
Abstract
Braille significantly facilitates independent travel, as with the use of braille on public signage. This study explored the current role of braille within O&M university programs and gathered perceptions from O&M specialists on the role of braille within pre-service training. A total of 44 participants (O&M specialists in the United States and Canada) completed an online survey on braille practices and perceptions. Participants rarely or never use braille in their practice (84%), and this is even more pronounced among those serving adults only (90%). Results suggest that braille competency may account for fewer O&M services that incorporate braille, particularly for those working with adults. Current O&M academic programs should consider offering supplemental courses for practitioners to ensure a basis of braille competency. Professional training to maintain skills should also be supported by places of employment to ensure that O&M specialists are able to provide braille support to clients of all ages.
Introduction
Braille is a tactile reading and writing system used by individuals who are blind, deafblind, or who have low vision (Jaiswal et al., 2020). Studies confirm that braille is associated with higher levels of education, income, and employment for those who are blind (Ryles, 1996; Rose et al., 2025). Additional studies highlight increased positive perceptions about blindness, self-efficacy, and overall independence, even among blind adults who learn braille later in life (Martiniello et al., 2022; Silverman & Bell, 2018). Evidence indicates that braille learning is possible throughout the life span, particularly when strategies are used to attach learning to meaningful goals, including those related to independent travel (Bola et al., 2016).
In the education system, braille literacy is primarily supported by teachers of students with visual impairments (TVIs). In the adulthood rehabilitation setting, braille is often taught by certified vision rehabilitation therapists (CVRTs) (Harley, 1990; Roe et al., 2014). To enhance independence, braille is also employed by other vision rehabilitation specialists who support client goals, including certified orientation and mobility specialists (COMS). Braille plays a key role in orientation, mobility, and the environmental accessibility of public places, as evidenced by legislation within different jurisdictions that highlight the critical role of universal design (Alagappan et al., 2018; Jacobs et al., 2021; Lobben & Lawrence, 2012). Braille provides access to tactile maps (Lobben & Lawrence, 2012), route instructions, and signage in public places, including elevators (Mesquita & Carneiro, 2016). Although audio-based technologies provide access to information during independent travel, braille may be preferable for accessing spelling (e.g., street names) or where ambient noises and other environmental limitations pose barriers (Mack, 1984).
Although there are a number of university programs to train future O&M specialists, there remain inconsistencies in the level of braille instruction provided to future practitioners (Council, 2023). A study conducted by Penrod et al. in 2020 established that the majority of in-service O&Ms in the United States considered it necessary to learn braille as part of their training (Penrod et al., 2020). However, this study did not compare braille perceptions and practices among O&M specialists who work with different age groups, or with those practicing in Canada. As Canada requires ACVREP certification for many of their O&M specialists and the practices are similar to those in the United States, the authors recommended that future research should explore these questions in greater depth. Such findings would provide additional context to ensure that future practitioners are best equipped to meet the needs of clients across the age spectrum, including older populations. The aim of this study was to explore the perceptions of braille among O&M specialists, and the use of braille in their practice to determine whether differences exist among specialists working with children and adults. Specifically, the research questions addressed were:
What are the perceptions regarding the role of braille among O&M specialists?
Are there differences in the braille practices and perceptions among O&M specialists working with children and those working with adults?
Methods
Data were collected through an anonymous online survey hosted on the Université de Montréal Lime Survey platform between May and December 2021. Ethics approval consistent with the Declaration of Helsinki (Association, 2001) was obtained through the Centre de recherche interdisciplinaire en réadaptation du Montréal métropolitain and the Université de Montréal. Prior to commencing the survey, participants read the Information and Consent form on the initial page of the platform. Informed consent was obtained by the decision to proceed to the online survey. Participants also had the option to provide their email address for the purpose of receiving an email summary of the results (for which 34 participants did so).
Eligibility and recruitment
Participation was open to orientation and mobility specialists working in the United States or Canada aged 18 years or older and who self-reported as being fluent in English or French, to complete the questionnaire in one of these two languages, which are the official languages of the two countries studied.
Participants were recruited using three main methods:
Announcements circulated to approved vision rehabilitation agencies (the Institut Nazareth et Louis-Braille and Lethbridge-Layton Mackay vision rehabilitation centers in Montreal, Canada)
Social media networks (Facebook, X, LinkedIn) including professional groups such as TVI and O&M, O&M for children, O&M specialist groups, among others.
Snowball sampling: Participants were asked to share the questionnaire with others in their networks.
Sample size
As this was an exploratory study, no power analysis was performed. However, a sample size of n = 50 was estimated based on a similar study (Penrod et al., 2020).
Materials and procedure
The questionnaire required an average of 22 ± 3 (SD) minutes to complete and consisted of between 35 and 46 questions, divided into five sections. The number of questions answered by each participant was variable as some questions were conditional based on the participant’s response to a previous question (i.e., if participant identified with low vision, blind, or deafblind they were asked about their diagnosis and personal braille use). Data were collected through primarily closed-ended (multiple choice) questions, with the option of providing additional open-ended comments (see Supplemental appendix for the full instrument). The survey was tested for accessibility by one person with low vision and two blind individuals. Section 1 (16–22 questions) collected demographic information, including age, geographic location, and place of work. Section 2 (five–eight questions) examined current braille use and focused on the participant’s practices with braille devices. Section 3 (three–five questions) was designed to gather information about the participants’ perceptions and use of braille in O&M. Section 4 (seven questions) examined factors related to braille instruction within O&M university training. Section 5 (four questions) included open-ended questions to gather additional comments on the themes highlighted.
Data analysis
Data analysis consisted of descriptive statistics. For several questions, participants could select more than one response; thus, the total number of responses may total more than the number of participants. This is indicated in the figure and tables, where applicable.
Results
Demographics
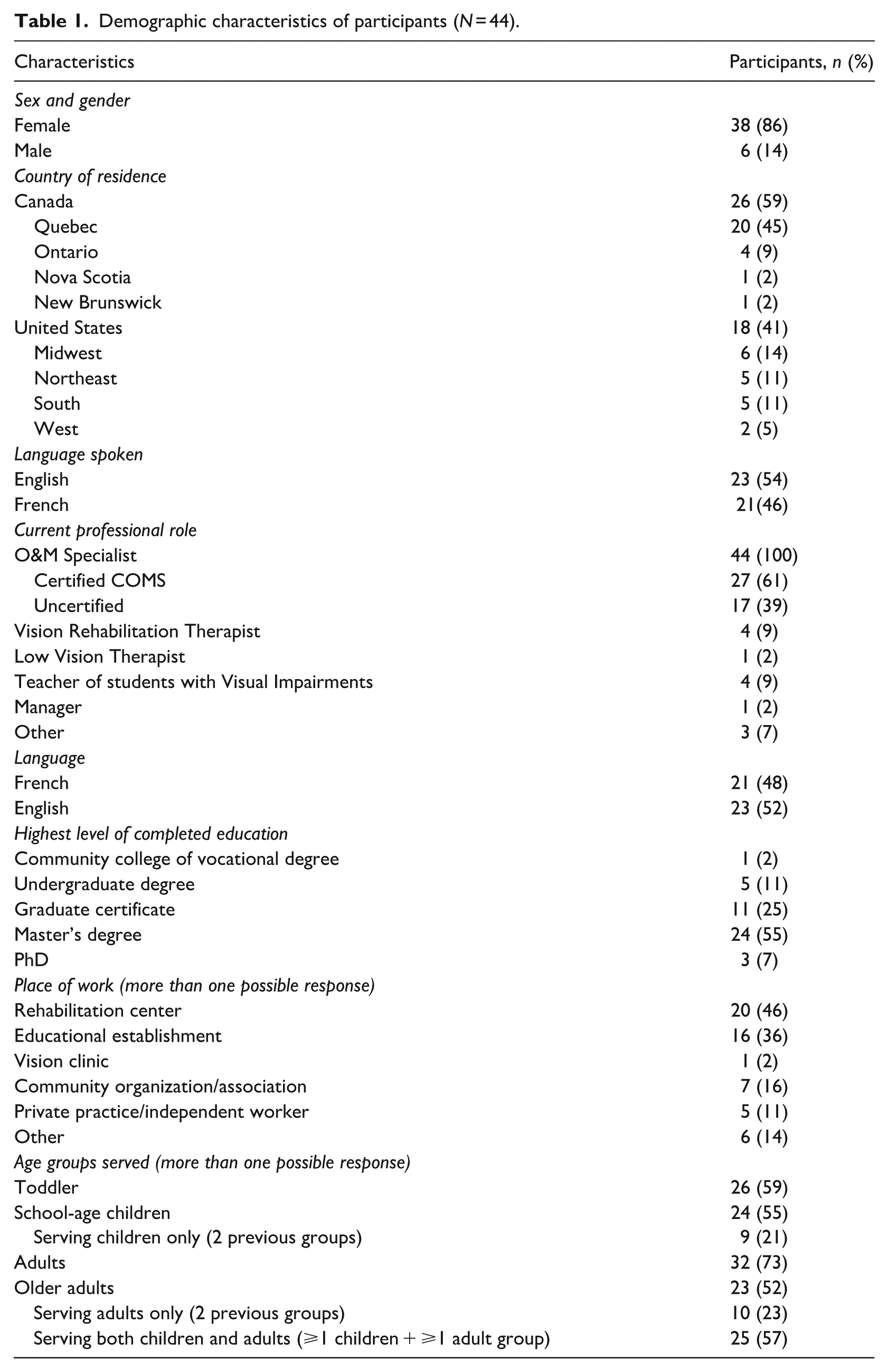
A total of 44 participants completed the questionnaire. All of them were practicing as O&M specialists in the United States or Canada. Of these, 86% were women (n = 38) and 14% men (n = 6). Forty six percent were French-speaking (n = 21) and 54% English-speaking (n = 23); 59% lived in Canada (n = 26) and 41% in the United States (n = 18). Participants’ ages ranged from 24 to 69 years old, with an average age of 46 ± 2 (SD). Participants practiced as orientation and mobility specialists for an average of 17 ± 10 (SD) years. Only one participant had a visual impairment and used braille for personal use.
To examine potential differences in braille practices among O&M specialists working with both client age groups, compared to those that exclusively work with only children or adults, the participants were subdivided into the following three groups:
Serve adults only (19+ years of age, n = 10, 23%)
Serve children only (0–18 years of age, n = 9, 20%)
Serve both age groups (0+ years of age, n = 25, 57%)
Thus, an O&M specialist that works with adults or children exclusively is classified into Group 1 or 2, respectively, but not 3. On the other hand, an O&M specialist that works with both age groups is only classified into Group 3. More detailed information about age groups served can be found in Table 1.
Demographic characteristics of participants (N = 44).
Braille use and training among O&M specialists
Half of all participants (n = 22, 50%) received braille training in their academic O&M program and half (n = 22, 50%) outside of their academic training. Of those that received it during their training, six (27%) were French-speaking, with the rest (n = 16, 73%) being English-speaking. For those that received braille outside their training, seven (32%) were French-speaking, with the rest (n = 15; 68%) being English-speaking. Most O&M specialists that received braille training in university-level O&M courses learned uncontracted braille (n = 14). Only two of the French-speaking participants that learned braille during their academic training (33%) indicated that they learned contracted braille, compared to 31% (n = 5) of the English-speaking participants who learned contracted braille. One English-speaking participant indicated only rudimentary braille knowledge. For those who received braille instruction, the most common braille tools learned during their academic training were the Perkins Brailler (n = 21, 96%) and slate and stylus (n = 18, 82%). See Table 2 for more detailed information.
Braille use and training.
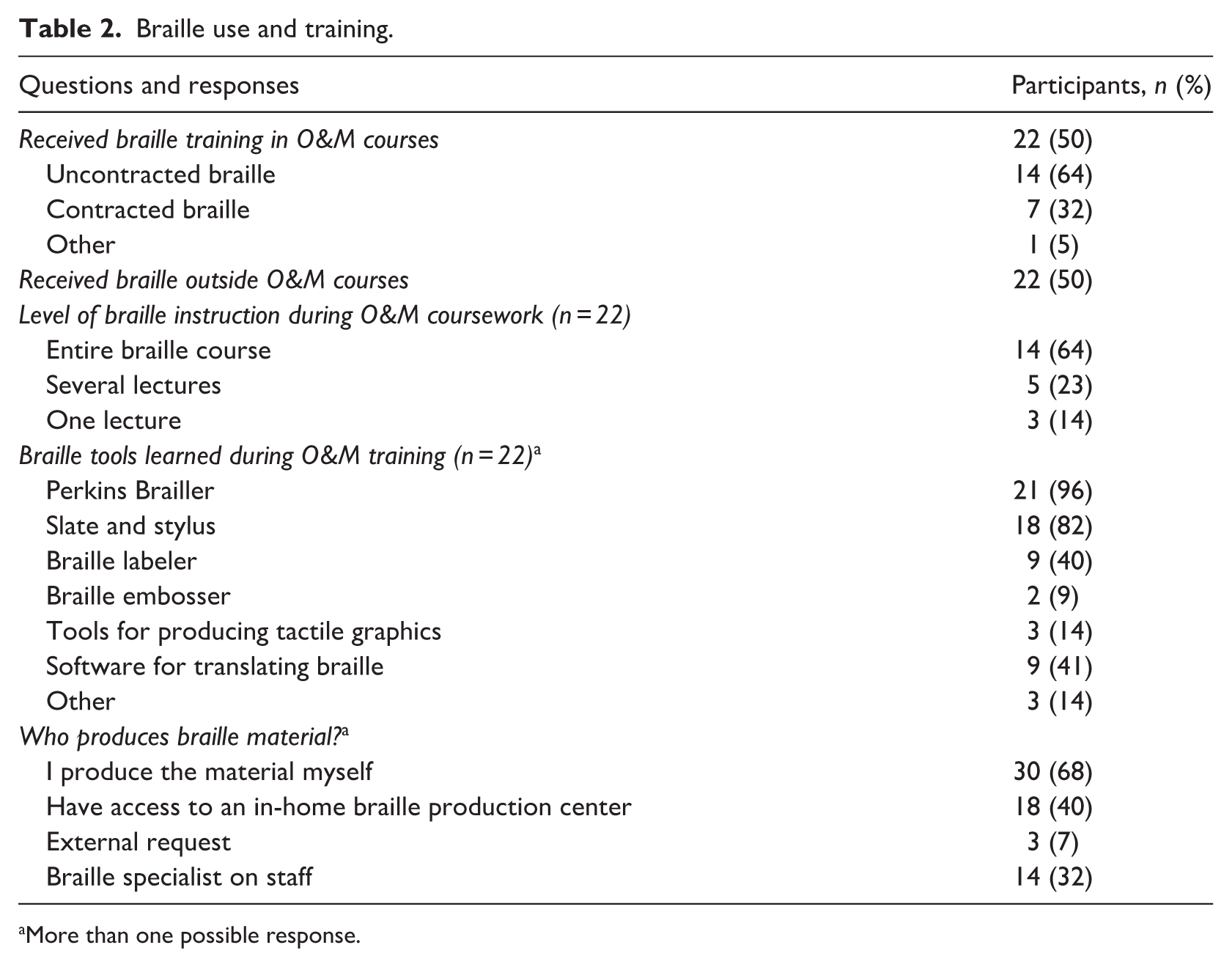
More than one possible response.
The use of braille among O&M specialists that work with children was more common than those working with adults (Figure 1(a)). For those that only work with adults, 90% (n = 9) rarely or never use braille with their clients. For the O&M specialists who only work with children, only 44% (n = 4) responded that they rarely used braille, and none responded that they never used it. Participants who work with both age groups indicated that they used braille more frequently with children clients than adults (Figure 1(a)).
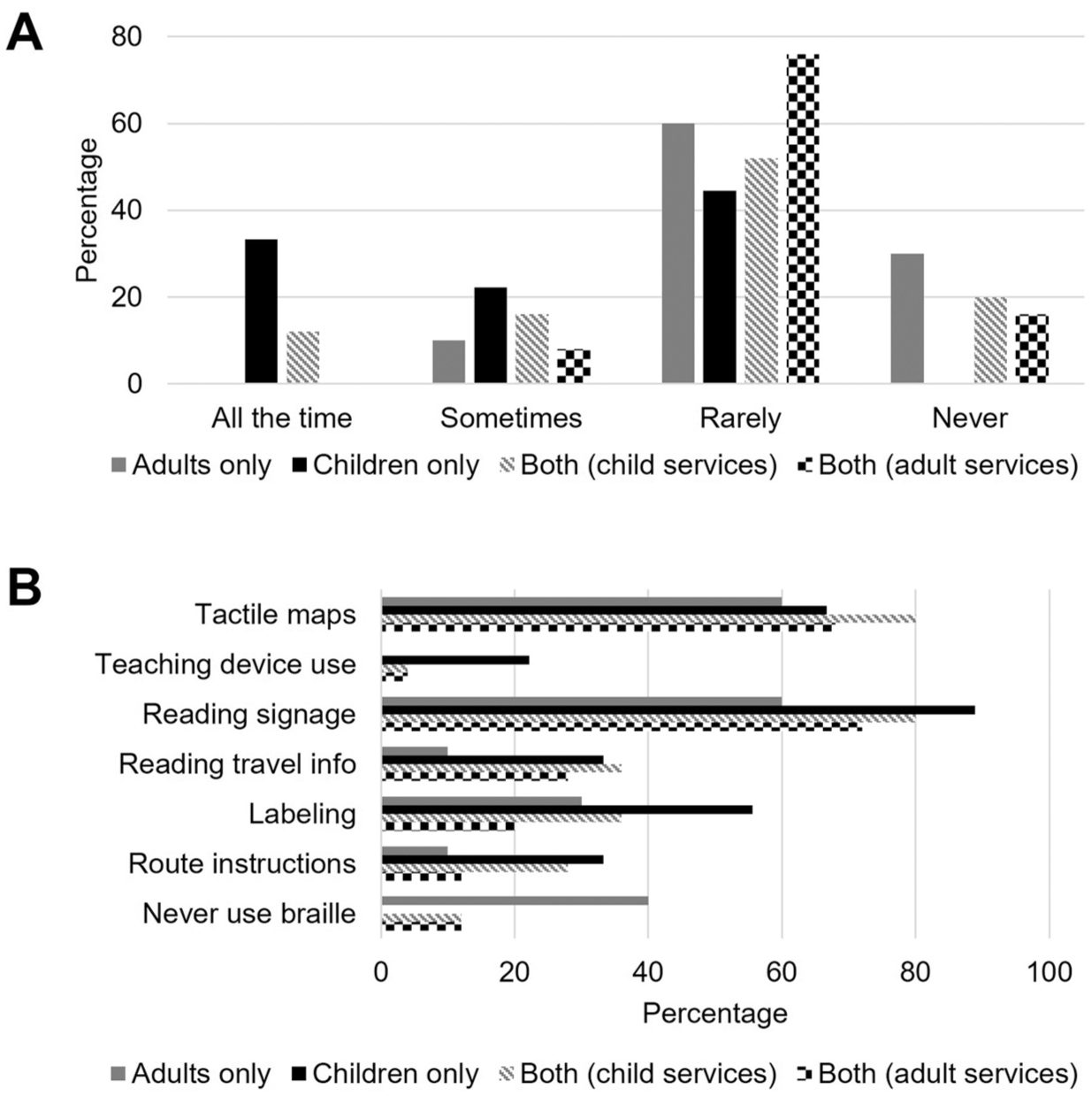
Braille use based on age group served. (a) Frequency of braille use when providing services for participants that serve adults only (gray bar, n = 10), children only (black bar, n = 9), and serve both age groups (n = 25) while serving either children (gray diagonal lines) or adults (black checkerboard). The percentage of participants for each response is represented on the y-axis. (b) Use of braille for different instructional methods for participants that serve adults only (gray bar, n = 10), children only (black bar, n = 9), and serve both age groups (n = 25) while serving either children (gray diagonal lines) or adults (black checkerboard). The percentage of participants for each instructional method is represented on the x-axis.
As seen in Figure 1(b), braille is used for more instructional methods for those working with children (Group 2) than those working with adults (Group 1). For those working with both age groups (Group 3), braille was used in more instructional methods when they worked with their younger clients. Using braille for tactile maps and reading signage was the most common across all groups. However, when working with adults (both Groups 1 and 3), most participants indicated never using braille in their practice and fewer used it for route instructions and labeling. More information can be seen in Figure 1(b). Other uses of braille include using a braille compass and transcribing O&M notes (not including route instructions) for the client. The majority of O&Ms produce braille material themselves (n = 30, 68%). More detailed information can be found in Table 2.
Perceptions of braille among O&M specialists
As seen in Table 3, many O&M specialists feel confident identifying whether their clients would benefit from braille in O&M, with only 32% (n = 14) indicating that they are less than confident in recognizing this need. Participants generally know where to refer a client, with n = 42 (95%) reporting “yes” and only 1 person reporting “no,” and 1 “unsure.” Slightly more than half of participants reported that they can only respond to simple braille requests (n = 23, 52%). However, O&M specialists working only with children are more likely to report that they can respond to any braille requests (n = 5, 56%), with this group including 3 TVIs.
Perceptions of braille.
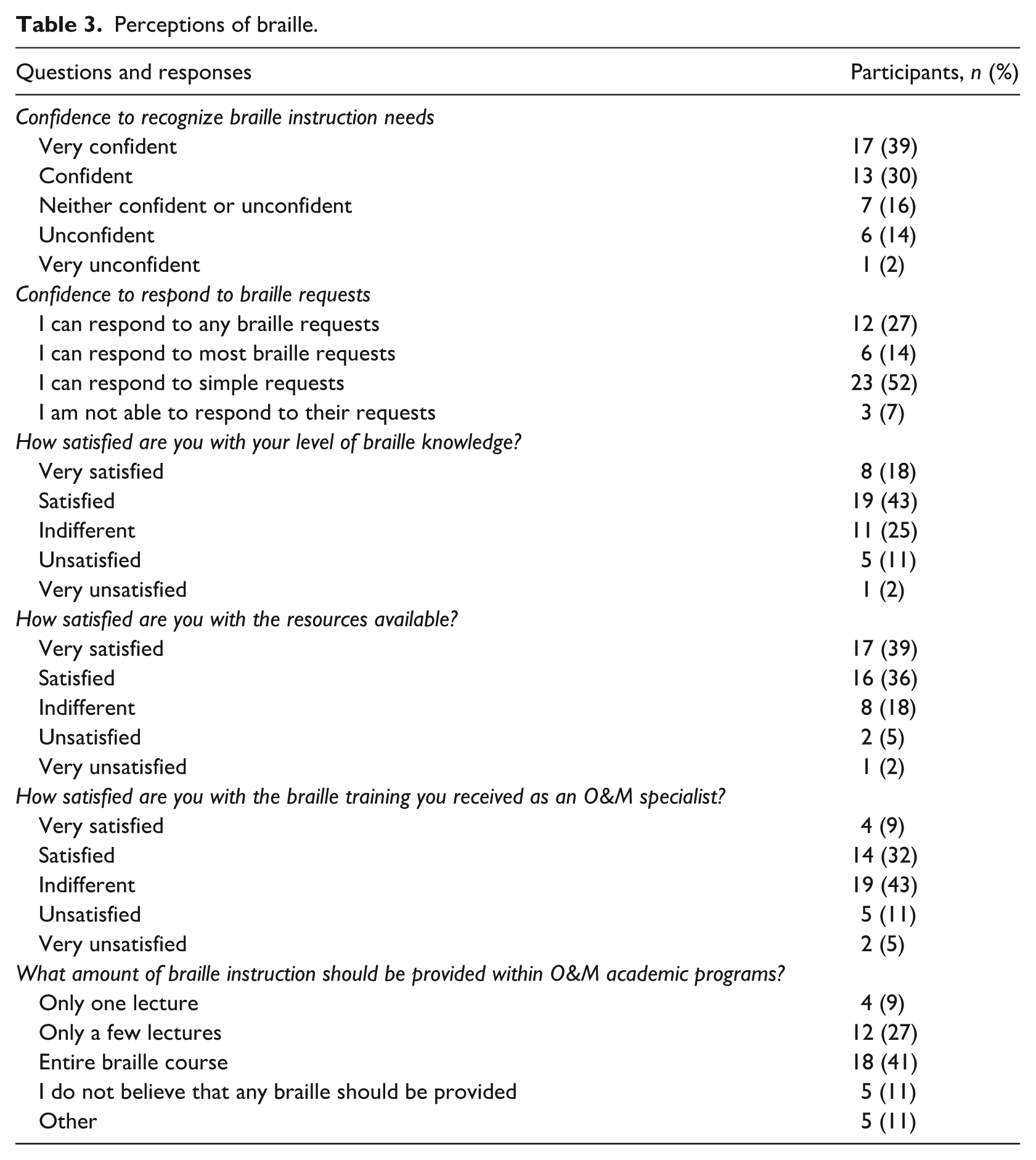
Overall, 39% of participants (n = 17) were not satisfied with their level of braille knowledge, but were more satisfied with the resources available at their place of work to respond to braille requests of clients (n = 33, 75% satisfied or very satisfied). Overall, a majority, 59% (n = 26) were either indifferent or not satisfied with the level of academic training received. This included 19 (43%) that were indifferent, 5 (11%) that were unsatisfied, and 2 (5%) that were very unsatisfied. However, this differed among O&M specialists working with different age groups. Eighty-nine percent (n = 8) of O&M specialists working with children exclusively were either satisfied or very satisfied with their braille training received. This is compared to 40% (n = 4) of those working with adults only and 60% (n = 15) of those working with both age groups.
Interestingly, only 25% (n = 11) of all participants feel that they require additional training and most expressed that they know where to go for this training (80%, n = 35). No participants stated that braille training should only be available to those serving children or adults, with the majority (66%, n = 29) responding that it should be available to all O&Ms regardless of age group. Only 18% (n = 8) mentioned that it should not be required at all, and another 7 with “other” responses. Some “other” responses included that the specialist should be a dual certified TVI, and that O&M specialists should be sensitized about braille tools and resources. The most common amount of braille instruction recommended by participants was an entire braille course (n = 18, 41%) or a few lectures (n = 12, 27%). Uncontracted braille was the level considered to be the most helpful for O&M specialists as reported by 55% (n = 24) participants with 25% (n = 11) indicating contracted braille and 20% responding they don’t know (n = 9). These responses were consistent across all groups. However, almost half (n = 4, 44%) of those working exclusively with children preferred contracted braille. Over half (55%, n = 24) of participants believe it should be a requirement for O&M professional certification, while 43% (n = 19) do not, and one gave an “other” response, stating “they should be dual certified.” More detailed information about the perceptions of O&M specialists can be found in Table 3.
Discussion
Braille is an integral part of rehabilitation for many individuals who are blind. It is important to understand what services are being offered and the level of training that children and adults with visual impairments receive over their lifespan. The aim of this study was to explore perception of braille among O&M specialists, and the use of braille in their practice. This study also sought to determine whether there is a difference between the use of braille among specialists working with children (0–18 yo), and those working with adults (19+ yo). This study found that level of braille knowledge differs among O&M specialists who work with children compared to those who work with adults.
Perceptions in braille training
These results demonstrate that overall braille is used as part of orientation and mobility services and is considered an important element of training. Most O&M specialists feel that braille training is necessary to help clients achieve various goals, regardless of their age group. These results confirm those established by Penrod et al. in 2020: the majority of O&M specialists consider braille to be important to their practice. However, depending on the clientele served, practices and perceptions regarding braille differ.
A majority of O&M specialists who work with adults rarely or never use braille for O&M instruction. Likewise, those serving children are more satisfied with their level of braille knowledge and feel more confident about their ability to respond to braille requests. This may be due to the fact that O&M specialists who work with children are more likely to be dual trained as TVIs and O&M specialists, as was seen in this study. While most participants lean toward learning uncontracted braille, those working with children highlight that contracted braille is more appropriate. Research has suggested that instructors less experienced in the use of braille tend to use it less (Ponchillia & Durant, 1995). This highlights the importance of ensuring that professionals who serve adults are competent in contracted braille, to meet these O&M needs when they arise. Many participants perceive themselves as less able to meet these needs. On the other hand, participants generally feel well able to recognize potential braille needs in their clients. Participants sometimes report turning to colleague braille instructors (e.g., CVRT) when they find braille training beyond their competency.
None of the O&M specialists that responded to the survey suggested that braille training should only be provided to O&M specialists who work with a specific age group. However, there is a recognized difference in the perceived level of braille training needed when working with these two age groups. Overall, those working with children use it more, consider it more useful, and are less satisfied with their training than their colleagues working with adults. Those working with children were also more likely to support more advanced braille training for O&M specialists and that this training should last from a few courses to a full session. In this study, contracted braille is also more used among O&M specialists working with children than those working with adults.
Use of braille when instructing adults and children
The percentage of professionals who rarely or never use braille during O&M training was higher among those working with adults, particularly if exclusively working with this population. It could be suggested that this is due to the perception that adults already have the competencies needed to integrate braille into O&M without additional support. Another possible explanation for the less extensive use of braille with adults could be that this clientele receive braille training from a CVRT in conjunction with O&M services. Based on our data in this study, it is likely that the O&M specialists working with adults felt less competent in supporting the use of braille themselves, as they favor additional professional training to further develop their braille competencies.
Interestingly, for O&M specialists working with both children and adults, both tactile maps and reading signage were the most common uses. Nevertheless, it is worth noting that O&M professionals in this study teach the use of route instruction and labeling more often with children. This may be due to the fact that adult braille users already come with these braille skills and can incorporate it more readily into O&M goals without the same level of instruction required. Moreover, adult braille learners may use braille to support specific objectives (e.g., reading the keypad on their building’s elevator) (Chan, 2010). Adults, especially those with acquired visual impairment (Dalby et al., 2009), may be more likely to use a wide range of methods, including braille and smartphone applications to identify the objects around them. Even when learned as an adult, learning braille generates higher self-esteem, a better quality of life, and more chances of getting a job (Silverman & Bell, 2018).
Implications for practice
Though O&M specialists in this study are generally satisfied with the braille resources available for their practice, they would like to have more braille courses included in university O&M training programs. These findings highlight that it is important to examine the academic structure of O&M programs due to the large percentage of O&M specialists surveyed who indicated that they did not receive sufficient training in braille. Findings also highlight the importance of enhancing the level of braille training provided to O&M specialists who work primarily with adults. Since they perceive that fewer of their clients have knowledge of braille and they rarely or never use it in their practice, their braille competency may be diminished over the course of their career. Though they could refer clients to a CVRT to improve their level of braille, O&M specialists will still be confronted with a lack of braille competency when providing instruction while traveling in public spaces with clients. The authors suggest that continuing education should be provided to O&M specialists currently employed to learn or update their current braille knowledge. This instruction should not exclusively be provided by CVRTs working in rehabilitation centers, because many O&M service providers do not have these specialists available. A discussion between the academic programs and O&M service providers could elucidate the most appropriate means for O&M specialists to provide basic services in braille to their clientele of all ages.
Conclusion
Braille remains a critical skill for individuals with visual impairments. To support braille goals across activities of daily living, it is essential that practitioners from across the rehabilitation team are equipped with the tools to support braille-related goals. This study highlights the need to better ensure that O&M specialists who serve adults are provided with greater opportunities to develop their braille competencies within the context of their university training program.
Limitations
As to not target any specific O&M program, participants were not asked which university they attended. In addition, this survey did not directly ask participants about the level of braille knowledge of their clientele; thus, it is possible that this may influence their perceptions about braille training. It should be mentioned that the caseload of each specialist may differ, which was not examined in this study, thus the frequency of braille use by each specialist may differ accordingly. As O&M training programs have been modified over recent years, it is likely that the more experienced O&M specialists in this study who were surveyed may lack the braille training that may now be offered to students currently enrolled in university O&M programs.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196251409315 – Supplemental material for Exploring braille practices and perceptions among orientation and mobility specialists working with different age groups
Supplemental material, sj-docx-1-jvi-10.1177_02646196251409315 for Exploring braille practices and perceptions among orientation and mobility specialists working with different age groups by Joseph Paul Nemargut, Natalina Martiniello and Marie Mansour in British Journal of Visual Impairment
Footnotes
Data availability
The data can be made available upon request by contacting the corresponding author.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval consistent with the Declaration of Helsinki was obtained through the Université de Montréal (2021-1172) and the Centre de recherche interdisciplinaire en readaptation du Montréal métropolitain (MP-50-2022-966).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.