
Abstract
A burgeoning literature considers caregiving in a relationship context and examines how the quality of caregivers’ relationships with care recipients influences their own appraisals of caregiving. Yet, extant research has mostly relied on cross-sectional data and utilized a unidimensional approach to examining relationship quality. This study extended prior research by examining (a) how positive and negative relationship qualities are associated with changes in caregiving appraisals over time, and (b) whether these associations vary by care recipients’ age and disabilities. We examined a longitudinal cohort of caregivers (N = 1,453, Mage = 62.11) from the National Study of Caregiving (wave 1: 2015, wave 2: 2017), in which caregivers rated positive and negative qualities of their relationships with care recipients aged 65+ (N = 1,047, Mage = 82.89), and reported on difficulties, burden, and rewards while serving as caregivers. Path analyses revealed that negative relationship quality at wave 1 was associated with increased difficulties and burden of caregiving over time, whereas positive relationship quality at wave 1 was associated with increased caregiver rewards. The associations between relationship qualities and caregiving difficulties as well as rewards varied depending on care recipients’ age and disabilities. Having negative relationships with care recipients was only associated with increased difficulties for caregivers who had younger care recipients, whereas having positive relationships was only linked to increased rewards for those with older care recipients. We also found that positive relationships were significantly associated with increased rewards in caregivers whose care recipients had fewer disabilities. This study refines our understanding of the role relationship quality plays in caregiving and highlights the lasting effects of relationships with care recipients on caregivers’ appraisals. Findings may help identify caregivers at greater risk for negative outcomes and suggest incorporation of relationship therapies in interventions to facilitate affection and attenuate conflicts in caregiving relationships.
Introduction
About one in every four Americans live with a disability in at least one activity of daily living (e.g., mobility), and the prevalence increases dramatically with age (Chatterji et al., 2015; Okoro et al., 2018). Older adults with disabilities often receive intensive care from their family members and friends, who serve as informal caregivers providing unpaid assistance at considerable emotional, physical, and financial costs (Cooper et al., 2007; Cuijpers, 2005; Zarit et al., 2019). Much of the literature has portrayed caregiving as a stressful task that compromises caregivers’ well-being (Davis et al., 2011; Zarit et al., 2019). Yet, more recently, scholars have paid greater attention to how caregivers appraise both burden and rewards of their duties, which influence the consequences of caregiving-related stressors (e.g., care recipients’ physical and cognitive limitations) for caregiver well-being (Galvin et al., 2020; Pristavec, 2019). Indeed, caregivers’ experience of difficulties and burden may not only reduce their own health, but also exacerbate care recipients’ well-being, such as increasing their hospitalization or mortality rates (Hooley et al., 2005; Lwi et al., 2017). Rewards of caregiving, however, can protect caregivers and alleviate their depressive symptoms (Abdollahpour et al., 2018; Fauth et al., 2012). It is thus crucial to identify factors that can shape caregivers’ appraisals of caregiving in a more positive and less negative manner, which may in turn benefit both members of the caregiving dyad.
Some studies and interventions have been designed to help informal caregivers, but they have either focused on educating caregivers or mobilizing multiple sources of support outside of the caregiving dyad (i.e., other family members, formal/paid services; Crellin et al., 2014; Zarit et al., 2014). A growing body of research emphasizes the ongoing relationship between caregivers and care recipients, where care occurs and evolves (Ablitt et al., 2009; Rippon et al., 2020; Quinn et al., 2009; Wadham et al., 2016). Yet, studies have primarily relied on cross-sectional data and revealed mixed findings of the impact this relationship had on caregiving experiences and outcomes (Hooker et al., 2015; Tough, Siegrist, & Fekete, 2017). Caregiving is not a static process, and caregivers’ appraisals of caregiving may change over time. The current study drew on longitudinal data to examine how the quality of caregivers’ relationships with care recipients contributes to the change in these caregivers’ appraisals over time.
Further, we asked whether the association between caregivers’ relationships with care recipients and their appraisals of caregiving varied depending on care recipients’ age and disabilities. Care recipients’ age and disabilities can elicit caregivers’ perceptions on care recipients’ limited time left (Sullivan-Singh et al., 2015; Wang et al., 2020; Wu et al., 2016), which may impact their attitudes towards care recipients and caregiving demands (Fingerman & Charles, 2010). Although the risk and prevalence of disabilities increase with age (Guay et al., 2014), age and disabilities may independently signal closeness to death and differentially influence how caregivers’ social experiences with care recipients shape their appraisals of caregiving work. Findings will help us identify caregivers at greater risk for negative health outcomes and allocate more appropriate resources towards this vulnerable population.
Positive and negative relationship qualities
The literature has linked relationship quality to caregiving outcomes (Rippon et al., 2020; Quinn et al., 2012; Tough, Siegrist, & Fekete, 2017), but we aimed to extend prior research by considering both positive and negative qualities of caregivers’ relationships with their care recipients. Scholars have increasingly recognized that such a 2-dimensional approach reveals both affection and conflict in a relationship and proves more informative than an overall/unidimensional measure of relationship quality (Mattson et al., 2007). Positive relationships are generally regarded as social resources that allow individuals to better cope with acute and chronic stress in life. Indeed, theorists suggest that social support, the main function of positive relationships, not only benefits individuals directly, but also may protect them from stress (Brady et al., 2013; Creaven et al., 2020; Greenglass et al., 2006). Negative relationships (e.g., marital strain), however, compromise individuals’ well-being and increase their reactivity to stress (August et al., 2007); these consequences are more salient than those of positive experiences (Rook et al., 2015).
Relationship qualities and caregiving appraisals
Previous research has mostly drawn on cross-sectional data to examine the impact of prior (pre-caregiving) or current relationship quality on caregiver outcomes (Ablitt et al., 2009; Lum et al., 2014; Rippon et al., 2020). Here, we focused on what happened after caregivers took on their roles: We assessed the quality of caregivers’ relationships with care recipients at a certain time-point and examined how it influenced changes in caregivers’ appraisals of caregiving in subsequent years. The Stress Process Model highlights that caregivers’ appraisals play major roles in the process where exposure to caregiving-related stressors (e.g., care recipients’ limitations, caregiving demands) influences their own well-being (Goode et al., 1998; Pearlin et al., 1990). Yet, we still know little about how factors specific to each caregiving relationship may shape caregivers’ appraisals.
In the current study, we considered caregivers’ appraisals of difficulties, burden, and rewards in assuming their duties. Some recent studies suggest that positive relationships may increase caregivers’ feelings of difficulties and burden by eliciting their emotional contagion to care recipients’ suffering (Kiecolt-Glaser & Wilson, 2017; Monin et al., 2017). Yet, overall, as posited by the stress-buffering hypothesis, positive relationships may still impart important social resources under stress, which protect caregivers’ well-being in the long run (Cohen et al., 2015; Cohen & Wills, 1985). Further, a burgeoning literature has explicitly shown that individuals with more positive relationships may be better able to identify positive aspects and rewards of caregiving (e.g., gains, gratification, increased family cohesion; Carbonneau et al., 2010; Yu et al., 2018).
Several additional models help us understand the exacerbating effect of negative relationship quality on caregivers’ appraisals. The Stress-Exacerbation Model suggests that individuals who report more negative relationships or experience social isolation are more reactive to stressors (August et al., 2007). More specific to caregiving, the Informal Caregiving Integrative Model posits that negative relationships with care recipients likely shape the way caregivers appraise caregiving-related stressors, which can make them more prone to caregiver burnout and distress (Gérain & Zech, 2019). Indeed, negative relationship quality often co-occurs with a lack of support and appreciation, which over time may deprive caregivers of psychological resources that can help them effectively cope with stressors.
Taken together, we hypothesized that caregivers with more positive and/or less negative relationships with their care recipients would report reduced appraisals of difficulties and burden, as well as increased rewards over time, when their baseline appraisals were considered.
Caring for persons of different ages and disabilities
We further examined whether the lasting impact of relationship qualities on caregivers’ appraisals of caregiving varies by care recipient age and disabilities. Age and disabilities are both common indicators of limited time left in one’s life (Carstensen & Fredrickson, 1998; Sullivan-Singh et al., 2015; Wang et al., 2020), which, according to the Social Input Model, may influence caregivers’ social experiences with care recipients and their caregiving appraisals in a relational context. The Social Input Model posits that individuals regulate their emotions and modify behaviors considering their social partners’ limited time left (Fingerman & Charles, 2010). For example, individuals are more likely to behave positively when interacting with an older adult (Fingerman et al., 2008). It is possible that caregivers who have care recipients with presumably less time left due to advanced age and/or disabilities would identify greater rewards from having more positive relationships with these care recipients and improving their quality of life by providing care. Prior research following the Social Input Model has also found that adults of all ages tend to downplay negative emotions when they are involved in a tension with an older adult (Luong et al., 2011). Individuals are less likely to confront and argue if they were told that some social transgressions or rude comments were made by an older social partner, compared to a younger social partner (Miller et al., 2009). Moreover, middle-aged children have been found to avoid conflicts with their older parents who had more disabilities (Wang et al., 2020).
It is worth noting that although individuals likely develop more severe disabilities as they age (Guay et al., 2014; Okoro et al., 2018), aging and disabilities do not always co-occur. The time left in life may become smaller with age, but research has considered health indicators (e.g., HIV, cancer, disabilities that often result from chronic health conditions) to disentangle age from closeness to death (Carstensen & Fredrickson, 1998; Sullivan-Singh et al., 2015; Wang et al., 2020). As such, we asked whether caregivers of care recipients who are older and who have more disabilities would be more buffered by positive relationships with these care recipients and less bothered by negative moments in their relationships.
In sum, this study tested whether and how the baseline positive and negative relationship qualities were associated with changes in caregivers’ appraisals of difficulties, burden, and rewards over time (Hypothesis 1; see Figure 1). We expected to observe weaker associations between relationship qualities and appraisals for caregivers whose care recipients were older or had more disabilities (Hypothesis 2). We adjusted for additional care recipient and caregiver covariates when testing these hypotheses, including gender, age, education, minority status, work status, type of relationship between care recipient and caregiver (e.g., spousal caregiver, child caregiver), self-rated health, having young children to take care of, and coresidence status between the caregiver and the care recipient. Lastly, prior research has found that caregiving setting (caring for an older adult in the community vs. an older adult in residential care settings) influences caregivers’ relationships with care recipients and the amount of assistance they provide. Thus, we adjusted for caregiving setting and the level of care activities. Conceptual model for caregivers’ appraisals of caregiving between waves. Note. RQ = relationship quality.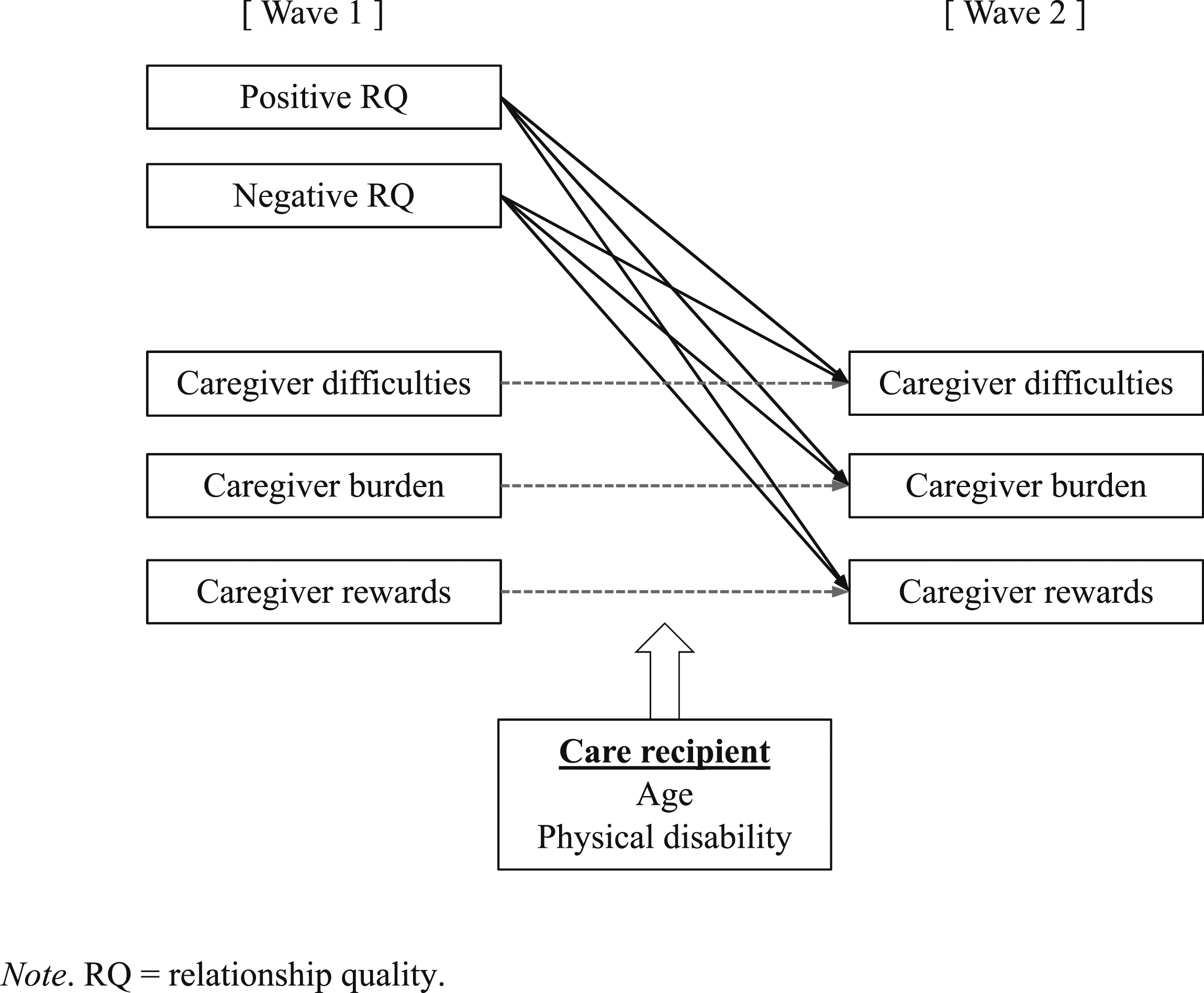
Materials and methods
Data and sample
Data for the current study were derived from the National Health and Aging Trends Study (NHATS) and the supplemental National Study of Caregiving (NSOC). The NHATS began in 2011 with Medicare beneficiaries aged 65 and older (“sample persons”), who have been interviewed on an annual basis. Participants were recruited across the United States, with stratified sampling used to ensure recruitment from each region of the country. Some sample persons reported receiving unpaid help with daily activities (i.e., mobility activities, self-care activities, and household activities) and family members and unpaid caregivers who helped these sample persons (i.e., their informal caregivers) were identified and contacted to participate in the NSOC (Freedman et al., 2019). In 2011 and 2015, caregivers reported on aspects of their caregiving work, demographic information, and well-being (interviewed caregiver N = 2,007 in 2011 and N = 2,204 in 2015). The NSOC followed the 2015 caregiver cohort and interviewed them again in 2017 (the 2015 cohort was the only longitudinal cohort available in the NSOC). This study thus used longitudinal data from both 2015 and 2017 waves. Please see detailed data collection procedures in the NSOC User Guide (Freedman et al., 2019). In total, 2,204 caregivers caring for 1,458 sample persons participated in the NSOC in 2015, and 1,453 of these caregivers returned in 2017. Of the 751 non-returning caregivers, most dropped out of the study because their care recipients: (a) were deceased (n = 164), (b) were too till to participate (n = 81), (c) refused to participate (n = 141), and (d) could not be contacted or located (n = 30). The remaining 335 caregivers dropped out due to personal reasons. The final sample included 1,453 caregivers who participated in both waves of data collection (wave 1: 2015, wave 2: 2017), and cared for 1,047 care recipients (i.e., sample persons). To clarify, care recipients might have had multiple caregivers, but the majority of the sample (69%) had only one caregiver. Because some caregivers devoted similar number of hours to caregiving, we adjusted for the level of care activities as illustrated in the measures below, rather than identifying a primary caregiver for each care recipient. These 1,453 caregivers were older and more likely to be a child of care recipients than the 751 caregivers who did not return. It is also worth noting that 201 care recipients (19%) could not provide self-reports on their disabilities due to illnesses such as dementia; we adjusted for an indicator of the source of reports on care recipients (1 = care recipient self-report,0 = proxy report).
Measures
Relationship qualities
In the NSOC, caregivers rated the extent to which (a) they enjoyed being with care recipients, (b) they felt appreciated by care recipients, (c) care recipients argued with them, and (d) care recipients got on their nerves (Moon et al., 2017). Responses were coded from 1 (not at all) to 4 (a lot). Mean scores were calculated to assess positive (ρ = .57; the first two items) and negative relationship quality (ρ = .71; the last two items; Eisinga et al., 2013), respectively.
Caregivers’ appraisals of caregiving
In this study, we considered three indicators of caregiving appraisals: difficulties, burden, and rewards. In the NSOC, caregivers indicated whether helping care recipients was (a) financially, (b) emotionally, and (c) physically difficult for them, and if so, how difficult it was (Wolff et al., 2016). Responses to these three items were rated from 0 (not at all difficult) to 5 (very difficult), and we calculated a mean score to measure difficulties of caregiving (wave 1 α = .64; wave 2 α = .65).
Caregivers also indicated caregiver burden by rating the extent to which (a) they were exhausted when they went to bed at night, (b) they had more things to do than they could handle, (c) they did not have time for themselves, and (d) as soon as they got a routine going, care recipients’ needs changed (Skolarus et al., 2017). Responses were rated from 1 (not so much) to 3 (very much), and we generated a mean score (wave 1 α = .74; wave 2 α = .76).
For rewards of caregiving, caregivers reported the extent to which helping care recipients (a) has made them more confident about their abilities, (b) has taught them to deal with difficult situations, (c) has brought them closer to care recipients, and (d) gives them satisfaction that care recipients are well cared for (Polenick et al., 2020). Responses were rated from 1 (not so much) to 3 (very much), and were averaged across items (wave 1 α = .72; wave 2 α = .71).
Care recipient age and physical disability
The NHATS collected information about care recipients’ age in years, and whether they received assistance in a variety of mobility activities, self-care activities, and household activities (Freedman et al., 2019). Mobility activities included getting around outside, getting around inside, and getting out of bed; self-care activities included eating, bathing, showering or washing up, getting to or using the toilet, and dressing; household activities included doing laundry, shopping for personal items, preparing hot meals, paying bills or banking, keeping track of medications, sitting in medical appointments, and making medical or insurance decisions. Assistance in each activity was coded as 1 (yes) or 0 (no), and we calculated a sum score of the items to measure disabilities (α = .84; range = 1–15).
Covariates
We adjusted for some caregiver and care recipient characteristics. The NHATS collected information on care recipient gender (1 = male, 0 = female), education in sequential categories (1 = no formal education, 2 = 1 st –8 th grade, 3 = 9 th –12 th grade, 4 = high school graduate, 5 = vocational, technical, business or trade school certificate, 6 = some college but no degree, 7 = Associate’s degree, 8 = Bachelor’s degree, 9 = Master’s, professional, or Doctoral degree), racial/ethnic minority status (1 = Hispanic/Latinx, Black, Asian or other races, 0 = non-Hispanic/Latinx White), and whether they coresided with each of their caregivers (1 = yes, 0 = no). Caregivers reported age, gender (1 = male, 0 = female), two dummy variables each indicating whether the caregiver was a spouse/partner (1 = yes, 0 = no) or a child/stepchild/child-in law (1 = yes, 0 = no), work status (1 = working for pay, 0 = not working for pay/retired), having any young child (under age 18), education in categories, and self-rated health (1 = poor to 5 = excellent; Idler & Kasl, 1995). We also considered whether reports on care recipients’ characteristics were provided by themselves (1 = yes, 0 = no), whether care recipients lived in the community (1) or in residential settings (0), and the level of care activities caregivers engaged in. Caregivers reported on the frequency with which they provided help with chores, shopping, personal care, getting around home, and transportation, on a scale from 1 (rarely) to 4 (every day). Following prior research, we created a sum score (α = .67; Moon et al., 2017).
Analysis
We estimated path analyses with Mplus 8.3, adjusting for the clustering of household (i.e., multiple caregivers could be responsible for one care recipient) and applying a full information maximum likelihood (FIML) procedure to handle missing data. We first tested whether the positive and negative relationship qualities at wave 1 were associated with caregivers’ appraisals of caregiving (difficulties, burden, and rewards) at wave 2 (Hypothesis 1)—controlling for the wave 1 appraisals. We examined this hypothesis in one model, allowing the covariance between residuals of these three outcome variables. Given that we adjusted for appraisal outcomes at wave 1, the models tested subsequent changes rather than exact levels of caregiving appraisals (Castro-Schilo & Grimm, 2018; Rovine & Liu, 2012). Next, to examine whether the association between relationship qualities and caregivers’ appraisals varied by care recipient age and disabilities (Hypothesis 2), we tested interaction terms of care recipient age and disabilities. We adjusted for caregiver covariates (i.e., gender, age, education, self-rated health, racial/ethnic minority status, work status, type of relationship with care recipient, having any young child under the age of 18, coresidence status, the level of care activities) and care recipient covariates (i.e., gender, source of report, caregiving setting). All continuous variables were centered on the sample mean, and simple slopes analysis was conducted to understand significant interactions; thus, we examined the associations between relationship qualities and outcome variables at different levels of the moderator (1SD above and below the sample mean).
Results
Summary of sample characteristics.
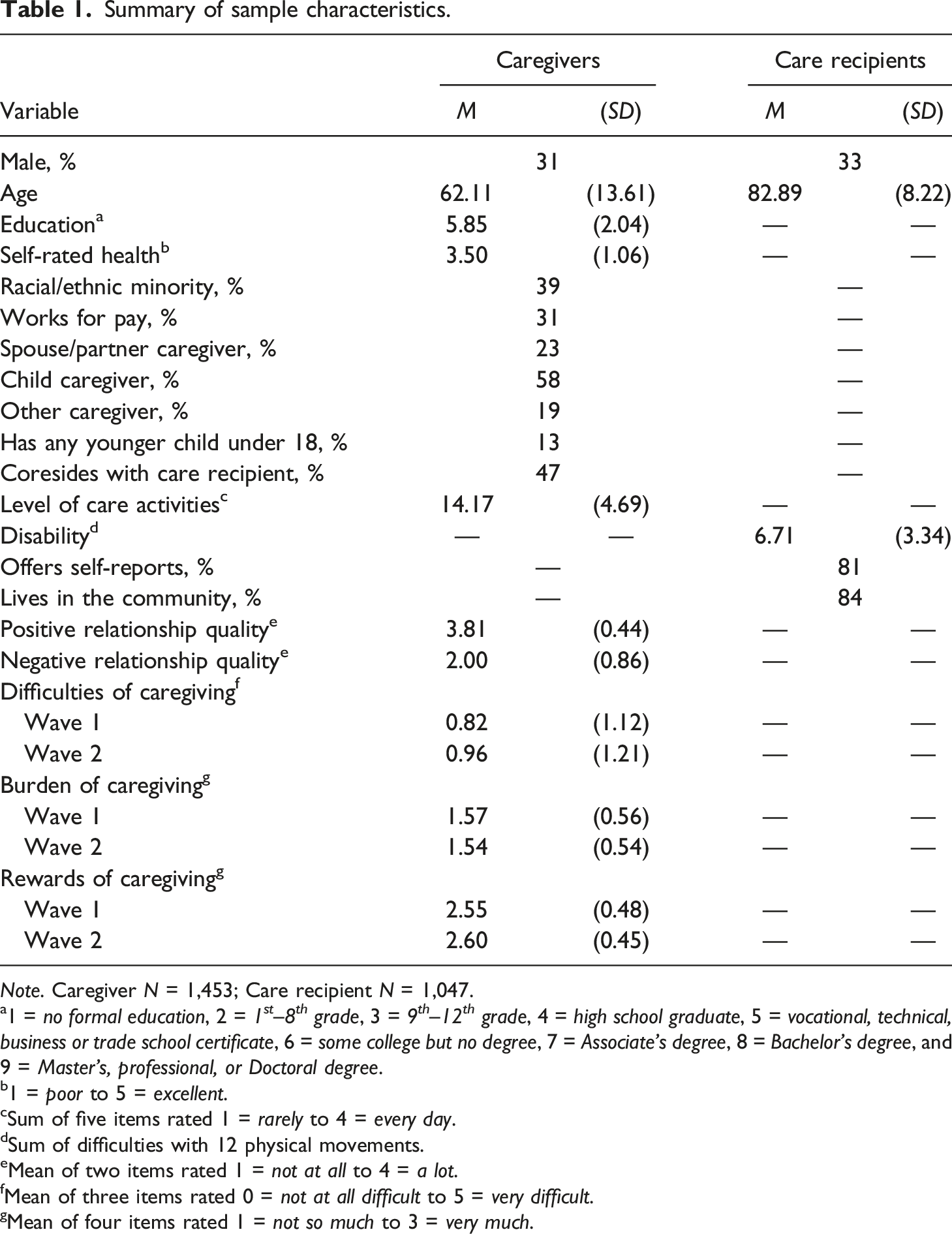
Note. Caregiver N = 1,453; Care recipient N = 1,047.
a1 = no formal education, 2 = 1 st –8 th grade, 3 = 9 th –12 th grade, 4 = high school graduate, 5 = vocational, technical, business or trade school certificate, 6 = some college but no degree, 7 = Associate’s degree, 8 = Bachelor’s degree, and9 = Master’s, professional, or Doctoral degree.
b1 = poor to 5 = excellent.
cSum of five items rated 1 = rarely to 4 = every day.
dSum of difficulties with 12 physical movements.
eMean of two items rated 1 = not at all to 4 = a lot.
fMean of three items rated 0 = not at all difficult to 5 = very difficult.
gMean of four items rated 1 = not so much to 3 = very much.
Path analyses predicting caregiving appraisals at wave 2 from relationship qualities.
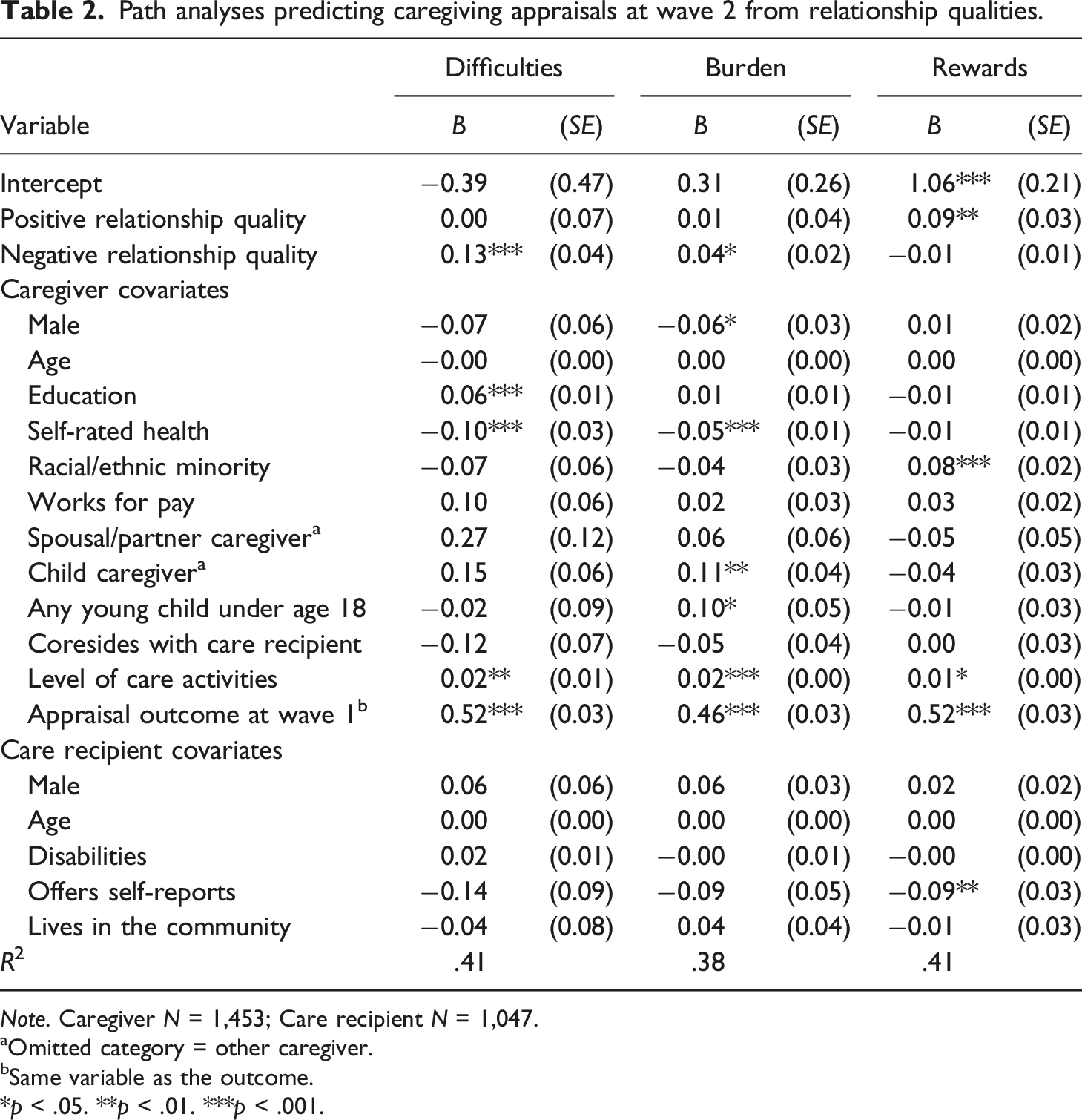
Note. Caregiver N = 1,453; Care recipient N = 1,047.
aOmitted category = other caregiver.
bSame variable as the outcome.
*p < .05. **p < .01. ***p < .001.
Care recipient age and disability as moderators in the association of relationship qualities with caregiving difficulties and rewards.
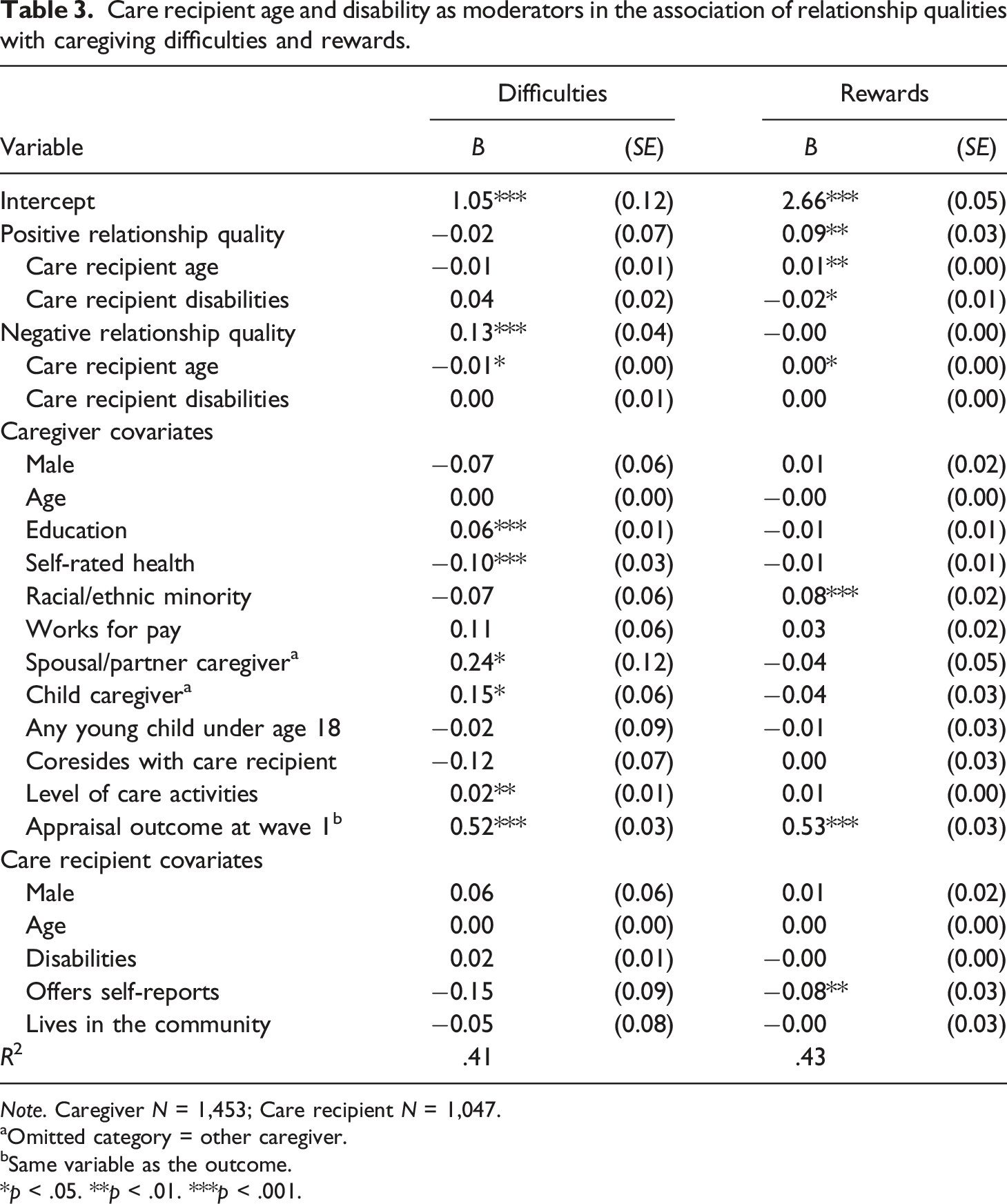
Note. Caregiver N = 1,453; Care recipient N = 1,047.
aOmitted category = other caregiver.
bSame variable as the outcome.
*p < .05. **p < .01. ***p < .001.
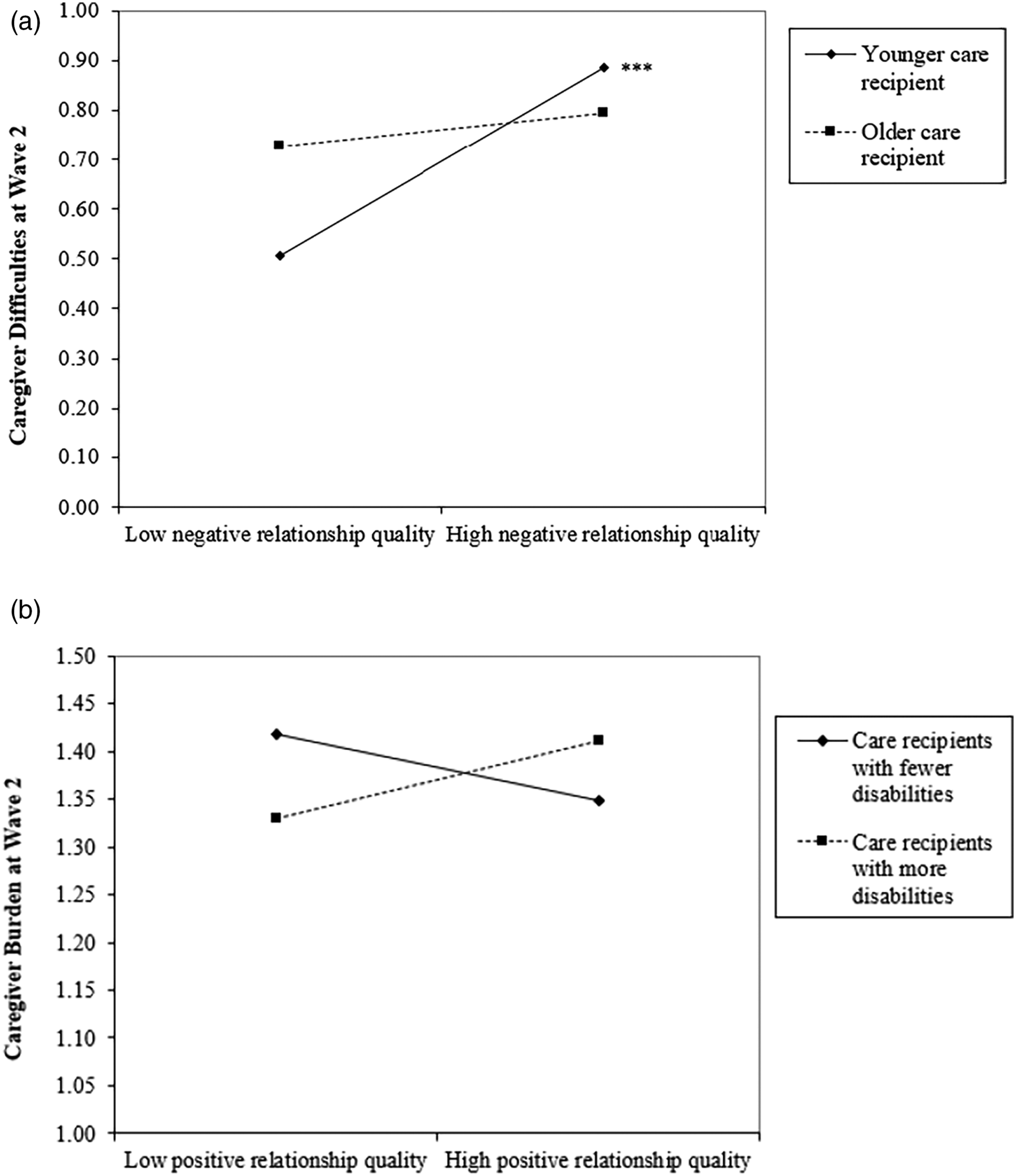
Interaction plots predicting difficulties and burden of caregiving at wave 2. Note. Interactions of relationship quality with (a) care recipient age and (b) care recipient disabilities predicting difficulties and burden of caregiving. ***p < .001.
For rewards of caregiving, we observed two significant interactions of positive relationship with (a) care recipient age (B = 0.01, p = .004) and (b) care recipient disabilities (B = −0.02, p = .040). Simple slopes analysis revealed that positive relationships with care recipients were associated with increased rewards of caregiving only for caregivers of relatively older care recipients (B = 0.18, p < .001)—but not for those with younger care recipients (B = 0.00, p = .89; see Figure 3(a)). Positive relationship quality was also associated with greater rewards of caregiving only for caregivers whose care recipients reported lower levels of disabilities (B = 0.15, p < .001), but not for those caring for recipients with higher levels of disabilities (B = 0.03, p = .36; see Figure 3(b)). Interaction plots predicting rewards of caregiving at wave 2. Note. Interactions of relationship quality with (a) care recipient age and (b) care recipient disabilities predicting rewards of caregiving. ***p < .001.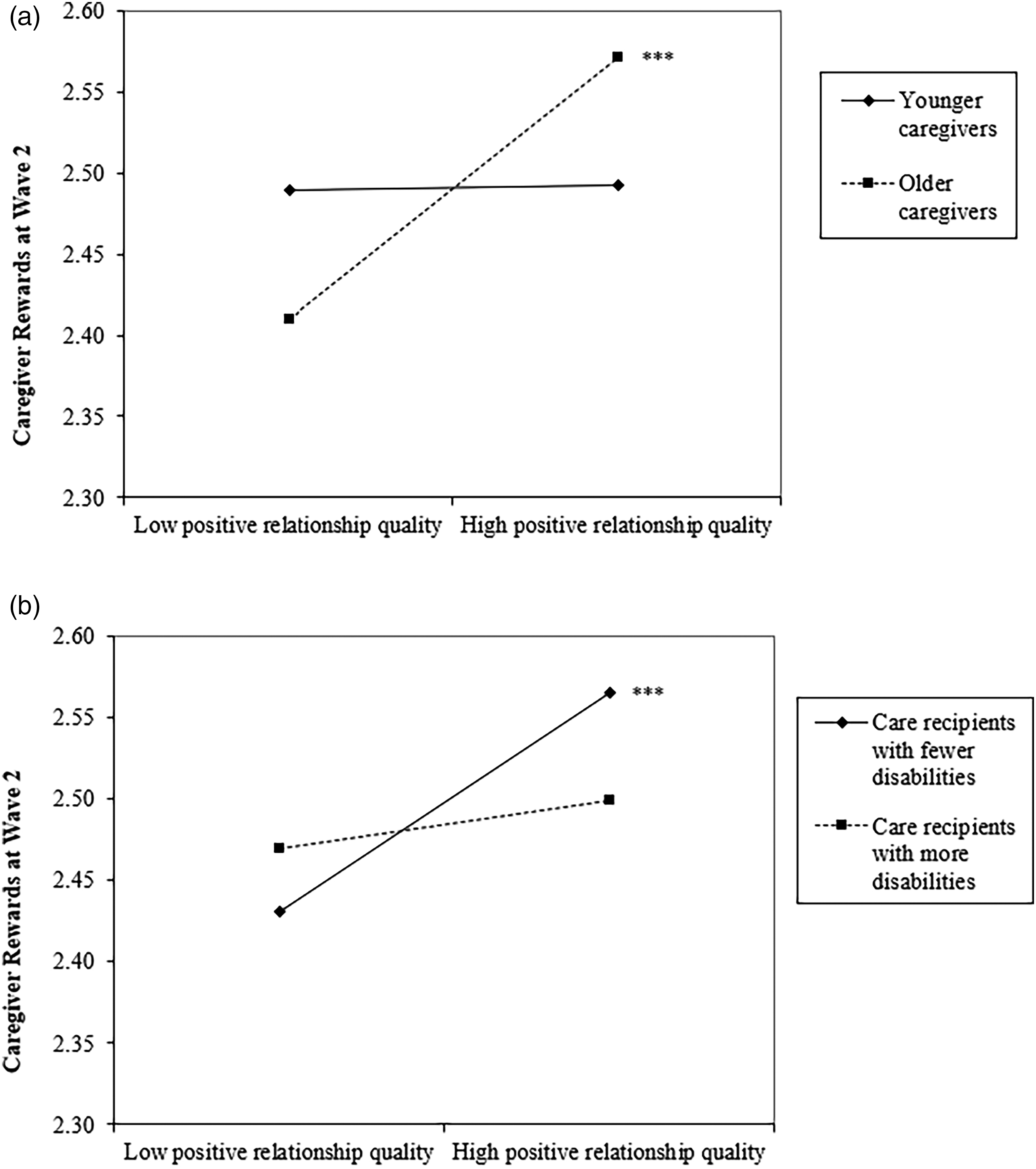
Post-hoc tests
We performed some post-hoc tests. Given the potential co-existence of positive and negative feelings in caregiving relationships, we re-estimated our models, treating ambivalence as the key predictor. In line with prior research (Gilligan et al., 2015), we calculated an ambivalence score by integrating both positive and negative relationship qualities. Findings revealed that caregivers who experienced greater ambivalence in their relationships with care recipients tended to report more increased feelings of difficulties (B = 0.10, p < .001) and reduced rewards over time (B = −0.02, p = .034). Also, this association varied depending on care recipient age (B = −0.01, p = .038), suggesting a stronger association among caregivers with younger care recipients (B = 0.14, p < .001).
We re-estimated models to examine differences by gender. We tested interaction terms of relationship qualities × caregiver gender and relationship qualities × care recipient gender and examined them in the same models. We did not find any gender differences. We also considered the moderating effect of coresidence but did not find any significant results.
Lastly, to address the potential impact of relationship type, we estimated additional models with interaction terms involving relationship type (caregivers other than a spouse/partner or a child were treated as the reference group). Findings revealed a stronger association between negative relationship quality and rewards of caregiving among adult child caregivers, as compared to other caregivers (B = 0.09, p = .010).
Discussion
The current study adds to the existing literature by presenting a longitudinal investigation of the association between relationship qualities and caregivers’ appraisals of caregiving, and specifying the distinct roles positive versus negative relationship qualities play. We found that caregivers who had more negative relationships with care recipients experienced more negative appraisals (i.e., a greater increase in difficulties and burden) over time, whereas caregivers with more positive relationships indicated a greater increase in rewards of caregiving. We also observed interesting variations in these associations between relationship qualities and caregiving appraisals, depending on care recipient characteristics. More negative relationships with care recipients were associated with increased difficulties only among caregivers with younger care recipients, whereas for caregivers with older care recipients, positive relationships co-occurred with increased rewards of caregiving over time. Interestingly, however, despite an established positive correlation between age and disabilities, we found that positive relationships between caregivers and care recipients were associated with increased rewards of caregiving only among caregivers whose care recipients reported fewer disabilities. Findings advance our understanding of social factors related to late life caregiving, and provide empirical evidence that may help better identify caregivers at greater risk for poor outcomes and inform non-drug interventions intended to benefit both members of the caregiving dyad in the long run.
Relationship qualities and caregiving appraisals
Along with the advocation for viewing caregiving as a relational process, there has been increasing interest in the impact of relationship quality on caregiver outcomes. More specifically, prior research has primarily relied on cross-sectional data when examining the buffering effect of high-quality relationships (Hooker et al., 2015; Lum et al., 2014; Tough, Brinkhof, et al., 2017). To extend prior research, we examined independent impacts of positive and negative relationship qualities, and asked how these relationship qualities at baseline were associated with changes in caregiving appraisals over time. We found that negative relationships further increased caregivers’ difficulties and burden, whereas positive relationships brought about more rewards. As such, our findings offer additional support for the recently proposed Informal Caregiving Integrative Model (Gérain & Zech, 2019), which has particularly considered negative relationship quality as one of the main determinants of caregiver burnout and distress. Additionally, negative relationships likely co-occur with low empathy, which underlies poor quality communication and support exchanges (Huo et al., 2019; 2020; Verhofstadt et al., 2016) that may eventually lead to unmet needs (Cohen-Mansfield, 2000). Caregivers who report more negative relationships with their care recipients may have difficulty perceiving and addressing their care recipients’ needs, which over time could reduce the quality of their caregiving and further elicit their feelings of frustration and burden (Gaugler et al., 2005; Monin et al., 2020; van der Roest et al., 2007).
Our findings also contribute to the growing body of research on positive aspects of caregiving. Although most research has focused on identifying and lessening caregiver burden, more recent notions emphasize the importance of increasing rewards of caregiving (Yu et al., 2018). Our findings were in line with qualitative research that identified love as a key factor that helped caregivers maintain positive attitudes towards caregiving (Lloyd et al., 2016). Caregivers may simultaneously have positive and negative appraisals of their caregiving experiences, and interventions would be more effective if targeting both aspects. This study offers insights into the development of such interventions. For example, intervention practitioners may consider adding relationship therapies that not only promote understanding and affection in caregiving dyads, but also help improve coping strategies in the face of negative experiences.
Caring for persons of different ages and disabilities
This study tested variations in the lasting impact of relationship qualities on caregiving appraisals by care recipient age and disabilities. We observed that negative relationships were only associated with increased caregiving difficulties when care recipients were relatively younger, and positive relationships were only associated with increased caregiving rewards when care recipients were older. These findings offer empirical support to the Social Input Model in the caregiving context (Fingerman & Charles, 2010). Caregivers may perceive limited time left in older relatives’ lives and feel more motivated to dampen negative feelings and focus on positive experiences when caring for older care recipients. Indeed, our post-hoc tests examining ambivalence—co-occurrence of positive and negative feelings in a relationship found that caregivers of younger care recipients were more vulnerable to ambivalence. Further, consistent with socioemotional selectivity theory, older care recipients may be better able to sustain pleasant encounters and to deal with unpleasant tensions with their caregivers due to age-related strengths in emotion regulation (Charles & Carstensen, 2010), which could presumably increase rewards and reduce difficulties for these caregivers. Prior research has mostly documented that the link between negative relationship quality and poor well-being may be weaker among older individuals (especially those aged 80+; Birditt et al., 2018). Our study corroborated these findings by suggesting both a boosting effect of age on the benefits of positive relationships and a buffering effect of age on the downsides of negative relationships.
Interestingly, we found that having positive relationships with care recipients seemed to be more important to caregivers whose care recipients had lower levels of disabilities. Caregivers’ positive relationships with care recipients were not associated with changes in caregiving rewards over time if these care recipients reported greater disabilities. People with fewer disabilities require less assistance from their caregivers, so it is possible that these caregivers can more effectively contribute to these care recipients’ welfare and thus to experience greater rewards related to relationship gains or sense of duty (Lloyd et al., 2016). For caregivers whose care recipients struggle with greater disabilities, however, they may not be able to enjoy caregiving even if they maintain highly positive relationships with these care recipients. Scholars suggest that positive relationships can trigger distress when these relationships involve health concerns and suffering (Kiecolt-Glaser & Wilson, 2017; Monin et al., 2017). It is worth noting that the data we drew from did not reveal specific causes of care recipients’ disabilities, which may or may not result from a life limiting illness (e.g., Parkinson’s or Alzheimer’s). Future research may benefit from examining relationship quality in more depth, such as by exploring the role of specific social experiences that may occur in more positive caregiving relationships (e.g., dyadic coping, mutual understanding).
Limitations and conclusion
There are several limitations that warrant consideration. Relationship quality was solely reported by caregivers, but prior research has documented discrepancy in spousal reports on relationship quality (Carr & Boerner, 2009), especially among caregiving couples (Clare et al., 2012). The 2-item measures of relationship quality used in the NSOC data are also limited. For example, the measure of positive relationship quality only tapped companionship enjoyment and appreciation—not love, affection, or support. Moreover, little context was provided regarding how long caregivers had been helping care recipients, and what their relationship was like prior to the 2015 measure. We drew on 2-wave data collected with an interval of 2 years. Researchers may examine even longer-term effects of relationship quality when future waves become available. Further, although we adjusted for care recipients’ physical disability at baseline, it would be helpful to obtain more information regarding how long they have been disabled. Indeed, the progression of disability may occur at different paces in different phases. Some older adults may live with one disability for many years, whereas those who have been restricted in many aspects of daily living may live under stress and are more likely to develop chronic health conditions and additional disabilities (Almeida, 2005; Knight et al., 2021). Lastly, it is worth noting that the small coefficients reported in this study, although statistically significant, should be interpreted with caution.
Despite these limitations, the current study offers a longitudinal investigation that advances our understanding of how the baseline quality of relationships between care recipients and caregivers may influence caregivers’ appraisals of caregiving over time. Our findings revealed both positive and negative impacts of caregiving relationships and identified individual differences in these impacts depending on care recipient characteristics. This study provides further empirical evidence regarding the need for dyadic interventions that foster mutually beneficial relationships between caregivers and their care recipients (Rausch et al., 2017). It is crucial to focus on both lessening negative appraisals of caregiving and promoting positive appraisals. We also argue that these interventions may be more effective for improving quality of life for caregivers caring for older care recipients, or those with lower levels of disabilities.
Supplemental Material
Supplemental Material - Lasting impact of relationships on caregiving difficulties, burden, and rewards
Supplemental Material for Lasting impact of relationships on caregiving difficulties, burden, and rewards by Meng Huo and Kyungmin Kim in Journal of Social and Personal Relationships
Footnotes
Author contributions
M. Huo planned the study, reviewed the literature, performed all statistical analyses and wrote the paper. K. Kim helped to plan the study, supervised data analysis, and contributed to revising the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open research statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.