
Abstract
Bonding social capital was previously found as more strongly associated with wellbeing in later life than bridging social capital. The present study explored a theoretical explanation found in the socioemotional selectivity theory, by examining whether this association is mediated by the experience of positive affect. According to this theory older adults prefer intimate social relationships that contribute to the experience of positive emotions. A sample of older adults (50–93 years) filled out two online questionnaires, with an interval of 4 weeks, measuring bonding and bridging social capital and positive affect on T1 (N = 319, Mage(SD) = 61.28(7.65)) and social, emotional and psychological wellbeing on T2 (N = 202, Mage(SD) = 61.31(7.47)), as well as relevant covariates. Associations were found between bonding social capital and all sub-dimensions of wellbeing. Mediation analysis showed that these associations were (partly) mediated by the experience of positive affect. Bridging social capital was only associated with social wellbeing and no association with the experience of positive affect was found. These findings support the socioemotional selectivity theory and further illustrate the importance of bonding social capital in positive aging as a resource of opportunities to experience positive emotions, contributing to wellbeing in later life. Theoretical and practical implications are discussed.
Keywords
During the last decade the world’s share of older adults has grown steadily. In 2019 20.3% of the population of the 27 countries of the European Union was above 65 years of age and this share will only increase in the coming decades (Eurostat, 2020). A similar trend can be seen worldwide (United Nations, 2019). Mental wellbeing of this age group has become an often addressed topic in psychological research literature, as either threatened by ageing processes and loss experiences (Djernes, 2006; Heun & Hein, 2005), or as a protective factor for the development of psychological and physical problems (Chida & Steptoe, 2008; Hill, 2011; Steptoe et al., 2015).
Mental wellbeing can manifest itself in different forms, often labelled as either hedonistic, referring to experiencing happiness and positive affect or eudaimonic, meaning having a fulfilling and satisfying life (Deci & Ryan, 2008). Both approaches can be recognised in the conceptualisation of wellbeing as consisting of three sub-dimensions, elaborately described in research (Keyes et al., 2008; Lamers et al., 2011; Robitschek & Keyes, 2009). Emotional wellbeing – corresponding with the hedonistic approach - concerns the satisfaction with one’s own life and the presence of positive emotions (Diener et al., 1999; Keyes, 2009). Psychological wellbeing – corresponding with the eudaimonic approach - refers to self-realisation and effective functioning (Ryff & Singer, 1998). The third dimension, social wellbeing, describes someone’s functioning in the community and society in general (Keyes, 1998), also corresponding with eudaimonic rather than hedonistic wellbeing.
In the research literature social capital has been recognised as an important ingredient of mental wellbeing in older populations (e.g. Biddle, 2012; Boen et al., 2020; Chipps & Jarvis, 2016; Christian et al., 2020; Keating et al., 2005; Nyqvist et al., 2014; Park et al., 2019). Social capital, in health and behavioural research usually referred to as networks, norms, and social trust that may facilitate coordination and cooperation for mutual benefit (Putnam, 1995; Forsman et al., 2013; Haslam et al., 2018; Nyqvist et al., 2013), provides for socioemotional and socio-economic resources. These resources are either provided by someone’s bonding or bridging social capital, two sub-dimensions that are distinguished in the literature (Chen et al., 2009; Coffé & Geys, 2007; Engbers et al., 2017; Putnam, 2000). Bridging social capital refers to wider networks of more business-like connections which are relatively weak (Bourdieu & Wacquant, 1992; Putnam, 2000; Woolcock, 1998), providing for socioeconomic resources (Zhang et al., 2011), while bonding social capital concerns the more intimate and close network of family and friends as a resource of social and emotional support (Adler & Kwon, 2002; Putnam, 2000). Several studies stress the importance of bonding social capital rather than bridging social capital with regard to mental wellbeing in later life (e.g. Litwin, 2011; Haslam et al., 2018; Norstrand & Xu, 2012; Nyqvist et al., 2006). Simons et al. (2020) recently found positive associations between bonding social capital and all three aforementioned sub-dimensions of wellbeing, whilst bridging social capital was only found positively associated with social wellbeing.
Research suggests that social networks can be expected to decrease in older age (Cornwell et al., 2008; Wrzus et al., 2013), but also often include a larger proportion of socio-emotionally important others than social networks of younger adults (Lang, 2001; 2004). These findings can be partially explained by loss experiences affecting one’s overall social capital, such as less involvement in work or other (social) activities, physical decline, and the passing of loved ones (Forsman et al., 2013; Wrzus et al., 2013). However, the shift towards more focus on close friends and family (bonding social capital) and less focus on more distant and varied relationships (bridging social capital), can be regarded as a conscious choice according to the socioemotional selectivity theory (Carstensen, 1992; Carstensen et al., 1999, 2003).
This lifespan theory of social motivation argues that the perception of time plays a crucial role in prioritizing social goals and subsequently social interactions. These social goals can be broadly categorized as either acquiring new knowledge and skills or the regulation of emotions (Carstensen, 1995, 2006; Carstensen et al., 1999). When time is perceived as limited (e.g. because of illness or old age) or the future as largely irrelevant (e.g. growing up in disadvantaged circumstances), people tend to become more present-oriented, a state in which emotion regulation goals predominate. In order to maximize the emotional reward gained from social interaction, social partners will then be selected that provide for positive emotions and familiar feelings in the present (Carstensen et al., 1999).
In line with this theory, Luong et al. (2011) illustrate in their review that with age, people indeed actively select social partners that are emotionally rewarding and end relationships that are less so, serving their goal of emotion regulation and optimizing their wellbeing. As a result the social network will become less varied and more close-knit, consisting largely of close friends and family (Carstensen et al., 1999; Luong et al., 2011). In addition, research indicates that older adults report experiencing more positive affect and satisfaction in their social interactions than younger adults (Birditt & Fingerman, 2003; Charles & Piazza, 2007). Thus, older adults may not only become more selective in their choice of social interaction, but also benefit more from this interaction with regard to their wellbeing.
In summary, following the socioemotional selectivity theory, it can be assumed that bonding social capital will be more important in later life than bridging social capital, because of the socio-emotional resources it contains. These resources are useful for goals of emotion regulation and - especially in later life - provide for the experience of positive affect while socially interacting within the close-knit circle of friends and family.
Present Study
The present study aims to further investigate this theoretical explanation for the importance of the bonding component of social capital in later life. A better understanding of the value of bonding social capital as a resource of positive social interaction in later life will add to present knowledge about positive aging processes and may guide in helping older adults to maintain or improve their wellbeing. The central research question that will be examined is whether the association between bonding social capital and wellbeing in old age is mediated by the experience of positive affect. The present study examines the following hypotheses: (H1) Bonding social capital is more strongly associated with psychological, emotional and social wellbeing in later life than is bridging social capital; and (H2) The associations between bonding social capital and respectively psychological, emotional and social wellbeing are mediated by the experience of positive affect.
Method
Procedure and Sample
This study was approved by the local research ethics committee and followed the American Psychological Association Ethical principles of psychologists and code of conduct (American Psychological Association, 2010). Data was collected in the Netherlands by undergraduate students of the Open University of the Netherlands within the context of a study assignment, using a mix of convenience and snowball sampling within both their personal and professional networks (students of this university are adults with heterogeneity in variables such as previous education, age, marital status, employment status, income etcetera). An online questionnaire (Limesurvey) was used, which could only be filled out after completing the included consent page. This consent page explained that participation was on a voluntary basis and could be stopped at any time without reason and without (adverse) consequences. Furthermore it stated that submitted questionnaires were used anonymously, in compliance with privacy rights and only for the purpose of this study. After completing the questionnaire, respondents were invited after 4 weeks to complete a second shorter online questionnaire. Inclusion criteria were age ≥50 years, and sufficient command of the Dutch language to understand the questionnaire and informed consent.
The first questionnaire (T1) was filled out by 319 Dutch adults of 50 years and older (Mage(SD) = 61.28(7.65), Rangeage = 50–93, Medianage = 60). The majority of the sample was born in either the Netherlands (58.6%) or Belgium (39.2%). The remaining respondents were born in France (n = 2), Turkey (n = 1), Indonesia (n = 1), Netherlands Antilles (n = 1), or Suriname (n = 2). With regard to socioeconomic status, 94.0% of respondents indicated to (probably) have enough financial resources to provide for oneself and (future) needed care, versus 6% that indicated to (probably) have insufficient funds (income level was not assessed as the majority of the sample was expected to be retired). Finally the vast majority of respondents (99.1%) lived independently in their own home, of which 5 respondents received care at home; 2 respondents lived-in with a family member.
About 63% of this group also filled out the second questionnaire after 4 weeks (T2) (n = 202; Mage(SD) = 61.31(7.47), Rangeage = 50–93, Medianage = 60), Relevant demographic covariates will be further described in the results section. Although the sample at T2 is smaller than the sample at T1, the number of participants can still be considered to be sufficient for the intended analyses, as a priori power analysis (f 2 = .15, α = .05) (Faul et al., 2009) indicated a minimum sample size of n = 119.
Measures
Bonding and Bridging Social Capital
Bonding and bridging social capital were measured at T1, using the Personal Social Capital Scale for the Elderly (PSCSE, Simons et al., 2020) - a validated Dutch adaptation of the Personal Social Capital Scale (Chen et al., 2009), containing two subscales. The subscale bridging social capital (BrSC), consisting of 16 items, addresses both government/corporate/social organizations and cultural/recreational/leisure organisations present in someone’s social environment. The items are distributed over five categories and were scored on a 5-point scale (1 = none; 2 = few; 3 = some; 4 = reasonably many; 5 = many). Four categories include each a statement – respectively (1) “As far as I know, ....... organizations can be found in my area”; (2) “....... of these organisations represent my rights and interests”; (3) “I participate in or am a member of ....... of these organisations)”; and (4) “If I need help, I can call upon ....... of these organisations” - that was scored for both government/corporate/social and cultural/recreational/leisure organisations. A fifth category consists of 4 statements addressing connections and influence these organisations may have (e.g. “....... of these organisations have (political) power or influence on (local) decision making” and “....... of these organisations have broad social connections”), again scored for both organisation types. Mean scores of each category were added to compute BrSC.
The subscale bonding social capital (BoSC) addresses different social groups with 21 items. These items are distributed over 5 categories and scored on the same 5-point scale as the BrSC items. Four categories each include a statement – respectively (1) “I have ....... close friends”; (2) “I keep a routine contact with ....... close friends”; (3) “I have ....... close friends that I can trust”; and (4) “I can ask ....... close friends for help” – that was repeatedly scored for four different social groups (family members/relatives; close friends; acquaintances; others). A fifth category consists of five items, addressing someone’s access to certain resources via personal social networks (e.g. “I know ....... people with certain political or other influential power” or “I know ....... people with broad social connections”). Mean scores of each category were added to compute BoSC.
Positive Affect
Positive Affect (PA) was measured at T1 by 10 PA items of the Positive affect Negative Affect Schedule (PANAS, Watson et al., 1988; Crawford & Henry, 2004), representing different types of positive affect (e.g. “excited”, “inspired”, and “enthusiastic”). Respondents were asked to indicate to what extent they experienced these in general on a 5-point scale (1 = very slightly or not at all; 2 = a little; 3 = moderately; 4 = quite a bit; 5 = very much). Mean scores were computed as the PA score.
Wellbeing
The sub-dimensions of wellbeing were measured at T2 with 14 items of the Dutch Mental Health Continuum - Short Form (MHC-SF, Lamers et al., 2011), distributed over the three subscales: emotional wellbeing (3 items; e.g. “In the past month, how often did you feel happy?”); social wellbeing (5 items; e.g. “In the past month, how often did you feel that you belonged to a community); and psychological wellbeing (6 items; e.g. “In the past month, how often did you feel that you are good at managing the responsibilities of your daily life?”). Participants responded on a 6-point scale, (1 = never; 2 = once or twice; 3 = about once a week; 4 = 2 or 3 times a week; 5 = almost every day; and 6 = every day). Mean scores for each subscale were computed.
Demographic Variables
Demographic variables that were included as covariates were, in addition to age and gender, educational level (0 = low: up till secondary school or vocational education, 1 = high: at least an undergraduate degree), the perception of one’s own physical health (5 point scale from 1 = poor to 5 = excellent), and whether someone has a life partner (1) or not (0). The latter two were found to be related to mental wellbeing (Cho et al., 2011; Hooghe & Vanhoutte, 2011) and are likely to undergo changes in later life stages.
Analysis
For the statistical analysis, SPSS version 25 (IBM Corp., 2017) was used. Demographic composition of attritors (respondents only included at T1) and non-attritors (respondents included at T1 and T2) was compared (Pearson’s χ2 and T-tests), as well as the scores on core variables. Reliability of the included scales was examined (Cronbach’s alpha) and (Pearson’s) correlations between core variables were computed. Potential differences in correlations between respectively BoSC and BrSC and the wellbeing scales were examined using the method described by Steiger (1980) and Lee and Preacher (2013).
To examine the association between the social capital subscales and the sub-dimensions of wellbeing as well as the assumed difference in strength of this association for either BoSC or BrSC (H1) three regression analyses were performed. Each of these analyses included both BoSC and BrSC as predictors, measured at T1, and respectively, social wellbeing, psychological wellbeing and emotional wellbeing, as dependent variable, measured at T2. Secondly, prior to the examination of the assumed mediating role of PA (T1), the associations between both BoSC and BrSC (T1) and PA (T1) were examined with regression analysis.
The assumed mediating role of positive affect (PA) in the association between BoSC and the sub-dimensions of wellbeing (H2), was then examined by mediation analysis (PROCESS, Preacher & Hayes, 2004; Hayes, 2013), using the bootstrapping method as well as the Sobel-test (Preacher & Leonardelli, 2001).
In both the regression and mediation analyses standardised scores of the core variables were used, and a priori confounders gender, age, having a life partner, level of education and perception of own physical health were included as covariates. In the mediation analyses BrSC was also included as covariate. Listwise deletion was applied in case of missing data.
Results
Demographic and core variables: examining attrition bias.
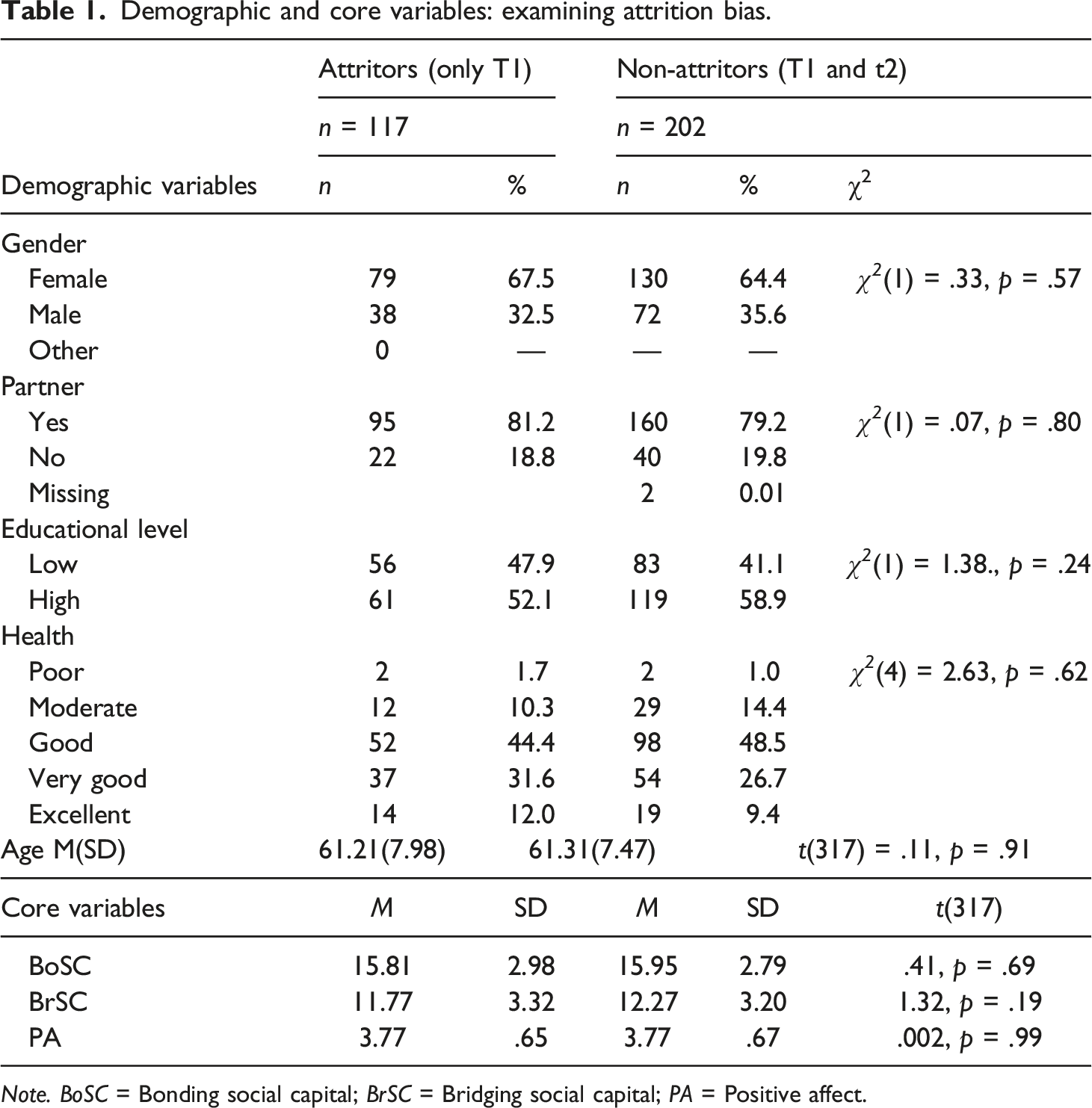
Note. BoSC = Bonding social capital; BrSC = Bridging social capital; PA = Positive affect.
Descriptives, reliability of scales and correlations of the sample (T2) included in the main analyses.
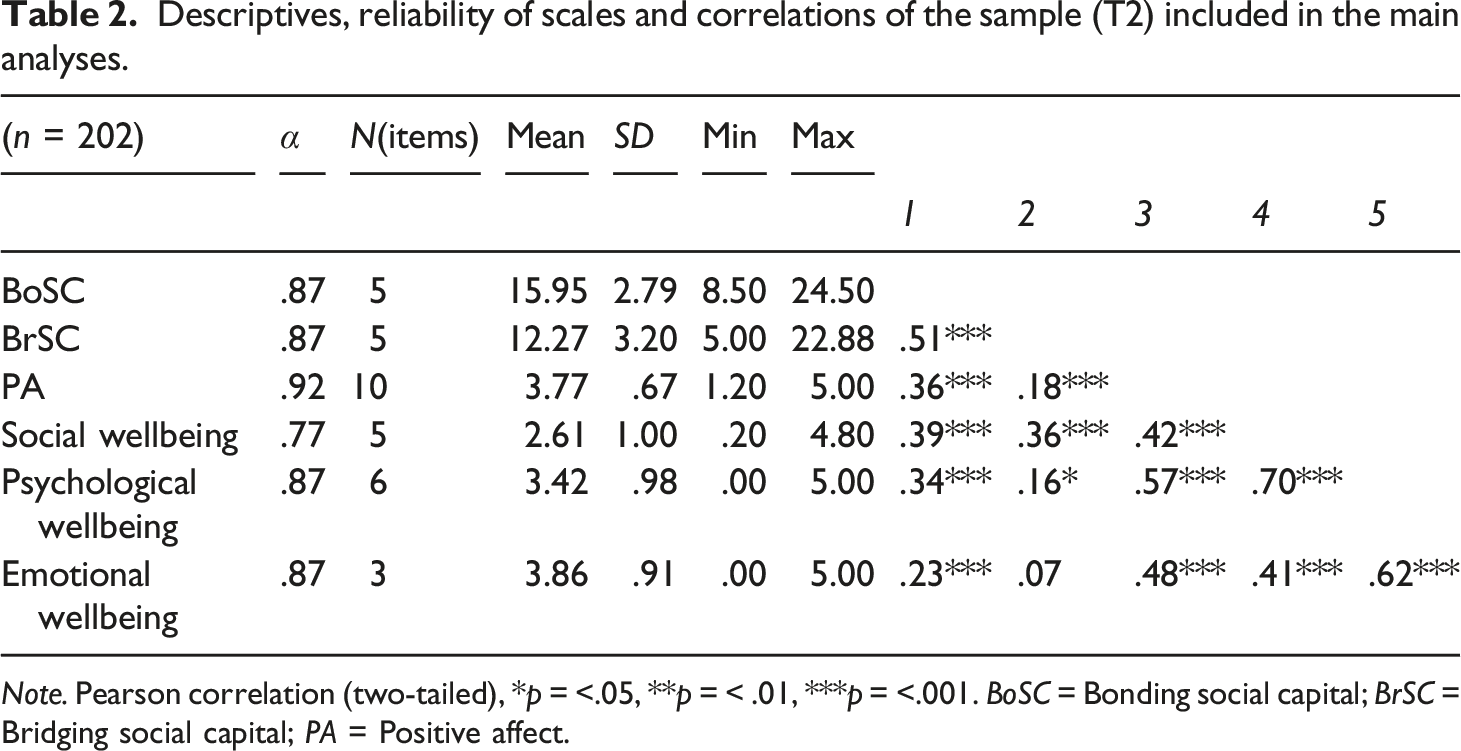
Note. Pearson correlation (two-tailed), *p = <.05, **p = < .01, ***p = <.001. BoSC = Bonding social capital; BrSC = Bridging social capital; PA = Positive affect.
Results of regression analysis of association between Bonding and Bridging social capital and Wellbeing subscales (N = 200).
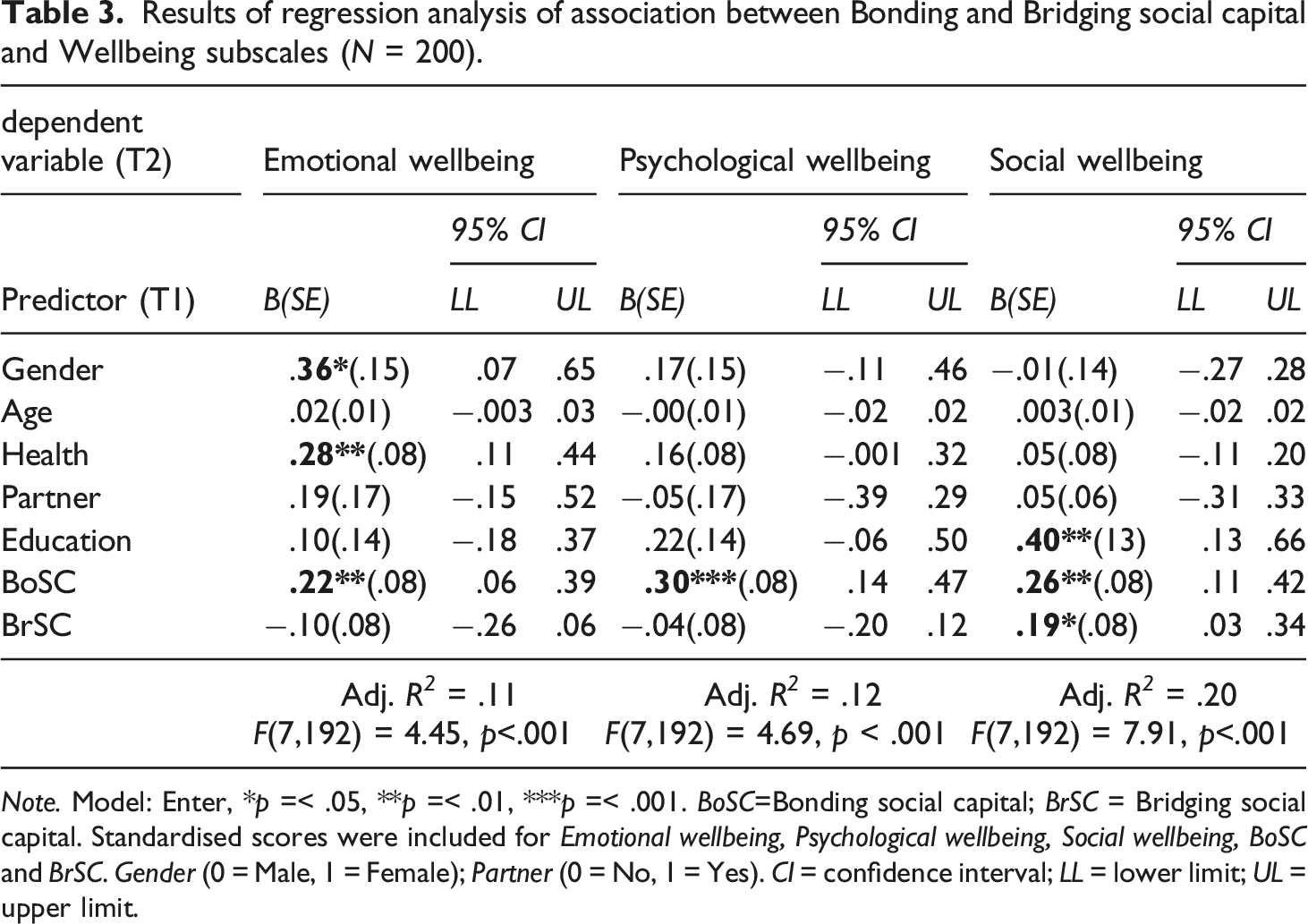
Note. Model: Enter, *p =< .05, **p =< .01, ***p =< .001. BoSC=Bonding social capital; BrSC = Bridging social capital. Standardised scores were included for Emotional wellbeing, Psychological wellbeing, Social wellbeing, BoSC and BrSC. Gender (0 = Male, 1 = Female); Partner (0 = No, 1 = Yes). CI = confidence interval; LL = lower limit; UL = upper limit.
These findings indicate that, in line with hypothesis 1, respondents with a higher score on BoSC experience more emotional, social and psychological wellbeing. Finding a positive association between BrSC and social wellbeing but no association with either of the other two sub-dimensions of wellbeing or overall wellbeing, supports the first hypothesis, assuming that in later life BoSC is more strongly associated with (the sub-dimensions of) wellbeing than is BrSC.
Results of mediation analysis (PROCESS) with Positive affect as mediating variable in the association between Bonding social capital and subscales of Wellbeing (N = 200).
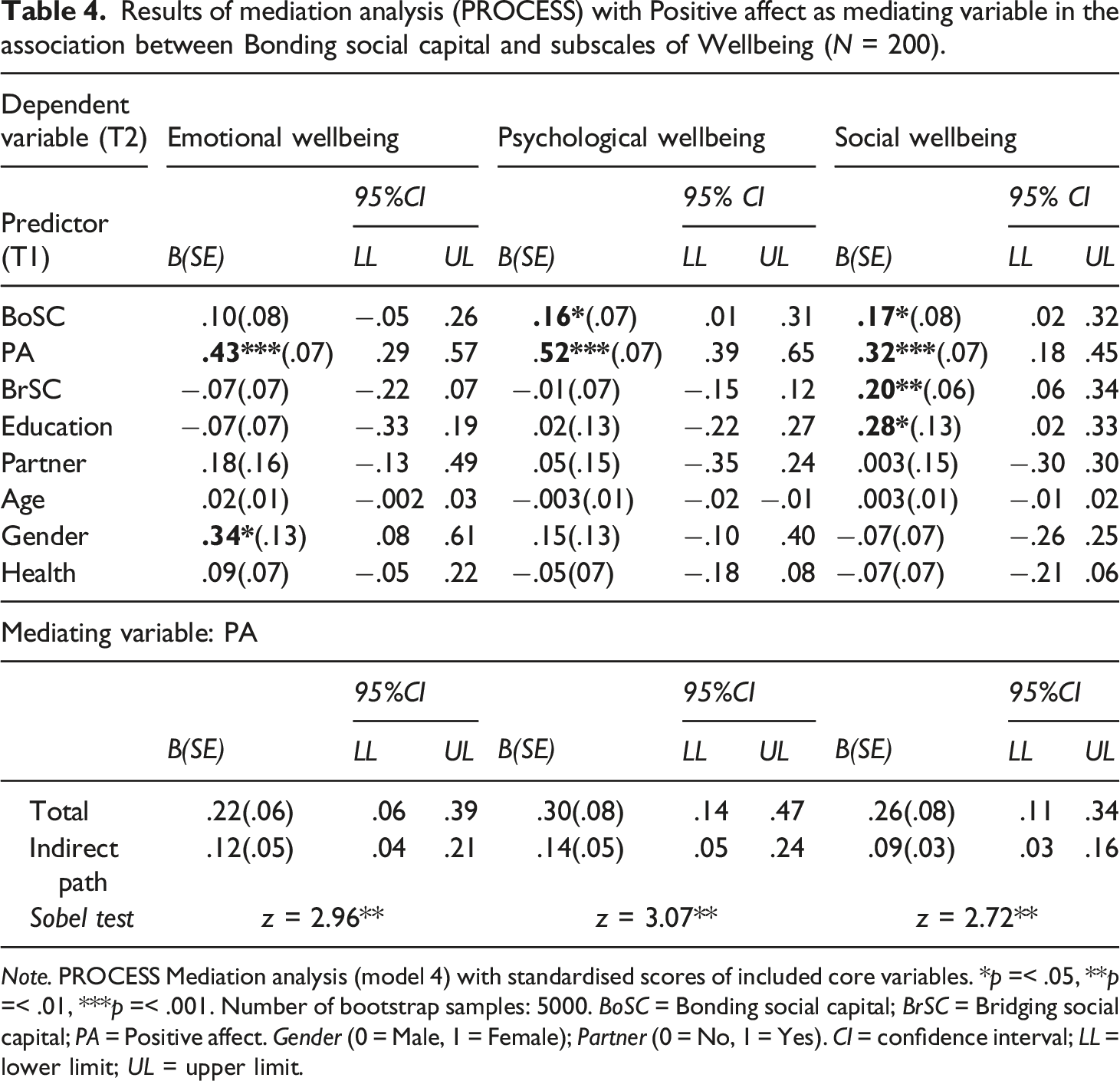
Note. PROCESS Mediation analysis (model 4) with standardised scores of included core variables. *p =< .05, **p =< .01, ***p =< .001. Number of bootstrap samples: 5000. BoSC = Bonding social capital; BrSC = Bridging social capital; PA = Positive affect. Gender (0 = Male, 1 = Female); Partner (0 = No, 1 = Yes). CI = confidence interval; LL = lower limit; UL = upper limit.
Discussion
In the present study, a theoretical explanation was examined for the previously established importance of bonding social capital for wellbeing in later life (e.g. Simons et al., 2020), found in the socioemotional selectivity theory (Carstensen, 1992; 1995; Carstensen et al., 1999). This lifespan theory argues that when the remaining life time is limited, people prefer intimate social relationships – rather found in their bonding social capital than in bridging social capital – that contribute to the experience of positive emotions (Carstensen et al., 2000; 2003; 2006; English & Carstensen, 2014). Additionally, research suggests that older adults may also benefit more from these socioemotional resources, as they reported experiencing more positive affect and satisfaction in their social interactions than younger adults did (Birditt & Fingerman, 2003; Charles & Piazza, 2007).
First associations were re-examined between both bonding and bridging social capital and respectively social, emotional and psychological wellbeing in an older population. Then it was analysed whether the experience of positive affect indeed mediates the association between bonding social capital and these sub-dimensions of wellbeing.
A significant positive association was found between bonding social capital and respectively social, emotional and psychological wellbeing, whilst only social wellbeing was found to be positively associated with bridging social capital. These findings support the first hypothesis - that is people with more bonding social capital report higher levels of social, emotional and psychological wellbeing – and corresponds with earlier notions that bonding social capital in particular is important for wellbeing in later life (Litwin, 2011; Haslam et al., 2018; Norstrand & Xu, 2012; Nyqvist et al., 2006; Simons et al., 2020). These results do not necessarily imply that bonding social capital is less important in other age groups, or that bridging social capital can be disregarded in old age. Research of social capital throughout the lifespan indicates that its association with wellbeing can vary among age groups and demographics. During childhood for instance, bonding social capital is important for emotional wellbeing (Tuominen & Haanpää, 2022). Nieminen et al. (2010) found positive associations between aspects of both bonding and bridging social capital and psychological wellbeing in age groups from 30 years up to 80+ years. Moore et al. (2009) found positive associations between individual social capital and wellbeing in higher educated adults, whilst this association was found to be negative for lower-educated adults. During adolescence and early adulthood, strong bonding social ties or a dense network of close family members and friends, were found to prevent young people from accessing new networks to broaden their view and experiences (Burt, 2001; Coleman, 1988; Ellison et al., 2014). This interaction between bonding and bridging social capital was also studied in an older population, alternatively observing that (close) friends can bridge an older adult with other worldviews and lifestyles, which may be helpful to cope with challenges in old age (Torrejón & Martin-Matthews, 2022). The association found in the present study between bridging social capital and social wellbeing may correspond with this observation. Additionally as the measurement of social wellbeing includes both someone’s functioning in the immediate social environment and in society in general (Keyes, 1998), an association with bridging social capital can also be expected in later life (Simons et al., 2020) as it was also found in other life stages (e.g. Villalonga-Olives & Kawachi, 2015).
The second hypotheses of the present study concerned a mediating role of positive affect. Following the socioemotional selectivity theory (Carstensen, 1992; 1995), more close intimate relationships were assumed to be preferable, providing positive and familiar feelings and experiences that add to wellbeing of the studied older sample. Examining this mediation for each sub-dimension of wellbeing resulted in a partly mediating role of the experience of positive affect in the association between bonding social capital and respectively psychological and social wellbeing. The association between bonding social capital and emotional wellbeing was fully mediated by the experience of positive affect. These findings support the second hypothesis and also indicate that the mediating role of the experience of positive affect is most obvious for emotional wellbeing.
The results are supportive of the socioemotional selectivity theory, from which the predominant goal of emotion regulation during later life stages can be recognised as the underlying explanation for the importance of bonding social capital for wellbeing in later life. As emotional wellbeing was conceptualised as one’s satisfaction with life and the presence of positive emotions (Diener et al., 1999; Keyes, 2009), the finding of a full mediation of the association between bonding social capital and emotional wellbeing by the experience of positive affect is not surprising. This is further elaborated in the next section based on the applied operationalisations of both positive affect and emotional wellbeing.
Critical Notes and Future Research
Interpreting the results, several critical notes should be taken into account concerning the research sample, applied research design and statistical analyses. These notions call for caution in drawing firm conclusions and are helpful in identifying next steps in future research.
Data were collected on two time points, with an interval of 4 weeks. About 37% of the respondents at T1 did not complete the second questionnaire at T2. However, the sample size at T2 was still sufficiently large for the intended analyses and no evidence for attrition bias was found. More female (64.4%) than male respondents (35.6%) took part in this study. Although the older general Dutch population (>60 years) consists of more women than men (Centraal Bureau voor Statistiek, 2020), the sample does not accurately reflect the male-female distribution of the intended population. Since gender was also found to be a significant factor in explaining variance in emotional wellbeing – which is consistent with previous research on gender differences in happiness scores (e.g., Simon, 2008; Solé-Auró et al., 2018) – one needs to be careful assuming the findings hold in the same way for men and women. For example, wellbeing has been shown to be a protective factor for the development of psychological and physical problems (e.g. Hill, 2011; Steptoe et al., 2015), indicating that gender should be taken into account when studying aging processes.
The majority of the sample indicated being in a relationship (79.2%) and to be physically in good shape (84.6%). This may be related to the somewhat skewed distribution of age (the proportion of old-old adults was relatively small) and explain why no significant contribution if these covariates was found in the mediation analyses. Health did play a significant role in the regression analysis with emotional wellbeing as dependent variable though. By including an equally wide but less skewed age range in future study samples, the role of age could be more elaborately studied, using for instance moderated mediation analysis (e.g. Edwards & Konold, 2020) to test whether the indirect effects of bonding social capital is indeed stronger for old-old than young-old adults. Educational level, found to be a significant covariate with regard to social wellbeing, was a bit more equally divided, although not representative for the overall population (Centraal Bureau voor Statistiek, 2018), as a little under 60% indicated having completed a higher level of education (college undergraduate or higher).
The measurements of emotional wellbeing (e.g. “In the past month, how often did you feel happy?”) and the experiences of positive affect (e.g. “excited”, “inspired”, and “enthusiastic”) could be perceived as measuring quite similar concepts, affecting the mediation analysis. In additional analysis the differences between correlations as displayed in Table 2 were therefore tested (Lee & Preacher, 2013; Steiger, 1980). No significant differences were found between the correlation of the experience of positive affect and emotional wellbeing on the one hand and correlations of the experience of positive affect and respectively social wellbeing (z = .09, p = .36) and psychological wellbeing (z = −1.78, p = .07) on the other, reassuring that the findings indeed support the explanation of the importance of bonding social capital in later life as given by the socioemotional selectivity theory (Carstensen, 1992; 1995).
Finally the research design and statistical analyses call for some caution when interpreting the results. Mediation is often interpreted from a causal perspective (Rohrer et al., 2021), while a research design with two measurement moments does not sufficiently meet the preconditions for causal research and drawing firm conclusions about causality (Rohrer, 2018). However, the current empirical findings fit into a well-established theoretical framework that was used as the basis for the mediation hypotheses. This provides sufficient ground to conclude that the findings point towards the type of causality assumed in the mediation model and support the socioemotional selectivity theory’s perspective that the value of social bonding in later life can be found in its resources of positive affect.
Future research would benefit from experience sampling or ecological momentary assessment (Hektner et al., 2007; Stone et al., 1999). Measurement of affect in a retrospective way, as was done in the present study, may suffer from issues such as giving more weight to peak moments (Diener et al., 1997) or ignoring the duration of an emotional episode (Frederickson & Kahneman, 1993). Experience sampling methods that measure actual momentary experiences of positive affect - for instance while in the presence of important others – suffer less from these issues and can provide researchers with more reliable and ecologically valid data (Brans et al., 2013; Myin-Germeys et al., 2009).
Theoretical and practical implications
Applying the socioemotional selectivity theory to better understand the value of social capital in older age has not revealed why bonding social capital becomes more important in later life, but also provides insights that help further investigate the interplay between bonding and bridging social capital throughout the lifespan. Two basic assumptions of the theory, (1) the perceptions of time guide us in selecting our social goals and (2) pursuing these goals directs our behaviour (Carstensen, 1995; 2006; Carstensen et al., 1999), will help better understand choices that are made regarding social partners in the various life stages or certain life circumstances. Also the interaction between bridging and bonding social capital found in different age groups (e.g. Ellison et al., 2014; Torrejón & Martin-Matthews, 2022) as earlier discussed in this section, may be better understood by investigating someone’s circumstances and the resulting social choices.
The research population of the current study is steadily growing. As pointed out in the Introduction, 20.3% of the population of the 27 countries of the European Union was above 65 years of age in 2019 and this share will keep growing in the coming decades (Eurostat, 2020). The understanding of motives for behaviour and resulting preferred selection of social partners, as well as the importance of these social partners for the wellbeing, can be used in many different areas, ranging from individual interventions for older adults, design of care institutions or residential areas to even housing policy. In these, facilitating access to one’s bonding social capital should always be a priority, enabling older adults to participate in social interaction that entails positive and familiar experiences, contributing to their emotional, psychological and social wellbeing.
Practical lessons drawn from the present study include that older adults who struggle to maintain a desired level of wellbeing may be helped more effectively by supporting access to socially-emotionally significant others, rather than organizing daytime activities involving lesser-known others. Abu Elheja et al. (2021) for instance, found recently that emotional loneliness in old age decreased following social interaction only when high levels of closeness in the interaction were experienced. A study by Luck-Sikorski et al. (2017) indicated that talking to friends and family was reported as one of the preferred treatment options by a sample 1230 older adults (75+ years) suffering from late life depression.
If important others become rare or difficult to encounter regularly, it might be useful to provide for opportunities to connect with like-minded people with whom a closer bond can be developed over time (e.g. Edward, 2016; Saarelainen et al., 2022). Additionally, as we have entered a hybrid world of offline and online environments in which some of today’s older adults, but certainly future older generations, will create, maintain and access their social capital, the use of digital media in relation to social capital and wellbeing of older adults, can be regarded another interesting angle of both research and the development of supporting tools (Chen & Li, 2017; Ryan et al., 2017; Simons et al., 2021; 2022).
Conclusion
Bonding social capital has been recognised as an important ingredient of mental wellbeing of the steadily growing population of older adults (e.g. Haslam et al., 2018; Simons et al., 2020). The present study supports the theoretical explanation given by the socio-emotional selectivity theory (e.g., Carstensen, 1992; Carstensen et al., 1999) for this finding, suggesting that the value of bonding social capital can be found in the socio-emotional resources it provides. Older adults prefer and seek social interactions within a close circle of friends and family that help them pursue emotion regulation and experience positive and familiar emotions in the here and now.
However, in later stages of life social capital tends to decline (Cornwell et al., 2008; Kalmijn, 2003; Wrzus et al., 2013) and access to socioemotionally important others can become less evident because of age-related loss experiences (Forsman et al., 2013; Wrzus et al., 2013; Simons et al., 2022). Facilitating access to one’s bonding social capital and providing opportunities to experience closeness within social interactions should therefore be a priority in elderly care, with a focus on positive and familiar experiences adding to emotional, psychological and social wellbeing. This can be sought in both physical interventions and the use of digital media applications (e.g. Simons et al., 2022).
Preliminary results of this study have been presented at the European Conference of Positive Psychology (ECPP), July 2022, Reykjavik.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information:This research was not pre-registered.
The data used in the research are available. The data can be obtained by emailing: