
Abstract
Having a pregnancy end without a live baby can result in mixed effects to the relationship with one’s living children, but this has mostly been examined in the first years after the loss. Research is needed to understand the implications for relationships in later life. Thus, the current study examined whether losing a pregnancy was associated with the relationship with one’s adult children. The study used data from the Survey of Health and Retirement in Europe (SHARE). It examined a sample of women aged 50+ who experienced stillbirth over their life and a comparison sample of women who didn’t experience stillbirth. Regression models were used to assess the association between experiencing stillbirth and the parent–child relationship. The results showed that women who lost a pregnancy reported more emotionally close relationships with their adult children. These results indicated that losing a pregnancy could have long-term implications on the relationship with one’s children in later life. These women might have been more likely to invest in the emotional bonds with their children.
Introduction
Losing a pregnancy can be a life-altering, devastating event, and is one of the most difficult events that a person can go through. Stillbirth is often defined as the birth of a baby with no signs of life at or after 28 weeks of gestation (Hug et al., 2021), although some studies define it at or after week 20 or 22 (Gold et al., 2010; Hug et al., 2021; Krosch & Shakespeare-Finch, 2017). In 2021, an estimated 1.9 million babies were stillborn worldwide, corresponding to a global stillbirth rate of 13.9 per 1,000 total births (World Health Organization, 2023). Europe has seen lower rates compared to the global average, with stillbirth rates declining from 6.9 per 1,000 total births in 2000 to 4.1 per 1,000 in 2019 (Hug et al., 2021).
Having a pregnancy end without a live baby is highly stressful and invokes negative emotional consequences, including heightened short-and long-term levels of grief, depression, anxiety, distress, post-traumatic stress, decreased well-being, and even increased mortality risks (Calderon-Margalit et al., 2007; Campbell-Jackson & Horsch, 2014; Westby et al., 2021). The impact of such a loss extends beyond the individual, influencing partners, family members, and the broader social context. Especially relevant is the relationship with one’s living children, which can be deeply affected. However, although much research focuses on the years immediately following stillbirth, less is known about its enduring effects, particularly as parents and children age. The present study aims to addresses this gap by examining how stillbirth is associated with parent–child relationships in later life.
Convoy model of social relations and life course perspective on stillbirth
To understand the long-term effects of stillbirth on the relationship with one’s (living) children, this study draws on two guiding theoretical frameworks: the Convoy Model of Social Relations (Kahn & Antonucci, 1980) and the Life Course Perspective (Elder Jr., 1994). The convoy model posits that individuals are surrounded by a network, or convoy, of close social relationships that provide support throughout life (Antonucci et al., 2014). These convoys are shaped by personal, structural, and situational factors and evolve over time, but core ties such as those with children often remain central and emotionally salient in later life (Antonucci et al., 2004). The model highlights both functional aspects of social ties, such as emotional closeness, and structural aspects, such as contact frequency, as key predictors of health and well-being (Santini et al., 2015; Schwartz & Litwin, 2017).
Complementing this, the Life Course Perspective emphasizes how early-life experiences and major life transitions reverberate across time to shape later life outcomes (Settersten, 2015). Applied in the context of stillbirths, this perspective could suggest that the effects of stillbirth may alter the relationships with living children in ways that persist throughout the decades.
Impact of stillbirth on individuals and families
The psychological effects of stillbirths often extend beyond the individual, impacting the relationship with the family and the community. Among partners, the loss may result in either strengthened emotional bonds or increased tension and conflict (Burden et al., 2016; Campbell-Jackson & Horsch, 2014; Gold et al., 2010; Horstman & Holman, 2018; Human et al., 2014). Extended family and community relationships can provide much needed support but may also be strained, particularly when the significance of the loss is not fully recognized or validated (Burden et al., 2016; Campbell-Jackson & Horsch, 2014; Human et al., 2014).
The impact of stillbirth on the relationship with one’s living children is especially pertinent, both for children who were alive during the loss and those born after the loss (O’Leary & Gaziano, 2011). These children could live and grow up in a family which is still in mourning and parents with attachment difficulties (Üstündağ – Budak et al., 2015). Such an event can change the behavior and type of care that parents provide for their children varying from overprotection, due to knowing what it is to lose a child, to the distancing from the children and neglect of parental obligations due to the parents being immersed in their own grief (O’Leary & Warland, 2012). The emotional needs of the older children within these families may go unmet due to the many demands of grief on the parents (Cacciatore et al., 2010). Stillbirth can also affect older siblings who experience feelings of guilt, fear, anxiety, and misunderstanding (Burden et al., 2016). Individuals who were born after perinatal loss, interviewed as adults, described feeling “invisible” when they grew up, possibly due to their mothers’ depression and difficulty forming an attachment to the children born after the loss (O’Leary et al., 2006).
Nevertheless, alongside these reports of negative effects of stillbirth, there are also indications of parallel, more positive effects on parenting. Although stillbirth is perceived as “senseless”, the search of meaning making can contribute to adaptation (Barboza et al., 2021). The notion of intentional parenting describes a different perspective of intentionality of parents who experienced a stillbirth: that of valuing their children’s life as a gift and not taking their parenting responsibility lightly or taking their children for granted (O’Leary & Warland, 2012). Accordingly, parents who reported finding a meaning in their child’s death had less mental distress, better physical health, and better marital satisfaction. Several years after the death, some parents reported a shift in priorities and enhanced appreciation for life (Burden et al., 2016; Cacciatore, 2013). Relevant to this is the possibility that stillbirth will lead to posttraumatic growth, conceptualized as positive psychological changes resulting from successfully coping with the consequences of traumatic events (Gul & Karanci, 2017). Studies focusing on mothers who experienced stillbirth found indications of their posttraumatic growth (Krosch & Shakespeare-Finch, 2017; Ryninks et al., 2022). The various studies on stillbirth often focus on the relationship with the living children in the few years after the loss. However, the reach of such traumatic events can stretch beyond these first years, well into the adulthood of these children and the later life of the parents.
Long-term perspectives on social relationships
As people age, their social convoys become especially crucial to well-being. In older adulthood, children often occupy the inner-most circles of emotional closeness and are frequent sources of support (Antonucci et al., 2004). Quality relationships with children are associated with better mental and physical health, healthcare engagement, and more positive views on aging (Cohn-Schwartz et al., 2022; Schafer, 2013; Wilkinson et al., 2023). However, the relationship with one’s children is often complex and can include ambivalence, conflict, or emotional distance contains negative affect as well (Birditt et al., 2017).
The convoy model underscores that emotional closeness and frequency of contact are key elements of relational functioning that influence mental and physical health, and are both modifiable across time. The Life Course Perspective reinforces the idea that earlier life disruptions, such as stillbirth, can alter these dimensions of parent–child relationships decades later. The current study builds on the conceptual link that stillbirth may intensify parents’ emotional investment in their children, increasing their perceived centrality and closeness in the social network. Therefore, this study sets out to examine the associations of stillbirth with the relationship with one’s children in later life. Specifically, the study will focus on mentioning the child as a close social network member, on the emotional closeness with the cited children and frequency of contact with them. Experiencing stillbirth is hypothesized to be associated with a better relationship with children in later life: 1. The children will be more likely to be cited as close network members. 2. The children in the network will be more emotionally close 3. The children in the network will be more frequently contacted.
Methods
Participants and procedure
The current study is based on the Survey of Health, Aging and Retirement in Europe (SHARE). The survey collects data from a nationally representative sample of community dwelling adults aged 50 and above and their spouses of any age across Europe (Börsch-Supan et al., 2013). Questionnaires on a variety of domains are administered in the respondents’ home by trained interviewers, following the participants’ informed consent. The current study combines data from waves three and four. The third wave of data collection, also called SHARELIFE, was collected in 2008–2009 and gathered retrospective information on respondents’ life course, including questions about stillborn children (a later wave of retrospective data, in 2017, did not inquire about stillborn children). Data from SHARELIFE was combined with the 2011 data collection (the fourth wave), which was the first to collect information on social networks in SHARE and closest in time to the retrospective wave. Participants came from twelve countries: Austria, Germany, Sweden, the Netherlands, Spain, Italy, France, Denmark, Switzerland, Belgium, Czech Republic and Poland.
The study focused on women, since only women were asked about a history of stillbirth. It also focused on those who had children. This focus allowed a comparison between women who experienced stillbirth and those who didn’t experience stillbirth but also wanted children. Thus, the study sample consisted of women who were aged 50 and above in the fourth wave of the survey, who participated in the retrospective wave three, who responded to the question about stillborn children and who had living children at the time of the fourth wave of the survey. This initial sample consisted of 9,585 participants, of which 7% (643) reported having had a stillborn child over the course of their lives. The stillbirth group was matched with a control group that did not experience stillbirth using propensity scores based on age and education via the Coarsened Exact Matching method (Iacus et al., 2011). The matched control sample included 643 respondents who did not report stillbirth, but who were similar in age and education to those who reported experiencing stillbirth. The study sample focused on the 1,145 respondents who had full information on the study variables. The analyses of emotional closeness and contact frequency focused on the 756 participants who had children in their network and provided further information about them. Missing data analysis indicated that those with missing data were older, were less likely to have high education, were in a worse financial and health status and less likely to be married (p < .05). They did not differ in relation to stillbirths, the relationship with their children and the number of children.
Measures
Stillbirth
Women participants were asked: “Have you ever had a stillborn child?”, with response options being “yes” or “no”. Those who answered positively were asked follow-up questions, including about the month in which the pregnancy ended. It is noted that while some participants have likely understood the stillbirth question to refer only to losses occurring at later pregnancy stages, about 46% of the stillborn children were reported to have been born in the fourth month of pregnancy or earlier.
Social networks
Social networks were assessed using a name-generator approach, which maps individuals’ social milieu from their subjective perspective. Respondents are asked to name up to seven persons with whom they discuss important matters and are subsequently asked to provide more information about these confidants and about the relationship with them (Cohn-Schwartz & Naegele, 2023). The study devised three outcome variables based on this measure. The first was a dummy variable indicating the citation (yes\no) of a child in the network. Emotional closeness was probed by asking respondents “How close do you feel to (confidant’s name)?” with answers ranging from “Not very close” (1) to “Extremely close” (4). The score on this measure was the average rate of emotional closeness with the cited children. Contact frequency was probed by asking respondents “During the past twelve months, how often did you have contact with (confidant’s name) either in person, by phone or mail, email or any other electronic means?” with answers ranging from “Daily” (1) to “Never” (7). The responses were reverse coded and the score on this measure was the average rate of contact frequency with the cited children, such that higher scores indicate more frequent contact.
Covariates
Several sociodemographic and health covariates were used, as these factors were previously shown to be associated with the relationship with one’s children in later life (e.g., Cohn-Schwartz & Schmitz, 2024; Ha et al., 2017; Wilkinson et al., 2023). Age was used as a continuous variable. Education was measured as a binary variable indicating below secondary education or secondary education and above. Financial status was measured using a question about the extent to which the respondent’s household can make ends meet. Its four response options range from “with great difficulty” (1) to “easily” (4). The covariates also include a binary variable indicating whether the respondent was married, and their number of living children. Self-assessed health was measured on a 5-point Likert scale, which was reverse coded such that a higher score indicated better perceived health. Physical health was also measured by the number of mobility, arm function and fine motor limitations (range: 0–10). Depressive symptoms were measured by the Euro-D, a 12-item measure meant to count late life depressive symptoms (Prince et al., 1999). The multivariate models also control for country of residence. All the covariates were measured at wave 4.
Data analysis
Data analysis first focused on descriptive data of the sample characteristics. It also examined the bivariate associations between stillbirth and the study variables. The analyses used chi-square tests for the association between the binary variables, t tests for the associations between binary and continuous variables and Pearson correlations for the associations between continuous variables. The final stage of the inquiry consisted of regression analyses, with the different aspects of the relationship with children as the outcome measures. Logistic regression was employed to model the binary outcome of whether a child was mentioned within the social network, as this method is appropriate for predicting variables with two possible values (0 = not mentioned, 1 = mentioned; (Bewick et al., 2005). Ordinary least squares (OLS) regression was used to model the continuous outcomes of emotional closeness and contact frequency with children. This approach is appropriate given the large sample size and the focus on estimating mean differences between groups. As demonstrated by Lumley et al. (2002), OLS regression does not require the outcome variable or residuals to be normally distributed with samples of 500 or more, as was the case in the current study. Variance Inflation Factor (VIF) in the regression models for both outcome variables was lower than 3, indicating no multicollinearity (Stevens, 2009). For each outcome variable, the regression model predicted the outcome variables using stillbirth and controlling for the covariates.
Results
Sample characteristics of the study.
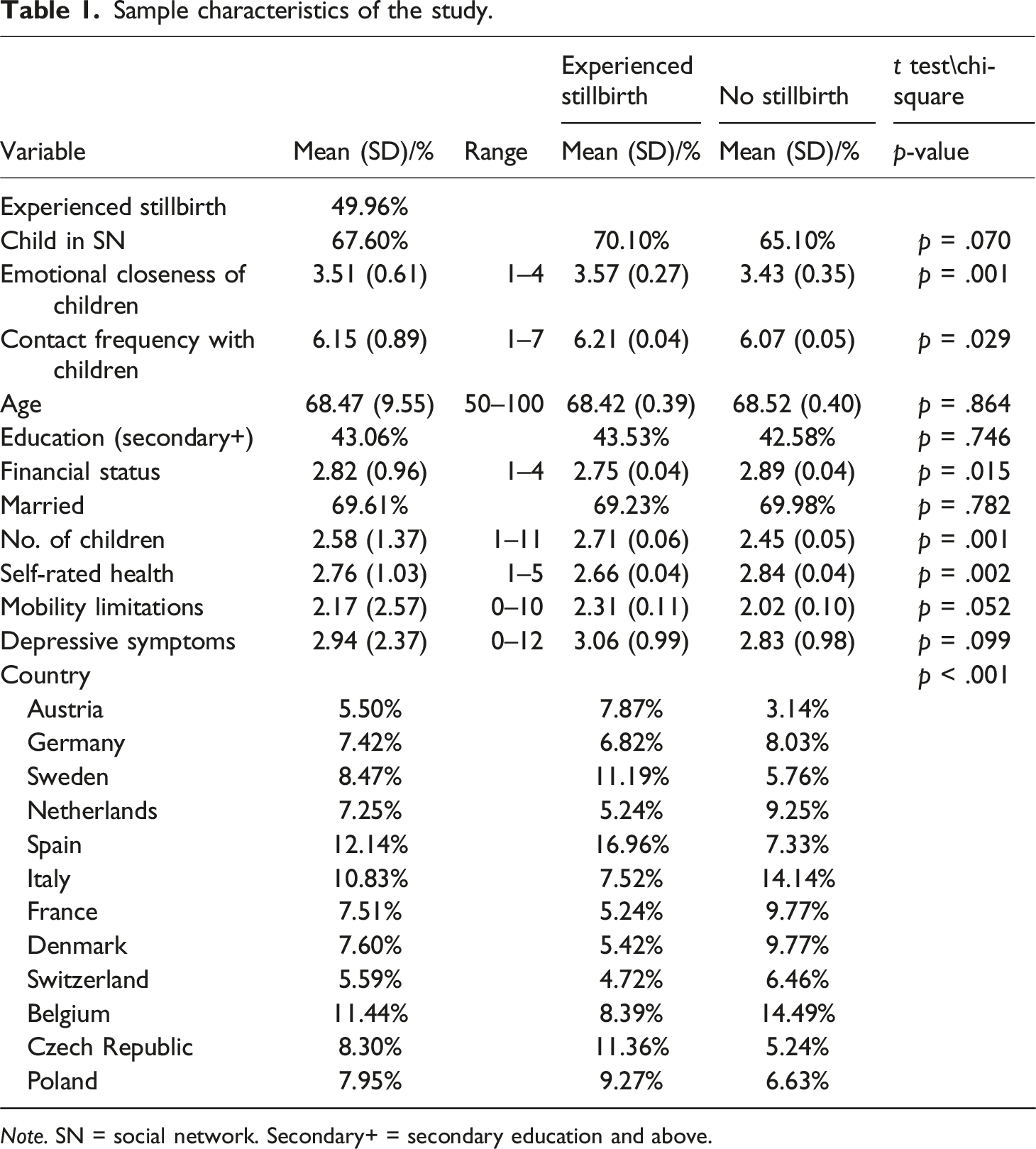
Note. SN = social network. Secondary+ = secondary education and above.
Table 1 also shows the bivariate comparison of the study variables between women who experienced stillbirth and those who didn’t experience such a loss (in the form of t tests or chi-square tests). Women who experienced stillbirth were slightly more likely to include their children in their social network, but this was only marginally significant (p = .07). They also reported higher emotional closeness and more frequent contact with their children who were cited as confidants. Women who experienced stillbirth had more children and were in a worse financial and health condition, compared to those who didn’t experience stillbirth. Women who experienced stillbirth were also more likely to live in Austria, Sweden, Spain, the Czech Republic and Poland. Those who didn’t experience stillbirth were more likely to live in the Netherlands, Italy, France, Denmark and Belgium. Women who experienced stillbirth did not differ from those who didn’t experience such a loss in their age and education level (by design to create two comparable groups, see the methods section for more information), in their marital status, depressive symptoms and mobility limitations. Supplemental Table S1 also examines these differences within the subset of participants who had children within their network, indicating similar trends. Specifically, the differences in this subset sample of participants who cited their children within their close network were that those who experienced stillbirth had more children and were in a worse health condition. Country differences were also seen, similarly to the large sample. In contrast to the larger sample, no differences were found in relation to financial status between those who experienced stillbirth and those who didn’t experience stillbirth. Similarly to the larger sample, there were also no differences in relation to age, education, marital status, depressive symptoms and mobility limitations.
Regression models predicting the relationship with children.
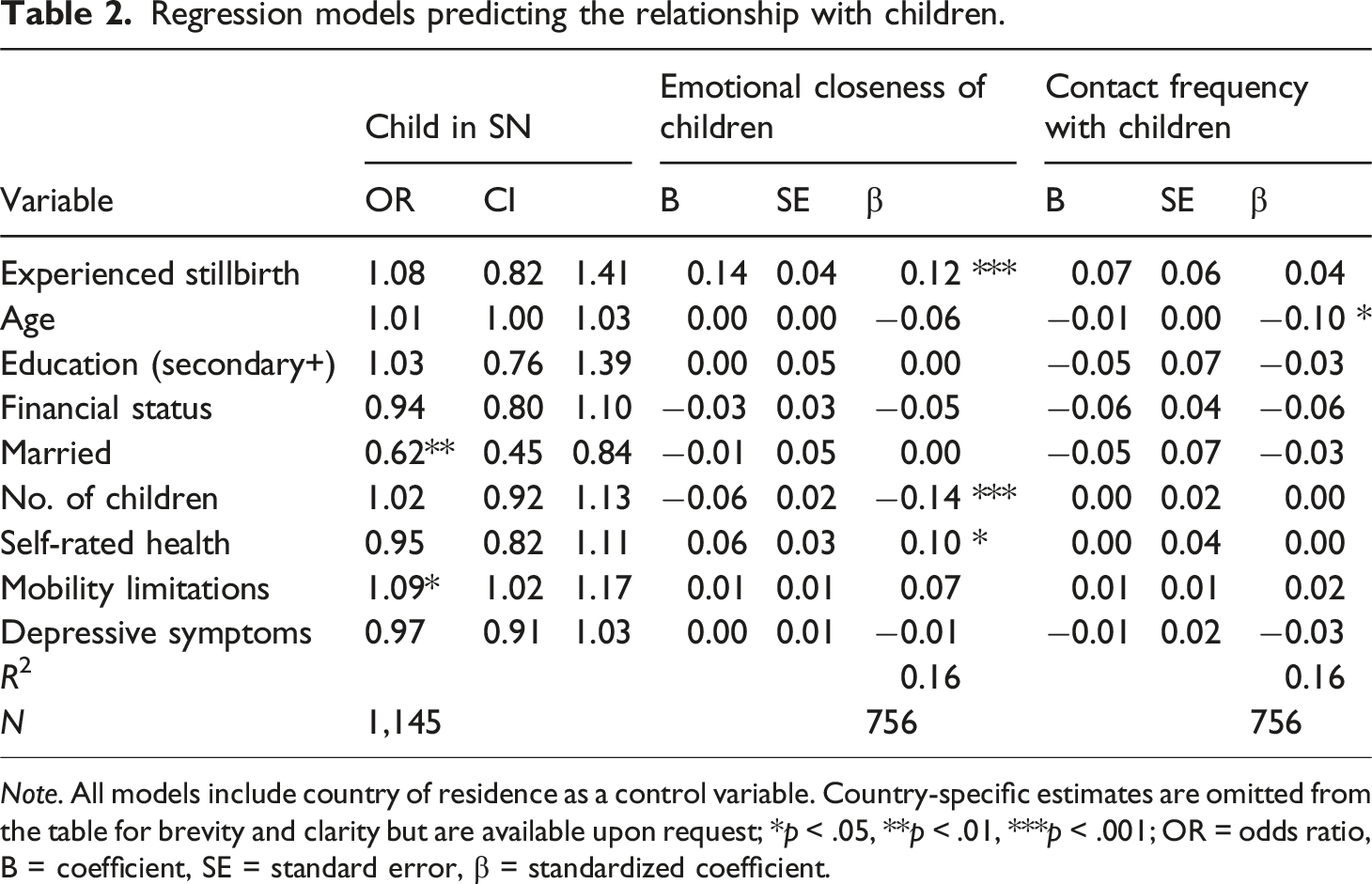
Note. All models include country of residence as a control variable. Country-specific estimates are omitted from the table for brevity and clarity but are available upon request; *p < .05, **p < .01, ***p < .001; OR = odds ratio, B = coefficient, SE = standard error, β = standardized coefficient.
The second column predicted the emotional closeness with the children who were cited as close, examining the second hypothesis that the children in the network will be more emotionally close among women who experienced stillbirth. The model found that experiencing stillbirth was significantly related to the emotional closeness with one’s children in the network, such that women who experienced stillbirth reported a closer relationship with the children in their network, compared to those who did not experience stillbirth. This result supported the second hypothesis. The third model in Table 2 predicted contact frequency with the cited children, in relation to the third hypothesis that the children in the network will be more frequently contacted by women who experienced stillbirth. It showed that stillbirth was not significantly associated with the contact frequency with children cited in the close network, contrasting with the third hypothesis. Among the covariates, a higher likelihood of mentioning a child in the social network was related to not being married and having more mobility limitations. Emotional closeness with the cited children was related to having fewer children and to better self-rated health, and frequent contact with the cited children was related to being younger. Additional analyses (available upon request) predicted binary measures of mentioning at least one extremely close child and one child who is contacted daily in the network, using logistic regressions, while controlling for the covariates. These analyses showed a similar trend - that participants who experienced stillbirth were more likely to report having an extremely close child in the network, compared to those who did not experience stillbirth. Stillbirth was not associated with having at least one confidant child who was contacted daily.
It might be possible that whether children were born before or after a stillbirth could have affected the relationship in later life. To examine this possibility, supplementary multivariate regression analyses were performed that separated the stillbirth into a loss prior to having children (21%) and loss following having children (29%; Supplemental Table S2). These analyses showed that experiencing stillbirth both before and after having children was related to a higher emotional closeness with one’s close children, as compared to not experiencing stillbirth. The supplemental regression analyses also showed that both types of losses were not related to citing a child in the social network or to contact frequency with the most contacted child.
Discussion
The current study set out to examine whether losing a pregnancy could be associated with the relationship with one’s children in later life, years and decades after the loss occurred. The findings suggest that such a tragic event could have long-term implications. Specifically, women who lost a pregnancy reported more emotionally close relationships with the children in their close networks in later life.
The main study finding was that women who experienced a stillbirth earlier in life and who reported a child in their social network were more emotionally close with their adult children, in partial support of the study hypotheses. This result can underscore that stillbirth is not only a deeply distressing event but also one that can alter the trajectory of the parenthood experience. The loss of a hoped-for child represents a rupture in the anticipated life course, often resulting in a sense of incomplete parenthood and enduring grief. However, these women might have experienced their parenthood differently following the loss, also being less likely to take their children for granted and more likely to invest in the emotional bonds with them (O’Leary & Warland, 2012). They might have found meaning in the loss they experienced, that affected their parenthood experience by fostering a deeper appreciation of their living children (Barboza et al., 2021). They might have shifted their priorities as parents into a greater focus on the relationship with their children, a changed focus which could have remained throughout their children growing up. Although the relationship with one’s children can include negative aspects (Birditt et al., 2017), the memory of losing a pregnancy could color such difficulties in a more positive light and make the parenthood experience focus on the positive aspects of this relationship, leading to a closer and better relationship in later life. These results can also reflect the possible posttraumatic growth experienced by these mothers following the loss (Krosch & Shakespeare-Finch, 2017; Ryninks et al., 2022).
Interestingly, the results were significant mostly in relation to the quality of the relationship with the children and less in relation to the more structural aspect of contact frequency (Antonucci et al., 2014). Although a significant association emerged of stillbirth with contact frequency with confidant children, it was significant only in the bivariate analyses and not in the multivariate regression. This trend may indicate that losing a pregnancy is more relevant for the emotional bonds with one’s close children, and frequency of contact could reflect less emotional aspects of the relationship such as the level of support needs and geographical proximity. In light of the convoy model, these results underscore how a significant early-life experience like stillbirth may shape the configuration and quality of later-life social ties. The model emphasizes that emotional closeness and structural aspects such as contact frequency are both central to understanding social relationships across the life span (Antonucci et al., 2014). The study findings, which point to stronger emotional closeness with children among women who experienced stillbirth, suggest that such a traumatic event can intensify the salience of these core ties. Importantly, this association emerged for emotional closeness rather than frequency of contact, highlighting the functional, rather than structural, dimension emphasized in the convoy model (Antonucci et al., 2014). The enduring impact of stillbirth on close emotional ties aligns with the model’s assertion that convoys are dynamic and shaped by both individual history and critical life experiences.
These results extend current research in several ways. First, they add to our knowledge of early-life factors that can impact relationships with children in later life, in accordance with the life-course perspective. Although some earlier-life factors have been identified, such as parental separation (Becker & Hank, 2022) and labor market involvement (Cohn-Schwartz & Naegele, 2023), the role of losing a pregnancy has not been examined. These findings are especially important given the valuable effects that a close relationship with one’s children can have in later life (Wilkinson et al., 2023). These findings also add to the literature on the effects of stillbirth on the parenthood experience. The existing literature mostly focuses on parents several months or years after the loss, when the loss is relatively fresh. Moreover, the existing literature shows mixed trends, of difficulties alongside a greater appreciation of parenthood (Burden et al., 2016; O’Leary & Gaziano, 2011; O’Leary & Warland, 2012). The current study indicates that over a longer time, of several decades, the effects on the parenthood experience could be relatively positive. It is possible that while in earlier years it could be more difficult to find meaning in the loss, over time the loss could motivate stronger emotional bonds and a renewed sense of purpose in parenting.
Some limitations of this study should be acknowledged. The question about stillbirth was asked using the phrase “a stillborn child”, however about 46% of the stillborn children were reported to have been born in the fourth month of pregnancy or earlier. Thus, it seems that at least some participants referred to earlier pregnancy stages. Nevertheless, the phrase “stillbirth” is used throughout the text of this study to be consistent with the question phrasing. An additional limitation is the focus on women. Even though mothers are more likely to report psychological symptoms and parenting stress compared to fathers after stillbirth (Faleschini et al., 2021), fathers also often suffer from grief, reduced well-being and adverse psychological effects (Badenhorst et al., 2009; Holman & Horstman, 2019; Obst et al., 2020). Thus, future studies should also consider the experiences of fathers and the experience of partners in single-sex relationships. Moreover, the measures in the current study were self-reported and collected via the same survey instrument, which raises the possibility that common method variance may have inflated the observed associations. While the use of a large, structured dataset such as SHARE reduces some forms of bias, future studies should consider using multiple data sources or time points to minimize the risk of shared method effects. Another possible limitation is the baseline differences between the two groups of those who experienced and did not experience stillbirth (i.e., financial status, self-rated health and number of children). Although the multivariate analyses controlled for these variables, the differences between the two groups could indicate that there may be additional variables influencing the findings. Additionally, the study focuses solely on the mother’s perspective of the parent–child relationship. However, children may perceive the relationship differently, and emotional closeness or frequency of contact may not be experienced or interpreted similarly by both parties. Future research should aim to incorporate the perspectives of both parents and children to better understand the complex nature of these relationships.
To sum up, this study suggests that stillbirth is related to an emotionally closer relationship with one’s living children who are confidants during later life. The findings of this study could give hope to parents who experienced stillbirth. Although when tragedy strikes, it is not necessarily imaginable to think of a positive outcome, in later stages of coping it might be possible to focus on these potential aspects of the loss. These findings support the need for interventions and support systems that address not only the immediate grief of pregnancy loss but also the long-term implications for the parenthood experience. Care providers should recognize that the effects of such loss can persist and transform over the life course, influencing how parents relate to their children. Support should especially extend beyond the parents to the entire family and focus on the relationships with one’s living children which can be affected by stillbirth, even those born after the loss. Family-based interventions can promote open communication, mutual support, and collective healing. Interventions with parents after stillbirth can foster meaning making in relation to the attitudes towards the living children. They can help couples in the process of their joint sense-making and encourage stronger communication in interactional sense-making (Holman & Horstman, 2019; Horstman & Holman, 2018). Care providers can acknowledge the emotional impact of the loss, validate the patient’s experience, and provide compassionate communication to support their journey after stillbirth - even many years after the loss occurred (Brann et al., 2025). While the findings suggest that women who experienced stillbirth report greater emotional closeness with their confidant children in later life, this does not suggest that the process of adaptation and meaning making is unnecessary or complete for all bereaved parents. The role of interventions promoting meaning making may be critical in facilitating this adaptive outcome over time and expanding it to more parents following stillbirth who may find it difficult to adapt without external support. Such interventions are not necessarily intended to address a lack of closeness, but to support parents in navigating grief, reframing their experience, and potentially deepening relationships with their living children. Therefore, support that promotes reflective processing and intentional parenting may be especially valuable in the months and years following loss - even if longer-term outcomes are positive.
Supplemental Material
Supplemental Material - From loss to closer bonds: Pregnancy loss and the emotional bonds with children in later life
Supplemental Material for From loss to closer bonds: Pregnancy loss and the emotional bonds with children in later life by Ella Cohn-Schwartz in Journal of Social and Personal Relationships.
Footnotes
Acknowledgments
This paper uses data from SHARE Waves 3 and 4 (DOIs: 10.6103/SHARE.w3.900, 10.6103/SHARE.w4.900) see Börsch-Supan et al. (2013) for methodological details. (1) The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006–028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782, SHARE-COVID19: GA N°101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, VS 2020/0313 and SHARE-EUCOV: GA N°101052589 and EUCOVII: GA N°101102412. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, BSR12-04, R01_AG052527-02, HHSN271201300071C, RAG052527A) and from various national funding sources is gratefully acknowledged (see ![]() ). The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6- CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4- CT-2006–028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782, SHARE-COVID19: GA N°101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, VS 2020/0313 and SHARE-EUCOV: GA N°101052589 and EUCOVII: GA N°101102412. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, BSR12-04, R01_AG052527-02, HHSN271201300071C, RAG052527A).
). The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6- CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4- CT-2006–028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782, SHARE-COVID19: GA N°101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, VS 2020/0313 and SHARE-EUCOV: GA N°101052589 and EUCOVII: GA N°101102412. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, BSR12-04, R01_AG052527-02, HHSN271201300071C, RAG052527A).
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Open research statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.