
Abstract
People often rely on partner support and shared reality during stressful and uncertain times. As such, the current research explored how these may relate to relationship satisfaction during the COVID-19 pandemic. To do so, 155 frontline health-care workers and their significant others completed measures of shared reality and relationship satisfaction, while also indicating their levels of perceived or provided support, respectively. We proposed that shared reality would foster partners providing and health-care workers perceiving support which would, in turn, promote greater relationship satisfaction. Overall, both shared reality and partner support were positively associated with relationship satisfaction for health-care workers and their significant others. Using the Actor-Partner Interdependence Model with Mediation (APIMeM), we found shared reality to be associated with greater relationship satisfaction through health-care workers perceiving greater support from their partner. Our research demonstrates that shared reality may be a way for people under stress to perceive greater partner support, providing relational benefits for the couple as a whole.
One year into the COVID-19 pandemic, the Public Health Agency of Canada (2021) and the Centers for Disease Control and Prevention (2021) estimated the number of confirmed cases to be approximately 910,000 in Canada and 29 million in the United States with a death toll surpassing 22,000 and 530,000, respectively. These numbers continue to rise as the novel coronavirus spreads rapidly on an international scale (Li et al., 2020; Wu et al., 2020). Frontline health-care workers are presently facing extreme circumstances as they assume the burden of treating patients who have been infected with the virus (Maunder et al., 2004; Nickell et al., 2004; Styra et al., 2008). While the long-term repercussions of the pandemic are still unclear, it is evident that health-care workers are experiencing increased levels of stress and uncertainty (Shanafelt et al., 2020), largely stemming from an excessive workload, lack of personal protective equipment, and a greater risk of infection (Cai et al., 2020).
Research shows that stress originating outside of the relationship can spillover into the relationship due to couples’ shared interdependence (Randall & Bodenmann, 2009; Story & Bradbury, 2004). Thus, ineffective handling of external stressors, such as health-care workers’ frontline experiences, may threaten relationship satisfaction and ultimately result in relationship dissolution (Bodenmann, 1995; see Randall & Bodenmann, 2017 for review). As the novel coronarvirus continues to disrupt the global community, what psychosocial resources can health-care workers and their significant others use to reduce the anticipated, aversive effects on their relationship? The literature suggests that during negative and uncertain times, people tend to rely on their significant other to experience shared reality (Bar-Shachar & Bar-Kalifa, under review; Echterhoff et al., 2009; Hardin & Higgins, 1996) and social support (Cohen & Wills, 1985; Dunkel-Schetter, 1984), which benefit relationship satisfaction and closeness (Girme et al., 2018; Gleason et al., 2008; Rossignac-Milon et al., 2020; Rossignac-Milon & Higgins, 2018). The current research extends this line of work to examine frontline health-care workers and their significant others during the COVID-19 pandemic. In doing so, the present study will identify potential mechanisms that partners can use to minimize the negative effects of frontline stressors on their relationship satisfaction.
Shared reality
In the present research, shared reality is defined in line with generalized shared reality in romantic relationships (Rossignac-Milon et al., 2020). Specifically, shared reality is the experience of having the same thoughts, feelings, and concerns about the world as one’s significant other and is especially sought out during negative and uncertain events (Bar-Shachar & Bar-Kalifa, under review; Hardin & Higgins, 1996). People experience both a relational and an epistemic motive to share a reality with their significant other (Hardin & Higgins, 1996). Namely, people possess a relational motive to feel a sense of closeness and intimacy with their close others (Baumeister & Leary, 1995). People also possess an epistemic motive to make sense of the world and to feel that their subjective experiences are true and real (Echterhoff et al., 2009; Higgins, 2012). Establishing a shared reality with one’s significant other is a means to fulfilling these relational and epistemic needs and is ultimately associated with greater relationship closeness and satisfaction (Rossignac-Milon et al., 2020). Despite the absence of literature on the dyadic effects of shared reality, there is some evidence that shared reality may also promote partner relationship satisfaction. For instance, shared reality is associated with greater meaning (Andersen & Przybylinski, 2018; Przybylinski & Andersen, 2015), which can create more positive relational experiences for one’s partner (Hadden & Knee, 2018). Hadden and Knee (2018) argue that this may be due to greater meaning allowing for more authentic and less controlled interactions.
Partner support
Decades of research has demonstrated that social support (i.e., aid and assistance provided to an individual by one’s peers; Barrera et al., 1981) is especially sought out in stressful times (e.g., Bolger & Amarel, 2007; Cohen & Wills, 1985; Collins et al., 2014). Romantic partners are one of the primary sources of support, and research indicates that partner support is positively associated with relationship satisfaction and stability (Cutrona et al., 2005; Girme et al., 2018; Sullivan et al., 2010).
Provided support
In the current paper, provided support is defined as the partner’s ratings of support they provided. While provided support promotes greater relationship satisfaction (Girme et al., 2018; Gleason et al., 2008), the association may depend on whether the support is visible or invisible (e.g., Bolger et al., 2000). Visible support (i.e., support noticed by the recipient) has been positively associated with relationship satisfaction (Girme et al., 2013, 2018; Maisel & Gable, 2009), as well as feeling closer to and more cared for by one’s significant other (Collins & Feeney, 2000; Gleason et al., 2008). This may be due in part to the relational benefits that stem from perceiving one’s partner as an available caregiver (Collins & Feeney, 2000; Feeney, 2004) who one may turn to for comfort and security (Carnelley et al., 1996; Feeney, 1996). In contrast, the influence of invisible support (i.e., support not noticed by the recipient) on one’s relationship remains unclear. Whereas invisible support was found to predict greater relationship intimacy for couples coping with cancer (Belcher et al., 2011), no effects were found when examining relationship satisfaction in the context of couples’ daily interactions (Gable et al., 2003). One possibility for these mixed results is that people might be less accurate about the support they received during highly stressful times (Bolger et al., 2000). Alternatively, it may take time for the affiliative benefits of invisible support to sink in (Girme et al., 2018), whereby people are only able to experience their subtle relational effects once they are no longer focused on the stressor at hand.
Perceived support
We define perceived support as the actor’s ratings of support they received from their partner; however, we are especially interested in examining this type of support controlling for the partner’s provided support. 1 This is consistent with previous work that has explored perceived support days, which were found to promote greater relationship satisfaction (Girme et al., 2018) and, when the support was also responsive, greater relationship connectedness (Maisel & Gable, 2009). Since both perceived support and visible support are noticed by the recipient, it is likely that the mechanisms driving the association between visible support and relationship satisfaction (e.g., perceiving one’s partner as an available caregiver; Collins & Feeney, 2000) can be applied to perceived support.
Of the various types of support, the current paper will examine invisible and perceived support and we expect that these kinds of support will also bolster the support provider’s relationship satisfaction. 2 For instance, when a partner indicates that they provided support they might feel needed and valuable (Batson & Powell, 2003) and also experience a sense of reciprocity (Ryon & Gleason, 2018). Similarly, people who perceive greater partner support often feel a sense of gratitude (Algoe et al., 2010) and trust (Cutrona et al., 2005), which may consequently provide a boost to the partner’s relationship satisfaction.
Shared reality and partner support
Whereas both shared reality and partner support promote relationship satisfaction, less is known about how they relate to one another. Across various definitions, support is based on one’s partner satisfying one’s needs (Cutrona, 1996). Thus, as shared reality fulfills one’s epistemic and relational needs (Rossignac-Milon et al., 2020; Rossignac-Milon & Higgins, 2018), experiencing a shared reality should lead people to perceive greater support from their partner. For example, a health-care worker may return home from the hospital after a 12-hour shift of treating COVID-19 patients. They may discuss their day’s experience with their partner and together the couple may vocalize shared feelings and co-construct a shared understanding of the health-care worker’s experience. These behavioral signatures of shared reality should promote feelings of shared reality (Rossignac-Milon et al., 2020), which should allow the health-care worker to feel more certain about their experience and closer to their partner. The health-care worker should feel more supported by their partner as a result, regardless of whether the partner interprets their actions as support provision.
Shared reality is also thought to involve a shared understanding of the self (Rossignac-Milon & Higgins, 2018), which should boost partner predictability (Swann et al., 1992) and allow partners to provide more effective support and perceive greater support (Avtgis, 2000; Reis & Clark, 2013; Reis & Gable, 2015). Lastly, it is theorized that shared reality creates a sense of shared identity (Rossignac-Milon & Higgins, 2018), whereby partners come to experience one another’s perspectives, resources, and identities as their own (Aron et al., 2013). Having a fused identity with one’s ingroup promotes support from that ingroup (Buhrmester et al., 2015; Gómez et al., 2011; Segal et al., 2018) partially due to feeling greater familial ties (Swann et al., 2014). Building on this literature, establishing a shared reality with one’s significant other may promote a sense of shared identity and relational ties that, in turn, bolster one’s desire to provide partner support.
Present Study
The present study examined frontline health-care workers and their significant others (N = 155 dyads) during the first wave of the COVID-19 pandemic. Couples from across Canada and the United States participated in an online survey where they completed measures of shared reality, support, and relationship satisfaction. Specifically, health-care workers rated the extent to which they received support, whereas their significant others rated the extent to which they provided support. Both members of the dyad reported on shared reality and relationship satisfaction. The present study examined a possible link between shared reality and relationship satisfaction during a global pandemic, and whether the association is facilitated through perceived (controlling for provided) and invisible (provided controlling for perceived) support. As such, we used the Actor-Partner Interdependence Model with Mediation (APIMeM; Ledermann et al., 2011) to examine the actor and partner effects of shared reality and partner support on relationship satisfaction. We expected positive within-person associations between shared reality, support and relationship satisfaction, for which we hypothesized that shared reality would predict relationship satisfaction through greater perceived and invisible support. In contrast, possible dyadic effects were more exploratory, and we did not have any prior hypotheses. We were especially interested in examining whether actor shared reality would be associated with partner satisfaction and whether perceived support or invisible support might mediate associations between shared reality and partner’s relationship satisfaction.
Method
Participants
We recruited frontline health-care workers and their significant others through social media and health-care associations across Canada and the United States. To be eligible, participants had to be between the ages of 21 and 49. One member of each couple was required to be a frontline health-care worker either directly or indirectly exposed to COVID-19 positive patients while the other member could not be a health-care worker. Participants were required to be in an exclusive relationship and to have been dating for at least 6 months. Responses were collected from 320 participants. After removing data where one partner did not complete the survey, our final sample size was 310 participants (155 couples; Ma ge = 32, SD age = 6 years) wherein 152 participants self-identified as female, 157 participants as male, and 1 participant as other. In terms of ethnicity, 65% of participants were White, 9% were Asian, 8% were African, 6% were Oceanic, 5% were Indigenous, 4% were Latinx, and 4% were Other. Six romantic couples were of the opposite sex and the average relationship length across all couples was 6.6 years (Median = 5.38 years, SD = 5.4 years). Participants varied in romantic relationship type, whereby 21% were exclusively dating, 36% were cohabiting, and 39% were married. Participants were residing in either Canada (81%) or the United States (19%). Whereas within Canada participants were largely from Quebec (33%) or Ontario (26%), those from the United States were widely scattered across states, with the largest percentage residing in New York State (7%). Lastly, of the 155 health-care workers, 50% were doctors, 36% were nurses, and 11% were other, including respiratory therapists and technicians.
Procedure
Couples were recruited through social media (e.g., Facebook groups) and health-care associations (e.g., bi-weekly newsletters) across Canada and the United States. Recruitment took place during what the most represented regions in our sample considered to be the peak of the first wave. Specifically, the sample was collected in late April and early May of 2020 during which time regions like Quebec, Ontario, and New York had reached or were reaching the height of daily confirmed COVID-19 cases from the first surge of the pandemic (Centers for Disease Control and Prevention, 2021; Public Health Agency of Canada, 2021). Interested couples completed an eligibility survey which included questions about their relationship and occupation. Eligible participants were then invited to take part in an online survey and were subsequently compensated with a $5 Amazon gift card.
Measures
Descriptive information
Participants completed demographic measures including questions about their age, relationship length and occupation.
Shared reality scale–generalized (M = 5.24, SD = 0.88, α = 0.84)
Shared reality was assessed using the Shared Reality Scale (Rossignac-Milon et al., 2020) measured on a 7-point Likert scale (1 = disagree strongly, 4 = neutral, 7 = agree strongly). The scale includes 8 items such as “We typically share the same thoughts and feelings about things” and “Events feel more real when we experience them together.” The instructions were modified from the original scale whereby participants rated their agreement with the items since the onset of the pandemic. Higher numbers indicated greater shared reality with one’s romantic partner during the pandemic.
Social support (M = 2.94, SD = 0.60, α = 0.73)
Social support was assessed with 5 items adapted from Murray and colleagues’ (1996) Interpersonal Qualities Scale, which were measured on a 5-point Likert scale (1 = not at all, 5 = extremely). These 5 items were chosen because they were believed to be appropriate in assessing high-quality support and responsiveness. Whereas all participants were asked to respond to the questions with regards to the previous 2 weeks, the items were framed in such a way that health-care workers were asked about support that they received from their significant other while significant others were asked about support that they provided to the health-care worker. For health-care workers, items included “My partner was helpful” and “My partner understood how I was feeling.” For significant others, items included “I was helpful” and “I understood how my partner was feeling.” Higher numbers indicated greater perceived or provided support.
Relationship satisfaction (M = 5.07, SD = 1.34)
Relationship satisfaction was measured using the 1-item Quality of Marriage Index (Goodwin, 1992; Norton, 1983; Spanier, 1976), which has been found to be an appropriate and brief diagnostic tool to measure overall satisfaction. Participants were asked to rate their degree of happiness in their relationship on a 7-point Likert scale (1 = very unhappy, 4 = happy, 7 = perfectly happy). Higher numbers indicated greater relationship satisfaction.
Data analysis
To explore our research question, we used the Actor-Partner Interdependence Model with Mediation (APIMeM; Ledermann et al., 2011) with R’s nlme package (Pinheiro et al., 2015). The APIMeM is a multi-level modeling approach which examines both actor and partner effects within a dyad, treating the couple as the unit of analysis. An actor effect represents the influence of one’s own predictor on one’s own outcome, whereas a partner effect represents the influence of one’s partner’s predictor on one’s own outcome. In our model (see Figure 1), actor and partner shared reality are the predictors, perceived and provided support are the mediators, and actor and partner relationship satisfaction are the outcomes. Due to health-care workers’ unique experience on the frontlines, we chose to model all of our paths as distinguishable whereby health-care workers and significant others have unique actor and partner effects.
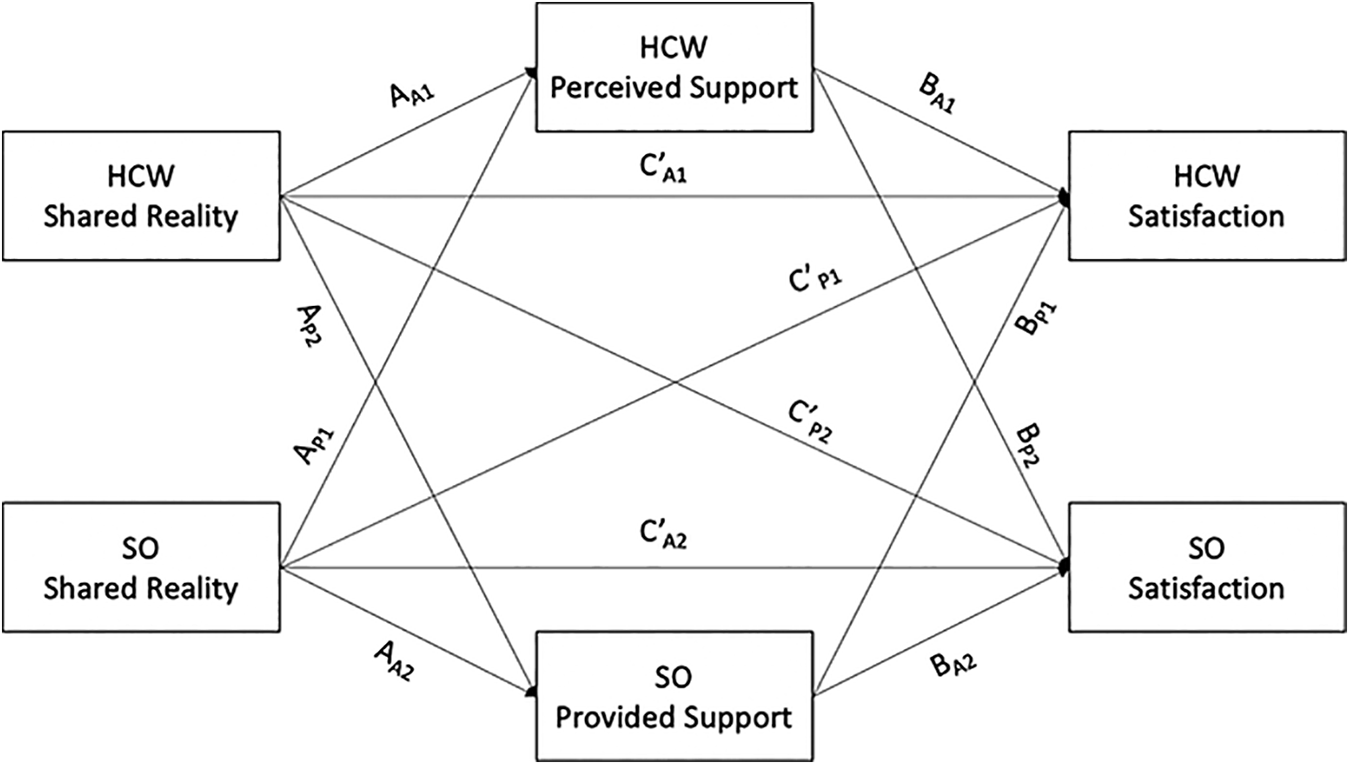
All effects were examined as distinguishable between health-care workers and their significant others. HCW refers to health-care worker, whereas SO refers to significant others.
The first part of the model in Figure 1 represents the A path of the mediation model (i.e., shared reality predicting support). The actor effects reflect the extent to which people’s own shared reality influences their own ratings of support; that is, perceived support for health-care workers (i.e., AA1) and provided support for significant others (i.e., AA2). In contrast, the partner effects (i.e., AP1 and AP2) represent the extent to which one’s partner’s rating of shared reality predicts one’s own ratings of support. When examining these effects, one controls for the other paths in the model, thus each unique effect accounts for the dyadic interdependence.
By including partner support as the mediator, the model examines eight additional effects (see Figure 1). Four of these effects, two actor and two partner, make up the B path of the mediation model (i.e., partner support predicting relationship satisfaction controlling for shared reality). For this path, since we model perceived and provided support simultaneously, perceived support represents support that health-care workers report receiving above and beyond what their significant other reported providing. In contrast, provided support represents significant others’ provided support that was not perceived (i.e., invisible support). For path B, the actor effects represent the extent to which health-care workers’ perceived support (i.e., BA1) or significant others’ provided support (i.e., BA2) predict their own relationship satisfaction controlling for their partner’s rating of support. In contrast, the partner effects illustrate the extent to which significant others’ invisible support (i.e., BP1) or health-care workers’ perceived support (i.e., BP2) predict their partner’s relationship satisfaction, controlling for their partner’s rating of support. This model also includes the direct effects of shared reality on relationship satisfaction controlling for partner support (i.e., path C’). The actor effects (i.e., C’A1 and C’A2) represent the influence of one’s own shared reality on one’s own relationship satisfaction. In contrast, the partner effects (i.e., C’P1 and C’P2) illustrate the influence of one’s partner’s shared reality on one’s own relationship satisfaction. While not part of the APIMeM model, we also examined the total effect of shared reality on relationship satisfaction (Path C), which is similar to Path C’ but does not control for perceived or provided support.
In our model, each couple had two sets of parameters, one for health-care workers and one for their significant others. Individual reports (Level 1) were nested within couples (Level 2). Intercepts were allowed to vary randomly across individuals and residual terms were allowed to be correlated between partners. Additionally, we allowed for different error variances for the two members of the couple. Lastly, to examine whether the indirect effects in this model were consistent with a pattern of mediation, we calculated the 95% confidence intervals for each indirect effect using the Monte-Carlo Method for Assessing Mediation (MCMAM; Selig & Preacher, 2008).
Results
First, exploring the A path of our APIMeM with shared reality predicting partner support (see Figure 2 and Table 1), the actor effects (i.e., AA1 and AA2), that is, whether shared reality predicted one’s own ratings of support, were significant for both health-care workers and significant others. That is, when health-care workers experienced shared reality they perceived more support, and when significant others experienced shared reality they provided more support. Health-care workers and significant others did not show a significant difference in their actor effects (b = −0.07, p = .37). The partner effects for the A path (i.e., AP1 and AP2), that is, whether partner shared reality predicted actor ratings of support, were significant for health-care workers but not for significant others. Thus, while significant others’ shared reality was associated with health-care workers perceiving greater support, health-care workers’ shared reality was not related to their significant other providing more support. However, there was no significant difference in these effects between health-care workers and significant others (b = −0.10, p = .20).
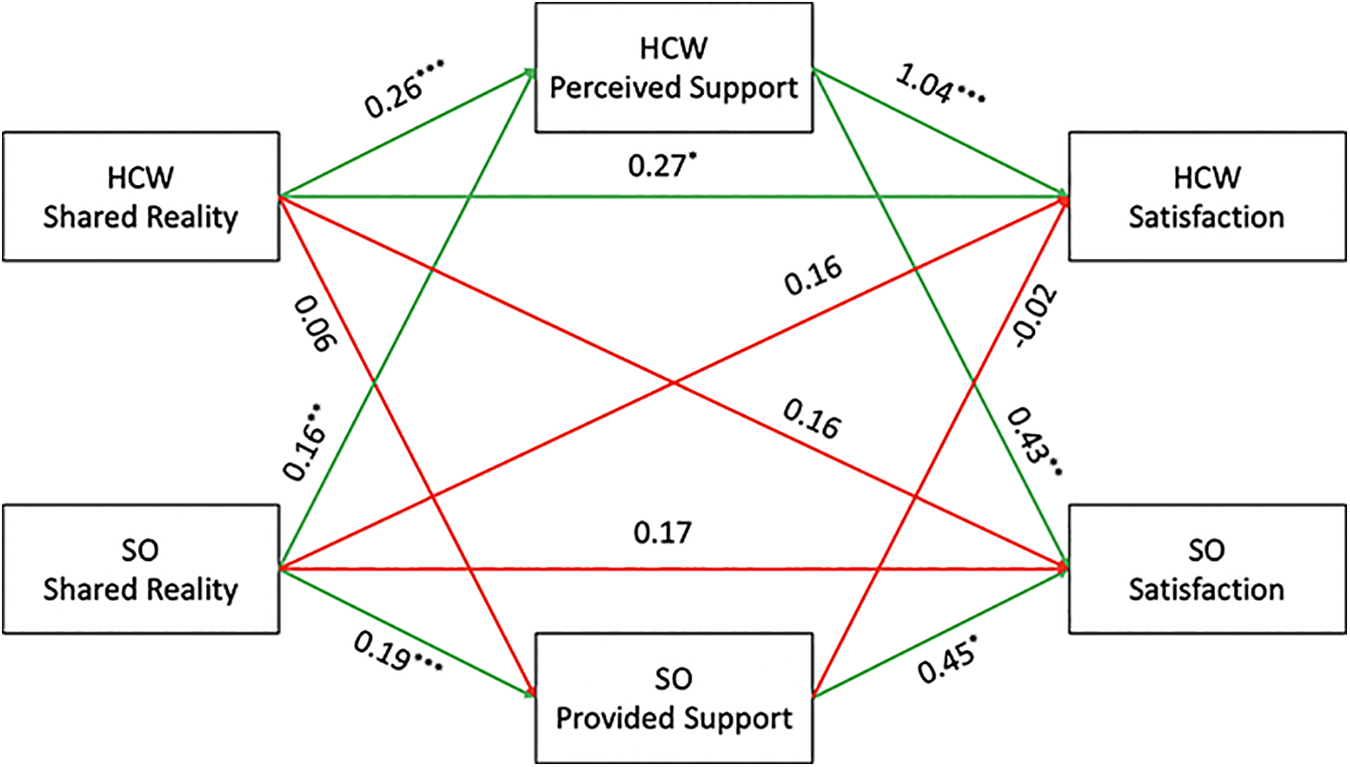
All effects were examined as distinguishable between health-care workers and their significant others. HCW refers to health-care worker, whereas SO refers to significant others.
Actor-Partner Interdependence Model with Mediation results.
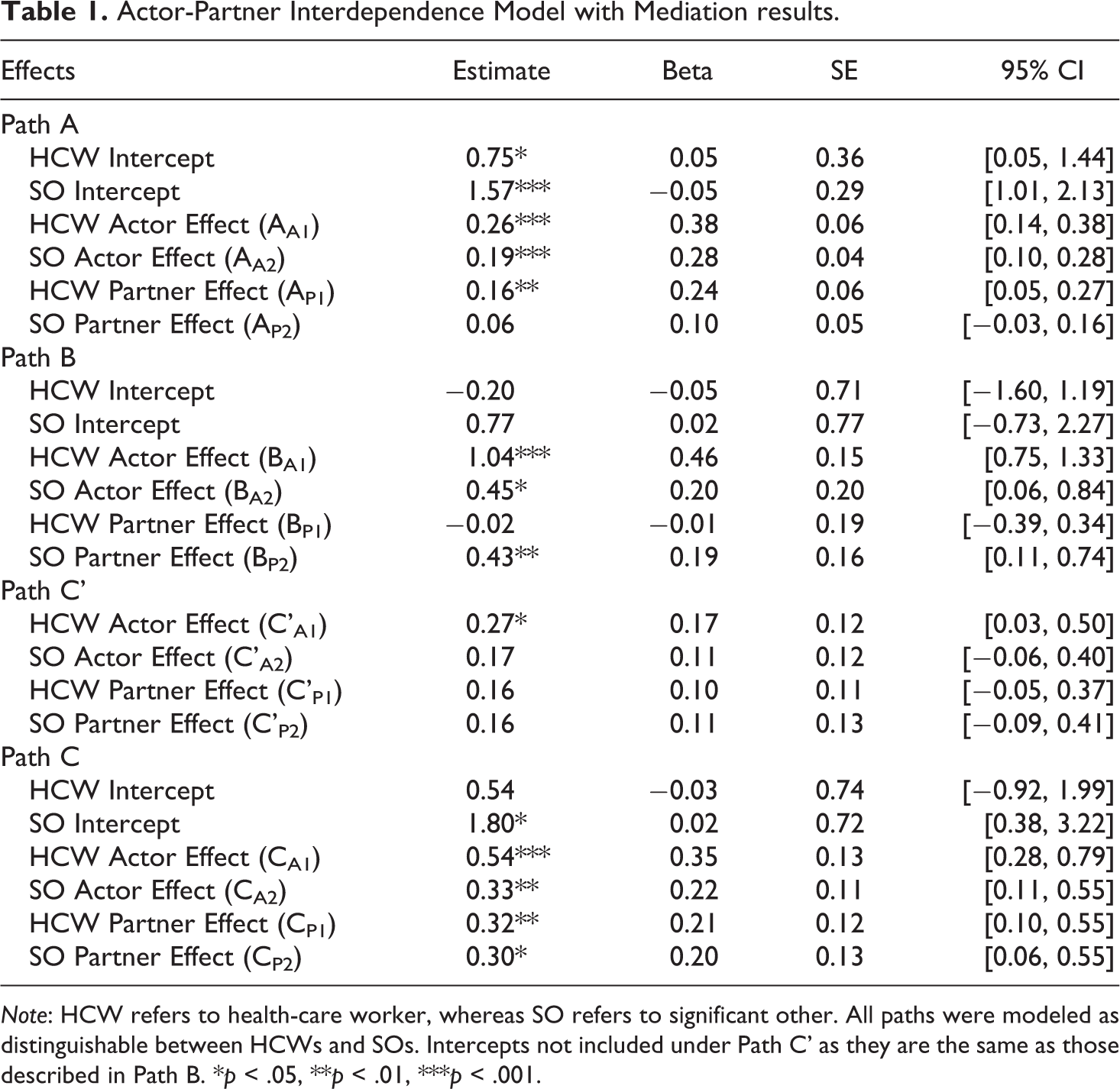
Note: HCW refers to health-care worker, whereas SO refers to significant other. All paths were modeled as distinguishable between HCWs and SOs. Intercepts not included under Path C’ as they are the same as those described in Path B. *p < .05, **p < .01, ***p < .001.
Moving onto the B path of the mediation model, we examined the influence of partner support on relationship satisfaction controlling for shared reality (see Figure 2 and Table 1). Of note, since the APIMeM adjusts for dyadic interdependence, the perceived support effects represent the influence of support that health-care workers perceived above and beyond what their significant other reported. On the other hand, the provided support effects represent the influence of the support that significant others reported providing but that health-care workers did not perceive (i.e., invisible support). For the B path, the actor effects (i.e., BA1 and BA2), that is, whether one’s own ratings of support predicted one’s own ratings of relationship satisfaction, were significant for both health-care workers and significant others. Specifically, when health-care workers felt that their significant other had been more supportive than their significant other claimed to have been they experienced greater relationship satisfaction. Similarly, when significant others provided support that health-care workers did not perceive, significant others also felt more satisfied in the relationship. These effects were significantly different, whereby health-care workers’ perceived support showed a greater effect than significant others’ provided support (b = −0.59, p < .05). However, the partner effects (i.e., BP1 and BP2), that is, whether partner support predicted actor ratings of relationship satisfaction, were significant for significant others but not for health-care workers. Thus, while the support that health-care workers perceived above and beyond what their significant other reported was significantly associated with their significant others’ feelings of satisfaction, invisible support was not associated with health-care workers’ relationship satisfaction. 3 Interaction analyses indicate a marginal difference in these effects (b = 0.45, p = .07), whereby perceived support had a marginally greater effect on significant others’ relationship satisfaction than did invisible support on health-care workers’ relationship satisfaction.
Lastly, we examined the total effects (i.e., shared reality predicting relationship satisfaction; see Table 1) and direct effects (i.e., shared reality predicting relationship satisfaction controlling for support; see Figure 2 and Table 1). For the total effects, the actor effects (i.e., CA1 and CA2), that is, whether one’s own shared reality predicted their own ratings of relationship satisfaction, were significant for health-care workers and for significant others. Specifically, when health-care workers and significant others experienced greater shared reality they also experienced greater relationship satisfaction, and these effects were not significantly different (b = −0.21, p = .25). The partner total effects (i.e., CP1 and CP2), that is, whether partner shared reality predicted actor relationship satisfaction, were also significant for both health-care workers and significant others. Thus, experiencing greater shared reality resulted in one’s partner feeling more satisfied in the relationship, and there was no significant difference between health-care workers and significant others (b = −0.02, p = .91). For the direct effects, the actor effects (i.e., C’A1 and C’A2), that is, whether one’s own shared reality predicted their own ratings of relationship satisfaction controlling for support, were significant for health-care workers but not for significant others. This finding indicates that when controlling for perceived and provided support, health-care workers’ shared reality influenced their own satisfaction while significant others’ shared reality did not; however, this effect was not significantly different (b = −0.09, p = .59). The partner direct effects (i.e., C’P1 and C’P2), that is, whether partner shared reality predicted actor relationship satisfaction controlling for support, were not significant for health-care workers or significant others. Thus, health-care workers’ and significant others’ relationship satisfaction was not associated with partner ratings of shared reality when controlling for social support, and there was no significant difference in these effects (b = 0.004, p = .98). To explore a pattern consistent with mediation, we also examined the indirect effects to assess whether the association between shared reality and relationship satisfaction could be explained by support.
Table 2 illustrates the eight indirect effects that were modeled to test whether support mediated the link between shared reality and relationship satisfaction. We conducted MCMAM-analyses (Selig & Preacher, 2008) with 3,000 iterations whereby the ab covariance was constrained to 0. The majority of the tested indirect effects were significant (see indirect effects in bold), with the exception of those that included the non-significant path from health-care worker shared reality to significant other provided support (i.e., AP2) and the non-significant path from significant other provided support to health-care worker relationship satisfaction (i.e., BP1). For the actor indirect effects, the actor-actor effect was significant for health-care workers (AA1BA1) and for significant others (AA2BA2). This finding suggests that shared reality predicted one’s own perceived or provided support which in turn predicted their own relationship satisfaction. The partner-partner effect was significant for significant others (AP1BP2) but not for health-care workers (AP2BP1) which suggests that significant others’ shared reality predicted their own relationship satisfaction by way of health-care workers perceiving greater support. However, these findings also suggest that health-care workers’ shared reality did not predict their own satisfaction through significant others’ invisible support.
MCMAM indirect effects.
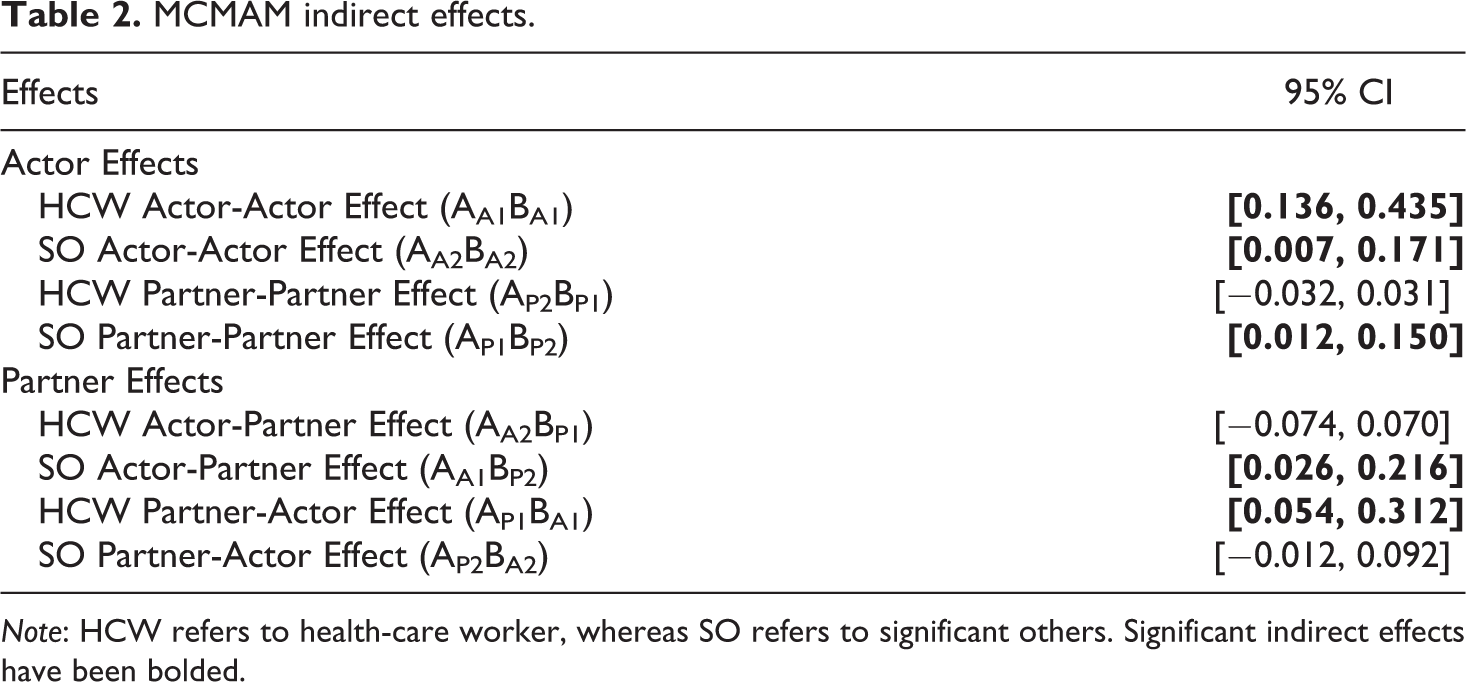
Note: HCW refers to health-care worker, whereas SO refers to significant others. Significant indirect effects have been bolded.
Moving onto the partner indirect effects, the actor-partner effect was significant for significant others (AA1BP2) but not for health-care workers (AA2BP1) which suggests that health-care workers’ shared reality predicted significant others’ satisfaction through health-care workers perceiving greater support from their significant other. However, invisible support did not influence the link between significant others’ shared reality and health-care workers’ relationship satisfaction. Lastly, the partner-actor effect (i.e., AA1BP2, AA2BP1) was significant for health-care workers (AP1BA1) but not for significant others (AP2BA2); thus, significant others’ shared reality was associated with health-care workers’ relationship satisfaction through health-care workers perceiving greater support. However, invisible support did not influence the link between health-care workers’ shared reality and significant others’ relationship satisfaction. Taken together, there was evidence consistent with a pattern of mediation for perceived support as the mediator but not provided support, with the exception of the significant other’s actor-actor effect.
Discussion
The present study explored how romantic partners can use shared reality and partner support to limit the potential threat of health-care workers’ frontline experience on their relationship satisfaction. In line with prior work (Cunningham & Barbee, 2000; Girme et al., 2018; Rossignac-Milon et al., 2020), the current research found shared reality and partner support to be positively associated with relationship satisfaction. Thus, in the face of the external pressure stemming from health-care workers’ frontline experience, sharing a reality with one’s partner along with providing and perceiving support allow romantic partners to feel more satisfied in their relationship. The present research also provides evidence for the dyadic effect of shared reality on relationship satisfaction. Specifically, one’s own shared reality was associated with their partner’s relationship satisfaction above and beyond the partner’s shared reality, and the effect was not significantly different between health-care workers and their significant others.
One possible explanation is that experiencing shared reality promotes feeling close to one’s partner and more certain about one’s subjective experience (Rossignac-Milon et al., 2020), which might ultimately provide positive, indirect benefits to how the partner feels about the relationship. For instance, there is evidence to suggest that shared reality plays a role in establishing meaning (Andersen & Przybylinski, 2018; Przybylinski & Andersen, 2015), which has been found to promote partner’s relationship experiences (Hadden & Knee, 2018). Hadden and Knee (2018) theorize that this may be due to partners experiencing more natural and less controlled interactions, which we argue could be positive for the partner’s relationship satisfaction. As people are more likely to seek out shared reality during difficult times (Bar-Shachar & Bar-Kalifa, under review; Hardin & Higgins, 1996), finding evidence of the positive, dyadic benefits of shared reality within this context is especially valuable.
The main purpose of this research was to explore the role of specific types of support (i.e., perceived and invisible support) as mediators in the association between shared reality and relationship satisfaction. Based on the indirect effects, there is evidence to suggest a pattern consistent with mediation for perceived support as the mediator. That is, shared reality experienced by health-care workers and their significant others was related to greater perceived support by the health-care worker which, in turn, was linked to greater relationship satisfaction for both members of the couple. Shared reality fulfills one’s relational and epistemic needs (Rossignac-Milon et al., 2020); in doing so, the satisfaction of one’s needs should lead people to feel more supported by their partner (Cutrona, 1996). Further, shared reality is theorized to promote a shared understanding of the self (Rossignac-Milon & Higgins, 2018), which should allow partners to provide more responsive support and ultimately enhance recipients’ perceptions of support (Reis & Gable, 2015). For instance, a health-care worker who comes home from work might want time to rest and unwind after a long day. If the couple shares a reality, they should also share an understanding of the health-care worker, including their post-work preferences. As a result, the partner could be responsive to the health-care worker’s needs by providing them with space and not probing them with questions about their workday. This should allow the health-care worker to perceive greater support from their partner (e.g., Repetti, 1989). Ultimately, this heightened perception of support should result in greater relationship satisfaction for the health-care worker (Girme et al., 2018) as it provides evidence that their partner is an available caregiver (Feeney & Collins, 2003; Girme et al., 2013). However, as evidenced by our findings, perceived support should also be positively associated with the partner’s relationship satisfaction, which could be due to the health-care worker feeling a sense of gratitude (Algoe et al., 2010) and trust (Cutrona et al., 2005) toward their partner.
Our findings also suggest that idealizing the amount of support that was enacted by one’s partner is beneficial to the relationship, expanding upon a widely accepted notion that idealized perceptions of one’s partner can promote relationship satisfaction (e.g., Murray et al., 1996).
On the other hand, support that significant others reported providing but health-care workers did not perceive (i.e., invisible support) was not associated with health-care workers’ relationship satisfaction. Further, when significant others’ provided support was examined as the mediator the indirect effects were not significant, with the exception of the within-effect for significant others (i.e., the actor-actor effect, AA2BA2). This finding does not support recent literature which indicates that invisible support is beneficial to relationship satisfaction over time (Girme et al., 2018); however, this may be explained by the context and population examined in the current research. It is possible that given the stressful and uncertain context in which health-care workers find themselves they may be more attuned to signs of support from their partner and appraise daily acts as especially important. This may lead them to pick up on more objective signs of support (Girme et al., 2013), which would no longer be considered invisible support. Zee and Bolger (2019) also argue that the effects of invisible support may depend on the recipient’s motivation, whereby invisible support is more beneficial when one is in an evaluative situation, which does not fit the current context. The present study also examined a summary of support across a 2-week period as opposed to daily reports, which might provide further insight into why our findings differ from recent work examining invisible support.
Lastly, health-care workers’ shared reality was not associated with their significant others’ ratings of provided support. It is possible that by fulfilling the health-care workers’ relational and epistemic needs through greater shared reality, significant others are simultaneously providing health-care workers with aid and assistance. However, fulfillment of these needs might not translate to the significant others indicating that they provided greater support as they may not consider this to be explicit support provision. Given that this is the first study to examine actor and partner shared reality and invisible support, these inferences are speculative and require further investigation.
Overall, the present study identifies shared reality and perceived support as mechanisms that can promote the maintenance of high-quality relationships in the face of external stressors. In light of these findings, it may be beneficial for health-care workers and their significant others to foster greater shared reality in their relationship. To achieve this, shared reality theory in close relationships (Rossignac-Milon & Higgins, 2018) suggests that partners should take part in joint activities (e.g., weekly cooking nights) while simultaneously fostering communication (e.g., self-disclosing, expressing one’s emotions). This may be very difficult during the pandemic as health-care workers may often be physically and emotionally depleted when they return home. However, any ways the couple can be together and share in some experience may bolster their shared reality, which should ultimately have a positive impact on health-care workers’ perceptions of support and the couple’s overall satisfaction.
In sum, although strong romantic relationships fulfill our basic need to belong (Baumeister & Leary, 1995), the foundation of these relationships can be undermined by external stressors (e.g., Randall & Bodenmann, 2017). The present study explored a unique context in which to examine the role that these stressors play on relationship satisfaction. Our findings provide evidence that shared reality and perceived support help to minimize their adverse effects on one’s romantic relationship. In doing so, this work has implications for how romantic partners can maintain satisfaction in their relationship even when they are confronted with stress and uncertainty.
Limitations and future directions
The current research is not without its limitations. Most notably, the cross-sectional design did not allow for evidence of mediation or causality. As a result, it is possible that relationship satisfaction promotes greater perceived support which in turn promotes shared reality. However, given prior research that highlights the influence of shared reality and partner support on relationship satisfaction and closeness (e.g., Girme et al., 2018; Rossignac-Milon et al., 2020), we believe that the direction of the proposed mediation model is adequately supported by theory. Shared reality was also found to have a non-significant effect on relationship satisfaction when controlling for support, with the exception of health-care workers’ shared reality predicting their own satisfaction. As a result, there does not appear to be evidence to support the reverse mediation model of support predicting relationship satisfaction through shared reality, as the B path in this model would not be significant. An additional limitation is that support was examined over a period of 2 weeks, which did not allow for the measurement of daily levels of support provision. Because prior work suggests that the effects of visible and invisible support may change across days (e.g., Girme et al., 2018), it may be beneficial to examine our hypotheses in a daily diary design.
Despite these limitations, the current research is the first to explore this pattern of mediation and to examine these constructs with a new operationalization of perceived support (i.e., perceived–provided) and a dyadic analysis of shared reality. This study is also the first to explore shared reality and partner support in this context and within this population. In doing so, the present research expands upon the current literature surrounding shared reality, partner support, and relationship satisfaction. Our findings provide valuable insight into a pattern of dyadic processes through which romantic partners can minimize the effects of frontline stressors on their relationship, the implications of which extend beyond the COVID-19 pandemic.
Conclusion
The present research explored frontline health-care workers and their significant others during the COVID-19 pandemic. Shared reality and support were examined as potential mechanisms through which romantic partners can maintain relationship satisfaction in the face of external stressors. Overall, both shared reality and partner support were positively associated with relationship satisfaction for health-care workers and their significant others. Moreover, health-care workers’ perceptions of support received were found to show a pattern consistent with mediation in the link between shared reality and relationship satisfaction. Taken together, the current work suggests that shared reality plays an important role in promoting perceived support and that the benefits of shared reality extend beyond one’s own outcomes, providing additional benefits for one’s significant other.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present research was supported by a Social Sciences and Humanities Research Council of Canada (SSHRC) Insight Grant (245846). The preparation of this manuscript was supported in part by funding from the SSHRC’s Canada Graduate Scholarship for the Master’s Program to M. Catalina Enestrom.
Open research statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This research was not pre-registered. The data used in the research are available. The data can be obtained by emailing: