bring up the safer-sex discussion with partners, Gerald noted, “I would generally expect that if I didn’t raise that... and the other person didn’t raise that, that would be a warning flag for me about the other person.” Maria suggested gender may play a role (for some participants) in who initiates the conversation: So, I have dated men, women, non-binary people. I would say that in general it is more common for me to be the one who initiates safer-sex conversations with cis, male partners. And I would say it’s been about equivalent as far as initiating safer-sex conversations with non-binary and female partners, people I’ve been dating.
Some participants did not identify who should initiate the conversations but did offer advice about how to build on these conversations. For example, Nori recommended stopping and evaluating when a new situation arises, doing lots of research beforehand, taking it slowly, and having many conversations, especially about consent. Nori’s intrapsychic script around communication was crucial to them. Similarly, Micah advised that every conversation will be different and that some level of awkwardness is expected, noting that even through that awkwardness these intrapsychic scripts are necessary to follow. Once partners communicated about the terms of the relationship, they could then more thoroughly discuss their intrapsychic scripts around protection.
Protection was a common theme for participants. Protection not only refers to contraception (e.g., condom use) but also refers to STI testing. Protection includes using hormonal birth control, as well as discussions about tubes being tied and hysterectomy. Within this theme of protection, some participants discussed pregnancy, not only the physical consequences but also how one feels about pregnancy and parenting, as articulated by Gerald: I am so terrified of ever being a parent. It is a huge trigger for me. I will literally freak out if I think there’s a chance that I’m pregnant and that was a thing with a partner, and so there’s different sensitivities about. Like, it’s not just the risk in terms of the physical consequences, but the risk in terms of how you feel about that.
Thus, as Gerald interacts with partners, protection is top of mind and an intrapsychic script he sets for himself.
Much of the discussion around protection was around STI testing and prevention. These scripts often played out interpersonally, yet participants mentioned drawing intrapersonal boundaries for themselves first. For instance, many participants talked about the idea of being “fluid-bonded” with another partner, of having sex without a barrier in place. For some participants, there were specific boundaries around when and with whom they would be fluid-bonded and/or would be comfortable with a partner fluid-bonding with someone else. Micah acknowledged that no fluid-bonding would occur with a new partner until each partner had a recent STI test because, as Stephen echoed, fluid-bonding increases risks for all partners. No matter the discussions that ultimately happened with partners, participants had to first decide for themselves the boundaries they were comfortable with around discussing their understanding of polyamory and protection measures.
Interpersonal scripts
As noted above, sexual scripts often interplay, building on and reinforcing one another. In interpersonal scripts, participants noted how their intrapsychic scripts underscored discussions with their partner(s) about boundaries regarding safety within the relationship(s). For example, drawing on the example used above from Joe, participants and their partner(s) often had to navigate what “sort of parameters” they are expecting in their relationships. This requires setting limits around the relationship and how the partners will engage in sex with one another and/or with others.
Participants explained the importance of ensuring everyone in the polycule’s safety needs are met. Nori, for example, explained that in their polycule, matching the partner with the highest need for safety was a way to ensure everyone was comfortable with the choices made. Leah echoed this sentiment commenting that prioritizing everyone’s need for safety was a dynamic process, requiring regular checking in, and Stephen noted it is because these decisions do not affect only one person or relationship, but everyone connected to the polycule. Thus, building interpersonal scripts that work within the relationship(s) is paramount.
For Gina, these conversations precede any sexual interaction. She explained that she asks potential new partners “what their safer-sex practices are because I wanna establish that I use condoms, and I ask them when the last time was that they were tested.” For Gina, a former partner’s enthusiastic condom usage was a sign of “care and integrity and it made me feel really good.” Similarly, Mia explained that she and her primary partner, who have been together five years, have a standing rule to always wear a condom when engaging in sexual interactions. That they have a specific rule within their relationship demonstrates their discussions and subsequent agreement on their interpersonal scripts. For some of our participants, then, discussing these safer-sex scripts is a form of relational connection and care.
This care extends to concerns around STIs and regular testing as well. Several participants mentioned specific STIs such as oral herpes/HSV and HPV and asking partners about practices to reduce the risk of infection such as the regular use of antivirals. Arthur described talking about “protection” to assess how partners can lower their risk: Especially if they have a partner who has a status that is known and it’s something like HSV or HPV. Like what are they doing? Like is that partner that has it on antivirals? Are they using condoms with them? Are there things they avoid because they can lower their risk?
Arthur’s questions reveal how imperative considering others in the relationship/polycule is when engaging in safer sex discussions. As we will discuss later, these interpersonal conversations are often ongoing and dynamic rather than one-time experiences. If participants’ intrapsychic scripts change or are influenced by cultural scripts, a new conversation with partners around interpersonal scripts may also need to be happen.
Cultural scripts
It is crucial to note here that the participants gave us insight into some of the societal norms guiding cultural scripts within the polyamory community. Although polyamorous cultural scripts may lie outside known monogamous relational scripts, we highlight some of the cultural scripts our participants identified.
Some participants indicated frustration around the cultural scripts within polyamory. Gina, for example, said, “I feel like polyamory, like the languaging around it, hasn’t always resonated with me, but I’ve been non-monogamous since I’ve been, like I don’t know, when I was dating people as a teenager.” Gina mentioned that her parents were also non-monogamous, acknowledging that her parents’ views also influenced her. Here, Gina noted not only some cultural scripting within the polyamory community but identifies how her own interpersonal scripts do not align and/or how the cultural scripts within her family may be different than the larger culture’s scripts.
For individuals who have less exposure to what polyamory looks like, these cultural scripts are likely more limited. Some participants noted that their education about polyamory was often informed by friends who were already in the community, doing their own research (online and/or reading books about the topic), and/or finding social media groups dedicated to the topic. Many participants recalled that they learned about the cultural scripts as they began opening up a prior monogamous relationship to polyamory. For some participants, this opening caused friction with their then-partner, elucidating concerns or issues about which they needed more communication. Others saw the opening of their relationship as a point of growth, and, although they may no longer be in the relationship with that partner, the process of opening a relationship together was a point of connection with that partner even still.
Participants often articulated the norms of the polyamorous community, especially when asked what recommendations they would give to someone new to the community. Maria said, I would reassure someone that it’s, as far as my experience goes in the community, these conversations are very normalized. They are typically very low pressure, and they can be had in a way that is casual and in a way that is even kind of like fun and flirtatious if it’s leading up to an initial sexual encounter with a new person.
Similarly, Ava said she recommended that people practice having the conversations since practice makes talking about sex “a lot more comfortable…just asking people out of curiosity as a regular topic, how they themselves choose to handle safe sex and learn to do that with people that they’re not trying to have sex with” so that the pressure was lower if dating did occur later. Repeatedly, participants emphasized the importance of open communication, that taking safer-sex conversations slowly, taking breaks and returning to the conversation as needed is important, identifying that these conversations are often dynamic, ongoing processes. Stephen said, “Talk often. Talk as much as you can. Be honest. Don’t hold anything back,” to indicate how vital participants found explicitly communicating in their relationships to be, especially as they engaged cultural scripts around safer sex in polyamorous relationships.
Conversation relational implications
RQ2 focused on the immediate and subsequent relational outcomes of the safer-sex conversations. Participants explained that communication was central to positive outcomes, both before sex and ongoing throughout the relationship. We will first discuss relational implications for pre-sexual encounters, followed by ongoing communication after a sexual encounter has occurred.
Pre-sexual encounters
Before a sexual encounter, participants often described patience, research, and communication as imperative. Participants claimed no action could or should be taken until communication happens, explaining it shows true caring, respect, and responsibility in thinking of others (rather than one’s own desires). Esther mentioned that sometimes potential partners will adhere to norms like optional condom use and responded with, So, for me that is, that’s not an option, you know, because one not using a condom is incredibly dumb. We learned a thing or two in the 80s. We’re not supposed to do that. And two…It’s not that you are responsible just for your own health. I’m responsible for the health of other people with whom I had conversations, and we have agreements in place. These agreements are usually just like oral agreements, but I still consider them binding.
Esther went on to explain in such a situation, they will offer a non-sexual relationship with a potential partner because they are not going to have sex with someone unless they had the conversation and agreed upon condom usage, framing the conversation as respecting the health of all partners involved.
Refusing to have a conversation about safer sex altogether was perceived to be problematic. For example, Gerald explained if a potential partner was hesitant to engage in the discussion because of lack of skills (or scripts) for talking about safer sex, he would be prepared to “teach them the skills and take it slow.” However, if a person simply refuses to have a discussion, that would be problematic, “That’s such a red flag of communication for me of like, if you can’t do that, I don’t trust you in consent discussions. I don’t think we can do things together. That’s not meeting the minimum level of communication for safe relationships for me.” Gerald understands communication to be a critical step before even considering a sexual encounter. Jess, too, said that if a potential partner reacted poorly to the idea of STI testing, that was a “red flag” to furthering a relationship. Similarly, Joe mentioned having a safer-sex discussion tells him a potential partner’s “communication capacity…emotional compatibility…Makes me feel like I can trust them…potential for greater intimacy.” Thus, the willingness to have these discussions was key for building trust.
Prior to sexual encounters, participants found it pertinent to have structure/boundaries in place, noting that this was a part of consent. As Stephen said, “Because that’s the whole thing with informed consent, as everybody has to be informed.” River commented that it is important to remember that partners come up with the guidelines together so they can change them together if, and when, necessary. Some participants explained that they would not even meet up with a potential new partner if there was not an STI test to share. One participant suggested that he might offer going to get tested together as part of a date to help normalize STI testing.
Post-sexual encounters
Participants indicated that perception checking was key to making sure their partner(s) were on the same page as them regarding ongoing communication. For some participants, regular relationship check-ins were imperative, although the time varied widely (monthly to every six months). This helped some participants come to major relationship revelations, such as the realization that they have taken the next step together in the relationship. Ava said that these conversations affected her decision-making, specifically whether she would date someone, what type of sex she and her partner could have, and how much she trusted them. Further, in doing so, trust is communicated and allows for understanding a partner’s other partners’ boundaries as well. Dragonfly said such conversations are a part of both foreplay and consent; they are additive, not subtractive for the relationship. Gina reflected that being able to have these types of conversations indicated, “There’s some longevity here. If we can navigate this [that is a good sign], because there’s gonna be other tough stuff that happens in the future [and] if we can’t even talk about using condoms easily, [what’s the point?]”. However, if these conversations were met with some push-back from one of the individuals, some negative feelings could emerge. Ava described a series of conversations with her nesting partner, Generally, I started asking questions that he doesn’t quite have answers for. And then he feels like uncomfortable. And he says, well, I haven’t had time to think about it or you’ve had all this time to think about it. And I haven’t. And then he gets frustrated. Then he’ll ask for more time… I get frustrated because I feel like we brought it up enough times that he would have thought about it.
Thus, participants express frustration when their partner(s) did not engage in conversations about safer-sex boundaries. Gerald, too, noted he sometimes has told a partner they need to have a discussion with their other partner(s) about safer sex, “I’m just like your other partner is not doing these conversations. Well, you need to go back in and actually get answers on some of these questions.” Regardless of frequency, participants indicated ongoing communication about safer sex boundaries to be an important relational value.
Establishing boundaries of safer sex
A few participants indicated that they felt like they were the ones focusing on safer-sex behaviors and setting those boundaries. Gina described one dating partner who regularly tried to pressure her to not use a condom during penile-vaginal (PV) sex. As an alternative to PV sex, the partner suggested unprotected anal sex, to which she said, And I was like, why would I not want to use a condom for ass stuff? Like, that’s like, I understand that people do that. But I was like, I also understand how, like, safer sex works and that it’s not a form of safer sex.
Gina later described that feeling pushback can be “very unsettling… Here’s why I’m looking back on it being like why didn’t you just go like if somebody was not willing to respect you even that amount? Why would I continue engaging in that relationship?” Sam, too, noted how respect of boundaries related to feelings of safety regarding sex. They said, I understand where, like, it can cost time or resources or things to get tested, so, like, I can envision a place where there is resistance towards that, but I think also in my brain like the type of person I’d want to be intimate with is the type of person who is open to having a conversation and wants both of us to feel safe and comfortable.
Summing up this idea, Grant explained that sexual consent, as an important component of boundary-setting, is imperative for any sexual relationship “to work and the gears to stay in movement.” At times, relationships did not work; next, we address those instances.
Relationship de-escalation
Some participants shared they decided to de-escalate their relationships when details about another partner’s health status, not previously disclosed, came to light. Arthur’s interpersonal script illustrated his decision to end the relationship with his partner, Bea, after he learned Bea was not using condoms with her other partner, Max, who was both HSV A and B positive. Although Max is on antiviral medicines, Arthur felt he should have clarified with Bea what “protection” included when they had their safer-sex talk: Initially we talked about the partner having a status and I made the mistake of assuming they were using protection because of that, didn’t explicitly ask and she didn’t share. So when we talked about it again later and she was like, we’re not using condoms, he’s just on antivirals. And I was like, OK, well, that’s a much higher risk than I’m willing to accept. So we ended up having to end our relationship at that point.
Similarly, Ava described a situation where her live-in (ex)partner was a married heterosexual man. Ava described that she knew that the married couple were barrier-free (i.e., fluid-bonded), and that she became barrier-free with her live-in partner. Yet, she was unaware that the wife had become barrier-free as well with a new partner until she found out “third hand” and had to bring up, “Hey, how come you didn’t tell me?” As a result, all individuals were tested, and Ava “took a month off sex” prior to ending the relationship. She stated that “they all had to get a little bit more responsible in disclosing things,” which she perceived positively, but still indicated her frustration at the entire process prior to ending her part of the relationship. In terms of interpersonal scripts, Stephen explained that each of his partners wants to be informed about the goings-on with other and/or new partners in different ways, so Stephen has had to discuss the communication expectations (i.e., setting a boundary) regarding safer sex within each partnership.
Other reasons for relationship de-escalation were described. Gina described how living situations changing required some frank conversations, especially as she and her partner both started seeing more people. Yet, she described some challenges in navigating those changes, especially since she still wanted that partner in her life, saying, He’s still incredibly important to me… Because [he] and I are friends and it’s an important relationship [it is important to communicate]. But then you know, at the end of the day, it’s kind of like the it’s a non-normative practice and there’s not a lot of like social support for this kind of relationship.
Even though the relationship had changed, it did not negate the fact that communication still mattered. Whether before or after a sexual encounter, participants identified the importance of ongoing metacommunication about the relationship to be crucial, especially surrounding topics of disclosure and boundaries.
Conversational health implications
RQ3 examined health implications resulting from participants’ safer-sex discussions. In the context of polyamorous relationships, where multiple partners’ health experiences are at stake, these conversations are of the utmost importance for health outcomes. We provide three implications: First, participants described individual-level behaviors they enacted. Second, participants described partner behaviors, and third, participants indicated a need for specific advice to navigate safety and risk in their relationships.
Individual-level behaviors
Some of the individual-level behaviors included engaging in explicit conversations about safer sex in all sexual encounters, carrying Plan B when going to polyamory events like conventions, and practicing having comfortable interactions so that everyone is informed. The protection theme was predominant with participants describing the use of some form of protection including condoms and dental dams. They also noted engaging in other forms of sexual activity without penetrative sex or activities that do not involve the exchange of bodily fluids. Some participants mentioned they have paid for STI checks for potential partners and have proactively shared their own test results.
Partner-level behaviors
Participants also described partner behaviors with themes of protection and boundaries of (safer) sex being commonplace. One participant described a gonorrhea scare, necessitating every person in the polycule to be tested for STIs. In fact, many participants talked about the frequency of testing and that regular testing was a mandatory part of their relationships. This meant getting retested every time a new partner may enter the polycule, getting tested every six months as a general relationship rule, and/or getting tested at least yearly if nothing in the polycule changes. Prioritizing early detection, open communication, and partner protection can reduce STI transmission rates in the larger community, which can improve STI protection.
Melissa explained she has boundaries with all her partners regarding protection. The safer-sex discussion with her comet (the partner whom she sees less frequently) led to them deciding not to have sex: I’ve told her that because she doesn’t use protection and she has a lot more, she has sex with a lot more men, that I don’t really have sex with men. And I was like, because you have sex with men, and you don’t use protection...We don’t really engage in sex because of that.
Thus, these conversations also reflected the decision of forgoing sexual activity due to one partner not using protection, in addition to regular STI testing.
Need for specific advice
Participants indicated a need for specific advice or recommendations, particularly given the stigma around STI testing. Nori, for example, explained that her polycule discusses potential new partners, including testing results, and everyone does their own research to decide what they are comfortable with, especially if this will result in newly erected boundaries around their health information. Another participant, Leah, would like to see everyone—whether polyamorous or not—get STI testing more frequently both as a health measure and as a destigmatizing measure for STI testing in general. One participant advised people new to the polyamorous community will need to spend time working through mononormativity, while another participant recommended more research on polyamory, in particular the discourses around it. One person even described participating in this project by saying it “felt like coming out.”
Participants articulated the risk individuals assume when engaging in polyamory. Matt, who considers himself relatively new to the community, explained the assumption of risk, perceived threat to health and safety, and the need for that to be communicated so individuals can give their consent: In my experience, everybody has understood that we are assuming a certain level of risk by having multiple partners and when there is a credible you know threat to your health or safety. Somewhere in like your chain that that should be communicated like so everybody has the ability to continue to give their consent to the risk level that they’re exposed to.
Interestingly, at the time of the interview with Grant, they were still concerned about COVID-19 when going out (e.g., to a bar/restaurant), so risk was an integrated part of life that informed every part of Grant’s experience at that moment. Thus, participants navigated their individual and collective health choices because of the conversations they engaged in regarding safer sex with their partner(s).
Discussion
Given the increasing interest in consensual nonmonogamy practices by individuals in the United States (Moors et al., 2021) as well as scholars who study relationships (Vilkin & Davila, 2023), and the health and relational implications of safer-sex talk, we used script theory to examine the presence of such conversations in polyamorous relationships. All but one participant noted having discussions about safer sex. Our data shows participants’ interpsychic and interpersonal scripts as well as the cultural scripts they have learned within the polyamory community. This is in line with previous research which suggests that CNM relationships are just as scripted as other lifestyles but in alternative ways (O’Byrne & Haines, 2021).
Lack of prevalent and accessible polyamorous cultural scripts leads to participants having to figure out how to have discussions. When asked what needs to be in place before these conversations occur, many participants said having an understanding about the relationship structure was key. This is echoed in previous research (Wosick-Correa, 2010) and more recently as well (Vilkin & Davila, 2023), indicating the importance of relationship agreements and conversations about interpersonal scripts. In a recent cross-sectional survey, CNM individuals who had relationship agreements, as compared to those who did not, reported higher scores on relationship satisfaction and decision making (Vilkin & Davila, 2023). Beyond discussing relationship structure, most participants felt the need to be direct and to make safer-sex conversations on an ongoing basis a key practice. This was also reported by Wosick-Correa (2010) who noted that “…polyamory is essentially predicated upon continual communication with all partners involved” (p. 52).
Participants discussed boundaries of sexual activity prior to having sex and as part of on-going discussions within multiple partnerships. This is also similar to Wosick-Correa (2010) in whose study participants reported restricting certain sexual acts out of health and relational concerns. Previous research has used Communication Privacy Management theory to conceptualize how boundaries are used in conversations about revealing and receiving sexual health information. The authors found that while many individuals choose to disclose their sexual health information, the same individuals do not feel that it is necessary to disclose the same information (Brannon & Rauscher, 2019; Coffelt et al., 2021).
Being able to have safer-sex discussions is important to trust building (Vilkin & Davila, 2023) and having both the flexibility and willingness to discuss safer sex allows for adaptation within relationships (Lamont, 2017). For many participants, these discussions are part of their interpsychic scripts regarding safety in relationships. A potential partner’s refusal to talking about safer sex or the idea of STI testing was perceived to be problematic. This is because participants considered the capacity to communicate about these topics and readiness of testing to be symbolic of emotional compatibility and necessary for trust building. Thus, being able to talk about safer sex also seems to have a metacommunicative force (Watzlawick et al., 2011).
One of the participants mentioned they have discussed not being exclusive with only one of their two partners. Although this raises ethical concerns regarding the practice of consensual nonmonogamy, Journey reported that her relationship with one of her partners has not reached the level of discussing (non-)exclusivity. She explained that she and her partner had not had the conversation about exclusivity yet because she felt the relationship has not reached the stage of having an open discussion. This may be a negative case analysis (Hanson, 2017), whereby a participant reported not telling another partner that the two of them are not in an exclusive relationship or discussing safer sex prior to engaging in sex. For most participants, having a conversation about the partnership structure where one shared details about their other partner(s) was the first step to having a safer-sex discussion and was required before sexual encounters. This ties into ethics and consent practices noted by many participants that CNMs consider as essential to understanding polyamorous relationships (Cardoso et al., 2021).
Previous research found that while STI testing is higher among sexually active individuals between 15-44 years of age who have multiple sexual partners when compared with those who have one partner, condom usage is lower (Copen et al., 2019). Yet many of our participants highlighted the importance of consistent condom use with most/all of their partners which echoes previous research (Edgar, 1992; Gause et al., 2018; Lehmiller, 2015). As compared to studies with heterosexual couples, where social capital (i.e., how one looks) is used as a proxy to be perceived as being “safe” or “clean,” our study findings centered within the polyamory context suggests condom use behavior along with sharing testing results and consent agreements are the gold standard.
Implications
Study findings have implications for designing safer-sex health messaging, and for communicative practices for health care practitioners and counselors. By investigating the challenges of safer-sex discussions in polyamorous relationships in a small sample, we hope to pave the way for subsequent survey research to further contribute to the existing literature on the relationship between safer-sex communication and safer-sex practices. Results indicated that conversations demonstrated trust in relationships. Explicit and profound communication between/amongst partners might be an effective practice to benefit all relationships, including monogamous and/or heterosexual ones.
Theoretically speaking, our study extends how sexual scripts theory can be used. Globally or at the cultural level, the thinking that one’s actions in sexual activities impacts the health of not only the individual but everyone else in the polycule or other partners seems to be prevalent in the participants. This has a bearing on participants’ interpsychic scripts, which are goals, plans, and desires. Thus, participants carrying condoms, Plan B, and their ability to offer non-penetrative ways to have sex show interpsychic scripts. Additionally, the various examples of encounters in which participants negotiated safer-sex practices via sharing of STI testing results, insistence on condom use, abstaining from having sexual relationships or de-escalation of relationships are illustrative of interpersonal scripts as these are realized in interactions. Like previous research (Haupert et al., 2017), we suggest that understanding how scripts work in CNM relationships might offer improved health possibilities for people in any relationship configuration. As many participants also shared that they get regularly tested for STIs and expect regular testing of their partners, people in the polyamorous community may also be contributing to cultural scripts for the community specifically, even if those scripts have not reached the overarching culture.
Considering how the polyamorous community might help effect cultural script change, healthcare practitioners and relationship counselors should consider offering STI testing to all individuals regardless of marital status, allowing for destigmatization of STI testing. This is particularly important for healthcare providers in certain regions (e.g., the southern part of the USA) given that some participants indicated that regional differences exist in how (if at all) healthcare providers recommend STI testing. Further, healthcare providers should consider offering communication skills training sessions to teach individuals communication strategies that can be used during stigmatized conversations like safer-sex discussions.
Limitations
As with all academic research, several limitations exist. First, the findings from this study are not intended to be generalizable to the broader public. The experiences described by the participants may not be comprehensive representations of various polyamorous communities. Future research should examine perspectives from a more diverse (e.g., racially, ethnically, age) participant pool. Further, future research could use larger scale surveys to examine if the issues described in this dataset are prevalent within the larger poly community. Second, we relied on individual interviews with one member of a polyamorous relationship (or polycule). Therefore, data is limited by self-report or recall bias and is limited to one person’s perspective. Future research should more comprehensively integrate multiple partners’ perspectives and include a mixed-methods research design to better triangulate the data, particularly since literature shows that the understanding of polyamory within the non-monogamous community is quite broad. For example, interviewing polycules as a small group interview or focus group would allow researchers to gain a broader understanding of perspectives of individuals within these communities.
Other future directions should examine the intersectionality of class (e.g., employment or occupational status; income; socioeconomic status, educational status), geographical location (e.g., rural/urban/suburban, country), and ability status with our participants’ unique lived experiences as these were outside the scope of this study. Doing so will allow for further generalizability of our findings to larger populations.
Conclusion
In this study, we interviewed 26 participants who self-identified as polyamorous to better understand how they navigate safer-sex discussions in their polyamorous relationships. We were also interested in the resulting relational and health outcomes of such discussions. Using sexual script theory, we found that participants used intrapsychic scripts to engage in discussions about safer sex and interpersonal scripts to create boundaries within their relationships around safer-sex practices. Although cultural scripts were less prevalent, participants demonstrated that cultural scripts around frequent STI testing within the polyamorous community may be forming. Findings have implications for open relational communication among social and personal relationships, trust building, and even healthcare messaging around STI testing. This study contributes thus to both theory and practical relationship guidance.
Footnotes
Author contributions
All authors contributed to the material preparation, data collection, and writing of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Our study was approved (Protocol # 2022–0484.2) by the University of Texas at Arlington’s Institutional Review Board (IRB). All participants provide informed consent via an IRB-approved consent document prior to study participation.
Open science statement
As part of IARR's encouragement of open research practices, the authors have provided the following information: This research was not pre-registered. The data used in the research are not available due to privacy and ethical concerns. The materials used in the research are available. The materials can be obtained by emailing
Data Availability Statements
The datasets generated during and/or analyzed during the current study are not publicly available due to privacy concerns.