
Abstract
In families facing parental cancer, children have an increased risk for impaired psychosocial functioning, such as lower quality of life and satisfaction with life, and increased posttraumatic stress symptoms (PTSS). These outcomes are likely affected by both dyadic and individual factors. The aims of the current study were to examine (1) the associations of sibling relationship quality (i.e., warmth and conflict) and emotion regulation problems with child functioning (i.e., quality of life, satisfaction with life, and PTSS) in families facing parental cancer; and (2) whether emotion regulation problems partially or fully mediate these associations. Our sample consisted of 161 children from 82 Dutch families facing parental cancer (84.6% maternal cancer). During home visits, children (mean age 12.1 years; 53.1% girls; 54.4% same-sex sibling pairs) filled out questionnaires about their sibling relationships and their own functioning. Mediation analyses showed no significant direct nor indirect effects of sibling warmth on quality of life, satisfaction with life or PTSS. Significant indirect (but not direct) effects were found for sibling conflict on quality of life and satisfaction with life and on PTSS, through emotion regulation problems. Children experiencing more sibling conflict reported more emotion regulation problems, which were linked to lower quality of life and satisfaction with life and more PTSS. Our study suggests that sibling conflict could be considered a risk factor for child psychosocial functioning in families facing parental cancer. The potentially beneficial effects of sibling warmth were not confirmed by our findings. Limitations and implications of the study and future directions are discussed.
Introduction
Families in which a parent has cancer are facing many challenges: Parents are dealing with their own or their partner’s health issues and related psychosocial problems, besides caring for their children. Additionally, children are confronted with the physical and psychological vulnerability of their parents and have to cope with the impact of the illness on the family. In such families, there is an increased risk for compromised psychosocial functioning of children (Visser et al., 2004).
Researchers have operationalized child psychosocial functioning in the context of parental cancer in different ways. Several studies have examined child maladjustment (see Krattenmacher et al., 2012; Morris et al., 2016 for an overview), including posttraumatic stress symptoms, in relation to the parent’s cancer (PTSS; Foran-Tuller et al., 2012). Additionally, other studies have focused on positive outcomes, such as quality of life (e.g., Inhestern et al., 2021) or satisfaction with life (e.g., Egberts et al., 2021). However, most of these studies only focused on single outcomes, neglecting the potentially different associations between predictive factors and positive versus negative indicators of psychosocial functioning. By including both positive (i.e., quality of life and satisfaction with life) and negative (i.e., PTSS) indicators, we can provide a more comprehensive picture of children’s psychosocial functioning in families with parental cancer.
Earlier work on children’s quality of life in the context of parental cancer, including perceived physical and psychological well-being, parent and peer relationship quality, and school environment (Ravens-Siebererer et al., 2007), has indicated that, overall, children confronted with parental cancer show average or even high quality of life (Bultmann et al., 2014; Egberts et al., 2021; Krattenmacher et al., 2014). However, research also indicates that quality of life might be impaired in certain domains (e.g., emotional wellbeing) (Hauken et al., 2018; Jeppesen et al., 2016) and that a substantial subgroup of children experiences below average overall quality of life (Egberts et al., 2021). Additionally, studies examining the impact of parental cancer on child functioning have shown that about 25% of these children show elevated levels of PTSS in relation to their parent’s cancer such as reexperiencing, avoidance and hyperarousal (Egberts et al., 2021; Foran-Tuller et al., 2012; Huizinga et al., 2005). In conclusion, whereas these findings show that children in families with parental cancer may be at risk for maladaptation, they also show that there are differences between children in their response to parental cancer. It is important to examine factors and processes that may explain these differences. One of these factors could be sibling relationships.
In families affected by parental cancer, support from significant others may become particularly important. According to the stress-buffering effect model, the impact of stressful circumstances is weaker when perceived support from significant others is high and stronger when perceived support is low (Aba et al., 2019). So, following the tenets of this model, the impact of parental cancer may be less pronounced if support of family members is high, thereby preventing child maladjustment (i.e., impaired quality of and satisfaction with life or PTSS). Whereas the protective role of the parent-child relationship has been confirmed in the context of parental cancer (e.g., Lewis & Darby, 2003), another potential source of support has, to our knowledge, not been examined: the sibling relationship.
Sibling relationship quality is most often represented by two broad dimensions, namely warmth and conflict (Buhrmester & Furman, 1990). Sibling warmth reflects positive aspects of the relationship, such as affection, companionship, and emotional support, whereas sibling conflict encompasses negative aspects such as quarreling, fighting, and hostility. A large body of research, including a meta-analysis of 34 studies (Buist et al., 2013), has consistently shown that children with higher levels of sibling warmth and lower levels of sibling conflict have lower levels of negative outcomes such as internalizing and externalizing problem behavior (Noller, 2005; Pike et al., 2005). Additionally, these children report more positive outcomes such as social competence (Buist & Vermande, 2014; Kim et al., 2007; Pike et al., 2005).
So, overall, more sibling warmth is linked to better functioning, whereas more conflict is linked to worse functioning. More specifically focusing on research concerning quality of life, satisfaction with life and PTSS, studies have shown that adolescents reporting more sibling support experience more satisfaction with life (Hollifield & Conger, 2015; Oliva & Arranz, 2005; Ponti & Smorti, 2019). Additionally, studies focusing on war-related trauma have shown that higher sibling relationship quality was related to lower self-reported PTSS in 10–14-year-old children (Palosaari et al., 2016; Peltonen et al., 2010). Based on these studies, we expected a direct association between sibling relationship quality and the positive and negative indicators of child psychosocial functioning under investigation in the present study.
Despite evidence that sibling relationship quality may be a salient predictor of child adjustment in the context of negative life-events, until now no empirical study has examined sibling relationship quality in the context of parental cancer. However, it is relevant to examine this topic, because a supportive sibling relationship could be beneficial in this context, whereas a conflictive sibling relationship could be a complicating factor. Research on potentially beneficial or complicating effects of sibling relationships in families affected by parental cancer could provide valuable knowledge. In turn, this might inform theorizing about mechanisms predicting child adjustment in these challenging situations, as well as the further development of (family) interventions fostering adjustment.
In families facing parental cancer, the adjustment of children and adolescents is likely affected by a combination of dyadic and individual factors. It is important to recognize that, besides dyadic factors such as sibling relationship quality, individual factors also play a pivotal role in predicting child and adolescent adjustment. One potentially critical individual factor is emotion regulation. Emotion regulation refers to the capacity to effectively manage one’s internal emotional experiences and outward expressions (Gross, 1998). Research has established a consistent association between emotion regulation and quality of life, satisfaction with life, and PTSS. For example, several studies have shown that effective emotion regulation was significantly linked to higher perceived quality of life in college students (Haga et al., 2009) and adults (Schutte et al., 2009). Additionally, Villalta et al.’s (2018) meta-analysis of 41 studies found that children and adolescents with more severe PTSS also reported more emotion regulation problems.
There are reasons to assume that the association between sibling relationship quality and the adjustment of children and adolescents to stressful events may not only be direct but might be partially or fully mediated by emotion regulation. Previous studies have suggested that the quality of sibling relationships is linked to the development of emotion regulation skills (Kramer, 2014; Lindsey, 2020), and that difficulties in emotion regulation, in turn, are associated with quality of life and PTSS (Egberts et al., 2022; Haga et al., 2009; Schutte et al., 2009). Combining these patterns, a mediation model may offer a suitable framework to explain the intricate interplay between these factors, shedding light on how sibling relationship quality indirectly affects child functioning through its impact on emotion regulation. However, studies examining emotion regulation as a possible mediator between sibling relationship quality and indices of child wellbeing and (mal)adjustment are lacking. As one exception, Padilla-Walker et al. (2010) found that adolescents’ ability to regulate their own behavior, emotions, and cognitions partially mediated the link between sibling affection and adolescent externalizing and internalizing behaviors. Besides a direct effect of sibling affection on adolescent externalizing problems, higher levels of sibling affection were linked to better child self-regulation, which was in turn associated with less externalizing and internalizing problems. In contrast, for sibling hostility, only a direct effect on adolescent internalizing problem behavior was found but no indirect effects. Sibling hostility was not associated with adolescents’ ability to regulate their own behavior, emotions, and cognitions. It is important to note that Padilla-Walker et al.’s study used a community sample and focused on mild internalizing and externalizing problems, so their findings may not generalize to a sample of families affected by parental cancer and to PTSS, quality of life and satisfaction with life. Notwithstanding these methodological differences from our study, their findings do suggest that the links between sibling relationship quality and child (mal)adjustment could indeed be partially mediated by emotion regulation.
Parental cancer may increase the likelihood of children developing difficulties in regulating their emotions. This is because the serious illness of a parent can elicit strong emotional responses in children which, in turn, places greater demands on their ability to manage and control their emotions (Katz et al., 2007, 2016). Children who struggle with emotional regulation face an elevated risk of experiencing PTSS (Badour & Feldner, 2013; Katz et al., 2016). Children and adolescents who experience more sibling warmth and less sibling conflict may feel more supported and comfortable to share their emotions with others in times of stress (i.e., are better able to regulate their emotions), which in turn might increase their quality of life and satisfaction with life and might decrease the risk for PTSS. However, to our knowledge, whether emotion regulation serves as a mechanism explaining the associations of sibling warmth and conflict with child quality of life and satisfaction with life as well as PTSS has not yet been studied. Examining these possible mediation patterns was therefore an additional aim of the present study.
The present study
The aims of the current study were to examine (1) associations of sibling relationship quality (i.e., sibling warmth and sibling conflict) and emotion regulation problems with indices of child functioning (i.e., quality of life, satisfaction with life, and cancer-related PTSS) in families with parental cancer; and (2) whether emotion regulation problems partially or fully mediate the associations between sibling relationship quality and child functioning.
Based on theoretical and empirical considerations, we expected that less sibling warmth and more sibling conflict would be linked to more emotion regulation problems, lower quality of life, lower satisfaction with life, and more PTSS. We also expected that more emotion regulation problems would be associated with lower quality of life, lower satisfaction with life, and more PTSS. Finally, we expected that the links between sibling relationship quality and child functioning would be at least partially mediated by emotion regulation problems.
Method
Procedure
This study is part of a larger longitudinal Dutch study on family adjustment after parental cancer. Families were eligible to participate if one of the parents had a current or past cancer diagnosis and had at least one child in the age of 0–18 years. Children from 8 to 18 years old were eligible to participate themselves 1 . Exclusion criteria included insufficient Dutch language proficiency and terminal stage of cancer.
Between September 2015 and April 2019, and between November 2019 and February 2020, families were recruited via announcements on social media, health care providers, and cancer support centers in the Netherlands. After signing up, parents were contacted to receive study details, discuss eligibility, and to participate in a semi-structured interview to gather information about illness and family characteristics. Data were obtained through questionnaires filled out by parents and children. Trained research assistants carried out home visits to support children in filling out the questionnaires. Participating parents and children all provided written informed consent.
The study was approved by the ethics committee of the Faculty of Social and Behavioral Sciences of Utrecht University (FETC15-061).
Sample
Sample characteristics.
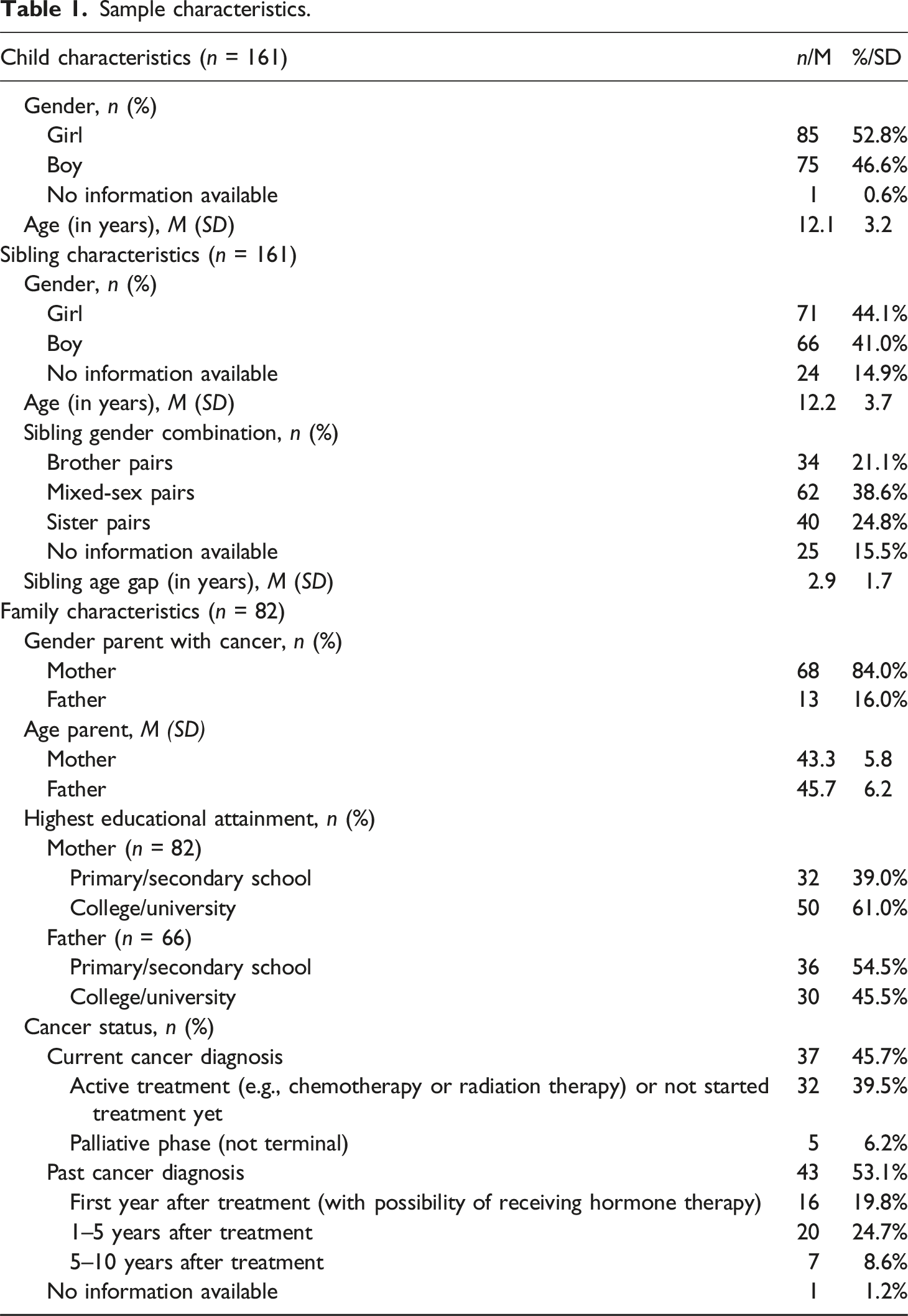
In these 82 families, cancer status was as follows: 45.7% had a current cancer diagnosis (i.e., briefly after diagnosis, in active treatment or no treatment) and 53.1% had a past cancer diagnosis (i.e., 1–10 years after completing treatment). Almost all parents had the Dutch nationality (98.6%; 1.4% had the Moroccan nationality). In 21 families (25.6%) one child participated in the study, in 47 families (57.3%) two children participated, in 10 families (12.2%) three children participated and in 4 families (4.9%) four children participated in the study.
The 161 children in our sample were aged between 6 and 20 years, with a mean age of 12.1 years (SD = 3.1 years), and 53.1% identified as girls and 46.9% as boys. They reported about the relationship with their siblings, whose mean age was 12.2 years (range 3–24 years) and a mean age difference between siblings of 2.9 years (range 0–8 years). Concerning sibling gender combinations, 25% were boys reporting on the relationship with their brother, 22.8% were boys reporting about their sister, 22.8% were girls reporting about the relationship with their brother and 29.4% were girls reporting about their sister.
Children filled out questionnaires assessing sibling relationship quality, emotion regulation problems, quality of life, satisfaction with life, and PTSS.
Measures
Sibling relationship quality
Sibling warmth and conflict were measured with 21 items of the Sibling Relationship Questionnaire (SRQ; Buhrmester & Furman, 1990). Children were asked to fill out questions about the relationship with their sibling. If they had more than one sibling, they were free to choose the sibling about whom they filled out the questionnaire. This approach stimulated participating children to provide information about the sibling relationship most salient for them.
All items were rated along a 5-point Likert-scale ranging from 1 = hardly at all to 5 = extremely much. The Warmth scale (15 items) consists of items reflecting sibling affection, companionship, intimacy, and admiration, and had a Cronbach’s alpha of .90. A sample item is, “How much do you and this sibling care about each other?”. The Conflict scale (6 items) consists of items indicating the degree of quarreling and antagonism between siblings and had a Cronbach’s alpha of .91. A sample item is, “How often are you and this sibling mean to each other?”. The Dutch SRQ has been found a valid and reliable measure of sibling warmth and conflict (Buist & Vermande, 2014; Derkman et al., 2010).
Emotion regulation problems
Emotion regulation problems were assessed with the Emotional control subscale of the Behavior Rating Inventory of Executive Function (BRIEF; Gioia et al., 2000). Children were asked to indicate how often they showed a given behavior during the past 6 months on a scale of 1 = Never, 2 = Sometimes, and 3 = Often. The Emotional control scale consists of 10 items measuring the capacity to modulate emotional responses. Sample items are, “I become upset too easily” and “I have explosive, angry outbursts”. Higher scores indicate more problems with emotion regulation. The Dutch BRIEF has been found a valid and reliable measure of emotion regulation problems in children between 5 and 18 years of age (Huizinga & Smidts, 2010). Cronbach’s alpha in the present study was .85.
Quality of life
Children reported on their quality of life through the KIDSCREEN-27 (Ravens-Sieberer et al., 2007). This 27-item questionnaire assesses quality of life across five dimensions, namely physical well-being (five items), psychological well-being (seven items), parent relations and autonomy (seven items), social support and peers (four items), and school environment (four items). Items are rated on a 5-point Likert scale, with 1 = not at all to 5 = extremely or (for some items) 1 = never to 5 = always. Cronbach’s alpha of the total Quality of Life scale was .89.
Satisfaction with life
Satisfaction with life was assessed with the Satisfaction With Life Scale for Children (SWLS-C). This scale is an adaptation of the Satisfaction With Life Scale (Diener et al., 1985), which assesses global life satisfaction. The SWLS-C consists of five items (e.g., “In most ways my life is close to the way I want it to be”) rated on a 7-point Likert scale (ranging from 1 = strongly disagree to 7 = strongly agree). A validation study of the SWLS-C has indicated sound psychometric properties, including adequate construct validity for children aged 9–14 years (Gadermann et al., 2010). The SWLS demonstrated good reliability (Cronbach’s a = .82) in the current sample.
Posttraumatic stress symptoms
Children reported on PTSS with the Child PTSD Symptoms Scale (CPSS; Foa et al., 2001). Children were asked to rate their symptoms in relation to their parent having cancer and its consequences. The CPSS assesses the frequency of 17 PTSD symptoms (as per DSM–IV; (American Psychiatric Association, 2000) throughout three symptom clusters: reexperiencing, avoidance, and hyperarousal. The 17 symptom items (e.g., “During the last two weeks, how often have you tried to avoid activities, people, or places that remind you of the event [your parent having cancer]?”) are rated on a 4-point Likert scale (0 = not at all, 1 = once a week or less, 2 = two to four times a week, 3 = five or more times per week). The total score is calculated by summing all items. This scale was developed for children aged 8–18 years and has good reliability and validity (Foa et al., 2001; Nixon et al., 2013). Cronbach’s alpha of the total scale was .85, indicating good reliability.
Analytic plan
To examine direct and indirect paths between sibling relationship quality, emotion regulation problems, and three indices of child functioning, we conducted mediation path analyses in Mplus (Muthén & Muthén, 1998-2017, version 8.7). We formulated a model in which sibling warmth and sibling conflict and emotion regulation problems predicted quality of life, satisfaction with life, and PTSS. We also included paths from sibling warmth and sibling conflict to emotion regulation problems. Finally, we estimated indirect effects from sibling warmth and sibling conflict on all three outcome variables, mediated by emotion regulation problems. See Figure 1 for the estimated model. In this model, we included child age and gender, sibling gender combination, and age gap between siblings, as well as cancer status as covariates (loading on the predictors as well as outcome variables). Cancer status was operationalized as a dichotomous variable with values reflecting either current cancer diagnosis (i.e., not started treatment yet, active treatment, or palliative phase (but not terminal)) or past cancer diagnosis (0–10 years after treatment). Diagram of the estimated model.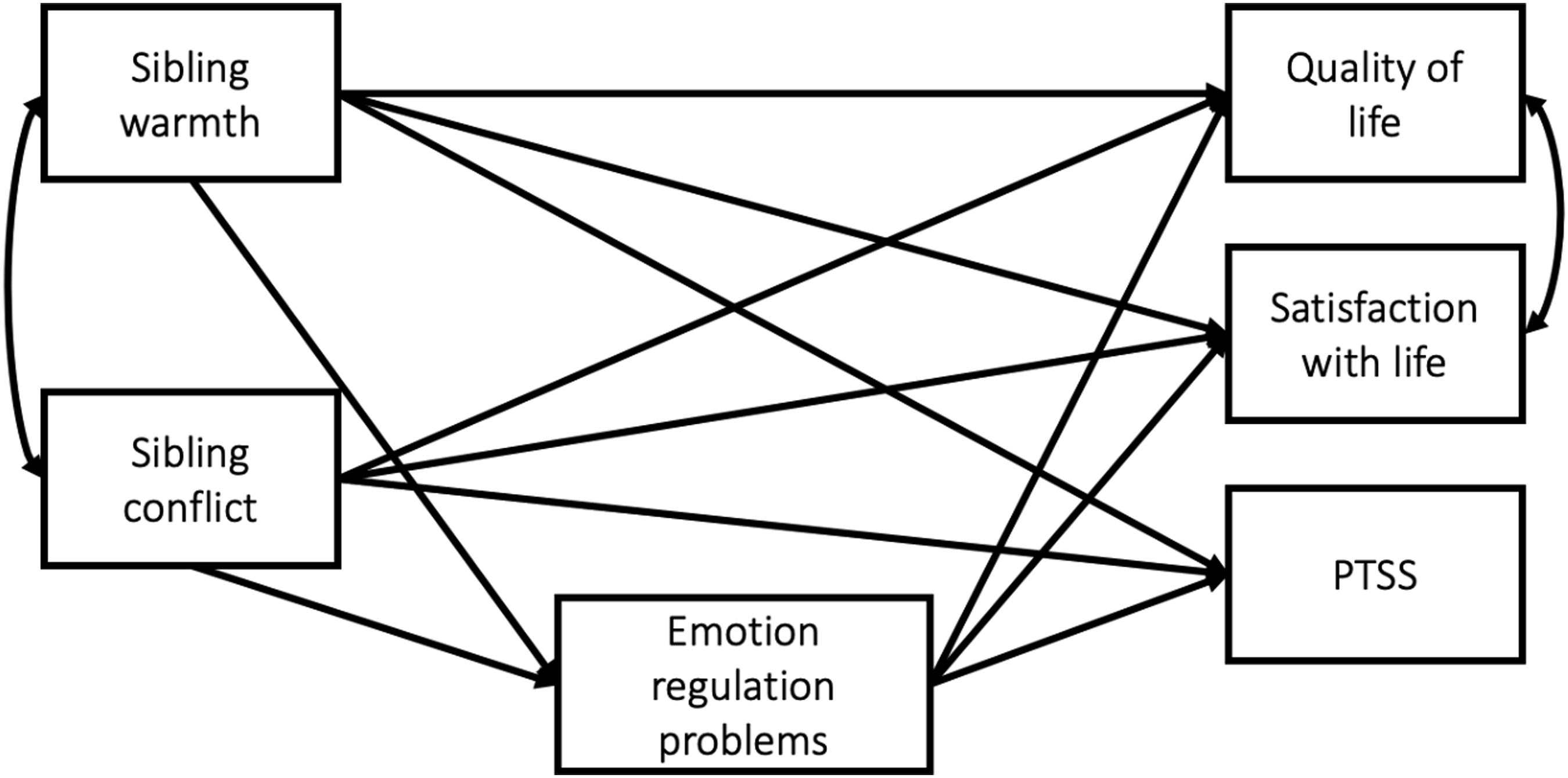
In many families, multiple children participated in the study. To control for the clustered nature of our data, we applied cluster-robust standard errors in Mplus, using family code as a cluster variable and MLR estimation. Cluster-robust standard errors have the advantage that they can be used without any change to the presumed model while at the same time fully address the clustered nature of data (McNeish et al., 2017).
Results
Descriptive statistics
Descriptive statistics and correlations study variables (N = 161).
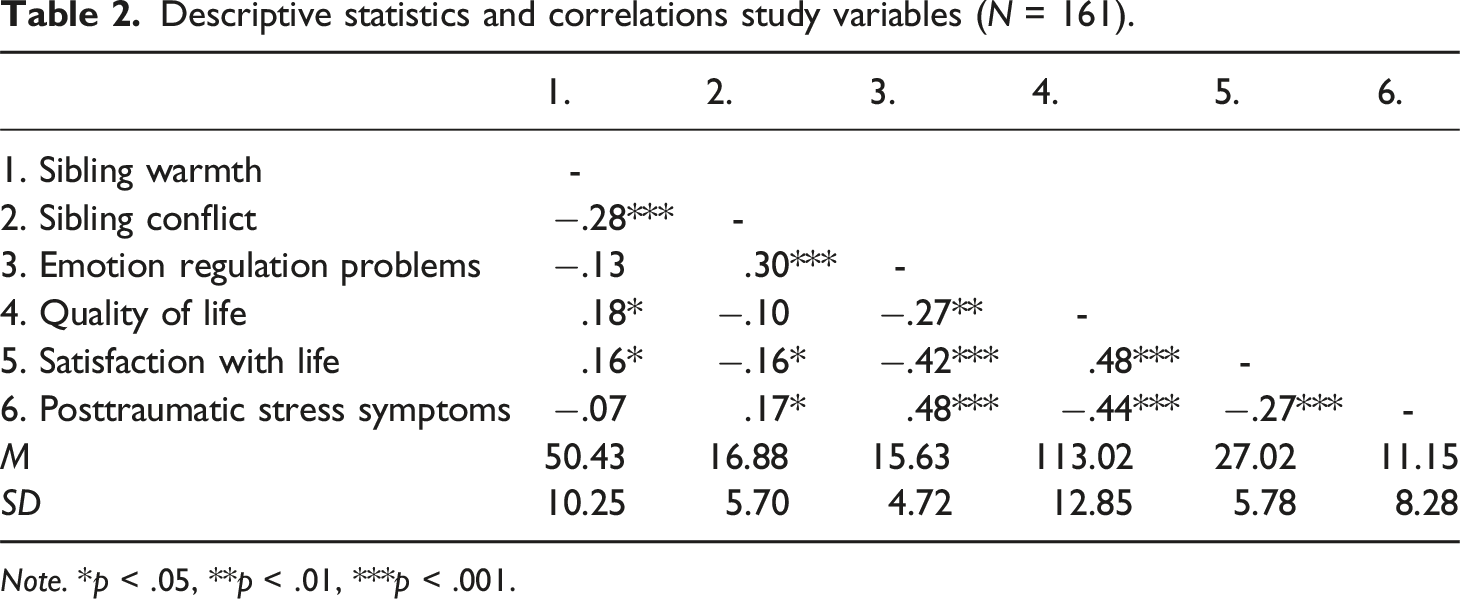
Note. *p < .05, **p < .01, ***p < .001.
Path analysis
Path analysis in Mplus showed that sibling warmth was not significantly associated with emotion regulation problems (β = .034, p = .694). Additionally, we found no significant direct nor indirect effects of sibling warmth on quality of life, satisfaction with life, or PTSS (see Figure 2 for an overview of the results and Table 3 for details). Standardized Coefficients Indirect Model (N = 161). Note: The model included child age and gender, sibling gender combination and sibling age difference, as well as cancer status (current vs. past diagnosis) as covariates *p < .05, **p < .01, ***p < .001 Standardized coefficients mediation analysis (N = 161). Note. BRIEF = Behavior Rating Inventory of Executive Function; CI = confidence interval; CPSS = Child PTSD Symptoms Scale; LL = lower limit; SRQ-W/C = Sibling Relationship Questionnaire Warmth/Conflict; SwL = Satisfaction with Life; UL = upper limit. The model included child age and gender, sibling gender combination and sibling age difference, as well as cancer status (current vs. past diagnosis) as covariates. *p < .05, **p < .01, ***p < .001.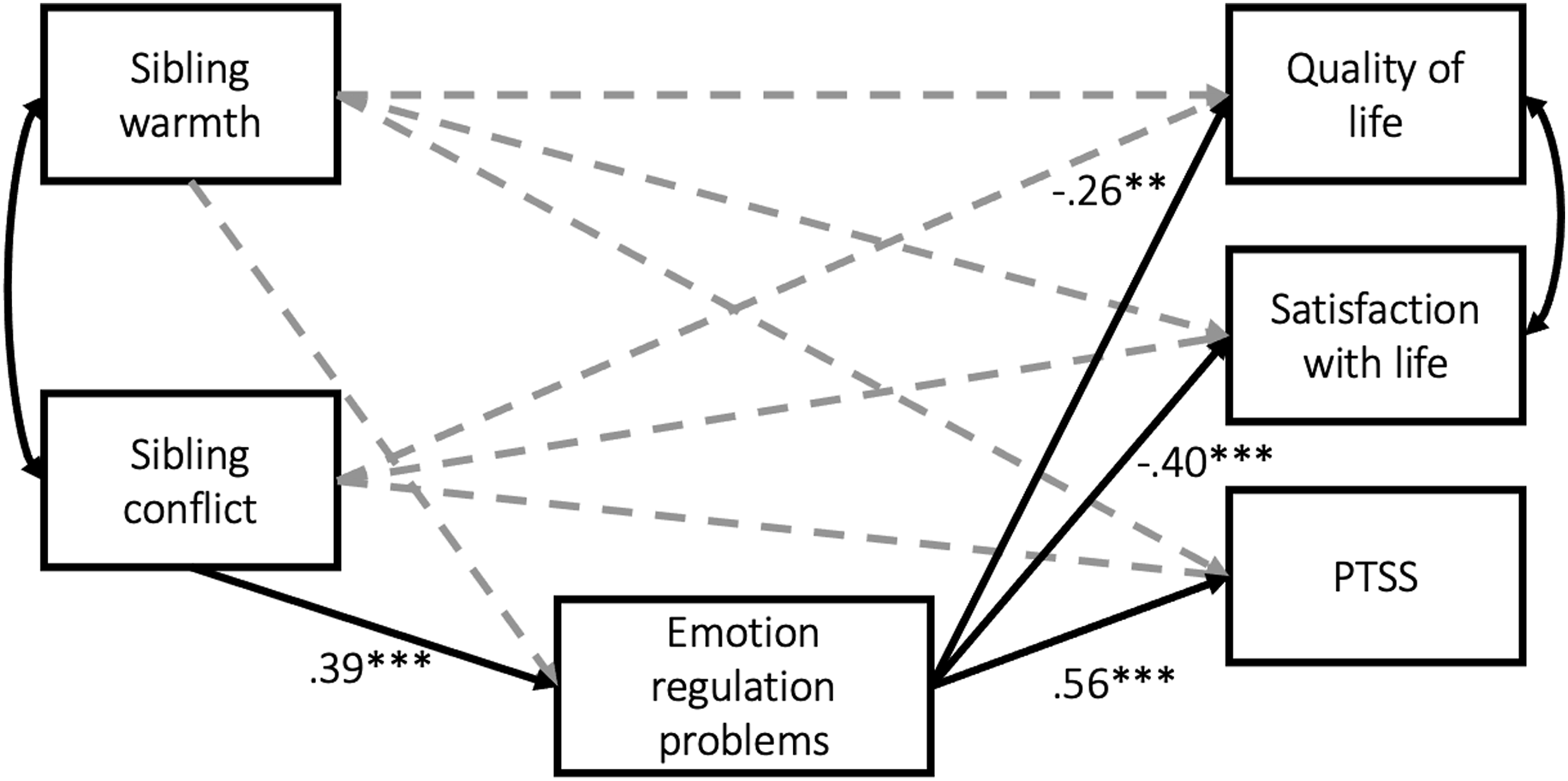
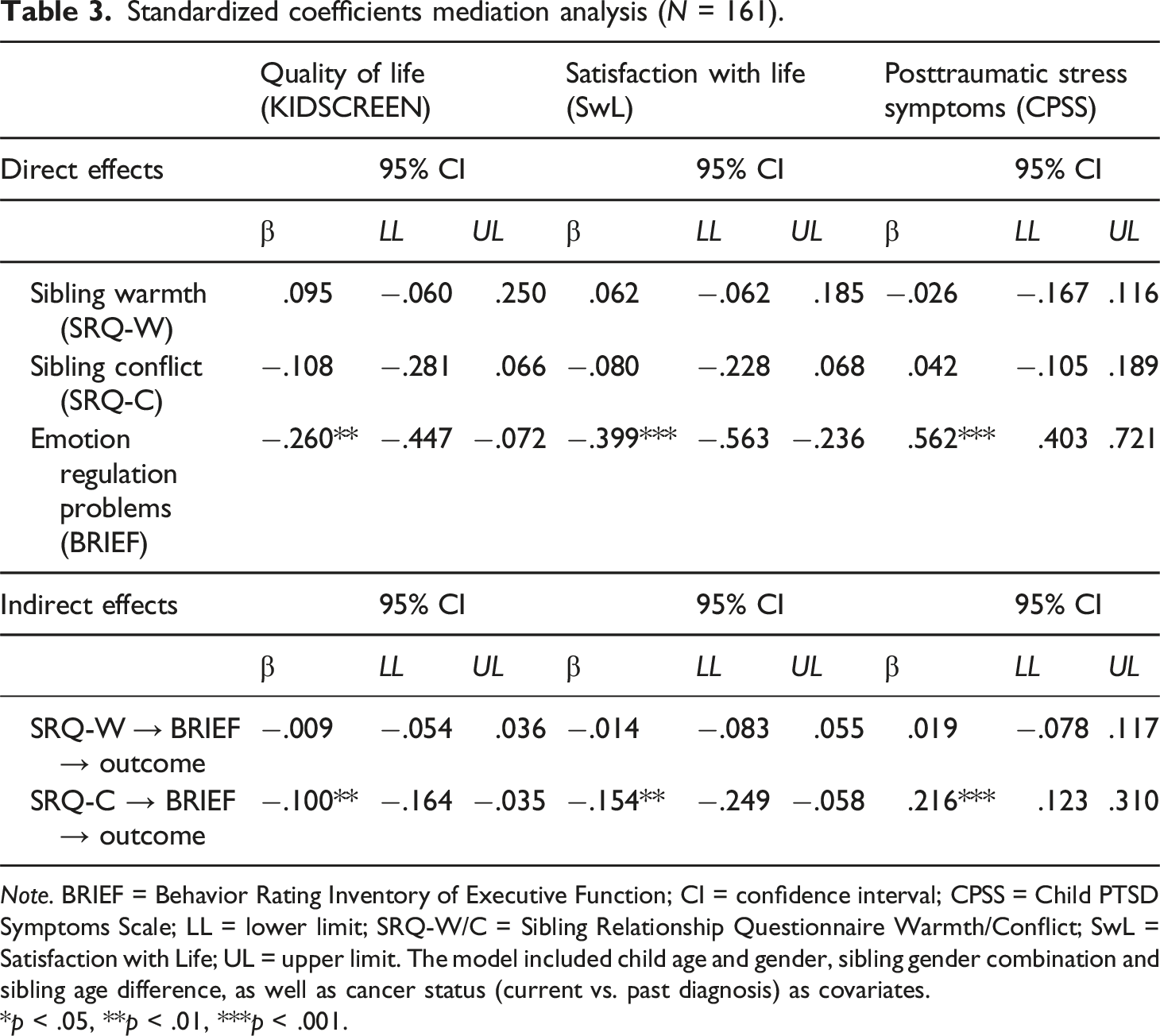
Sibling conflict was significantly associated with emotion regulations problems (β = .385, p < .001), but no statistically significant direct paths were found between sibling conflict and quality of life, satisfaction with life or PTSS. However, we did find a consistent pattern of significant indirect effects, with more sibling conflict linked to lower quality of life (β = −.100, p < .01), lower satisfaction with life (β = −.154, p < .01), and higher levels of PTSS (β = .216, p < .001) through higher levels of emotion regulation problems. Thus, sibling conflict seems to be a risk factor in families with parental cancer by increasing emotion regulation problems which in turn are linked to decreased child functioning.
We found very few significant paths for the covariates. Cancer status was significantly linked to satisfaction with life (β = .142, p < .05) and emotion regulation problems (β = .247, p < .01). Gender had a positive association with quality of life (β = .155, p < .05) and emotion regulations problems (β = .198, p < .05), and sibling gender combination was significantly associated with emotion regulation problems (β = −.268, p < .01). Finally, age had significant negative associations with quality of life (β = −.425, p < .001), satisfaction with life (β = −.377, p < .001), and sibling conflict (β = −.254, p < .01),
Sensitivity analyses
To assess the robustness of our findings, we conducted two sensitivity analyses. As mentioned earlier, in some families, multiple children participated in the study, often reporting about each other. In that case, the dependency of data is the strongest, potentially inflating effect sizes. We therefore reran our model in this subsample of reciprocal sibling dyads (n = 111). Like in the main analysis, we applied cluster-robust standard errors, using family code as a cluster variable and MLR estimation, to control for the interdependency of data. This sensitivity analysis showed virtually identical results for this reciprocal sibling subsample, compared to the total sample. The results of this analysis can be found in Supplemental Table A.
As a second sensitivity analysis we ran a model in which the mediation path was reversed. In this reversed model, sibling relationship quality was included as a mediator of the association between emotion regulation problems and quality of life, satisfaction with life, and PTSS. Results showed that none of the indirect paths from emotion regulation to the three outcome variables via sibling relationship quality were significant. The results of this analysis can be found in Supplemental Table B. In sum, both sensitivity analyses confirmed the robustness of our findings.
Discussion
Aims of the current study were to examine (1) associations of sibling relationship quality, emotion regulation problems with three indices of child functioning in families affected by parental cancer; and (2) whether emotion regulation problems partially or fully mediated these associations.
We expected that less sibling warmth would be linked to more emotion regulation problems, lower quality of life and satisfaction with life, and more PTSS. Whereas bivariate correlation analyses showed significant links between sibling warmth and quality of life and satisfaction with life, these associations were not significant in the full path model containing all hypothesized paths. In fact, sibling warmth was only significantly associated with sibling conflict, but not directly nor indirectly with any of the other study variables.
We also expected that more sibling conflict would be linked to more emotion regulation problems, lower quality of life, lower satisfaction with life, and more PTSS. Again, bivariate correlations largely confirmed this hypothesis. However, the full path model showed a different pattern. Whereas we found no significant direct effects of sibling conflict on any of the outcomes, we did find significant indirect effects of more sibling conflict on all outcomes through more emotion regulation problems.
Our finding that sibling conflict is more strongly associated with child and adolescent functioning than sibling warmth is consistent with earlier work: A meta-analysis examining both sibling warmth and conflict demonstrated that the effects of sibling conflict on internalizing and externalizing problems were much stronger (Buist et al., 2013). The relatively few studies focusing specifically on PTSS seem to confirm that mainly higher levels of sibling conflict (and not lower sibling warmth) predict increased PTSS (Palosaari et al., 2016; Peltonen et al., 2010). Our findings show that in the context of parental cancer, sibling conflict seems to have a stronger link with child and adolescent quality of life, satisfaction with life, and PTSS than sibling warmth, which does not seem to have a meaningful protective role in this context. The processes involved appear to be indirect, in that sibling conflict increases emotion regulation problems, which in turn decrease quality of life and satisfaction with life and increase PTSS.
Consistent with our expectations, we found that more emotion regulation problems were significantly directly associated with lower quality of and satisfaction with life, as well as with more PTSS. Both the bivariate correlation analyses and the full path model supported this hypothesis. Children who have more difficulties in regulating their emotional responses also report lower quality of life, lower satisfaction with life and increased PTSS.
Combined, these results point to emotion regulation problems as a key construct in explaining both positive and negative indicators of child and adolescent functioning in families with parental cancer. This is in line with earlier work demonstrating that constructive emotion regulation strategies (e.g., reappraisal) are linked to higher satisfaction with life, and that destructive emotion regulation strategies such as suppression are linked to lower satisfaction with life (Haga et al., 2009; Schutte et al., 2009). Besides positive outcomes (e.g., satisfaction with life) emotion regulation problems have also been linked to negative indicators of functioning such as child PTSS (Egberts et al., 2022; Villalta et al., 2018).
The current findings shed further light on the role of emotion regulation problems in the family context. More sibling conflict might compromise a child’s abilities to reflect on their emotions and to accept or manage them, which limits the ability to cope with the stressful situation of having a parent with cancer. Moreover, sibling conflict may be an additional burden on top of the stressors associated with parental cancer, with negative effects on child emotion regulation and functioning. These potentially underlying mechanisms warrant further research.
Strengths and limitations
To our knowledge, our study is the first study to examine the role of positive and negative aspects of sibling relationship quality in children’s functioning in the context of parental cancer, including both positive and negative indicators of the child’s functioning. A further strength is that we examined the robustness of our findings in several sensitivity analyses, which confirmed our findings. Notwithstanding these strengths, our study also had a number of limitations.
First, our sample was relatively small. This limits the statistical power to examine these complex processes, although we were able to partly confirm our hypotheses. Additionally, it is not entirely clear whether our sample is representative of families affected by parental cancer. Our recruitment method was designed to leave the initiative of participation with the families. This may have created a self-selection bias. However, when dealing with people in vulnerable situations, such as families facing a health crisis, it remains of the utmost importance to avoid placing any extra burden or pressure on them as much as possible.
Another limitation is that we used cross-sectional data to test our mediation models. Whereas cross-sectional data do not preclude the testing of mediation hypotheses (Hayes, 2013), future research utilizing longitudinal designs could test the robustness of our findings and examine these processes over time. Relatedly, the quality of the sibling relationship was only assessed after the parental cancer diagnosis, so it is unknown whether the quality of this relationship changed in response to parental cancer. It would be relevant to further study these potential changes in the sibling relationship as perceived by children and relate these to indices of child functioning.
Some potentially important characteristics of participants (e.g., physical or cognitive ability; sexual orientation) were not registered and future research is needed to examine if these characteristics affect the associations examined in this study.
Finally, we used a broad measure to assess emotion regulation problems. Moving forward, it could be fruitful to examine the patterns under investigation with measures that tap into different emotion regulation strategies (Lindsey, 2020).
Conclusion
Our study suggests that sibling conflict is a potential risk factor for psychosocial problems in families with parental cancer. Sibling conflict appears to have a detrimental effect on emotion regulation skills, which in turn may lead to lower quality of life and satisfaction with life, and more PTSS.
If our findings are confirmed in future longitudinal research, they may have important theoretical and clinical implications. From a theoretical viewpoint, it may be useful to further investigate what other negative aspects of the sibling relationship may affect children’s functioning in the context of parental cancer and to what extent positive aspects (other than warmth) may play a role in this context.
From a clinical perspective, our findings could inform the improvement and application of interventions aimed at improving sibling relationship quality. Up to now, interventions for families facing parental cancer have not included the sibling relationship (see Chong et al., 2024 for an overview). However, outside the context of parental cancer, the relatively few interventions focusing on sibling relationship quality have shown promising results (Kothari et al., 2017). For example, the Siblings Are Special program (Feinberg et al., 2013) and the More Fun With Sisters and Brothers Program (Kennedy & Kramer, 2008) successfully increased sibling relationship quality. Additionally, the Promoting Sibling Bonds intervention, specifically aimed at strengthening sibling relationships in foster care, significantly decreased sibling conflict (Linares et al., 2015). Our findings suggest that for interventions aimed at supporting families who are coping with parental cancer, focusing on mitigating negative aspects of the sibling relationship seems more fruitful than focusing on strengthening the positive aspects.
Supplemental Material
Supplemental Material - Associations of sibling relationship quality and emotion regulation with child functioning in families with parental cancer
Supplemental Material for Associations of sibling relationship quality and emotion regulation with child functioning in families with parental cancer by Kirsten L. Buist, Marthe R. Egberts, and Paul A. Boelen in Journal of Social and Personal Relationships
Footnotes
Acknowledgements
We thank all parents and children that participated in this study, all master students that contributed to the data collection and Mariken Spuij for her contribution to the research project.
Author contributions
Our gratitude is also due to Dineke Verkaik and Michelle To for their input on draft versions of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by Pink Ribbon (Grant 2014-193).
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research cannot be publicly shared due to the privacy of the participants but are available from the corresponding author on reasonable request by emailing:
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.