
Abstract
In March of 2020, state governments in the United States began implementing stay-at-home orders in an attempt to curtail the spread of COVID-19. As a result, most people experienced a decrease in face-to-face interactions as they limited their participation in social gatherings, travel, and in-person work. Although these orders aimed to stop the spread of COVID-19, a potential unintended consequence of these guidelines was an increase in loneliness, which has several negative mental and physical health consequences. The goals of the present study were to investigate the extent that one’s romantic relationship status and living arrangements affected self-reports of loneliness and to track how self-reports of loneliness changed over the span of 1 month following the first stay-at-home orders in the United States. Participants (N = 311) reported their loneliness at three time points in 2-week intervals. Results showed considerable overlap between living arrangements and romantic relationship status in predicting loneliness; however, it appears that living with another person has a greater protective effect against loneliness compared to relationship status. That is, whereas living with others or being in a romantic relationship both predicted lower loneliness scores, one’s living arrangements accounted for variance in loneliness scores beyond what was accounted for by one’s relationship status. The researcher also explored whether loneliness increased across three time points throughout data collection. Results showed that loneliness levels remained approximately the same across time. An unhypothesized interaction effect did emerge between time and age. Subsequent probing of this interact effects showed that young adults experienced the greatest level of loneliness but this loneliness decreased over the month, whereas older adults experienced less loneliness but experienced a small increase in loneliness over the during this time. Together, these results suggest that certain groups of people were more likely to experience loneliness during the COVID-19 pandemic.
On January 9, 2020 the World Health Organization determined a disease outbreak in Wuhan, China was caused by a novel coronavirus (World Health Organization [WHO], 2020). Approximately 2 months later on March 11, 2020, the WHO declared that the outbreak of COVID-19, the disease caused by the novel coronavirus, was a global pandemic. Researchers determined that this novel coronavirus was easily transmissible from person to person via respiratory droplets produced during breathing, talking, coughing, and sneezing, and therefore recommended people avoid being within six feet of other (Centers for Disease Control and Prevention [CDC], 2020). Within days of the WHO’s pandemic declaration, state governments in the United States began implementing stay-at-home orders and social distancing guidelines in an attempt to curtail the spread of COVID-19. These stay-at-home orders led to decreased population movement and reduced person-to-person contact with those outside of one’s household in the ensuing months (Moreland et al., 2020).
However, prior to the COVID-19 pandemic, the United States was experiencing a loneliness epidemic, with loneliness rates among the U.S. adult population increasing from 54% in 2018 to 61% in 2019 (Cigna, 2020). Because several health detriments correlate with loneliness, including depressive symptoms, suicide ideation, and parasuicidal behaviors, it is unsurprising that Surgeon General Vivek Murthy had previously declared loneliness to be a public health crisis (Murthy, 2017). Whereas loneliness is often combatted or prevented through meaningful social interactions and receiving social support, recommendations for preventing the spread of COVID-19 such as social distancing and stay-at-home orders may have prevented many of these social interactions from occurring in face-to-face settings (Saltzman et al., 2020).
Preliminary research during the COVID-19 pandemic has shown that being under stay-at-home orders leads to greater loneliness (Tull et al., 2020). Therefore, the goal of this study is to identify whether specific life situations made certain individuals particularly susceptible to loneliness during the COVID-19 pandemic. Specifically, the researcher considers how subjective reports of loneliness are affected by people’s romantic relationship status (i.e., whether someone is in a committed romantic relationship) and their living arrangements (i.e., whether someone lives alone or with others). The researcher also explored whether loneliness self-reports changed over a 1-month span during the onset of the stay-at-home orders and social distancing in the United States. The forthcoming literature review overviews the prevalence, causes, and health detriments of loneliness, the importance of meaningful social interactions in combatting loneliness, and why one’s relationship status and living arrangements may be particularly important in attenuating perceptions of loneliness.
Loneliness prevalence and known health detriments
Loneliness is a distressing psychological state in which a person perceives a deficit between their experienced and desired levels of connection, both in terms of quantity and quality (Cacioppo et al., 2006); however, not all experiences of loneliness are the same. Experiencing intermittent loneliness at various points in one’s life is a universal experience (Hawkley & Cacioppo, 2010; Rokach & Bauer, 2004), and as reported by Hawkley and Cacioppo (2010) intermittent loneliness prevalence is highest among adolescents (80%) and the elderly (40%). More concerning, though, is that approximately one in five adults in the United States experience chronic loneliness (i.e., often or always feeling lonely; Ballard, 2019).
Experiencing chronic loneliness is consequential and, as a robust body of research has illustrated, loneliness has detrimental effects on one’s mental and physical health. In terms of mental health, those who are chronically lonely are more likely to experience eating disorders (Levine, 2012), alexithymia (Qualter et al., 2009), and cognitive decline (Gow et al., 2007). Additionally, those who are lonely are more likely to engage in suicide ideation and parasuicidal behavior (Goldsmith et al., 2002; Gow et al., 2007; Stravynski & Boyer, 2001). Loneliness has also been associated with both clinical and subclinical depression (Aylaz et al., 2012; Cacioppo et al., 2006) and recent cross-sectional research conducted in Germany has shown greater reports of depression during the COVID-19 pandemic (Bauerle et al., 2020).
Regarding one’s physical health, lonely individuals experience higher all-cause mortality (Cacioppo et al., 2002; Shiovitz-Ezra & Ayalon, 2010). More specifically, researchers have consistently demonstrated associations between loneliness and cardiovascular issues such as hypertension (Momtaz et al., 2012) and coronary heart disease (Thurston & Kubzansky, 2009), as well as experiencing greater inflammatory responses to stressors and greater likelihood of experiencing sleep dysfunction and fatigue (Hawkley et al., 2010; Jaremka et al., 2013). Given the well documented health detriments of loneliness, and considering chronic loneliness rates were at epidemic levels in the United States prior to the COVID-19 pandemic, it is worth reviewing what predicts loneliness. Doing so may help identify those whose life circumstances may make them particularly susceptible to experiencing greater loneliness, particularly during the COVID-19 pandemic.
Causes and predictors of loneliness
Scholars have identified various causes of loneliness, but perhaps the most compelling reason is that humans possess a fundamental need to belong (Baumeister & Leary, 1995). The crux of this “belongingness hypothesis” is that humans’ well-being is affected by the quantity and quality of meaningful relationships they form and maintain. Thus, a lack of fulfilling social connections often leads to subjective feelings of loneliness (Rokach & Brock, 1996). Furthermore, researchers have established that in-person interactions buffer against loneliness (Pea et al., 2012; Steptoe et al., 2013) and adolescents who lack in-person interaction but engage in high social media usage report particularly high levels of loneliness (Twenge et al., 2019).
An important lingering question, though, is what prevents people from forming and maintaining meaningful relationships? One possibility is that one’s living arrangements (e.g., living alone or with others) may contribute to a lack of opportunity to develop or maintain meaningful relationships through daily in-person interactions. Indeed, prior research has shown that living alone is a consistent predictor of loneliness within elderly populations (Victor et al., 2000), not only in the United States, but across several continents (Savikko et al., 2005; Steed et al., 2007; van Tilburg et al., 2004; Yeh & Lo, 2004). Moreover, in two studies—one with a sample of adults aged 57 or older and the other with a sample of adults aged 65 or older—those who lived with a spouse or romantic partner were significantly less lonely than those who lived alone (Greenfield & Russell, 2011; Sundström et al., 2009).
These findings have also occurred in studies with young adults. For example, a study of college students found that those with roommates were less likely to report loneliness than their counterparts who lived alone, perhaps due to consistently socially engaging with their roommate (Henninger et al., 2016). Finally, prior research has found that women living entirely alone without roommates or pets reported greater loneliness than women who lived with other people or pets (Zasloff & Kidd, 1994). Together, these findings suggest that living with at least one other person combats loneliness by providing an opportunity to consisting engage in social interaction with another person, whether they be a roommate or romantic partner. Therefore, the following is hypothesized.
A lack of social connections may also occur, in part, due to one’s romantic relationship status. Perhaps the most important ongoing, meaningful relationship one experiences is with a spouse or committed romantic partner. In addition to the health promoting effects of marriage (Rook & Zettel, 2005), such long-term committed romantic relationships are particularly potent against feelings of loneliness. This is because these relationships are characterized by “stability, affective concern, and continuation into foreseeable future” (Baumeister & Leary, 1995, p. 500), all of which help meet the need to belong. Unsurprisingly then, loneliness often occurs when one experiences separation from a partner, either through relationship dissolution or death (Rokach & Brock, 1996; Savikko et al., 2005).
However, those who are not recently single may also be more susceptible to feelings of loneliness. Studies have shown higher loneliness rates for elderly people who are single (Steed et al., 2007). Not being in a committed romantic relationship may contribute to some people’s feelings of loneliness because spouses are typically the primary source of social support for those in relationships (Coyne & DeLongis, 1986; Thoits, 1995) and a lack of social support has been associated with loneliness (Floyd, 2014; Rokach, 1985). Together, these findings suggest that being in a romantic relationship combats loneliness. Therefore, the following is hypothesized:
Considering the potential for living alone and not being in a committed romantic relationship to cause greater feelings of loneliness, and considering that prior research has shown that those who live with a spouse or romantic partner are the least likely to experience loneliness (Greenfield & Russell, 2011; Sundström et al., 2009), the following is also predicted.
It is also worth considering how perceptions of loneliness may have changed or remained stable during the months immediately following state governments in the United States implementing stay-at-home orders. Population movement and close contact with others outside of one’s household decreased in places where stay-at-home orders were implemented, at least during the first 2 months following the WHO’s pandemic declaration (Moreland et al., 2020). Given that loneliness is oftentimes the result of not forming or maintaining meaningful social connections (Rokach & Brock, 1996) and that a lack of in-person interaction leads to loneliness (Twenge et al., 2019), it is possible that stay-at-home orders acted as a barrier preventing people from engaging in behaviors that mitigate loneliness. In non-pandemic times, a portion of the population experiencing loneliness would feasibly address their loneliness by seeking out social connection or social support, as prior research has shown these actions to be common ways people address loneliness (Rokach, 1990; Rokach & Brock, 1998). However, with stay-at-home orders in place, loneliness levels may increase due to a sense of both being lonely and not being able to address their loneliness by forming or maintaining relationships through in-person interactions.
Alternatively, the availability of several computer-mediated channels for communicating with others (e.g., video calls, text messages, social media) may have prevented any increases in loneliness during the onset of the pandemic. Prior research has shown that using communicating through computer-mediated communication can provide opportunities for seeking social support (Correa et al., 2013) and can mitigate loneliness and increase perceived social support (Shaw & Gant, 2002). Thus, people may have maintained a level of social connection similar to what they experienced before stay-at-home orders were implemented, maintaining their relationships primarily through computer-mediated channels as opposed to a combination of in-person and computer-mediated interactions. If this were the case, then loneliness levels may have remained relatively stable and unchanged while stay-at-home orders were initially implemented. However, recent research showed that, for younger adults in particular, social media usage increased during the COVID-19 pandemic, which contributed to greater feelings of loneliness compared to older adults (Lisitsa et al., 2020). Given the variety of potential outcomes of stay-at-home orders on experiences of loneliness, the following research question is posed regarding longitudinal changes in loneliness while people were asked to stay-at-home and engage in social distancing. RQ: How, if at all, did loneliness levels change throughout the early months of the COVID-19 pandemic in the United States?
Method
Participants
Study recruitment occurred through multiple avenues. Initially, participants were recruited through a call for participants made on the communication discipline’s listserv: Communication, Research, and Theory Network (CRTNET). Additional participants were recruited through posts on Facebook pages for the National Communication Association and International Communication Association’s Health Communication Divisions and through the researcher’s personal networks. Participants were also recruited through the researcher’s upper-division and graduate-level communication courses—asking students to participate and to share the study with family members and friends. Participants were entered into a drawing for one of twelve $50 Amazon e-gift cards. A total of 485 individuals completed the first survey, 367 completed the second survey (i.e., the first follow-up survey), and 345 completed the third survey. Those who did not participate in all three surveys or who did not provide data on the variables tested in the study’s hypotheses and research question in any of the three surveys were removed from the dataset. Statistical analyses were conducted to determine if those who completed the study significantly differed from those who did not complete all three surveys on each of the study’s variables of interest as well as demographic variables. There were no significant results—suggesting no meaningful difference between those who completed the study and those who did not complete the study.
The final sample was 311 participants ranging in age from 18 to 75 years (M = 35.44; SD = 13.85). Most reported their biological sex as female (n = 248), with 59 identifying as male and 4 not reporting their sex. The majority of the participants were White (66.2%), with other participants identifying as Asian/Pacific Islander (10.6%), Hispanic/Latinx (10.4%), or Black (2.9%). Others reported multiple ethnicities (9.0%), identified as “other” (0.3%) or did not report their ethnicity (0.6%).
Procedure
Participants completed three online surveys administered between March 24 and May 10, 2020. Surveys distribution occurred through Qualtrics and was configured so that follow-up surveys were automatically emailed to participants 2 weeks after they completed the prior survey. Thus, regardless of the specific day that participants completed the initial survey during the timeframe when the initial survey was available, each participant received their first follow-up survey 2 weeks later and the third follow-up survey 2 weeks after completing the first follow-up survey.
In the initial survey, participants completed measures of trait-level loneliness, extroversion, and affection deprivation. Participants also provided demographic data in the initial survey, including biological sex, ethnicity, age, household income, highest level of education completed, whether they were in a romantic relationship (i.e., dating, engaged, or married), and whether they lived alone. During the initial survey and in the two follow-up surveys, participants reported their state-level loneliness. Further details on these measures are reported next.
Measures
Intercorrelations among the study’s independent and dependent variables appear in Table 1, and Table 2 presents these variables’ means, standard deviations, and internal reliability estimates. 1
Intercorrelations among the study’s independent and dependent variables.
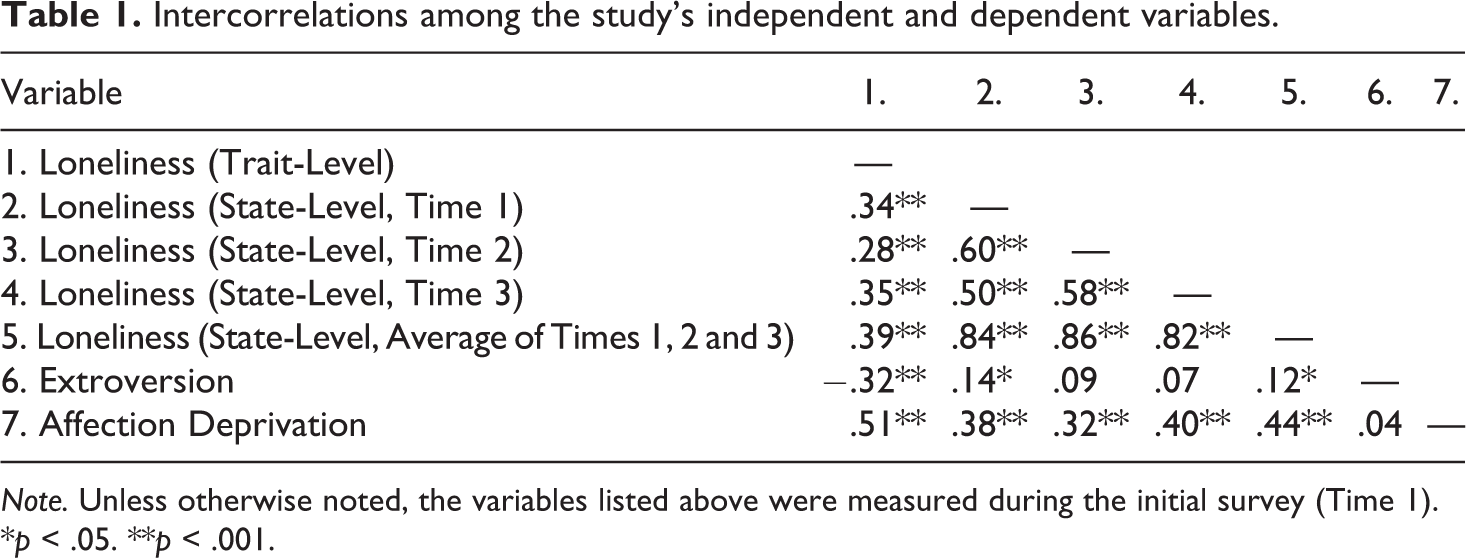
Note. Unless otherwise noted, the variables listed above were measured during the initial survey (Time 1).
*p < .05. **p < .001.
Means, standard deviations, and internal reliabilities.
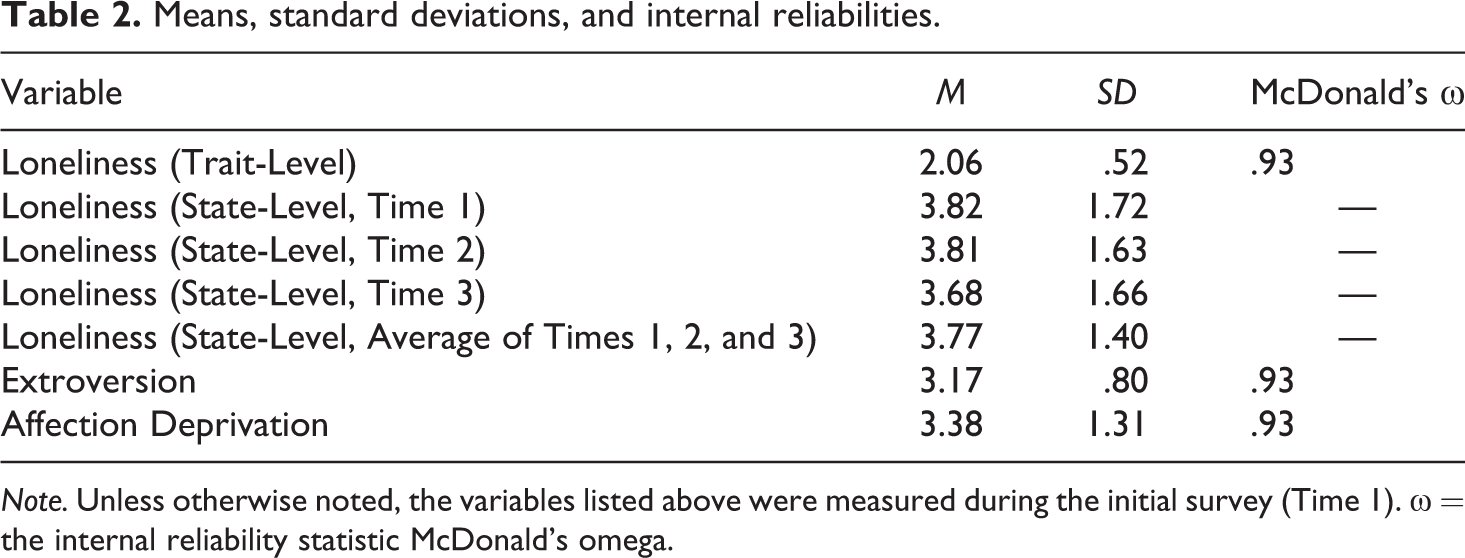
Note. Unless otherwise noted, the variables listed above were measured during the initial survey (Time 1). ω = the internal reliability statistic McDonald’s omega.
Trait-level loneliness
The researcher measured trait-level loneliness with the UCLA Loneliness Scale Version 3 (Russell, 1996). The scale consists of 20 Likert-type items that asks how frequently participants have experiences related to loneliness (e.g., “How often do you feel you lack companionship?” and “How often do you feel left out?”). Participants’ response options range from 1 (never) to 4 (often). Nine of the 20 items are reverse scored (e.g., “How often do you feel part of a group of friends?”).
Extroversion
Extroversion was measured using the extroversion factor of the Eysenck Personality Questionnaire Brief Version (Sato, 2005). Participants responded to 12 Likert-style items (e.g., “Do you usually take the initiative in making new friends?”) with response options ranging from 1 (not at all) to 5 (extremely). Two of the 12 items were reverse scored (e.g., “Are you mostly quiet when you are with other people?”).
Affection deprivation
The researcher measured affection deprivation using an 8-item scale developed by Floyd (2016). The scale measures, in general, the extent to which individuals are displeased with the amount of affection they receive (e.g., “In general, I feel deprived of affection,” “Affection is something I could use more of in my life”). Two of the 8 items were reverse scored (e.g., “I get enough affection in my life”). The scale was presented as a series of Likert-type items in which participants’ response options ranged from 1 (strongly disagree) to 7 (strongly agree).
State-level loneliness
State-level loneliness was measured in each of the three surveys using the same single item (“I feel lonely”) with participant response options ranging from 1 (strongly disagree) to 7 (strongly agree). Using a single item to measure state loneliness follows protocols from prior studies on loneliness (e.g., Roddick & Chen, 2020; van Roekel et al., 2018). In the analyses testing H1a–H1c, participants’ loneliness scores from the three time points were averaged. In the analysis investigating the research question, participants’ loneliness scores were not averaged, as that question explored changes in participants’ perceptions of loneliness over time.
Romantic relationship status
Participants completed one open-ended question (“What is your current romantic relationship status?”) that the researcher used to determine the participant’s romantic relationship status. Based on the responses received, the researcher categorized participants as single, dating, engaged, married, divorced, or widowed. Those who responded as dating someone, being engaged, or married were considered to be in a committed romantic relationship, whereas those who reported being single, divorced, or widowed were considered as not being in a committed romantic relationship.
Living arrangements
To determine whether participants lived alone or with others, the researcher asked the open-ended question, “How many other people are currently living with you in your residence? Don’t include yourself.” Those who replied zero were noted as living alone, whereas those replying any value besides zero were noted as not living alone.
Results
Hypotheses H1a–H1c
The researcher hypothesized that following initial COVID-19 stay-at-home orders in the United States that those living with at least one other person would experience significantly less loneliness than those who lived alone (H1a), those who were in a committed romantic relationship would experience less loneliness than those who were not in a committed romantic relationship (H1b), and those who were in a committed romantic relationship and living with at least one other person would experience the lowest levels of loneliness (H1c). To test these hypotheses, the researcher conducted two hierarchical regressions that investigated if living arrangements and romantic relationship status predicted the average of the participants’ state-level loneliness scores. Conducting hierarchical regressions allowed the researcher to determine if either of these predictor variables (living arrangements and romantic relationship status) explained variation in participants’ loneliness scores while controlling for the other variable.
The first hierarchical regression was conducted with living arrangements, participants’ age, and trait levels of loneliness, extroversion, and affection deprivation in the first block. The second block added the romantic relationship status variable to determine if being in a romantic relationship accounted for significant additional variance while controlling for the variables in the first block. Results showed a significant main effect for living arrangements. Adding romantic relationship status in the second block did not result in a significant increase in the amount of variance in loneliness scores accounted for by the model (i.e., when controlling for living arrangements and the other control variables, romantic relationship status did not significantly predict loneliness). Full results of this regression appear in Table 3.
Hierarchical regression testing romantic relationships status as a predictor of loneliness while controlling for living arrangements.
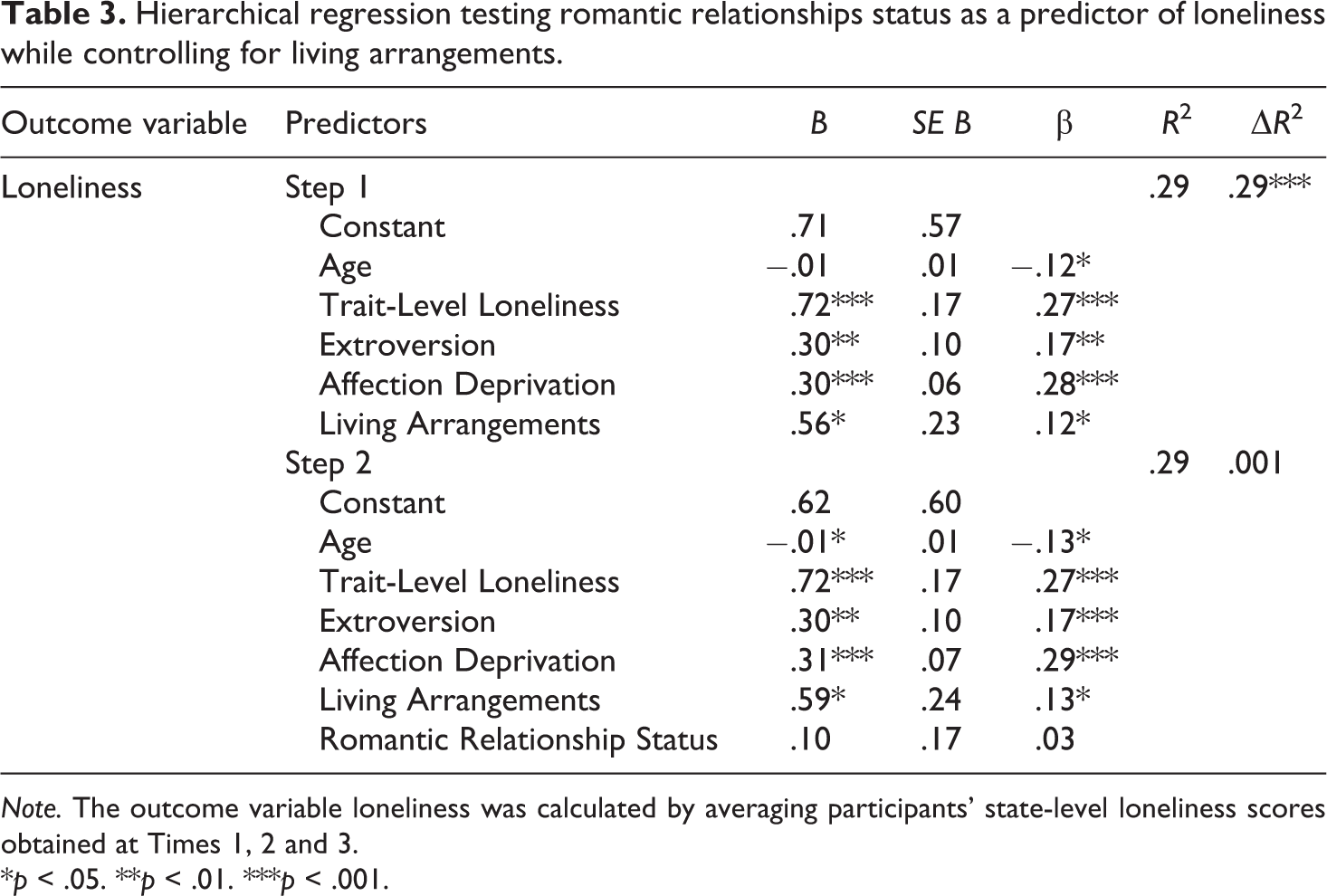
Note. The outcome variable loneliness was calculated by averaging participants’ state-level loneliness scores obtained at Times 1, 2 and 3.
*p < .05. **p < .01. ***p < .001.
In the second hierarchical regression, romantic relationship status, participants’ age, and trait levels of loneliness, extroversion, and affection deprivation were entered in the first block. The second block added the living arrangements variable to allow the researcher to ascertain whether one’s living arrangements accounted for significant variance in loneliness scores while controlling for the variables in the first block. A significant main effect for romantic relationship status occurred. Unlike in the first regression, adding living arrangements in the second block led to a significant increase in the amount of variance in loneliness scores accounted for in the model. Full results of the second hierarchical regression appear in Table 4.
Hierarchical regression testing living arrangements as a predictor of loneliness while controlling for romantic relationship status.
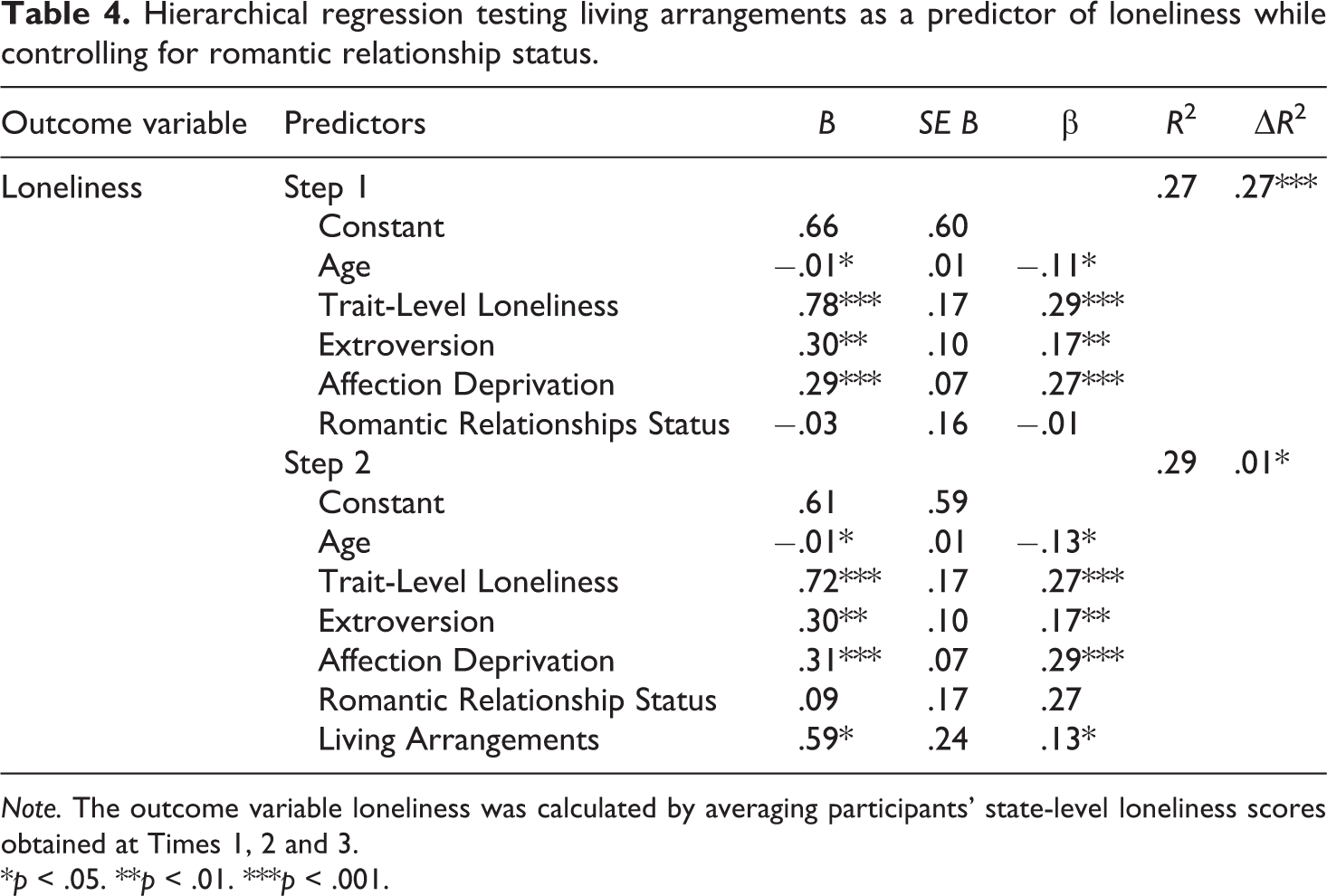
Note. The outcome variable loneliness was calculated by averaging participants’ state-level loneliness scores obtained at Times 1, 2 and 3.
*p < .05. **p < .01. ***p < .001.
Together the results of these regressions suggest qualified support for the study’s hypotheses. The results showed mean differences in loneliness scores based on living arrangements (H1a) and romantic relationship (H1b) status as predicted. These results, however, are qualified by the results of H1c, which predicted those who were in a committed romantic relationship and living with at least one other person would experience the lowest levels of loneliness. The results of the two regressions suggest substantial overlap in the variance in loneliness scores predicted by living arrangements and romantic relationship status. That is, the support found for living arrangements predicting loneliness scores is not completely independent of the support found for romantic relationships status predicting loneliness scores. It does appear, though, that living arrangements was a stronger predictor of loneliness scores than romantic relationship status based on the significant results from the second block of the second regression. At best, the researcher concludes that those living with another person and who were in a romantic relationship during the onset of the COVID-19 pandemic in the United States experienced the greatest loneliness, but the extent to which this was a function of living arrangements or romantic relationship status requires further study.
Research question
The researcher also investigated a research question regarding how loneliness reports changed across three time points during the early months of social distancing and stay-at-home orders in the United States. The researcher performed a within-subjects ANCOVA to control for age and trait-level measurements of loneliness, extroversion, and affection deprivation. Mauchly’s test of sphericity was significant, suggesting that the statistical assumption of homoscedasticity was violated at the repeated measures level. To address this, a Huynh-Feldt correction was used to interpret the results. 2
Results showed a nonsignificant decrease in state-level loneliness across the three measurements, F(1.99, 2.64) = 2.17, p = 12, Time 1: M = 3.82, SD = 1.72; Time 2: M = 3.80, SD = 1.63; Time 3: M = 3.68, SD = 1.66. Thus, it appears that across all participants state-level loneliness did not significantly change in the early months following stay-at-home and social distancing orders in the United States.
Of note, though, was an unhypothesized significant interaction effect between time and age that yielded significant differences in loneliness scores, F(1.99, 4.45) = 3.67, p = .026. To probe this interaction effect, the researcher transformed the participants’ ages into three age groups with approximately the same number of participants in each group. Doing so created age groups of 18–26, 27–39, and 40–75 years. Mean scores for each time loneliness was measured were determined for each age group (see Figure 1). Young adults aged 18–26 experienced the greatest loneliness at all three time points, but they also experienced the greatest decrease in loneliness across the three times points. Adults aged 27–39 reported lower loneliness scores than those aged 17–26, and their loneliness scores were nearly identical between Time 1 and Time 2 before showing a slight decrease between Time 2 and Time 3. Participants aged 40–75 initially reported the least loneliness but showed an increase between each time point, surpassing the loneliness scores of those aged 27–39 at Time 3. Together, these results suggest that young adults experienced more loneliness than other adults, and that the trajectory of loneliness during the early months of social distancing and stay-at-home orders differed across age groups in the United States.
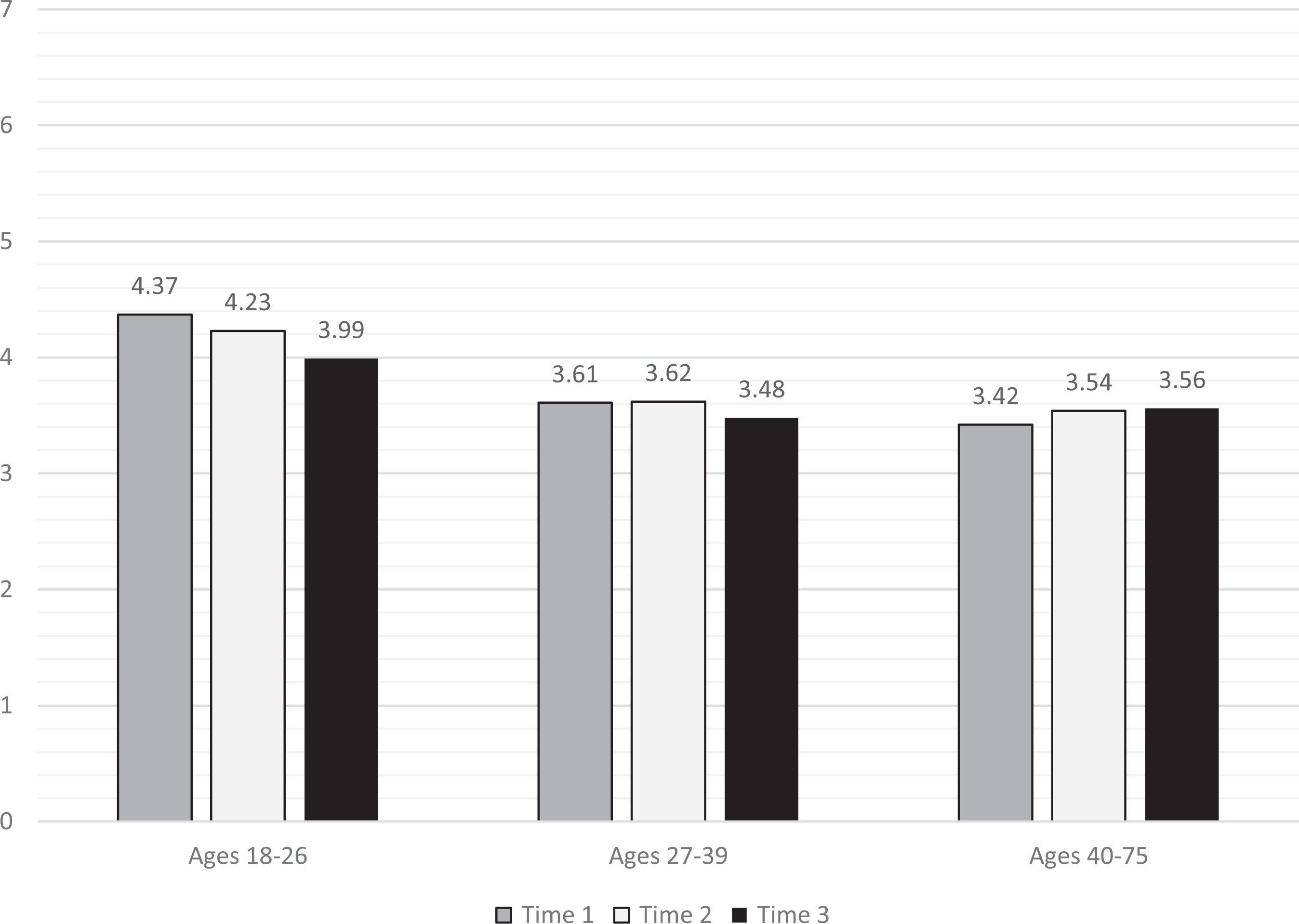
Changes in loneliness scores by age group: An unhypothesized finding.
Discussion
The goal of this study was to determine whether one’s living arrangements and relationship status affected experiences of loneliness, and to investigate if loneliness levels changed during the time following the initial stay-at-home orders and social distancing orders in the United States. As predicted, living with another person and being in a romantic relationship both mitigated loneliness during this time. Those who lived with another person were significantly less lonely than those who lived alone, and those in a romantic relationship reported less loneliness than those who were single. However, due to considerable overlap between these two variables, further research is needed to verify if cohabiting indeed provides protective effects against loneliness beyond the significant effects of being in a committed romantic relationship. Interestingly, reports of loneliness did not significantly increase or decrease in general, but varying patterns loneliness scores did occur when analyzing loneliness across age groups. The remainder of this section interprets these findings in light of prior loneliness research and provides recommendations for how these findings can be used to develop loneliness interventions and combat the COVID-19 pandemic.
As noted earlier, social distancing and stay-at-home orders could simultaneously mitigate the COVID-19 pandemic while potentially exacerbating the loneliness epidemic in the United States. Although intermittent loneliness is a universal experience (Rokach & Bauer, 2004), this study’s results reaffirm that certain groups of people are more susceptible to loneliness even under the circumstances of social distancing during the COVID-19 pandemic. Identifying individuals whose life situation (i.e., relationship status and living arrangements) make them prone to loneliness may motivate those people’s contacts to make a greater effort to check in and maintain relationships with those individuals.
Likewise, clinicians treating those who are experiencing mental health issues would be wise to consider the added importance of living arrangements and relationship status during the COVID-19 pandemic. These findings can also inform the development of interventions aiming to reduce loneliness. Most loneliness interventions have typically focused on adolescents, young adults, and the elderly because they have the highest prevalence of loneliness (Victor & Yang, 2012). These results suggest that other factors in addition to age—namely living arrangements and relationship status—should be considered when determining the populations that would benefit the most from loneliness interventions.
Recent research has shown that loneliness correlates with lower enactment of COVID-19 preventative behaviors such as social distancing (Stickley et al., 2020). This aligns with prior research that has shown connections between loneliness and adherence to taking medications (Avci, 2018; Segrin & Passalacqua, 2010). In light of this study’s findings, it is possible that those who live alone or who are not in a committed romantic relationship might be more likely to eschew social distancing guidelines to meet their needs for human connection. Thus, consideration of humans’ need for social connection should be part of the public health effort to stop the spread of COVID-19 or any other communicable disease that could lead to social distancing or stay-at-home orders. As mentioned earlier, creating loneliness interventions may combat health issues such as depression which were elevated as the result of the pandemic (Bauerle et al., 2020). But perhaps more importantly, loneliness interventions may actually reduce the spread of COVID-19, and the results of this study suggest that such interventions should target those who live alone or who are not in a committed romantic relationship.
Results also showed that people’s loneliness levels, in general, did not significantly increase over the course of the study. One possibility is that the data collection occurred so soon after the initial implementation of social distancing guidelines and stay-at-home orders that loneliness had simply not set in yet. However, these same statistical analyses revealed an unhypothesized effect in which changes in loneliness scores differed across age groups. Young adults aged 18–26 reported the greatest loneliness at all three time points but also reported a notably greater decrease in loneliness over the course of the study compared to the 27–39 age group and 40–75 age group. Prior research has shown that young adulthood is a time when people are particularly susceptible to intermittent loneliness (Hawkley & Cacioppo, 2010; Victor & Yang, 2012). Thus, it is unsurprising that young adults reported higher levels of loneliness during the early months of the COVID-19 pandemic.
Perhaps more intriguing was the significant decrease in loneliness reported by young adults throughout the study. One explanation is that this age group is particularly well equipped to handle a transition to maintaining their social relationships primarily through computer-mediated channels such as video calls (e.g., Zoom or FaceTime) or social media platforms. Another possibility is that young adults maintained a level of in-person social interaction similar to what they experienced prior to the pandemic. Young adults (ages 18–29) were the least likely to socially distance and adherence to social distancing guidelines decreased during the months when data was collected for the present study (Hutchins et al., 2020). Choosing to violate stay-at-home orders and participate in face-to-face social interactions over the course of the data collection would potentially account for the observed decrease in loneliness for this age group. Having discussed the study’s results, it is now worth considering the study’s strengths and limitations, as well as future research directions.
Strengths, limitations and future directions
As with any research endeavor, the present studied endured limitations; however, many of these limitations also provide pathways for future research. The most notable limitation of this study was the overlap that occurred between participants’ living arrangements and romantic relationship status. Hierarchical regressions did allow for the researcher to determine that living with another person accounted for additional variance in loneliness scores beyond being in a romantic relationship. Additional research is needed though to determine to what extent each of these variables are affecting perceptions of loneliness.
A second limitation of this study was the unbalanced sample in terms of sex, as there were far more female participants than male participants. This is notable considering prior loneliness research has found that loneliness is more prevalent for males than females (e.g., Greenfield & Russell, 2011; Knox et al., 2007); however, preliminary data analyses showed no significant sex differences in the study’s sample in terms of the dependent variables tested in the hypotheses and research question. Whereas this study focused on the magnitude of loneliness that individuals experienced, future loneliness research should explore how experiences of loneliness differed qualitatively during the pandemic, if at all, based on one’s sex.
A final limitation of this study worth noting was the inability to have participants’ loneliness scores prior to the COVID-19 pandemic and the implementation of stay-at-home orders and social distancing. Thus, it cannot be claimed definitively that the differences in loneliness scores based on living arrangements or romantic relationship status were influenced by the stay-at-home orders and social distancing guidelines implemented at the onset of the pandemic. One potential remedy to this issue would be to measure the same sample’s loneliness scores in the time after the WHO declares the United States has entered the post-pandemic phase or has achieved herd immunity. Such an analysis, though, would assume a return to relatively similar social practices after the pandemic has ended, but it may provide an approximation of this sample’s experiences of loneliness during a non-pandemic time.
One strength of this study was the sample’s average age and the dispersion of participants’ ages. Most loneliness research focuses on adolescents and elderly populations (Knox et al., 2007) because these two groups report the highest prevalence of loneliness (Victor & Yang, 2012). However, the current study had participants from several different points in adulthood, suggesting that living arrangements and romantic relationship status affect perceptions of loneliness for people of all ages, not just college-aged students or the elderly. Whereas researchers have developed loneliness interventions for elderly populations (for review, see Cattan et al., 2005), and researchers have called for interventions to be developed specifically for the elderly who live alone (Greenfield & Russell, 2011), this study serves as evidence for developing loneliness interventions for those who live alone, regardless of age.
Finally, the study’s longitudinal design was both a strength and a weakness. Collecting data at three different time points allowed for capturing changes in people’s loneliness during an important societal event. However, the timeframe in which the data was collected may have been exclusively during a “honeymoon” period of social distancing and stay-at-home orders. That is, loneliness may have increased more drastically in the months after this data collection. This study’s data collection may have occurred at a time when the newness of social distancing had not subsided and a lack of in-person social interaction had not significantly affected the study’s participants. Once possible, researchers should compare loneliness data collected during the COVID-19 pandemic to loneliness data collected in the months and years after the World Health Organization declares that the global population has moved into a post-pandemic phase.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open research statement
As part of IARR’s encouragement of open research practices, the author has provided the following information: This research was not pre-registered. The data used in the research is not available. The materials used in the research are not available.