
Abstract
Social disconnection represents a growing public health concern. While Behavioral Activation (BA), an evidence-based intervention that reduces behavioral withdrawal by increasing engagement in meaningful activities, demonstrates efficacy for depression, its potential for enhancing social connection remains largely unexplored. The purpose of this systematic review was to synthesize current evidence for BA’s impact on social connection and develop a conceptual framework explaining potential mechanisms among individuals across all ages. Following PRISMA guidelines, electronic databases (CINAHL, Embase, PsycInfo, and PubMed Central) were searched for studies published between January 2015 and June 2024 that met the following inclusion: (1) randomized controlled trial or pre-post studies that used BA as a standalone or core intervention component; and (2) reported social connection (functional, structural, and quality-related measures) as a primary or secondary outcome. Two reviewers independently screened articles, extracted data, and assessed quality of the studies. Narrative synthesis was used to synthesize the data. Eight studies met inclusion. BA delivered via telehealth with coaching support produced the strongest and sustained effects. BA improved functional dimensions of social connection (loneliness, perceived support) consistently. One study in residential care settings showed null effects, suggesting environmental/contextual moderators may be important. BA shows promise as an intervention for social disconnection, particularly for reducing loneliness and enhancing perceived support. The conceptual framework proposed in this review has identified five potential mechanisms: increased social reinforcement, environmental enrichment, value-based social actions, reduced avoidance, and enhanced social self-efficacy. BA’s adaptability suggests potential for scalable implementation. However, limited structural and quality outcome assessment and measurement heterogeneity limit definitive conclusions. Future research should employ comprehensive social connection measures, test proposed mechanisms, and optimize BA protocols specifically for social connection.
Keywords
Introduction
Social connection—a multidimensional construct encompassing functional (perceived and received social support, loneliness), structural (social network size, marital status, social isolation), and quality-related (relationship satisfaction, conflict) dimensions of social relationships (Holt-Lunstad, 2024)—is now widely recognized as a critical determinant of human well-being and survival, affecting physical and mental health across the lifespan (Lutz et al., 2021; Necka et al., 2021; Umberson & Montez, 2010). In contrast, the absence of meaningful social connection—or social disconnection— is an umbrella term encompassing deficits across multiple domains of social connection, often measured through loneliness and social isolation. Loneliness refers to the subjective feeling of being alone or disconnected (Perlman & Peplau, 1981), whereas social isolation reflects the objective lack of social contacts, ties, or interactions (Cudjoe et al., 2020). While conceptually distinct, these constructs often co-occur and are jointly associated with poor health outcomes (Holt-Lunstad, 2024).
Recent epidemiological and interdisciplinary reports have positioned social connection alongside nutrition, exercise, and sleep as fundamental pillars of public health (Holt-Lunstad, 2023; Office of the Surgeon, 2023; WHO, 2024). Extensive evidence links higher levels of social connection with reduced risk, while social disconnection increases the risk for premature mortality and detrimental health (Farrell et al., 2022; Holt-Lunstad et al., 2015; National Academies of Sciences & Medicine, 2020; Proctor et al., 2023; Office of the Surgeon, 2023). In light of this, there is growing attention to developing national health guidelines and scalable interventions that target social connection (Holt-Lunstad, 2023; Merlo et al., 2025).
A deeper understanding of the potential mechanisms underlying social connection has also emerged in the current scientific literature. Behavioral research highlights the role of the brain’s reward systems, social cognitive processes, and the regulation of emotions in the formation and maintenance of social bonds (Delgado et al., 2023). For instance, even transient social contact with strangers has been shown to boost mood and well-being (Van Lange & Columbus, 2021), yet people often underestimate the value of these exchanges and avoid initiating them often due to the role of faulty social cognitions.
Faulty social cognitions—including overestimations of social risk, underestimations of others’ interest, and diminished perceptions of empath— may shape whether people initiate or avoid social connection (Epley et al., 2022; Pei et al., 2025). Epley et al. (2022) describe this phenomenon as undersociality, a form of miscalibrated social cognition in which individuals hold inaccurate beliefs about how others perceive them or how beneficial social engagement will be. These distorted expectations can create self-reinforcing cycles of avoidance, further reducing opportunities for social reinforcement and heightening social isolation (Pei et al., 2025). For example, Rodriguez et al. (2025) found that how individuals interpret solitude— whether framed as chosen (solitude) or imposed (rejection)—profoundly shapes their experience of loneliness.
Beyond the psychological domain, substantial evidence from relationship science and health psychology shows that social connection also influences health through biobehavioral and neuroendocrine pathways. Specifically, emotionally supportive relationships can buffer stress responses (e.g., reducing HPA axis activity), regulate neuroendocrine function (e.g., cortisol, oxytocin), and promote healthy routines such as regular sleep and physical activity (Delgado et al., 2023; Proctor et al., 2023). Given these multiple pathways, interventions like Behavioral Activation (BA) that simultaneously target behavioral engagement, and the cognitive antecedents of social withdrawal are especially promising. By helping individuals re-engage in valued, pleasurable, and interpersonal activities, reducing avoidance, and reshaping individuals’ beliefs about their capacity for meaningful connection, BA may not only reduce social disconnection but also initiate downstream improvements in mental and physical health via these intertwined pathways.
BA, originally developed as a psychotherapy for depression (Sturmey, 2009), offers a theoretically grounded and potentially adaptable approach to enhancing social connection. BA is rooted in the principles of the behavioral theory of depression by Lewinsohn (1975), which posits that depression emerges from diminished response-contingent positive reinforcement. The theory describes a self-perpetuating cycle: depressed individuals disengage from rewarding activities, experience reduced pleasure, which further increases depression and promotes additional withdrawal (Lewinsohn, 1974). BA disrupts this cycle by systematically increasing engagement in personally meaningful and reinforcing activities, thereby restoring the positive feedback loop between behavioral activation and mood improvement.
The evolution of BA as a manualized standalone intervention emerged from component analyses of Cognitive Behavioral Therapy (CBT). Notably, Jacobson et al. (1996)’s seminal work on dismantling CBT demonstrated that BA alone achieved outcomes equivalent to full CBT protocols for depression. This finding catalyzed extensive validation across diverse populations and contexts, establishing BA as a parsimonious, flexible, and cost-effective intervention (Lejuez et al., 2001). More recent BA protocols have streamlined delivery from the original 20+ sessions to approximately 10 sessions while maintaining efficacy (Lejuez et al., 2011). This contemporary approach involves individualized, collaborative approach wherein trained therapists guide clients through systematic identification of value-driven goals and implementation of structured activity monitoring and scheduling.
There are several therapeutic modalities that might be suitable to address social connection, including CBT, interpersonal therapy (IPT), and mindfulness-based approaches. But these do not offer the same degree of simplicity and scalability as BA. CBT and IPT, for example, often require extensive training, longer treatment durations, and a focus on internal cognitive restructuring or relationship dynamics, which may limit their adaptability in low-resource settings. In contrast, BA is grounded in a straightforward principle and emphasizes re-engagement with value-aligned and positively reinforcing activities, particularly those involving social interaction. This makes BA especially well-suited to targeting behavioral pathways to social connection deficits—helping individuals rebuild social routines, test assumptions about others’ responsiveness, and experience success in interpersonal engagement. Moreover, BA places active emphasis on observable behavior change and measurable social outcomes (e.g., frequency of contact, participation in group activities, relationship quality). Through a structured process, BA equips individuals with skills such as activity monitoring (to identify patterns of avoidance and low-reward behavior), values clarification (to align actions with personally meaningful domains like friendship or family), and activity scheduling (to increase participation in socially meaningful routines).
Additional components such as graded task assignment, behavioral experiments to test maladaptive social assumptions, and problem-solving strategies to overcome logistical or emotional barriers support incremental progress toward stronger social connection. These BA techniques help develop social self-efficacy, emotional regulation in interpersonal contexts, and consistent engagement in connection-promoting behaviors. Because of its simplicity, focus on observable behavior change, and flexible format, BA can be readily adapted for delivery across diverse populations, including older adults, young adults, and individuals managing comorbid health conditions.
Given these strengths, BA represents a particularly promising approach to promoting social connection in diverse settings. Following widespread disruptions to social dynamics during the COVID-19 pandemic and rising national and global attention to the health consequences of social disconnection (Office of the Surgeon, 2023; WHO, 2024), there is a pressing need to identify scalable and theory-driven strategies for strengthening social connection. While BA has demonstrated robust effects in reducing depressive symptoms, its potential for enhancing structural, functional, and perceived dimensions of social connection has not been synthesized or conceptually clarified. Several trials have reported secondary improvements in social outcomes rather than primary endpoints following BA interventions delivered in clinical populations (e.g., individuals with major depressive disorder, older adults with chronic illness). However, these social outcomes have not been systematically reviewed. Existing reviews have focused on BA’s impact on depressive symptoms or cognitive functioning, but none have synthesized its role in fostering social connection across diverse populations and settings. A systematic synthesis is therefore needed to (1) assess the strength and consistency of the evidence base, (2) clarify what dimensions of social connection BA may influence, and (3) explore whether the social benefits of BA are consistent across varying contexts. This review addresses these gaps in the literature by evaluating empirical findings across studies that directly or indirectly measured social connection outcomes in the context of BA and integrating it with a conceptual framework that delineates potential mechanisms through which BA may promote social connection across diverse populations.
Methods
Search strategy and study selection
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A comprehensive literature search was conducted in June 2024 across four electronic databases: CINAHL, Embase, PsycInfo, and PubMed Central. The search strategy combined controlled vocabulary (MeSH terms, subject headings) and free-text keywords related to behavioral activation (e.g., “behavioral activation therapy,” “BA intervention”) and social connection (e.g., “loneliness,” “social isolation,” “social support,” “relationship satisfaction”). The complete search strategy for each database is provided in Supplemental Material S1. Additional manual searching was performed using Google Scholar to capture relevant literature or studies not indexed in the primary databases. Reference lists of included studies were hand-searched for additional relevant citations.
Eligibility criteria
We intentionally included studies across all age groups and populations to assess the generalizability and lifespan relevance of BA. Studies were included if they met the following criteria: (1) peer-reviewed empirical studies published in English from January 2015 and June 2024. This timeframe (2015–2024) was selected to capture trials implemented after the formal dissemination of BA as a standalone treatment and to reflect increased interest in social connection interventions before and after the COVID-19 pandemic; (2) implemented BA as either a standalone intervention or core component (namely, activity monitoring, values-based goal setting, and activation) of a multimodal intervention; (3) employed randomized controlled trial (RCT) or pre-post study designs to examine both early-stage and fully developed interventions; and (4) reported at least one quantitative outcome measure of social connection (loneliness, social isolation, social support, relationship quality). Given the emerging nature of this literature, both full-scale trials and pilot/feasibility studies were included to capture the insights of evolving intervention approaches. Studies were excluded at the screening phase if they were: (1) reviews, meta-analyses, reports, or commentaries; (2) conference abstracts or proceedings without full results; (3) protocol papers without outcome data; (4) dissertations, theses, or grey literature (e.g., non-peer reviewed materials); or (5) studies where BA was not clearly identifiable as a distinct intervention component.
Screening and selection process
Following duplicate removal using EndNote X20, two reviewers (EM and ML) independently screened titles and abstracts using Covidence systematic review software. Studies meeting initial screening criteria underwent full-text review by the same reviewers. Discrepancies were discussed and resolved collaboratively. In two instances where consensus could not be reached, a third reviewer (MY-J) was consulted and adjudicated the final inclusion decision. Overall, reviewer agreement was high across all screening phases.
Data extraction and quality assessment
A standardized data extraction form was developed and piloted on three randomly selected studies. Two reviewers independently extracted the following data: (1) study characteristics (authors, year, country, design); (2) participant characteristics (sample size, age, clinical population, recruitment setting); (3) intervention details (BA protocol, duration, number of sessions, delivery format, therapist qualifications); (4) comparison conditions; (5) social connection measures and assessment timepoints; and (6) relevant outcomes and effect sizes when reported. Study quality was independently assessed by two reviewers using the Joanna Briggs Institute (JBI) Critical Appraisal tool (Barker et al., 2023), selected for their design-specific criteria. The JBI tools evaluate methodological rigor across domains, including randomization, blinding, outcome measurement, and statistical analysis. Any discrepancies between raters were resolved via inter-rater discussion or by involving a third reviewer.
Data synthesis and framework development
Due to substantial heterogeneity in intervention protocols, populations, comparison conditions, and outcome measures, meta-analysis was not feasible. Instead, a narrative synthesis was employed (Popay et al., 2006). Following Popay et al.’s narrative synthesis guidance, we conducted (1) preliminary organization of results by social connection dimensions (functional, structural, and quality), (2) textual narrative description of study characteristics, BA components, and outcomes, and (3) grouping and tabulation of findings based on presence or absence of statistically significant effects. Using the data extraction form, we first created an evidence table summarizing study characteristics and findings, which were then used to identify emergent patterns across studies regarding BA components most relevant to social connection outcomes. We then explored how intervention characteristics (e.g., format, duration, delivery mode) may relate to observed social connection outcomes. Based on this synthesis, we then developed a conceptual framework through an iterative process. Initial framework components were derived from identified patterns in the data, then refined through team discussion and comparison with existing theoretical models of both BA and social connection. The resulting framework delineates proposed mechanisms through which BA influences social connection and identifies opportunities for intervention optimization. These steps facilitated the synthesis of heterogeneous outcomes in the absence of meta-analysis.
Results
Figure 1 provides PRISMA flow diagram (Page et al., 2021) for the literature review screening and selection process. The systematic search yielded 220 citations initially, of which 218 underwent title/abstract screening after duplicate removal. Following a full-text review of 29 articles, eight studies met the inclusion criteria. PRISMA 2020 flow diagram.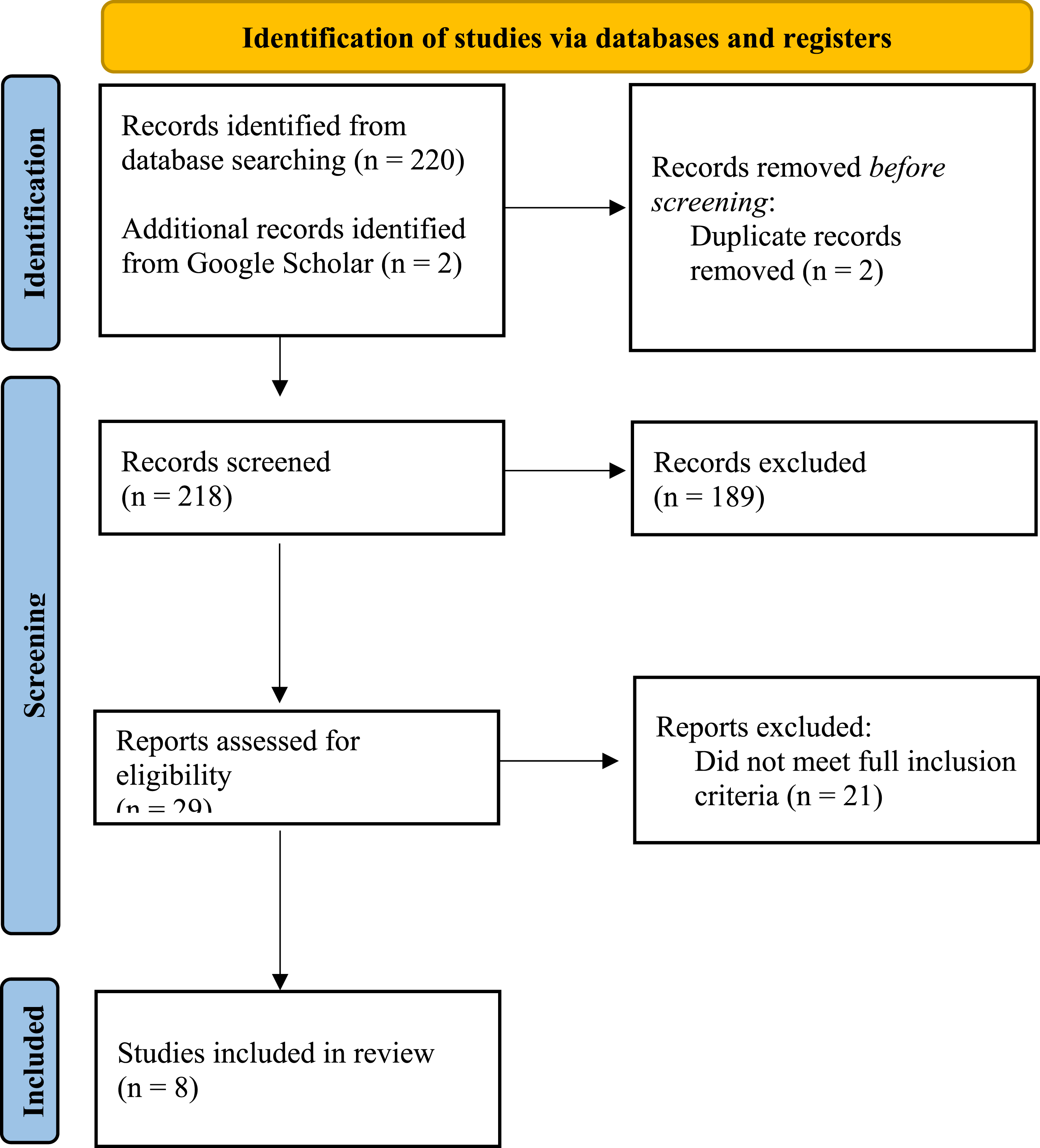
While pre-post studies were eligible, none met inclusion criteria after full-text review. All included studies were randomized controlled trials (RCT). According to JBI Critical Appraisal criteria, there were consistent limitations related to blinding across all studies—neither participants nor interventionists could be blinded due to the active nature of BA interventions (Figure 2). As shown in Figure 2, all studies reported using appropriate trial designs and statistical analyses (Items 11–13). Randomization procedures were clearly described in all studies (Item 1), but allocation concealment (Item 2) was not reported in more than half (n = 5) of the studies. Outcome measurement was consistent across studies as all studies used valid and reliable outcome measures (Items 8–9) across treatment groups. Blinding of participants (Item 4), interventionists (Item 5), and outcome assessors (Item 7) was often not feasible due to the behavioral nature of BA interventions, and thus was mostly not reported, reflecting challenges in behavioral intervention trials. Only four studies reported blinding outcome assessors. Overall, all studies showed low risk on randomization procedures, baseline comparability, and statistical analysis, but most had higher risk regarding blinding and allocation concealment. JBI quality appraisal.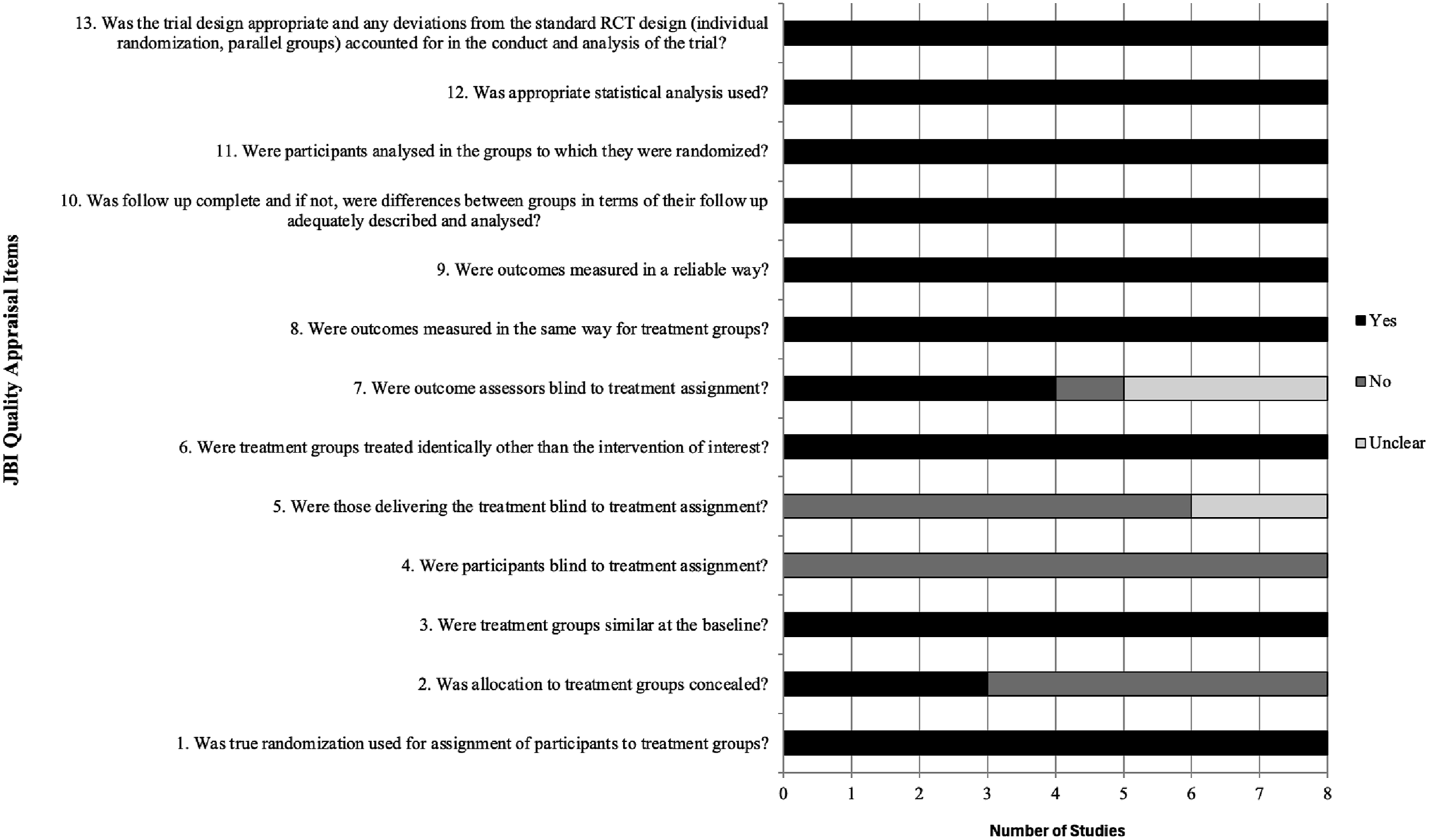
Sample characteristics and settings
Characteristics of included studies (in chronological order).
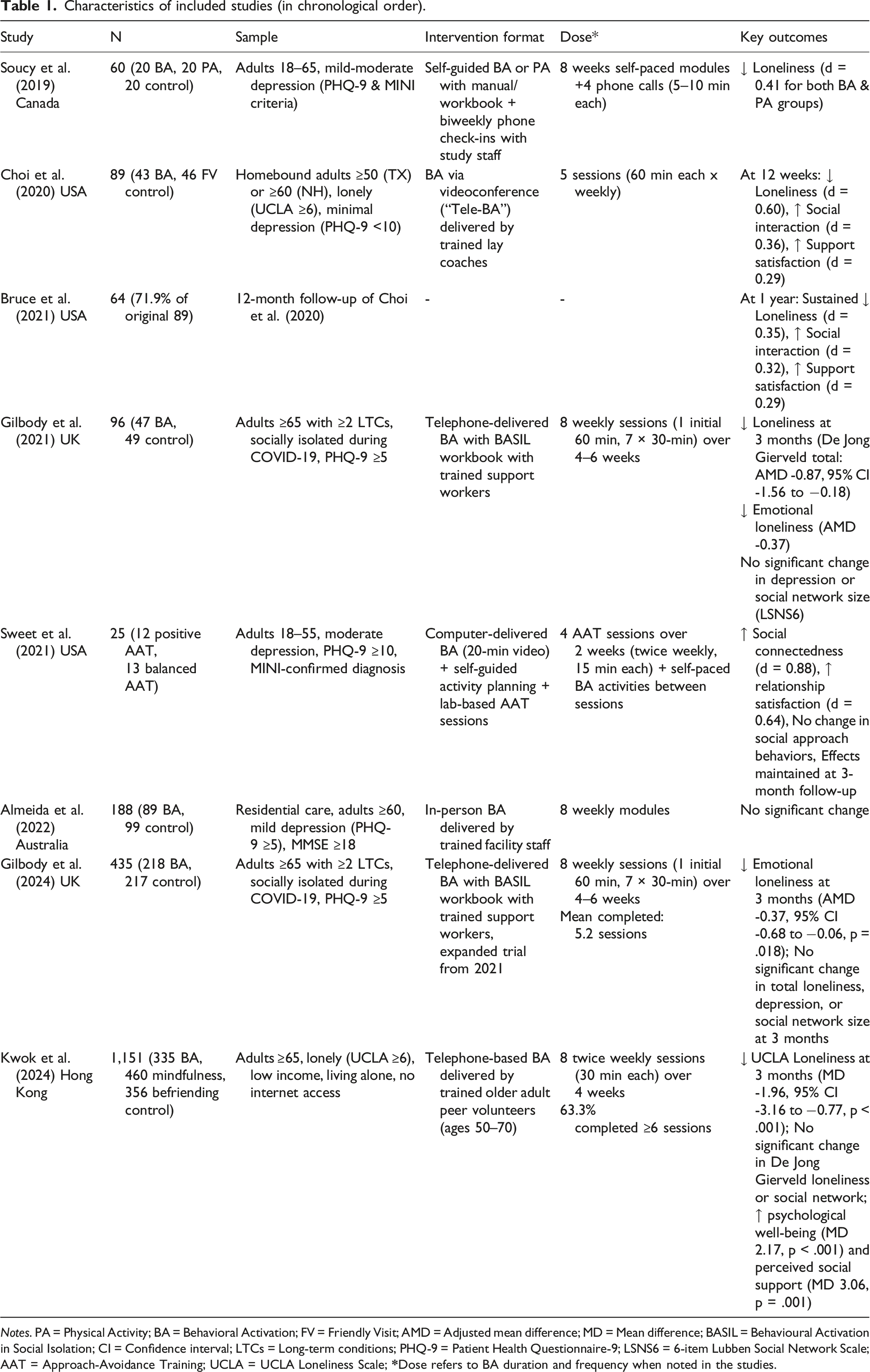
Notes. PA = Physical Activity; BA = Behavioral Activation; FV = Friendly Visit; AMD = Adjusted mean difference; MD = Mean difference; BASIL = Behavioural Activation in Social Isolation; CI = Confidence interval; LTCs = Long-term conditions; PHQ-9 = Patient Health Questionnaire-9; LSNS6 = 6-item Lubben Social Network Scale; AAT = Approach-Avoidance Training; UCLA = UCLA Loneliness Scale;
Intervention characteristics
BA interventions demonstrated considerable heterogeneity in delivery format, duration, and intensity. Three primary delivery modalities emerged: (1) Telehealth-delivered BA. Five studies employed trained therapists or laypersons delivering intervention sessions via telephone or videoconferencing, with sessions ranging from 30-60 minutes. Notably, both the BASIL (Gilbody et al., 2021, 2024) and Tele-BA (Bruce et al., 2021; Choi et al., 2020; Kwok et al., 2024) explicitly incorporated social reconnection goals within their BA frameworks. Interestingly, one study (Kwok et al., 2024) utilized peer volunteer model using older adults aged 50–70 with shared lived experience to deliver Tele-BA to their peer participants. (2) Digitalized self-administered BA. Two studies utilized online modules that combined BA with complementary interventions, such as approach-avoidance training (Sweet et al., 2021) or physical activity promotion (Soucy et al., 2019). These interventions (2–8 weeks) emphasized self-directed learning. (3) In-person BA. A study by Almeida et al. (2022) implemented BA within residential care facilities through en-housed mental health counselor staffs delivering 8 weekly modules over 8–12 weeks to their residents.
The heterogeneity of control conditions across the eight included studies provides important insights into BA’s specific versus non-specific effects. Three distinct control approaches emerged: waitlist/usual care (n = 4) and active controls providing social contact without BA techniques (n = 3), with one without a true control group. The BASIL trials (Gilbody et al., 2021, 2024) and Almeida et al. (2022) employed usual care controls, where participants continued receiving standard primary care or facility services without additional intervention. Soucy et al. (2019) implemented a three-arm design comparing BA and physical activity (PA) interventions against a waitlist control, with both BA and PA interventions showing similar improvements in loneliness compared to the control group. Choi et al. (2020) and Bruce et al. (2021) utilized “Friendly Visiting” via teleconference as an active control, providing equivalent therapist contact time and social interaction but without BA’s structured techniques or skill development. This design allows isolation of BA’s specific behavioral mechanisms from the non-specific benefits of increased social contact. Kwok et al. (2024) employed the most rigorous design with a three-arm trial comparing BA to both befriending (active control providing emotional support without skills training) and mindfulness, enabling direct comparison of different therapeutic approaches. Sweet et al. (2021) compared two active versions of their combined BA + AAT intervention (approach-positive versus balanced AAT) without a true control group, limiting conclusions about efficacy but establishing feasibility.
Measures and dimensions of social connection
Social connection measures across studies.
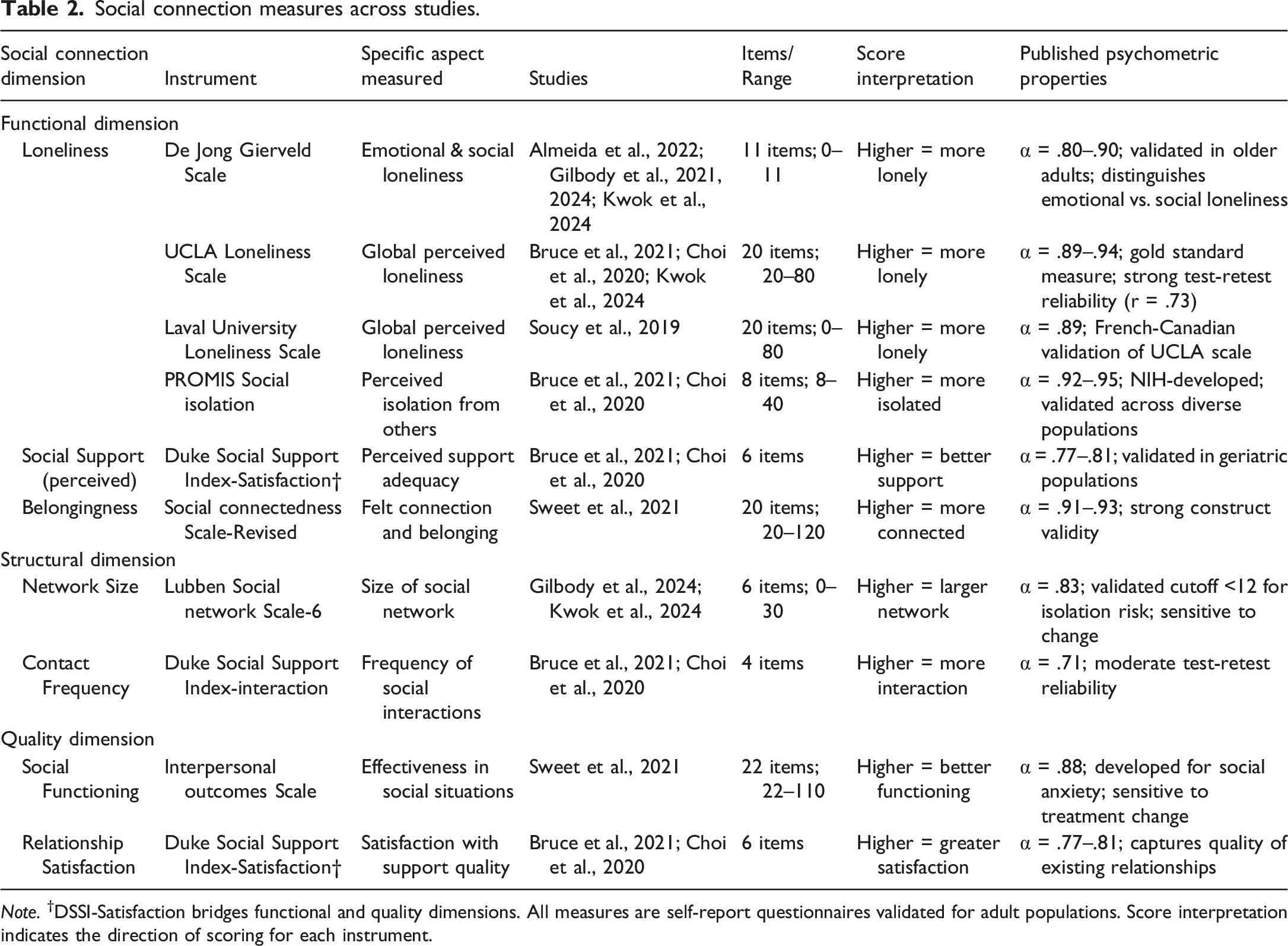
Note. †DSSI-Satisfaction bridges functional and quality dimensions. All measures are self-report questionnaires validated for adult populations. Score interpretation indicates the direction of scoring for each instrument.
Synthesis of the findings
Seven of eight studies (87.5%) demonstrated statistically significant reductions in loneliness following BA interventions. Effect sizes varied considerably with large effects shown with Tele-BA. For instance, Tele-BA produced Cohen’s d = 0.83 at 6 weeks, sustained at d = 0.68 at 12 months, relative to Tele-FV or friendly visit as an active control condition (Bruce et al., 2021; Choi et al., 2020). Similar patterns were shown with Kwok et al. (2024) where it showed d = 0.45 at 3 months compared to active control condition (friendly telephone call). Moderate effects were shown with BASIL interventions, which yielded d = 0.45–0.52 across follow-up periods compared to their usual care conditions (Gilbody et al., 2021, 2024). Small-to-moderate effects were demonstrated with digital interventions, d = 0.32–0.41 (Soucy et al., 2019; Sweet et al., 2021). The single null finding (Almeida et al., 2022) occurred in residential care settings, suggesting potential contextual moderators of BA effectiveness.
Studies assessing perceived social support consistently reported improvements. Choi et al. (2020) found significant increases in both social interaction frequency (d = 0.51) and satisfaction with support (d = 0.43) compared to active control condition. Gilbody et al. (2024) and Kwok et al. (2024) found no significant change in social network size despite improvements in loneliness, suggesting BA may primarily influence subjective rather than objective social connection dimensions.
Synthesized conceptual framework
Based on our synthesis, we propose a conceptual framework delineating five interconnected mechanisms of action through which BA affects social connection outcomes (Figure 3). The key moderating factors include individual characteristics (e.g., age, socioeconomic status, psychosocial factors, health conditions), contextual factors (e.g., community-dwelling, residential care setting, institutionalized), and the intervention factors (e.g., intervention format/delivery –digital self-guided vs. telehealth vs. in-person; duration (2–12 weeks); and inclusion of explicit social goals). This framework is grounded in the theoretical underpinnings of the behavioral theory of the BA (Lewinsohn, 1974), that extends beyond mood regulation, incorporates empirical findings from the included studies in this review, and identifies areas for further evaluation. This proposed framework is by no means exhaustive, but it provides a starting point to encourage further discussions and research in this area. Conceptual Framework of Behavioral Activation for Social Connection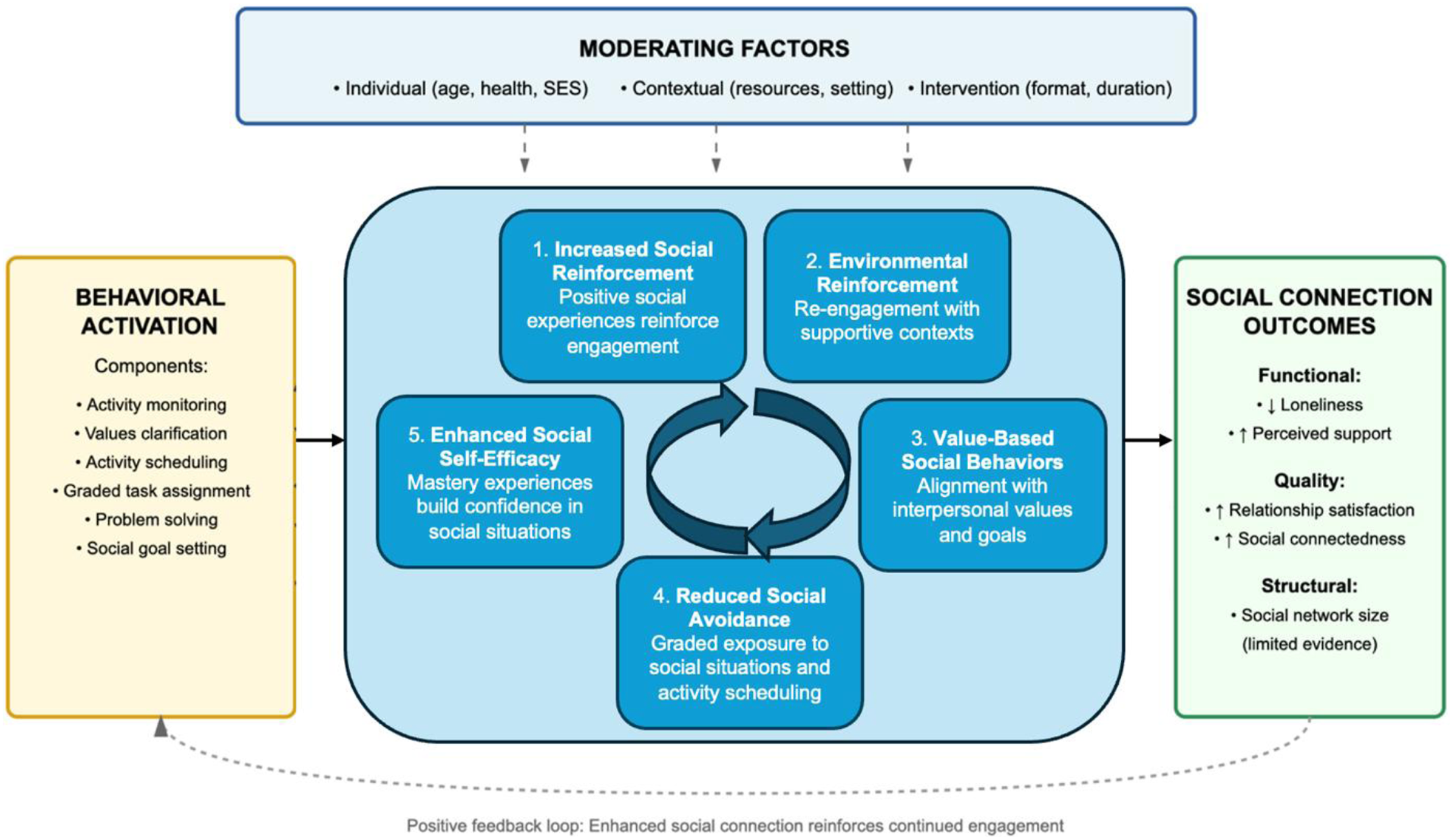
Mechanism 1: Increased social reinforcement
Consistent with Lewinsohn’s (1974) model, BA facilitates re-engagement with socially reinforcing experiences/activities. By systematically scheduling social activities and monitoring their impact, individuals experience immediate positive reinforcement from social interactions, increasing the likelihood of sustained engagement. This aligns with the operant model of behavior (Staddon & Cerutti, 2003) or operant conditioning (Skinner, 1937), which posits that behaviors are learned through consequences and that positively reinforced behaviors or actions are more likely to be repeated (increased frequency).
Mechanism 2: Environmental reinforcement
The operant model of behavior suggests that behavior is shaped and maintained by the availability of reinforcing experiences from one’s environment. Socially supportive environments (e.g., community centers, religious organizations, support groups, family networks) provide opportunities for social interactions and relationship formation. BA helps individuals identify and re-engage with environments rich in social reinforcement, thereby enhancing both the quantity and quality of social interactions. For example, the BASIL pilot trial (Gilbody et al., 2021) was implemented as a response to the isolation brought by the COVID-19 pandemic, which greatly impacted people’s social environments. The BASIL sought to help participants re-engage with rewarding activities that would reduce loneliness despite the mandatory isolation precaution.
Mechanism 3: Activation of value-Based social Behaviors
Central to BA’s effectiveness is the alignment of activities with personal values, i.e., activities that provide meaning. Social connection is often a core life value, even for individuals who have withdrawn from social relationships. BA encourages individuals to clarify their values related to relationships, community, and belonging, and then systematically incorporate actions that reflect those values. When individuals identify interpersonal connection as a core value, BA provides structured pathways to translate these values into concrete social behaviors, enhancing the meaningfulness and sustainability of social engagement. As an example, participants in Tele-BA were assisted by the layperson coach in identifying value-based activities to reduce barriers to social connection. They were then assisted in developing goals and coached through the process of engaging in those goals, which ultimately resulted in greater social interactions in six weeks (Choi et al., 2020).
Mechanism 4: Reduced social Avoidance and withdrawal
Behavioral theories emphasize that individuals often avoid situations perceived as stressful or aversive, leading to behavioral avoidance (Krypotos et al., 2015). Behavioral avoidance maintains social isolation by preventing individuals from experiencing potentially rewarding social interactions. BA systematically addresses this through graded exposure and structured activity scheduling, progressively building tolerance for social discomfort while establishing positive associations with interpersonal contact. Sweet et al. (2021) provide unique insight into this mechanism by combining BA with approach-avoidance training (AAT). In their framework, individuals with depression exhibit both implicit (automatic) and explicit (conscious) avoidance tendencies that diminish engagement with potentially rewarding social activities. Their intervention targeted these dual pathways—AAT modified implicit approach-avoidance biases through computerized training, while BA addressed explicit avoidance through conscious behavioral planning. This combined approach produced significant improvements in both social connectedness (d = 0.92) and interpersonal functioning, suggesting that addressing avoidance at multiple levels may enhance outcomes. The success of this dual-targeting approach highlights an important refinement to our understanding of BA’s mechanisms. While traditional BA focuses on conscious behavioral choices, the integration with AAT suggests that addressing automatic avoidance responses may amplify effects on social connection. This finding aligns with dual-process theories of behavior change (Houlihan, 2018) and suggests future BA protocols might benefit from incorporating implicit bias modification techniques alongside traditional activity scheduling.
Mechanism 5: Improved social self-efficacy and mastery
BA’s structured approach to goal achievement builds social self-efficacy through progressive mastery experiences. By dismantling complex social goals into manageable steps and systematically tracking progress, individuals develop confidence in their ability to navigate social situations and engage in social relationships successfully. Soucy et al. (2019) explicitly demonstrated this mechanism by having participants create hierarchies of “challenging personally relevant objectives” that progressively increased in difficulty. This graduated approach produced measurable increases in self-efficacy that not only emerged during the intervention but continued to strengthen post-intervention, suggesting a self-reinforcing process. The sustained improvement indicates that mastery experiences during BA may fundamentally shift individuals’ beliefs about their social capabilities. However, while Almeida et al. (2022) employed a similarly structured eight-module progression, the study failed to produce significant social connection improvements, possibly because study modules emphasized general BA rather than social-specific goals. This difference suggests that building generic self-efficacy may not be sufficient and that the mastery experiences must specifically involve social challenges to translate into improved social connection. The role of self-efficacy as a mechanism is further supported by theoretical models positing that loneliness is maintained partly through low social self-efficacy, which leads to self-protective withdrawal (Masi et al., 2011). By providing structured opportunities for social success, BA may interrupt this cycle, replacing expectations of social failure with evidence of social competence. This mechanism may be particularly important for sustaining long-term gains, as enhanced self-efficacy may allow individuals to continue pursuing social opportunities independently after intervention completion.
Potential outcomes on social connection
While not all studies observed and/or assessed changes in structural dimension of social connection, many demonstrated improvements in subjective/functional dimension of connection (e.g., feeling less lonely or more supported). This suggests that BA may primarily influence functional dimension of connection, which may (or may not) facilitate structural change (e.g., forming new relationships). This measurement imbalance suggests the current evidence base solely addresses whether BA reduces subjective feelings of disconnection rather than whether it changes actual social behavior or relationship structures. This limitation should be explicitly acknowledged when interpreting the framework and highlights the need for more comprehensive assessment in future studies.
Discussion
This systematic review provides initial evidence that BA, despite its origins as a depression treatment, demonstrates promise as an intervention for enhancing social connection across diverse populations. Seven of eight studies reported significant improvements in social connection outcomes, with effects most pronounced for subjective/functional dimensions (loneliness, perceived support). The consistency of positive findings on available dimensions of social connection across the studies varied in the delivery formats, from lay-coached telehealth to self-administered digital platforms, which suggests that BA’s core mechanisms may be robust to adaptation while highlighting important contextual factors for its effectiveness.
The proposed conceptual framework advances our understanding of how BA may influence social connection through multiple, potentially synergistic pathways. While Lewinsohn’s (1974) original behavioral theory emphasized the role of positive reinforcement in mood regulation, our synthesis suggests these same principles extend naturally to social domains. The mechanism of increased social reinforcement appears particularly salient—as individuals schedule and complete social activities that are meaningful to them, they experience interpersonal rewards and self-efficacy that strengthen approach behaviors while weakening avoidance patterns.
Across the studies reviewed, common BA components included activity monitoring, value clarification, identifying avoidance patterns, setting behavioral goals, and scheduling reinforcing activities—with a focus on increasing social and interpersonal engagement. Notably, the trial demonstrating the strongest effect (Bruce et al., 2021; Choi et al., 2020) explicitly incorporated social goals within their BA protocols, suggesting that intentional targeting of social behaviors may amplify outcomes beyond what occurs through traditional BA approach. These findings align with goal-setting theory (Locke & Latham, 2002) and underscore the feasibility of adapting BA to explicitly target social goals rather than assuming social benefits will emerge secondarily from mood improvement.
Several studies also included graded task assignment, where individuals gradually built confidence by initiating lower-stakes social interactions before progressing to more complex social goals. These techniques are particularly powerful because they not only increase the frequency of social contact but also help shift underlying cognitive patterns that maintain social withdrawal—such as fear of rejection or assumptions about others’ availability. The finding that both BA and physical activity reduced loneliness in Soucy et al. (2019) raises important questions about common/broad versus specific factors. While structured activity engagement may provide non-specific benefits for social well-being, BA’s incorporation of values clarification, systematic monitoring, and explicit problem-solving around barriers may confer additional advantages. Future dismantling studies are needed to isolate these components to optimize BA’s effect on social connection.
The differential impact on dimensions of social connection warrants careful consideration. While perceived loneliness and support showed consistent improvement, only Gilbody et al. (2024) and Sweet et al. (2021) assessed network size and number of social activities, respectively, finding no significant change in the structural aspect of connection. This may suggest that BA primarily influences the subjective experience and quality of existing relationships and that BA’s effect on network expansion may be limited or slower to manifest. Such findings echo broader literature that distinguishes between perceived and received support (Haber et al., 2007), where subjective appraisals of support predict health outcomes more strongly than objective measures. More studies are needed to assess the multidimensional nature of social connection to fully understand the BA’s capacity in improving varied dimensions of social connection in the short- and long-term. In addition, the null finding in Almeida et al.'s (2022) residential care study provides crucial insight into potential structural and contextual conditions for BA effectiveness. The constrained social environment of institutional settings, the advanced age of participants (mean age 83.9 years), and the delivery through facility staff rather than dedicated interventionists may explain the null findings. These suggest that environmental constraints and implementation fidelity may significantly moderate BA’s impact on social connection.
The heterogeneity in delivery formats offers both challenges and opportunities. Telehealth delivery with human support (whether therapist or layperson) produced the most consistent effects, potentially because this format combines structured accountability with modeling of social interaction through the therapeutic relationship itself. In contrast, purely self-administered digital interventions showed small effects. This gradient suggests that the interpersonal context of BA delivery may be an active ingredient. Importantly, the sustained benefits observed at one-year follow-up (Bruce et al., 2021) distinguish BA from other psychosocial interventions where effects often attenuate post-intervention. This sustaining effect may reflect BA’s emphasis on building self-sustaining behavioral patterns rather than requiring ongoing professional support, which is a critical consideration for scalability and implementation.
BA offers distinct advantages over existing social connection interventions. Unlike social skills training, which assumes deficits in interpersonal competence, BA works within individuals’ existing capabilities while addressing motivational and avoidance barriers. While some interventions targeting various dimensions of social connection emphasize group-based bonding or cognitive restructuring (Masi et al., 2011), BA mobilizes participants through personally meaningful, real-world actions. This may increase ecological validity and adaptability to diverse settings, including primary care and community-based models, as well as to those with cognitive impairments. The adaptability of BA—via telehealth, lay facilitation—also positions it as a low-cost and scalable strategy across diverse populations and settings without requiring extensive interventionist training or group facilitation skills needed for many social interventions. Its use in older adults with chronic conditions (Gilbody et al., 2021, 2024), low income (Kwok et al., 2024), and those that are homebound (Bruce et al., 2021; Choi et al., 2020), illustrates the potential for its reach among populations most vulnerable to isolation.
Implications of BA extend beyond clinical settings. At a population level, policies and public health strategies could draw from BA principles to promote structural supports for behavioral engagement. For example, community-based BA-informed programs could be developed to help individuals identify and re-engage in social routines disrupted by isolation, unemployment, caregiving burdens, or health challenges. Workforce development efforts—particularly in peer-support, lay health worker, and behavioral health coaching models—could integrate core BA techniques to address loneliness and disconnection across diverse populations. This aligns with the guidelines proposed by Holt-Lunstad (2023), which emphasize the need for evidence-based strategies to increase social connection at individual, community, and societal levels. By highlighting practical behavioral skills (e.g., scheduling social activities, problem-solving avoidance, and reinforcing progress), BA offers a translatable framework that can inform public health messaging, digital interventions, and policy toolkits aimed at preventing the epidemic of disconnection.
Several limitations warrant cautious interpretation of the findings drawn from our review. The small number of studies, combined with substantial heterogeneity in study populations, control conditions (e.g., usual care, attention control, psychoeducation), interventions, and outcome measures, precludes definitive statements about BA’s effectiveness for social connection and complicates direct comparisons and generalization. Publication bias may influence the observed patterns, as studies with null or unfavorable results may be underreported. The restriction to English-language publications from the past decade may have excluded relevant international research or earlier foundational work. Most critically, no studies explicitly tested the proposed mechanisms, leaving our conceptual framework largely theoretical rather than empirically validated. Although overall methodological rigor of the included studies as observed, common risks of bias—particularly in blinding procedures and allocation concealment—were evident and may have affected internal validity. The reliance on self-report measures across all studies raises concerns about social desirability bias. Future research should incorporate objective behavioral indicators (e.g., smartphone-based social contact monitoring) and biomarkers of social connection (e.g., inflammatory markers, cortisol patterns) to triangulate subjective reports. Additionally, ecological momentary assessment could capture real-time social experiences rather than retrospective recalls. The measures employed across studies predominantly captured functional dimensions of social connection, particularly loneliness and perceived support, while structural and quality dimensions remained largely unexamined. As such, conclusions about BA’s impact should be interpreted within this scope and not assumed to reflect structural changes in social networks without further evidence. This measurement bias limits conclusions about BA’s impact on the full spectrum of social connection (Holt-Lunstad, 2024) and highlights the need for conceptual clarity in future studies and to fully capture all aspects of social connection. Finally, while BA shows promise for enhancing certain dimensions of social connection, this review was not designed to compare BA’s effects on social connection outcomes against other evidence-based interventions (e.g., CBT, IPT). Future research is needed to empirically test whether BA offers unique advantages or operates through distinct mechanisms compared to other strategies.
Methodological improvements in future trials should include: (1) standardized core outcome measures to allow for cross-study comparison and eventual meta-analysis; (2) longer follow-up periods to assess maintenance of gains; (3) formal mediation analyses to test proposed mechanisms; and (4) implementation-effectiveness hybrid designs that simultaneously evaluate clinical outcomes and real-world feasibility. Beyond addressing methodological limitations, several substantive questions merit investigation. First, optimal matching of BA variants to individual characteristics remains unexplored. For example, younger adults may benefit more from digital delivery while older adults may require human support, but empirical testing of such moderation hypotheses is needed. Second, the integration of BA with other evidence-based components (e.g., mindfulness, compassion-focused techniques) may enhance outcomes but requires careful evaluation to avoid therapeutic dilution. Finally, implementation science approaches should examine how BA for social connection can be integrated into existing service structures. Primary care, where many lonely individuals first present, offers one promising avenue. Training medical assistants or community health workers to deliver brief BA could extend reach while maintaining fidelity to core components.
Conclusions
This systematic review provides promising initial evidence that BA can effectively enhance social connection, particularly subjective experiences of loneliness and social satisfaction. However, its effects on actual social engagement behaviors or on more structural dimensions of social connection remain less clear. The proposed conceptual framework offers a theoretical roadmap for understanding BA’s mechanisms of action and optimizing its application to social connection outcomes. While important questions remain about optimal delivery, mechanisms of change, and moderating factors, the current evidence suggests BA as a scalable, adaptable intervention well-suited to address the growing public health crisis of social disconnection. As many systems seek evidence-based solutions to end the epidemic of loneliness and isolation, BA’s combination of theoretical grounding, empirical support, and implementation feasibility and adaptability positions it as a valuable tool warranting continued development and dissemination.
Supplemental material
Supplement material - Behavioral activation for social connection: A systematic review and synthesized conceptual framework
Supplement material for Behavioral activation for social connection: A systematic review and synthesized conceptual framework by Emily Myers, Michelle Lin, Archana Asundi, Namkee G. Choi, Moka Yoo-Jeong in Journal of Social and Personal Relationships
Footnotes
Acknowledgements
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author contributions
Emily Myers: Methodology, Formal analysis, Visualization, Writing - original draft, Writing - review & editing, Project administration
Michelle Lin: Data curation, Writing - review & editing, Validation, Project administration
Archana Asundi: Writing - review & editing
Namkee G. Choi: Writing - review & editing
Moka Yoo-Jeong: Conceptualization, Methodology, Investigation, Resources, Writing – original draft, Writing - review & editing, Supervision, Validation, Funding acquisition
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute on Aging K01AG090135 (M.Yoo-Jeong).
Open science statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research are not available as it already reviews on existing studies. The materials used in the research are not available.
Ethical consideration
There are no human participants in this article and informed consent is not required.
Data Availability Statement
This article is a review of previously published studies. All data discussed are available within the cited articles and sources in the reference list. No new datasets were generated or analyzed for this review.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.