
Abstract
Research examining the effects of severe, prolonged early deprivation has shown elevated rates of neurodevelopmental symptoms, which frequently persist into adulthood and are associated with functional and social relationship difficulties, as well as elevated rates of mental health problems. The behavioural manifestations of these symptoms closely resemble those of ADHD and also ASD. Here, we used qualitative methods to explore and characterise the social experiences and difficulties encountered by young adults exposed to profound early deprivation, in part to highlight any apparent parallels between the experiences in this group and those identified in typically developing samples with ADHD or ASD. To do so, we interviewed young adults and their adoptive parents (N = 18) from the English and Romanian Adoptees study, about their social lives. Participants were keen to describe not only the challenges they faced but also adaptive responses. A semantic/descriptive thematic analysis revealed that the young adults strongly desired social relationships but struggled to navigate social norms, resulting in frustration and frequent loss of relationships. This was accompanied by strong feelings of loss and rejection, all of which were perceived to have a negative impact upon self-esteem and mental health. Adaptive strategies included the fostering of casual friendships with older individuals and seeking employment with strong social components. Similarities and differences between our findings and the social difficulties experienced by typically developing groups with neurodevelopmental problems, and adopted individuals more generally, are discussed.
Keywords
Prolonged, early and severe deprivation has been shown to increase the risk of neurodevelopmental conditions, particularly symptoms of attention deficit hyperactivity disorder (ADHD), Autism Spectrum Disorder (ASD), Disinhibited Social Engagement Disorder (DSE) and Cognitive Impairment (CI) (Rutter & Sonuga-Barke, 2010). These symptoms appear to have strong persistence into adulthood (except in the case of CI which shows signs of remittance) and have been shown to be risk factors for adult onset of emotional problems (i.e., symptoms of depression and anxiety, see Sonuga-Barke et al., 2017). Quantitative cascade models show that this association is partly mediated by social difficulties (Golm et al., 2020; Rizeq et al., 2022). Relatedly, there is evidence that the development and maintenance of positive peer relationships may promote resilience against some mental health issues for individuals who have endured neglect in the early years of life (Collishaw et al., 2007). Whilst these quantitative studies can help identify particular risk and protective factors, they are not suited for characterising specific mechanisms and informing interventions. This is particularly salient in an area as broad and complex as social relationship difficulties, which can take many forms, including withdrawal, patterns of conflict and problems in navigating complex societal norms (Hill et al., 2008).
The English and Romanian adoptee (ERA) study provides a valuable opportunity to explore these issues. It follows the development of children who experienced severe institutional neglect during infancy within Romanian residential childcare institutions in the late 1980s before being adopted by UK families (Sonuga-Barke et al., 2017). From the 1960’s until the late 1980s, Nicolae Ceausescu implemented policies to increase the population in Romania. However, due to widespread poverty, many families could not afford to support their children and handed them over to the State to be raised in residential care institutions. With growing economic problems, during the 1980s Romania’s childcare institutions became increasingly poorly provisioned and support workers within them were overwhelmed (Kligman, 1998; Morrison, 2004; Rutter et al., 2010; Ward, 2011). The conditions in residential childcare institutions were often described to vary from poor to appalling with children confined to cots, few toys, if any, to play with, very little personalised attention and caregiving, and an environment that was often physically harsh (Rutter et al., 2010). Despite improvements in the care system in Romania and a commitment by all United Nations member States to put an end to child institutionalisation (United Nations General Assembly, 2020), globally there are millions of children still reared in institutional care (van IJzendoorn et al., 2020).
The ERA study is a prospective longitudinal study with assessments across childhood, adolescence, and young adulthood and is consequently well placed for investigating the social lives of those with a history of adversity. Whilst social relationships during adulthood in previously and globally deprived individuals remain understudied, previous work has investigated this issue in the ERA sample in childhood. This work showed that at age 4, those exposed to deprivation showed a pattern of disrupted social interactions, including difficulties referencing others’ mental states and restricted pretend play (Kreppner et al., 1999). At age 15, peer problems were again found in those exposed to early deprivation (Sonuga-Barke et al., 2010). These findings are aligned with the broader literature on social relationships in those with a history of early adversity during childhood and adolescence (e.g., Waldinger et al., 2002).
Meanwhile, studies of social relationships in adoptees in general (many of whom will have been exposed to early adversities) have tended to focus on disruptions of early attachments and subsequent difficulties forming close bonds during adolescence, and, to a more limited extent, into adulthood, albeit with a clear focus on romantic rather than peer relationships (Field & Pond, 2018). In general, this literature shows more similarities than differences between adopted and non-adopted individuals with the majority of adopted adults reported to be well-adjusted (e.g., Borders et al., 2000), although elevated rates of social difficulties are also reported (Feeney et al., 2017). Quantitative work has shown that one area of difficulty is a greater risk of insecure attachment in adulthood (e.g., Borders et al., 2000). More experiential focused work has highlighted a heightened sensitivity to fear, loss and rejection (e.g., Corder, 2012), and an avoidance of interpersonal closeness and difficulties trusting others (e.g., Nowlan, 2016). There is also evidence to suggest that social relationship difficulties are associated with the specific type of early adversity experienced with experiences of abuse being linked with oppositionality towards others while experiences of neglect have been linked with anxiousness (Waldinger et al., 2001). Importantly, there is a consensus among researchers that these issues frequently persist into adulthood (Janus, 1997; Pivnick, 2010).
Theoretical frameworks have stressed the importance of social contexts and social experiences with peers, friends and family in providing critical feedback for the development of self-concepts (Hartup & Stevens, 1997; Prinstein & Giletta, 2016; Swann et al., 2007), which in turn have been related to mental health outcomes for adoptees (Collishaw et al., 2007). Importantly, the period of transition to adulthood is characterised by key developmental tasks such as gaining greater independence from one’s family and forming strong social ties, including romantic relationships. It is also considered a significant time for identity exploration and consolidation (Arnett, 2000). These novel demands on the self and relationships require the development of more complex social competencies (Cashen & Grotevant, 2020). The ways in which the social demands of this period are managed can have profound implications for sense of self and wellbeing.
Studies that have focused on the associations between neurodevelopmental conditions and social relationships have primarily focused on relationship experiences of children with ADHD and ASD. Our focus here is mainly on ADHD in adulthood, given A) the historical focus on childhood and adolescence, B) that it has been found to be most common among those with a history of adversity and C) its link with poorer functioning (Kennedy et al., 2016; Sonuga-Barke et al., 2017). The literature on typically developing ADHD paints a picture of impaired social functioning and fewer social relationships. There is a broad consensus among researchers that those with ADHD are criticised and admonished socially to a greater degree than their non-ADHD peers, particularly around perceived inattention and emotion dysregulation (Beaton et al., 2022) and that this pattern of criticism appears to persist into adulthood (Beaton et al., 2020). Other studies, including experimental and peer informant designs, suggest that those displaying ADHD behaviours tend to be less liked by their peers and are more likely to be avoided socially and consequently may struggle to establish friendships (Paulson et al., 2005; Pelham & Bender, 1982). When friendships are established, there is evidence to suggest that they tend to be characterised by greater conflict and are less reciprocity (Normand et al., 2013) and that there may be a heightened sensitivity to rejection (Bondü & Esser, 2015). For the most part it is unclear whether these difficulties persist into adulthood. However, they are thought to be a risk factor for later conduct problems and substance misuse (Soucisse et al., 2015).
There is also evidence showing that ASD symptoms may also be associated with problematic outcomes (Rodriguez-Perez et al., 2023). It has been documented that autistic adults are equally likely to desire social relationships as their non-autistic peers, despite struggling to navigate and maintain them (e.g., Creswell et al., 2019). Some of these challenges include misinterpreting social cues and misunderstanding the mental and emotional states of others (Muller et al., 2008). This may lead to fewer social connections overall and friendships which tend to revolve around activities rather than reciprocal emotional bonding (Petrina et al., 2014). Nevertheless, when not experienced as burdensome, social connectivity can play an important role in psychological well-being (Cassidy et al., 2018). Consequently, some studies have begun to investigate the positive role that neurodivergent peer groups might play, given the fatigue and effort required to maintain social connections with neurotypical individuals (e.g., Crompton et al., 2020).
Objectives
Given the unique combination of a history of early deprivation followed by adoption and the presence and persistence of symptoms of neurodevelopmental conditions, this study documents the social experiences of a selected group from the ERA sample who experienced prolonged deprivation in early life and present with patterns of ADHD in adulthood. The objective is to identify potential areas of challenge and strengths in this sample.
Qualitative work is well suited to exploring complex lived experiences (Macgowan, 2008). Specifically, by using a semantic/descriptive qualitative approach, we are able to characterize our participants’ experiences, with a view to informing both theories and interventions and to relate these experiences to what is already known about early adversity, adoption and neurodevelopmental conditions. Given that ADHD symptoms have been shown to apply most broadly to those with a history of early deprivation and their role in predicting poorer outcomes, this study is based on a selected sub-sample of the ERA cohort of those who had spent at least six months in a Romanian institution and who showed elevated presence of ADHD symptoms and co-occurring conditions in adolescence. To better understand experiences of social relationships in this group, the current study conducted a reflexive thematic analysis of a series of semi-structured interviews, which were held separately with the adoptees themselves and their parents – the latter providing a valuable additional perspective. Our research was guided by three main questions: • RQ1: What are the experiences of adult social relationships in this group? • RQ2: What do parents and young adults see as the perceived areas of difficulty and strengths, in relation to social relationships? • RQ3: What are parents’ and young adults’ perceptions of the impact of social relationship difficulties, particularly on wellbeing and mental health?
Method
Participants
The ERA study recruited its sample from a pool of 342 children who were adopted from Romania into the UK via legal channels between 1990 and 1992. Using stratified random sampling by age at placement and gender, where possible, 144 institution-reared and 21 children who were otherwise deprived but had not experienced institutional care were entered into the study, alongside 52 children adopted as young infants from within the UK who had not experienced deprivation (see Rutter et al., 2010 for details). Both young adults and their parents were invited to participate and both were aware of the other’s participation.
For this study, we focused on adoptees who had spent more than the first 6 months of life in Romanian care institutions and who exhibited a complex pattern of overlapping neuro-developmental problems previously described in individuals who suffered extended deprivation (Sonuga-Barke et al., 2017). The presence of ADHD symptoms during the transition to young adulthood has been shown to be an important predictor of functional impairment in young adulthood (Kennedy et al., 2016), and our strategy focused on the presence of ADHD based on our research assessment when adoptees were 15 years old. ADHD symptoms at age 15 were frequently associated with a broader pattern of problems including ASD, CI and DSE (Kennedy et al., 2016, 2017). 95 participants in the ERA cohort (total N = 217) had spent at least their first 6 months of life in Romanian orphanages. 18 of these participants met DSM criteria for ADHD at age 15. Of these 18, 16 adoptees agreed to participate in this part of the study. As well as ADHD, 69% met criteria for at least one other deprivation-related problem at age 15 (22% CI, 28% DSE, 28% ASD). The adoptees were on average 19.06 months old (SD = 8.71) when they left their institutions and entered the UK. At the time of interviews, the young adults were on average 24.70 years old (SD = 0.79), 62% were men, 47% were not in employment, education or training, 59% had left education following post compulsory GCSEs and 17% were registered as disabled.
Parents of all 18 eligible young adults agreed to participate. The mean age of the parents was 60.62 years (SD = 4.23). In 10 cases, parent interviews were conducted with adoptive mothers and fathers at the same time. In 7 cases, parent interviews were conducted only with mothers, in 1 case an interview was conducted only with a father. All participants gave informed consent for the larger follow-up assessment, of which the interviews formed a part.
Procedure
Semi-structured interviews were used, following a standard topic guide. The topics explored participants’ perceptions of the journey from adolescence to adulthood; any challenges they faced during the transition, and how they managed these; becoming more independent; relationship experiences; and perceptions of achievements. Interviews took place in the individuals’ homes and were conducted by either the first or fourth author. The researchers were instructed to be flexible in their interviewing (e.g., to provide prompts where necessary, allow for breaks, provide opportunities to reflect on and revisit previous questions) to accommodate neurodiversity and variations in mental health in this sample. Interviewers were also instructed to halt interviews should a participant become upset or uncomfortable. Interviews lasted on average 39 minutes with young adults and 41 minutes with their parents. In accordance with good practice, interviews were recorded and transcribed with written consent from participants and all data were anonymised during analysis. Transcription was ‘intelligent verbatim’ (Bucholtz, 2000), whereby verbal utterances (e.g., “uhm” and “ah”) were retained but non-verbal (e.g., sighs and laughter) were not. All named were replaced by pseudonyms. Ethical approval was obtained via the University of Southampton, UK.
Qualitative data analysis
Given our study aims, we chose inductive, reflective thematic analysis as appropriate (Braun & Clarke, 2019). Given that thematic analysis is not tied to any specific theory or epistemological perspective, we applied Shenton’s (2004) four strategies (credibility, transferability, dependability and confirmability) to ensure that our approach was trustworthy and sufficiently rigorous. The analyses were conducted by the second author and were completed using NVivo software. The six-step analysis procedure was as follows:
Initially, the young adult and parent transcripts were separated in order to be analysed separately, and the transcripts of the interviews were read repeatedly and each interview recording was listened to. Given that the interviews covered multiple conceptually distinct topics of interest (see Edwards et al., 2023; Edwards et al., 2024), steps 1–3 were carried out in unison with those of our other analyses and then steps 4–6 were conducted separately for each analysis. We estimate that over this period, each transcript would have been read over 100 times.
Steps 1 and 2; initially, the focus of the reading of transcripts was to get a sense of the data, as CE had not been involved with conducting the interviews for the study. CE then moved to active reading in which they made written notes on what the participants indicated was important in relation to topics and experiences relevant to the research questions, they also made written summaries of the transcripts to assist with getting an initial sense of the data set. CE and MK then used Nvivo to read and consider patterns across the transcripts in relation to the focal topic and to develop initial thematic codes (Step 2). Using NVivo, initial case notes were made. (familiarisation with the data). Again using NVivo, initial codes were generated inductively, that is, using a bottom up, data-driven approach, as opposed to being decided a priori. During this process, the data were coded into units of meaning relevant to the research aims via the use of ‘nodes’ in NVivo.
Step 3; codes/nodes were discussed in team meetings. During this process, it was discussed whether the codings contained sufficient context and whether they appeared to be useful in addressing our research questions or whether they could be discarded. In doing so, our work satisfies the criteria of credibility (generation of initial codes). Adoptee and parent interview transcripts and preliminary notes on potential themes were read and cross-referenced by the coder. Codes were expanded upon to include more detail on the adoptees’ self and relationship experiences and parents’ perceptions. Tables presenting candidate theme titles, explanations of the candidate theme titles and examples were formed by the coder (generating themes).
Steps 4 and 5; in the fourth (reviewing themes) and fifth steps (defining themes), candidate themes, explanations of themes and exemplars were again presented at team meetings. The most apt and salient candidate themes in relation to the research aims were selected and developed into themes and sub themes. CE and MK presented candidate themes and exemplars in team meetings, they were critically discussed and evaluated by the team. CE most frequently met with MK, JK and ESB to discuss transcripts, patterns across the transcripts, candidate themes, exemplars, and possible interpretation biases. CE and MK would be asked to develop certain themes further, explore the transcripts or develop different candidate themes, at which point they would re-read the transcripts and develop thematic codes. Larger group meetings with the whole team were arranged after sets of themes had been developed, themes and exemplars were critically discussed and next steps regarding the analysis were considered. Decisions regarding which themes to develop were made in light of what was already known from previous ERA studies, the research questions and whether the themes related to topics which seemed particularly salient to the participants. In discussing the data from multiple perspectives in this manner, we aimed to reduce the impact of any potential bias, thus satisfying the criteria of confirmability. Sixth, data from the transcripts were anonymised. Appropriate quotes were selected for illustrations of themes (producing the report). With regards to transferability, we have included in this report details on the particular exposure to adversity and later demographic information, as well as detailed reflections on similarities and differences between the findings presented here and those from other studies. Regarding dependability, we have characterised the cohort characteristics, including exposures to adversity, quality of the caregiving environments post-adoption and the mental health profiles of our participants both in general and specifically those in the current analyses in detail both in this paper and in our previous publications.
Findings
Themes and sub-themes (N = 18).
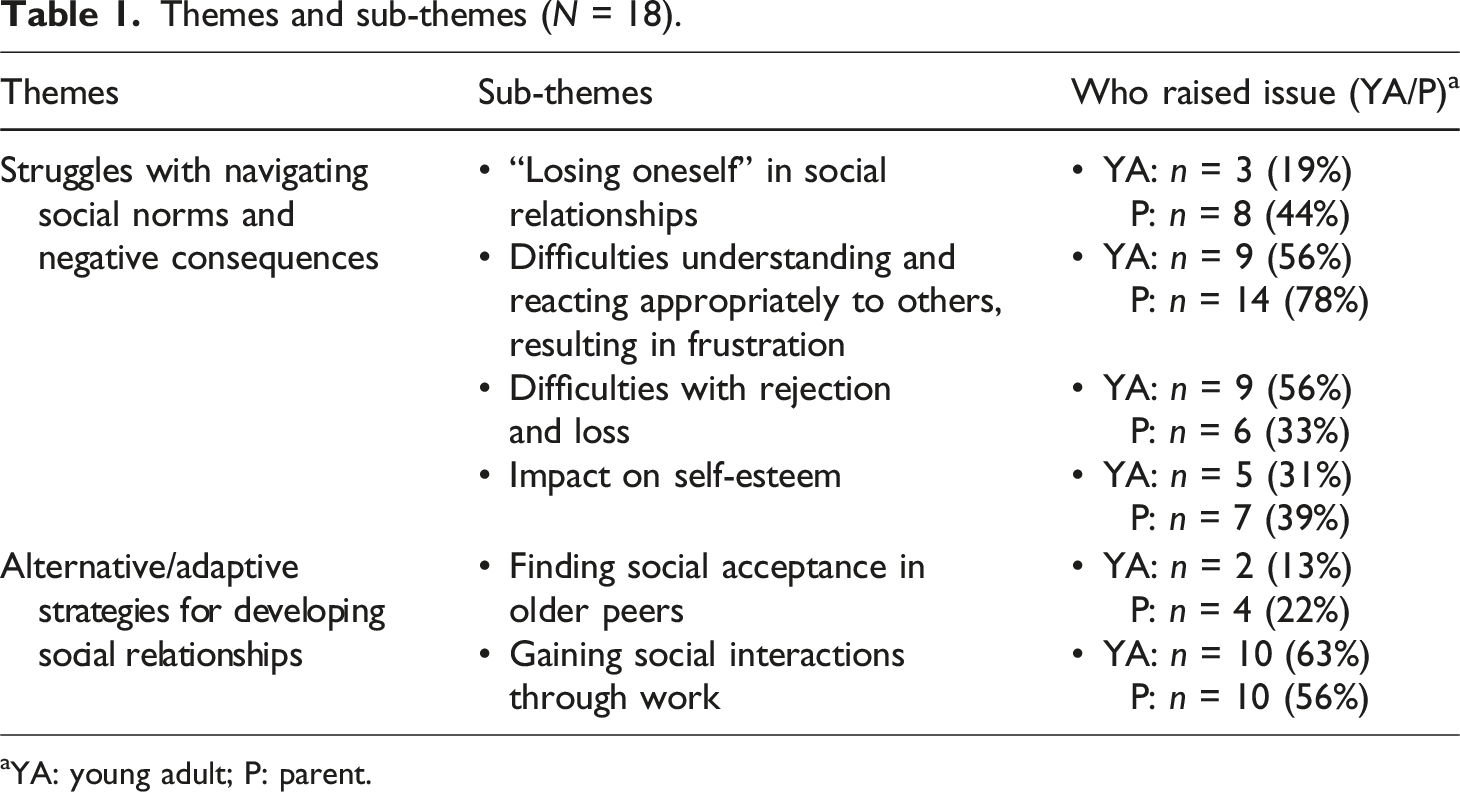
aYA: young adult; P: parent.
Theme 1: Strong desire for social relationships, but struggles with navigating their norms
Our first theme reflects a complex situation whereby the some of the young adults would seek social relationships with such intensity that they would set aside their own needs and even aspects of their own identity. Instead, they focussed predominately on pleasing the other person or changing aspects of themselves to better align with the other person’s persona or interests. Challenges with navigating social norms of relationships were also described, including, for example, difficulties with emotion dysregulation/conflict management and understanding appropriate expectations. The participants also outlined several negative outcomes of these issues.
“Losing oneself” in social relationships
Some parents and to a lesser extent the young adults themselves, described the young people as lacking a robust sense of self: “they are always looking for reassurance.” This was accompanied by a strong desire for social relationships, accompanied by a form of social absorption, whereby the young adult would adapt their own identity to align with their peers. For example, one parent described their child as being: “a real sponge who would absorb anyone around them.” Concerns were raised that some adoptees could lose their autonomy in the company of others. One parent described that their child: Is very outgoing and lively and attractive and appears very confident, but underneath is very vulnerable. And so they (adoptee) become sort of what they (other person) want really, you know.
From some parents’ perspectives, loose boundaries between their children and peers had affected their children’s decisions and actions. For example, some parents believed that their children had difficulty refusing the requests of others; one parent reflected that their child would have “difficulty saying “no” to anything.” Parents also expressed concerns that this had placed their child at risk. For example, one parent explained that their child “wouldn’t want to be on their own and so they would do whatever people wanted for them to, to stay with them (adoptee).”
Difficulties understanding and reacting appropriately to others, resulting in frustration
Most of the young adults and the vast majority of parents (almost 80%) described persistent difficulties with maintaining social relationships. This was described as both a lack of understanding of social norms and not possessing the skills required to navigate social situations effectively. In particular, this seemed to centre around understanding the thoughts and feelings of others and responding appropriately. For example, one parent mentioned that in some circumstances the young person: “will literally laugh when they should not and be upset when there’s no need to be…I mean they really can’t read a social situation very well at all.” This appeared to reflect a persistent and underlying deficit or difference in social appraisals.
While parents tended to focus on what may drive these sorts of interactions, the young adults themselves tended to focus on the immediate consequences that difficulties navigating social situations might cause, highlighting how others would often react negatively even in some cases leading to unwanted confrontations. For example, one young adult described how they would often be misunderstood as acting confrontationally, when they had not intended to: Like my friends always tell me off because I do this like in bars or something, if someone says something stupid, I will be like ‘Why did you say that? What was your reasoning? What was your thought pattern behind that comment you just made?’ and try and make them think of why they said it. Normally they would just be like ‘Oh, just a throwaway comment. Didn’t really mean it’. Like ‘Well, be careful what comes out of your mouth’. Yeah, I get told off for doing that a lot.
It was apparent that no offense had been intended in such cases, but only upon reflection, and/or being informed by others, was it clear how interactions of this sort could be perceived negatively. This pattern had also been noticed by others, for example teachers and social workers, who had informed the young adult that their behaviour might be considered “abrasive” by others. When such misunderstandings did occur, it was seen that the same set of underlying issues meant that the young adults struggled to resolve them, leading to frustration, which tended to exacerbate the issue: Erm, I try and get my point across but then I am regularly misunderstood. So, what I try and say comes out wrong or the right way but just in the wrong context. And that can have some negative impact. It’s horrible. Especially when you’re the one trying to be in control, it can really f**k up a situation. And it does that a lot, which is why when a situation occurs, I have to compensate for the fact that I know I’m going to screw up. You know, like if I’m trying not to shout at somebody and get quite a valid point across and, you know, state things clearly that are factual and true, and then I stammer or f**k up on something I’m saying. I end up flagging and then I look like an idiot when all I’m trying to do is to, you know, the situation has risen to a point so far that I’ve had to end up shouting.
The quote above suggests an effortful attempt to overcome these sorts of challenges and for intentions to be more clearly understood. When unsuccessful, such interactions were described as having negative consequences both for the young adults themselves and for the relationship with the other person. Whilst the young adults mostly focused on more immediate impacts, the parents frequently felt that this ongoing difficulty had resulted in the strain and occasional loss of relationships altogether. Parents also noted how the resulting disagreements seemed to be felt very strongly. Reflecting on the apparent mismatch between how the young adult wanted to come across and how they were perceived, parents explained that their child would often see such disagreements as a betrayal and they resulted in a lot of hurt: They can be a really good friend. But then their weakness is the minute the friend does something that they think is against them … they won’t be their friend again. So, they have a huge string of ex-friends.
Similar difficulties within family relationships were also reported. For example, arguments with parents were described by both young adults and the parents themselves. However, one parent noted that the relationship improved once the adoptees moved out of the family home: They were horrible to their other parent for quite a long time; they were awful to them. Really nasty with them. So, it was a good thing that they moved out, and we get on loads better now when they, you know, because when they come back it’s lovely now.
Another example, seemingly arising from difficulties understanding others’ thoughts and feelings, comes from a parent describing how their child did not seem to understand when they (parent) needed time and space to emotionally recover from disputes with them which were upsetting: Even now when they upset me and they want five minutes later to come back and have a hug and they think it’s all over and I’ve forgotten it all, and they do not appreciate how they have hurt me and I might need a little bit of time to come round. They don’t see that at all. And everything is on their terms.
Taken together, the experiences described seem to suggest specific challenges with moderating how one comes across as intended and understanding others’ internal states. Importantly, the young adults recognised such encounters as challenging and offered descriptions which are reflective of insight into the difficulties and attempts to overcome them. However, despite their efforts, difficulties appear to persist and to be a source of great distress for those affected with relationships being lost.
Difficulties with rejection and loss
More than half of the young adults described intense and long-lasting emotional difficulties after friendships had broken down. Given how effortful social relationships were described to be and how strongly felt the loss of them was, the young adults commonly described quite restrictive social networks: I’ve got a little bunch of friends, not too many friends, but enough to call a little group, and that’s when I’m happy. I don’t like big groups of friends, because you have to be committed, and I’m not good at committing to a bunch of people.
A parent described that their child was “very sad” about the loss of one important friendship: “They miss their friend. I know they miss their friend now, they will say occasionally ‘I wish I was still in touch with x’. It seemed rejection was experienced for a long time afterwards.
Intensely upsetting experiences were also reported concerning the loss of romantic relationships. One parent said that their child: “finds it very, very, very difficult to detach” from romantic relationships and their communication with ex-partners could become strained. One young adult described significant difficulty after a relationship did not develop in the way they had hoped, but with time and after discussing the issue with a therapist, they reflected: I do look back on it and I think we were both quite young and at the end of the day they were going to go off and do their thing and I did my thing, which was a lot better in hindsight now, but there’s still that sort of horrible feeling of rejection, which is like, it’s just, and when you feel like that anyway, what the depression does I think as well is like just makes you very, you feel so isolated, you don’t feel like people get it.
Impact on self-esteem
Around a third of the young adults and their parents linked self-esteem and difficult social experiences. In particular, some participants described how others not responding positively to the young adult resulted in feelings of low self-worth. For example, one parent reported an incident in which their child was upset because they had come to believe that new colleagues would dislike them because of their inter-personal challenges. One young adult described a period in which they had begun to feel uncomfortable about themselves and felt the problem was exacerbated by “people judging them by what they looked like” and led to some incidents of anxiety and low mood. The following description was provided by a parent: They have picked up that [others] are a bit sceptical about them. You know, and they are very unsure of themselves really, deep down. They are always looking for reassurance and erm… it’s not a chip on their shoulder, yeah, they’ve got a low self-esteem.
The complex relationship between these young people’s difficult start in life, ongoing social difficulties and low self-esteem were recognised by several parents. For example, one parent noted: Inside they still think they are quite worthless, and I think a lot of that has got to be their start in life. I’m sure…..That is something; I can’t understand that of course. I’m sure that that’s what that is, that they actually feel, that, that they are crap because they are worthless. “Aren’t they?”, “why wouldn’t they be”? I think deep down they could get upset about that. I think deep down that’s the way they feel.
This frequent pattern of struggling to understand relationships, struggling to repair relationships and experiencing breakdown as rejection was described as having a tremendous impact on the young adults. One parent commented that their child is “very belittling of themselves, they straightaway look at something and just say “I can’t do that” which was affecting their day-to-day life. In such cases, parents were concerned about the limiting role that such low self-esteem might play in the future, for example with work and in developing relationships with colleagues, potential friends and prospective romantic partners.
Theme 2: Alternative/adaptive strategies for developing social relationships
Some of the young people and parents described mechanisms the young people used as apparent ‘work-around’ to the difficulties they experienced during more typical social relationships. As such, this theme reflects the young adults’ adaptive or compensatory strategies for obtaining social companionship. There were two main ways in which this was attained. First, a minority of participants described having found social relationships with people who were much older than themselves and consequently, these relationships were seen as less demanding. Second, more than half of the young adults had found social relationships through their workplace, in which social roles were more clearly defined from the outset (e.g., being a carer).
Finding social acceptance in older peers
Whilst many adoptees were highly motivated to develop relationships with peers around their own age, 13%–20% (self-report and parent-report, respectively) described developing strong bonds with people who were much older than themselves. For example, one young adult commented that: “My social group is people in their forties, weirdly enough, … and they seem to understand me so it works.” Another young adult emphasised; “I prefer people who are like a bit older than me; thirties and upwards.”
Relationships with older individuals were described as positive, albeit somewhat different to the those with people their own age in terms of shared activities; for example, tending to socialise within the home, rather than going to places/doing things together. Relationships with older partners were also described as of reduced intensity with fewer demands placed on the young adult, the older person was described as being more forgiving and understanding of the young adult’s challenges and the relationship appeared altogether easier to manage over a sustained period of time. Parents described a similar pattern. For example, one parent reflected that their child: “has always done their voluntary work. They love being with older people.” Another parent noted that their child had enjoyed the company of older people: I’ll meet people and they will say ‘Oh, aren’t (they) lovely, your child?’ Because they will talk, and when they worked in the old people’s home, oh they [adoptee] thought they [people being supported] were lovely. They would listen to their stories and, you know, all these stories of the war and things like that, and they thought they [adoptee] was great there.
Whilst acknowledging the positives that this brought, some parents did raise concerns about a lack of peers of a similar age: They should be out with friends of their own age. And they don’t seem to mind older peoples’ company, and I keep pushing them towards people, and I think they should be with their peers.
Gaining social interactions through work
Despite acknowledging social difficulties, the young adults were overwhelmingly characterised as highly considerate, helpful and social individuals. One adoptee reflected, “I suppose, I’m quite a motherly figure I think with a lot of my friends”. Another adoptee shared: And me and Rachel, because we both have different variations of disability, we both picked each other up when one of us was down…frequently, we both support each other. Like I do with my friend, with Claire. I speak to Claire in my spare time as well because she gets sad because she’s a bit lonely.
Described as a consequence of this caring demeanour, more than half of the participants described gaining social companionship through some form of caring work; for example providing care/support for children, animals or older people. One parent reflected on this strength: “having a chat with people and making them feel better, that’s what they [their child] are good at.” The parent went on, “she’s always done her voluntary work.”
It was felt that the adoptees who had undertaken professional work in the care sector were adept within those roles. Importantly, some parents reflected that their children’s support roles had helped them develop confidence, self-esteem and connections with others. One parent reflected on their child’s care work: She did, she enjoyed that and I think that was her best progress, because she felt as if she could hold her own. When she was at school, I mean, she’s far from stupid, she knew the clever girls, clever boys and she knew that she couldn’t mix…with them.
Some adoptees had a long-standing ambition to work in care roles and found high levels of satisfaction within them; “I really enjoy, and that’s always what I’ve wanted to do; was do care.” Some had discovered a passion for care work initially via volunteering. One young adult emphasised that they had found their voluntary work in a care role more fulfilling than their paid occupation at the time and consequently sought a career in the care sector: You know, it’s [present, paid occupation] hard to get worked up about. So that’s, that’s why I really wanted to do something…where I felt like I was doing something positive, and that’s why I started volunteering at the helpline. And that’s been really great, to actually be doing something…as opposed to just, you know, and I really enjoy doing that.
In the context that many young adults had experienced some difficulties with personal relationships or finding employment, it was felt that many had found an adaptive niche in care/support roles through which they could retain an occupation and connection with others. This was seen by parents and young adults as overwhelmingly positive, in terms of providing a role in which the young adult could excel professionally whilst gaining social interactions in a structured way. In contrast to the relationships with older individuals, these in-work interactions were not seen as friendships and there appeared to be no expectations of the relationships being reciprocal. Taken together, these adaptive strategies appeared to offer adequate opportunities for sourcing rewarding, positive social experiences with others.
Discussion
The current study sought to better understand the social relationships of young adult adoptees with a history of early adversity and associated neurodevelopmental problems. To achieve this, we used semi-structured, non-clinical interviews, which focussed upon a broad range of the adoptees’ social experiences during the transition to adulthood. This allowed both the young adults themselves and their parents to characterise in more depth the sorts of social difficulties and strengths experienced in this group and to expand on our previous quantitative findings (e.g., Kennedy et al., 2016). It is clear from the themes identified that social relationships were a very high priority in the lives of the adoptees in this sample, but there were several areas of difficulty with managing them. Below, we will reflect on our main findings.
First, consistent with the broader literature on adoption and our own previous work, the findings highlight some heterogeneity of response, with difficulties being described by around a third to a half of the group (e.g., Borders et al., 2000). Again, similar to other work, participants described these problems as persisting from childhood into adulthood (Feeney et al., 2017). These findings also support our previous quantitative results, suggesting that a lack of understanding of others’ mental states is a core driver of difficulty (Kreppner et al., 2010) and the current findings are the first to suggest that these difficulties are persistent from childhood into adulthood. Our findings also align with those in the literature more generally that social difficulties present as a key target for interventions, given their direct impact on wellbeing (Rizeq et al., 2022).
Second, our findings highlight both similarities and differences between our participants and the broader literature on social relationships in those with neurodevelopmental difficulties. Whilst ADHD symptomatology was the most common area of difficulty identified in the sample, the social relationship difficulties described here appear to align more closely with those reported in the ASD literature. In particular, the most common difficulty was around navigating social norms. Another parallel with the literature on adult autistic samples, was that alternative sources of social companionship had been developed (Crompton et al., 2020). It may be the case that care roles and friendships with older individuals provide reliable and understandable relationships with others and it could be that the creation of more opportunities to engage in roles with a strong social component but with defined, clear structure and expectations about the social engagement, would be of some help to some of the adoptees in the cohort. In direct contrast to the ADHD literature (e.g., Paulson et al., 2005), our participants did not describe experiences of being avoided socially. Whilst there was some frustration around difficulties with reciprocal communication, there were no reports of conflict, or conduct problems more generally. Furthermore, there were no reports of an overestimation of social abilities, nor any suggestion of a limited insight into those difficulties.
Third, in addition to issues associated with neurodevelopmental problems, other issues were identified that more closely aligned with the literature on social experiences among adoptees, in particular a lingering impact of rejection and loss (Field & Pond, 2018). However, this was not described in terms of attachment, unresolved loss or necessarily related to adoption itself, but rather in terms of how effortful relationships could be, resulting in a more profound sense of loss at being unable to maintain them.
Strengths, limitations and future directions
The present study had a number of strengths. One key strength is that, as part of a broader prospective longitudinal study, we were able to clearly identify those with neurodevelopmental problems at age 15 without the use of any retrospective measures. Similarly, in contrast to much of the literature on this topic, exposure to early adversity was also established and validated prospectively. Another strength is the inclusion of both the young adults and their adoptive parents, the later providing a second, valuable additional perspective, in light of the documented difficulties with insight into social relationship issues among those with ADHD (Hoza et al., 2005). As a result, our study was able to reveal both areas of overlap and also areas raised predominately by either the parents or the young adults, for example, parent’s broader concerns about longer term outcomes, which was not raised by young adults.
Nevertheless, there are also a number of important limitations. Given that the participants in this study left compulsory education around a decade ago, it is not clear to what extent the difficulties we identify here may be mitigated by more modern approaches to inclusion, support, and understanding of neurodiversity in schooling in the UK today. Finally, we did not include questions around the issue of gender identity, which may also be a limitation.
There are two important avenues for future research that arise from our findings. The first is to further understand the relationships we identify here, using a quantitative approach. For example, whether theory of mind deficits mediate some of the poorer mental health outcomes previously identified (Sonuga-Barke et al., 2017). Another example would be investigating the longer-term impact of the seemingly adaptive alternative social relationships outlined here and whether they are protective in terms of mental health or whether they may have negative outcomes due to lacking important features of more typical friendships. The second centres around interventions; whilst there has been some research looking at the relative efficacy of mental health interventions in people with a history of early adversity (Kuzminskaite et al., 2023), there is not a literature on interventions aimed at reducing/mitigating the impact of neurodevelopmental symptoms.
Implications
A key implication of our findings is that the social relationship difficulties associated with neurodevelopmental problems and early adversity identified in childhood appear to persist into adulthood and are experienced as problematic by a significant proportion of the current sample. Another important implication is that these difficulties have apparent similarities with those experienced in idiopathic autism and to a lesser extent ADHD, which is especially important given service providers’ propensity to overlook or otherwise misunderstand the impact of early adversity on brain development (Edwards et al., 2023; Kildahl et al., 2020). Consequently, it is important that support acknowledges both conventional adoption-related issues and neurodevelopmental issues. Similarly, adoptive parents may benefit from this broader understanding and what sorts of social support may be beneficial.
Our findings also have implications for guiding interventions. For example, the young adults noted that they have tendencies to say or act in ways which might not follow social norms and consequently struggled to navigate social contexts, which appeared to be a factor in relationship breakdowns. The identification of whether some relationship issues relate to emotion regulation, self-understanding, social understanding or social competence is a topic for future investigation and intervention, given their importance highlighted both by our participants here and as a predictor of poorer outcomes identified in the literature. Based on the experiences described here, another possible avenue of support is to explore volunteer/professional roles with an element of social interaction. It is less clear whether these function as a means of scaffolding the necessary skills to develop and maintain social connections elsewhere or instead act as a more permanent replacement. Nevertheless, the evidence presented here would appear to support the argument these alternative sources of social connectivity may offset some of the negative impact on self-esteem and wellbeing.
Conclusions
In addition to conventional issues sometimes found in adopted individuals, such as struggles with rejection and loss, the participants in this sample often described difficulties more closely aligned with those experienced by autistic individuals, despite greater levels of ADHD. However, several compensatory mechanisms were found, which represent a second important contribution of this study. These findings emphasise not only a need for support in this group but also highlight several potential targets for interventions.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all the families and young people who have participated in this study over the many years it has been running. Without them this work would not be possible. We would also like to thank Michael Rutter (King’s College, London) for initiating the study, as initial PI and for his support throughout the project, Robert Kumsta (Ruhr University Bochum) and Wolff Schlotz (Max Planck Institute for Empirical Aesthetics) for their roles as co-PIs, Claire Ballard and Rosanna Vassiliou (King’s College, London) for their support during the most recent phase.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof. Sonuga-Barke reports funding from Shire, Medice, grants from QBTech, personal fees from Neurotech Solutions. All other authors report no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the ESRC (ES/I037970/1) and the Waterloo Foundation (686-4339).
Ethical statement
Open research statement
This research was not pre-registered. Due to the sensitive and confidential nature of the interview data involved in this investigation, it has been decided not to make original data publicly accessible.