
Abstract
Children and adolescents with visual impairments (VIs) often face challenges in developing social-emotional skills (SESs) and rely on compensatory strategies. Assessing and teaching SESs are crucial; however, Swiss practitioners lack suitable tools. This study used the French version of the Social Skills Improvement System Social-Emotional Learning Edition Rating Forms (SSIS-SEL RFs) to collect data on perceptions of SESs from students (self-assessment), parents, and teachers in a sample of 43 children and adolescents with VI. Although comparisons with normative sample data showed no significant differences at the group level, individual analysis revealed a wide range of profiles, with a substantial proportion of children scoring well below or well above the average. According to parent-reported scores, students with mild VI had significantly higher SESs than those with moderate VI to blindness, particularly in the domains of social awareness and relationship skills. In addition, higher SES scores were reported for older participants, girls, and those involved in inclusion-based activities. These results highlight the importance of detailed evaluation across different domains of SESs to guide individualized teaching and suggest the use of the SSIS-SEL RFs as part of a comprehensive assessment approach.
Keywords
Introduction
Social-emotional skills (SESs) are essential for effective social interactions and building friendships (Smith & Hart, 2022). Scientific literature indicates that children and adolescents with visual impairments (VIs) may face difficulties in developing these skills (Pérez Pereira & Conti-Ramsden, 2020; Roe & Webster, 2002). Accordingly, specialized curricula emphasize the importance of assessing and explicitly teaching SESs to this population (Allman & Lewis, 2014; Hewett et al., 2022). However, in Switzerland, recent research suggests that practitioners still lack adequate tools to evaluate SESs (Barras et al., 2023).
SESs involve processing social information (e.g., recognizing the emotions of others) and adapting behaviours for effective interactions across contexts (e.g., in class with peers and teachers or at home with parents; Beauchamp & Anderson, 2010). These skills develop as a result of environmental influences and the maturation of the sensory system (e.g., gaze tracking), motor system (e.g., triadic interactions), and socio-cognitive system (e.g., theory of mind; Fernyhough, 2008; Soto-Icaza et al., 2015). Sighted children and adolescents with typical development primarily acquire SESs through observation and imitation in emotionally meaningful interactions – a process supported by the visual and socio-cognitive systems, with cultural tools (e.g., language, symbols, and signs) serving as mediators (Bøttcher & Dammeyer, 2016; Vygotsky et al., 1997).
Children and adolescents with VI often encounter difficulties in developing SESs due to limited access to visual cues (e.g., facial expressions, gestures) and challenging environments (e.g., noisy classrooms that hinder auditory emotion recognition), leading them to rely on compensatory strategies (e.g., understanding others’ emotions by listening to tone of voice; Pérez Pereira & Conti-Ramsden, 2020). In childhood, difficulties may arise in joint attention (Bigelow, 2003; Tadić et al., 2009; Urqueta Alfaro et al., 2018), emotion recognition (Dyck et al., 2004; Minter et al., 1991), emotion regulation (Chennaz et al., 2022), and theory of mind (Brambring & Asbrock, 2010; Green et al., 2004); however, these challenges often decrease with age (Peterson et al., 2000). Other sensory modalities, such as auditory and kinaesthetic cues (e.g., sound variations, air currents, echolocation) may support joint attention and emotion recognition (Battich et al., 2020). Stereotypical behaviours, including self-stimulatory movements (Molloy & Rowe, 2011), may help regulate emotions and gather environmental information (Galiano et al., 2024; Molinaro et al., 2020; Pérez Pereira & Conti-Ramsden, 2020). Caregivers must understand these behaviours and compensatory strategies (e.g., recognizing that stillness may indicate interest and attention to a stimulus rather than disengagement; van Eijden et al., 2023). In school-age children, challenges in peer interactions (Runjić et al., 2015), pragmatic communication (James & Stojanovik, 2007; Pijnacker et al., 2012), and social problem-solving (McAlpine & Moore, 1995) may lead to reduced social networks and increased loneliness in adolescence (Huurre & Aro, 2000; Kroksmark & Nordell, 2001). Support from caregivers should foster positive social experiences and provide scaffolding without over-supporting (Roe, 2019). Given the emphasis on SESs in the Expanded Core Curriculum (ECC; Allman & Lewis, 2014) and in the Curriculum Framework for Children and Young People with Vision Impairment (CFVI; Hewett et al., 2022), explicit SESs teaching is both recommended and effective (Caron et al., 2023; Sacks & Page, 2017).
Before explicit teaching, assessment is crucial and can be conducted through various methods, including direct observation, behaviour rating scales, semi-structured interviews, sociometric assessments, and problem-solving scenarios (Whitcomb, 2018). Behaviour rating scales are valued for their time efficiency and ease of use by multiple observers, even though they capture perceptions rather than direct observations (Whitcomb, 2018). Commonly used in VI research (Birch et al., 2007; Chennaz et al., 2022; de Boer et al., 2004), they have been applied in several studies to assess SESs in population with VI (Buhrow et al., 1998; Huurre & Aro, 1998; Lang et al., 2017; Matson et al., 1986; Ozkubat & Ozdemir, 2014; Salleh et al., 2011; Zebehazy & Smith, 2011). Findings indicated that, on average, school-aged students with VI exhibit significantly lower SES levels than their sighted peers (Buhrow et al., 1998; Ozkubat & Ozdemir, 2014; Salleh et al., 2011). These challenges are also observed in early childhood (Lang et al., 2017) and persist into adolescence (Huurre & Aro, 1998).
Regarding behaviour rating scales, due to the lack of standardized tools for this population, Sacks (2014) recommends considering standardized SES behaviour rating scales designed for the general population. In a systematic review, Cordier et al. (2015) highlighted the Social Skills Improvement System Social-Emotional Learning Edition Rating Forms (SSIS-SEL RFs; Gresham & Elliott, 2017) as a tool with robust psychometric properties. This tool is structured around the Collaborative for Academic Social and Emotional Learning (CASEL, 2020) framework for social-emotional learning (SEL; Durlak et al., 2015). This framework outlines five key SEL domains (CASEL, 2020): Self-awareness (e.g., understanding one’s own emotions, thoughts, and behaviour), self-management (e.g., regulating emotions, thoughts, and behaviours), social awareness (e.g., empathizing with others and understanding diverse perspectives), relationship skills (e.g., building and maintaining supportive relationships), and responsible decision-making (e.g., making thoughtful and ethical choices). The SEL frameworks enable the identification of individual SES profiles and support both the assessment and teaching of these skills (CASEL, 2020).
To gain a detailed understanding of the strengths and challenges in SESs of children and adolescents with VI, the scientific literature requires stronger empirical evidence based on standardized assessment tools. Furthermore, a recent study conducted in the Swiss context highlighted a general willingness among teachers of students with VI (TVIs) to teach SESs. However, it also revealed a significant lack of training in teaching these skills, as well as limited awareness of appropriate assessment tools for evaluating them effectively (Barras et al., 2023).
To address this gap, the present study employs the French version of the SSIS-SEL RFs (Elliott & Gresham, 2021; Gresham & Elliott, 2017) to determine the SES profiles of children and adolescents with VI attending mainstream schools in Switzerland. Specifically, this behaviour rating scale was used to collect data on SESs perceptions from students (self-assessment), parents, and teachers, based on a sample of 43 children and adolescents with VI. Although not specifically designed for this population, the tool’s strong reliability and validity support its use and may guide future development of tools tailored to this population’s needs. The findings could inform educational policy and practice by identifying support needs and guiding SEL integration into the Swiss curriculum (Conférénce Intercantonale de l’Instruction Publique de la Suisse Romande et du Tessin, 2010). The data further allowed for an exploration of whether SES perceptions vary with the severity of VI and sociodemographic factors such as age, gender, and participation in inclusive activities. In addition, comparing the perspectives of students, parents, and teachers may help to identify differences in how SESs are perceived across home and school settings. Based on these aims, the main research questions were as follows:
RQ1. Do the perceptions of SESs of children and adolescents with VI differ from those in the general population?
RQ2. Do students, parents, and teachers hold differing perceptions of SESs of children and adolescents with VI?
RQ3. Do the perceptions of SESs of children and adolescents with VI vary according to the severity of VI and sociodemographic factors (such as gender, age, and participation in inclusive extracurricular activities and sport)?
Method
Sample population
A total of 43 children and adolescents with VI were recruited from mobile services associated with the Educational Centre for the Visually Impaired (Centre Pédagogique pour Handicapés de la Vue, CPHV) in Lausanne, Switzerland (CPHV, 2025). The inclusion and exclusion criteria were as follows: individuals aged 3 to 18 years old and who met the International Classification of Diseases (ICD-11) definition of VI (World Health Organization, 2022). Children and adolescents with additional difficulties, such as specific learning disabilities (SLDs), attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), and developmental speech or language disorders (DLD), were eligible, as they attend mainstream educational settings either fully or partially. However, children with intellectual and developmental disabilities (IDD) were not included in the study, as they are most often enrolled in the specialized school affiliated with the CPHV and do not share the same educational context as the rest of the sample.
The age range of the participants was 3.5–18.6 years (M = 10.84; SD = 4.49), and the sample showed a balanced gender distribution (23 girls and 20 boys). VI severity was classified as mild (N = 18), moderate (N = 10), severe (N = 3), blindness (1; N = 1), and blindness (3; N = 1), according to the ICD-11 classification (World Health Organization, 2022). Most participants attended mainstream school exclusively (N = 32), whereas the remainder were enrolled in both mainstream and special school settings (N = 8). All sociodemographic data are presented in Table 1.
Sociodemographic data of the study sample.
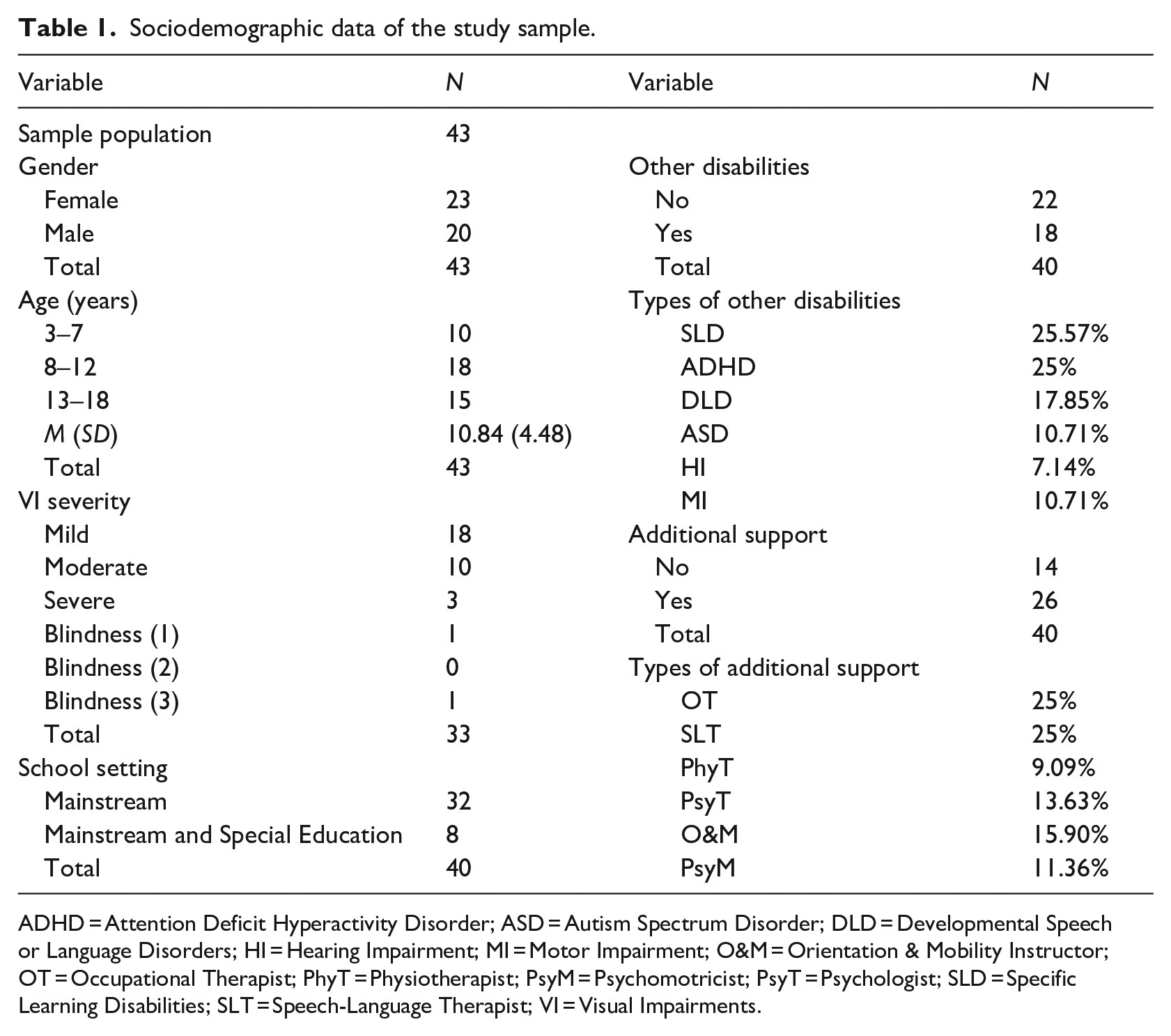
ADHD = Attention Deficit Hyperactivity Disorder; ASD = Autism Spectrum Disorder; DLD = Developmental Speech or Language Disorders; HI = Hearing Impairment; MI = Motor Impairment; O&M = Orientation & Mobility Instructor; OT = Occupational Therapist; PhyT = Physiotherapist; PsyM = Psychomotricist; PsyT = Psychologist; SLD = Specific Learning Disabilities; SLT = Speech-Language Therapist; VI = Visual Impairments.
Instruments
SES data were collected using the French version of the SSIS-SEL RFs (Elliott & Gresham, 2021; Gresham & Elliott, 2017). This tool is based on a well-established SES assessment framework (Gresham & Elliott, 1990, 2008) and includes multi-respondent questionnaires for students (for ages 8–12 and 13–18 years; 46 items), parents (for ages 3–7, 8–12, and 13–18 years; 51 items), and teachers (for ages 3–7, 8–12, and 13–18 years; 51 items). Responses are rated on a 4-point Likert-type scale (from 0 = never true to 3 = almost always true). The French version was standardized on a representative sample of 638 children and adolescents from France and Belgium, demonstrating strong psychometric properties: internal consistency (α = .68 to .97), test–retest reliability (corrected r = .73 to .91), and inter-rater reliability (corrected r = .60 to .65) (Elliott & Gresham, 2021). The tool provides standardized ‘SES total scores’ and ‘SEL domains scores’ (M = 100; SD = 15). Scores of 70–85 indicate ‘below average’, whereas those below 70 are ‘well below average’. In addition, a response pattern index signifies response tendencies. A low index suggests repeated selection of the same response (students: 0–5; parents: 0–13; teachers: 0–12), whereas a high index denotes a cyclic pattern (students: 42–45; parents: 42–50; teachers: 42–50). A midrange index indicates an acceptable response pattern (students: 6–41; parents: 14–41; teachers: 13–41). As a practice-oriented tool, the SSIS-SEL RFs identify specific ‘SEL domains scores’ where children or adolescents have difficulties, guiding targeted interventions (Elliott & Gresham, 2021).
Moreover, a sociodemographic questionnaire was administered to collect data on gender, age, VI severity, school setting, additional disabilities or support, and participation in inclusive sports and extracurricular activities.
Data collection and analysis
The research project was first approved by the Ethics Committee of the Canton of Vaud. 1 Before data collection, the project was presented to TVIs, who acted as intermediaries between the researchers and respondents (students, parents, and mainstream school teachers) who assessed the SESs of children and adolescents in the sample. With the help of TVIs, parents of children under 14 years of age were contacted and provided with information sheets about the study. Written consent was obtained from the parents to allow their children’s participation. Adolescents aged 14–18 years provided consent independently. A total of 68 consent forms were distributed, and 51 were returned. Data collection began after consent was obtained.
For data collection, the questionnaires were distributed via email and completed on online platforms compatible with screen reading technologies for people with VI. First, a sociodemographic questionnaire was created and administered through LimeSurvey (LimeSurvey GmbH, 2025). For children under 14 years of age, this questionnaire was completed by parents; adolescents aged 14–18 years completed it either independently or with assistance from TVIs. Second, the French version of the SSIS-SEL RFs (Elliott & Gresham, 2021) was administered through Q-global (Pearson Clinical, 2025). The student version (for ages 8–12 and 13–18 years) was completed by children and adolescents with VI, with help from their TVIs if necessary. The parent version (for ages 3–5, 5–12, and 13–18 years) was completed by parents, and the teacher version (for ages 3–5, 5–12, and 13–18 years) was completed by mainstream school teachers who had the most interaction with the students with VI.
In total, questionnaires were distributed to the 51 participants who provided written consent, and responses were received for 43 children and adolescents. To be included in the study, at least one completed questionnaire was required per participant. However, responses from all three sources (students, parents and teachers) were not obtained for all 43 children and adolescents. In total, responses were obtained from 25 students, 35 parents, and 27 teachers. A detailed breakdown of respondents per child and adolescent with VI is provided in Figure 1.
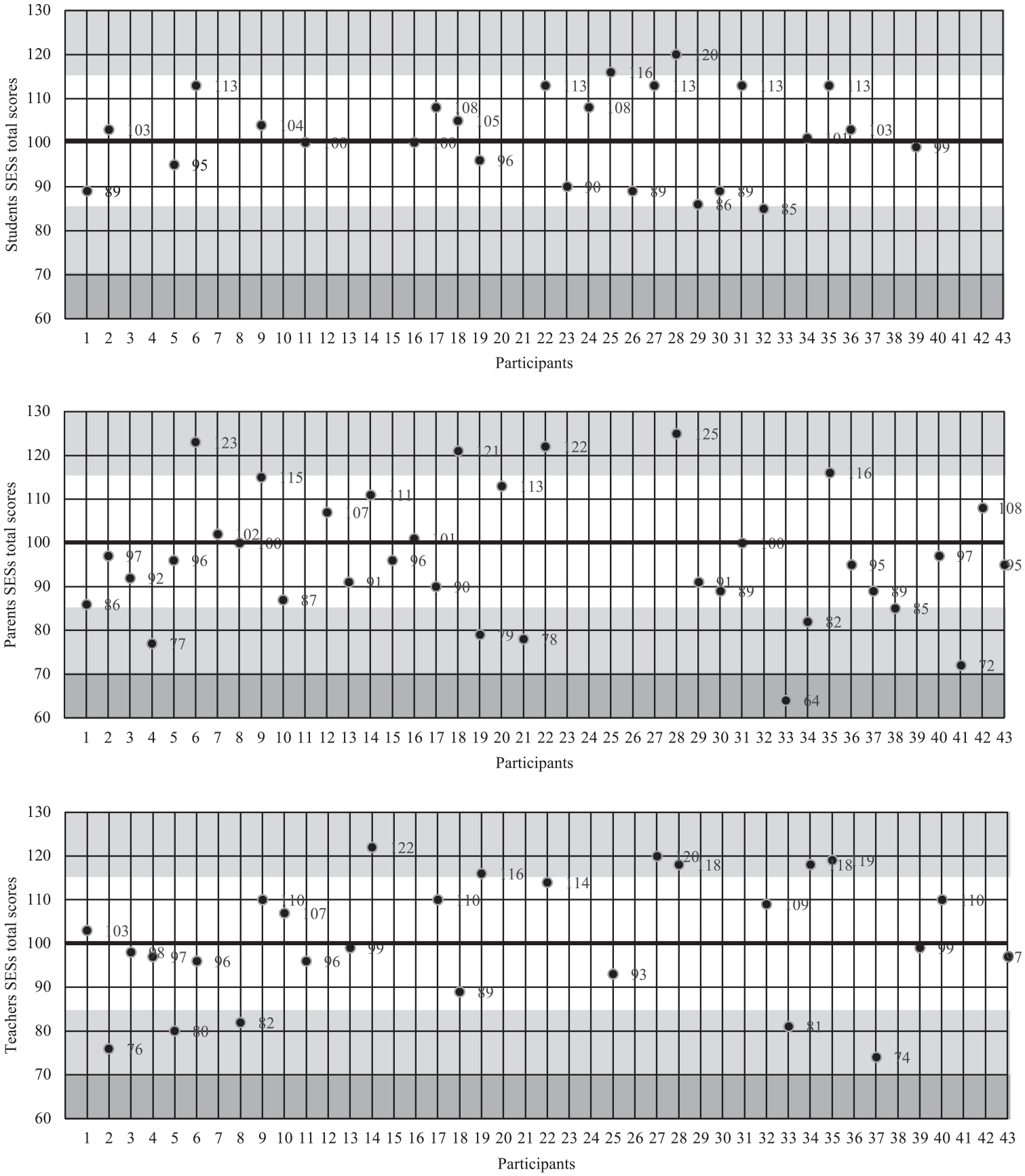
SES total scores from SSIS-SEL RFs.
For data analysis, responses from the sociodemographic questionnaire and the French version of the SSIS-SEL RFs were anonymized and analysed using SPSS software.
Results
The French version of the SSIS-SEL RFs (Elliott & Gresham, 2021), completed by students (self-assessment), parents, and mainstream school teachers, was used to collect data on perceptions of SESs in a sample of 43 children and adolescents with VI. The findings, in combination with the sociodemographic data, address the main research questions.
Do the perceptions of SESs of children and adolescents with VI differ from those in the general population?
Responses were obtained from 25 students, 35 parents, and 27 teachers on a sample of 43 children and adolescents with VI. The response pattern index indicated acceptable consistency across all respondents: students (scores ranging from 17 to 38), parents (scores ranging from 20 to 39), and teachers (scores ranging from 21 to 39). The results, including ‘SES total scores’ and ‘SEL domains scores’ (Self-Awareness, Self-Management, Social Awareness, Relationship Skills and Responsible Decision-Making), are displayed in Table 2.
Means and standard deviation scores from SSIS-SEL RFs.
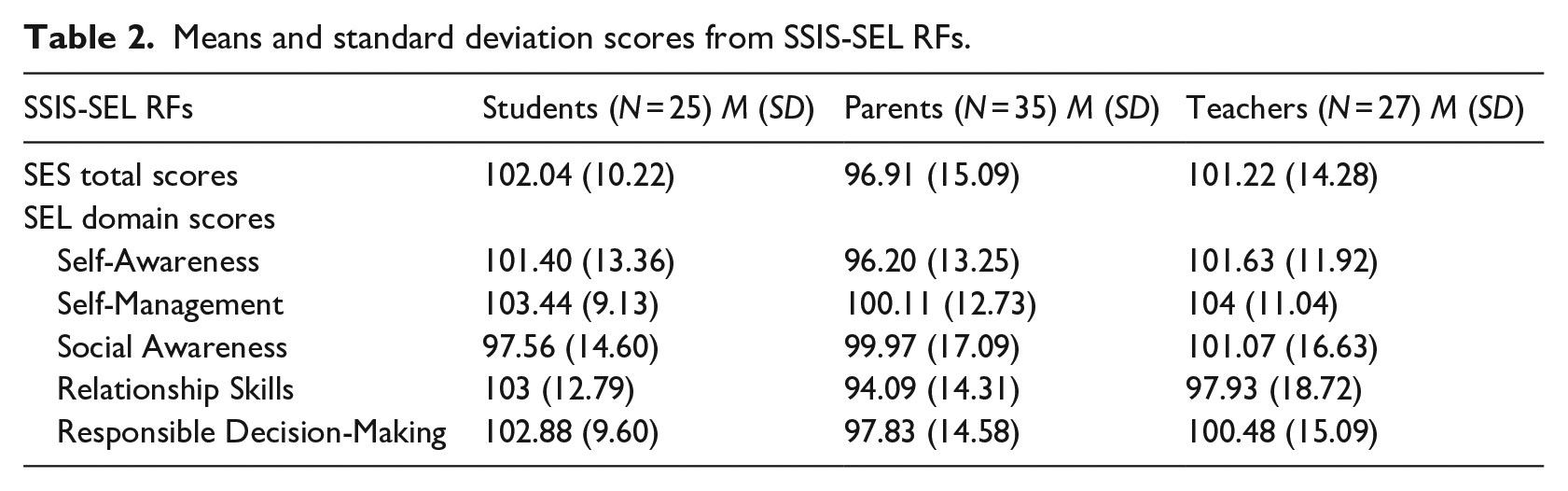
A single-sample t-test revealed no significant differences between the average ‘SES total scores’ of the sample and the test value of 100, the average score of the general population. For students (N = 25; M = 102.04; SD = 10.22), the test result was t(24) = 0.997, p = .32. For parents (N = 35; M = 96.91; SD = 15.09), the test result was t(34) = −1.209, p = .23. For teachers (N = 27; M = 101.22; SD = 14.28), the test result was t(26) = 0.445, p = .66. These results, based on assessments from all three respondent groups in this study sample, indicate that the perceived SESs of children and adolescents with VI did not differ significantly on average from those of the general population.
An analysis of individual scores (see Figure 1) further refined these results. The graphs show that scores generally align with those of the general population. From the children and adolescents’ perspective (first graph), none of the 25 participants scored ‘below average’ (<85) or ‘well above average’ (>130). From the parents’ perspective (second graph), six out of 35 participants (17.14%) were classified as ‘below average’ (<85), with one participant scoring ‘well below average’ (<70) and five participants (14.29%) scoring ‘above average’ (>115). From the teachers’ perspective (third graph), five out of 27 participants (18.52%) fell within the ‘below average’ range (<85), whereas six participants (22.22%) were classified as ‘above average’ (>115).
Do students, parents, and teachers hold differing perceptions of SESs of children and adolescents with VI?
Correlation analysis was performed for children and adolescents with VI who had data from both sources (N = 17 for student-parent and student-teacher; N = 22 for parent-teacher). A strong positive correlation was found between ‘SES total scores’ reported by students and parents, r(15) = 0.727, p < .001. However, no significant correlations were observed between student and teacher ratings, r(15) = 0.223, p = .39, or between teacher and parent ratings, r(20) = 0.275, p = .21. These results suggest that students and parents share more similar perceptions of SESs, whereas teachers’ assessments differ.
Do the perceptions of SESs of children and adolescents with VI vary according to the severity of VI and sociodemographic factors (such as gender, age, and participation in inclusive extracurricular activities and sport)?
Regarding the severity of VI, participants were divided into two groups: ‘mild VI’ (N = 18) and ‘moderate VI to blindness’ (N = 15). Figure 2 shows the overall ‘SES total scores’ reported by students, parents, and teachers for both groups.
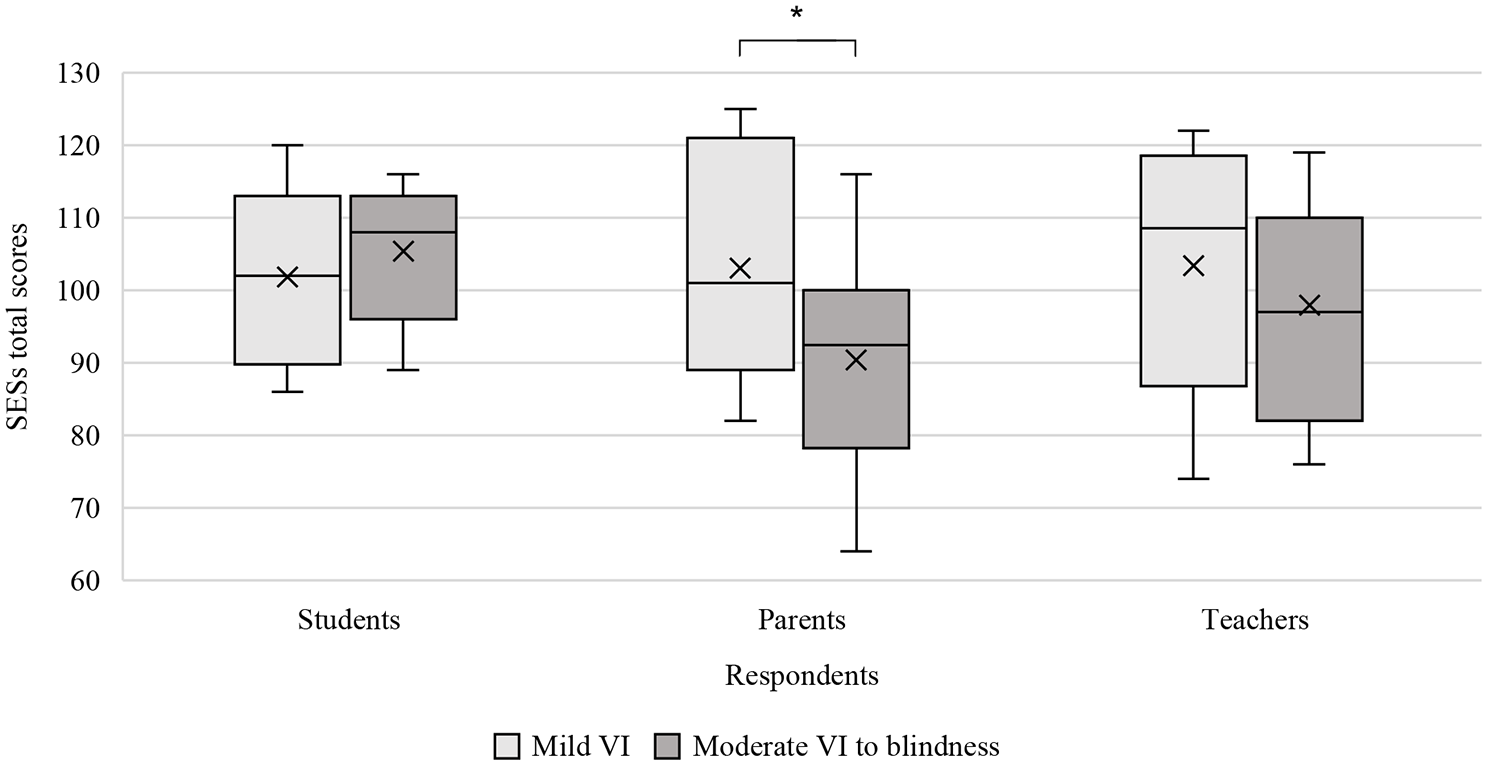
Variation in ‘SES total scores’ reported by three respondents according to severity of VI.
Independent samples t-tests compared the ‘SES total scores’ between children and adolescents with ‘mild VI’ and those with ‘moderate VI to blindness’. Parents reported significantly higher ‘SES total scores’ for the ‘mild VI’ group (N = 15, M = 103.07, SD = 14.77) than for the ‘moderate VI to blindness’ group (N = 12, M = 90.42, SD = 14.17), t(25) = 2.250, p < .05. No significant differences were found for students (‘mild VI’: N = 14, M = 101.79, SD = 10.82; ‘moderate VI to blindness’: N = 8, M = 104.63, SD = 9.51), t(20) = −0.617, p = .27, or for teachers (‘mild VI’: N = 10, M = 103.40, SD = 17.74; ‘moderate VI to blindness’: N = 11, M = 97.91, SD = 14.30), t(19) = 0.784, p = .22. Further analysis of the ‘SEL domains scores’ using independent samples t-tests revealed that parents rated the ‘mild VI’ group significantly higher than the ‘moderate VI to blindness’ group regarding Social Awareness (‘mild VI’: N = 15, M = 108.27, SD = 16.00; ‘moderate VI to blindness’: N = 12, M = 90.08, SD = 16.93), t(25) = 2.860, p < .05, and Relationship Skills (‘mild VI’: N = 15, M = 99.27, SD = 12.76; ‘moderate VI to blindness’: N = 12, M = 89.50, SD = 14.49), t(25) = 1.861, p < .05. No significant differences were found in other ‘SEL domains scores’ given by parents, teachers, or students. These findings suggest that parents perceive children and adolescents with ‘mild VI’ as having better Social Awareness and Relationship Skills compared to those with ‘moderate VI to blindness’.
Additional analyses were conducted on sociodemographic factors, including gender, age, and participation in inclusive sports and extracurricular activities. Regarding gender, independent samples t-tests were used to compare the ‘SES total scores’ between ‘boys’ and ‘girls’ with VI. ‘SES total scores’ for ‘girls’ were significantly higher than those for ‘boys’, as reported by both parents (‘boys’: N = 17, M = 91.65, SD = 14.92; ‘girls’: N = 18, M = 101.89, SD = 13.86), t(33) = −2.104, p < .05, and teachers (‘boys’: N = 12, M = 93.42, SD = 13.72; ‘girls’: N = 15, M = 107.47, SD = 11.7), t(25) = −2.871, p < .05 rated ‘girls’ SESs significantly higher. No significant difference was found in scores self-reported by students (‘boys’: N = 11, M = 102.36, SD = 9.36; ‘girls’: N = 14, M = 101.79, SD = 11.2), t(23) = .137, p = .44. These results suggest that parents and teachers perceive ‘girls’ as having higher SESs, whereas students’ self-reported scores did not differ by gender, indicating that the relationship between gender and SESs varies depending on the respondent.
The Pearson correlation analysis was performed to assess the relationship between age and ‘SES total scores’ in children and adolescents with VI. A significant positive correlation was found for parents, r(33) = 0.332, p < .05, and teachers, r(25) = 0.410, p < .05. However, no significant correlation was observed for students, r(23) = 0.251, p = .11. These results suggest that age was positively associated with SESs from the parents’ and teachers’ perspectives but not from the students’ perspective.
Regarding inclusive extracurricular activities (e.g., music and theatre were most common in this study sample) and inclusive sport activities (e.g., gymnastics, swimming, skiing, climbing, dance, and cycling), independent samples t-tests compared the ‘SES total scores’ between children and adolescents with VI who do and do not participate in such activities. The reported ‘SES total scores’ were significantly higher for participants in inclusive extracurricular activities across all respondent groups: students (yes: M = 104.00, SD = 10.43; no: M = 94.00, SD = 7.95), t(14) = −2.01, p < .05; parents (yes: M = 100.38, SD = 13.63; no: M = 85.38, SD = 15.20), t(22) = −2.44, p < .05; and teachers (yes: M = 110.30, SD = 9.019; no: M = 96.33, SD = 16.56), t(14) = −2.20, p < .05. These findings suggest that participation in inclusive extracurricular activities is associated with higher ‘SES total scores’ for children and adolescents with VI, as reported by all respondents. Moreover, the ‘SES total scores’ were significantly higher for children and adolescents with VI participating in inclusive sports activities, as reported by parents (yes: M = 100.28, SD = 13.81; no: M = 86.78, SD = 14.98), t(25) = −2.329, p < .05, and teachers (yes: M = 109.85, SD = 8.76; no: M = 93.60, SD = 17.09), t(16) = −2.701, p < .05. No significant differences were found for self-reported scores of students (yes: M = 103.79, SD = 10.78; no: M = 94.25, SD = 7.41), t(16) = −1.643, p = .06. These results suggest that participation in inclusive sports is associated with higher ‘SES total scores’ according to parents and teachers but not as strongly from the students’ perspective.
Discussion
The statistical analysis suggested no significant differences in SESs between children and adolescents with VI and the general population. This partially contrasts with previous studies that reported greater difficulties in SESs for children and adolescents with VI (Buhrow et al., 1998; Ozkubat & Ozdemir, 2014; Salleh et al., 2011). Although these findings are based on perceptions rather than direct observations of SESs, they suggest that disparities in SESs may be less pronounced than previously believed (Manitsa, 2023). Several factors may explain this discrepancy. First, most participants attend inclusive educational settings, where positive school climates (Hess, 2010) and supportive social interactions (De Verdier, 2016; Jessup, 2022) may foster the development of SESs (Miyauchi, 2020; Ozkubat & Ozdemir, 2014). Second, the participants, aged 8 to 18, may have developed socio-cognitive skills through compensatory strategies (Peterson et al., 2000) and the use of language as a tool for self-regulation (Pérez Pereira & Conti-Ramsden, 2020; Vygotsky et al., 1997). Finally, evaluators may rate SESs more favourably because of the participants’ status as children and adolescents with disabilities – a bias known as ‘benevolent ableism’ (Nario-Redmond, 2020). However, these group-level findings should be interpreted with caution. An individual-level analysis revealed considerable variability, with a substantial number of children and adolescents with VI receiving ratings of either ‘below average’ or ‘above average’ from parents and teachers. This underscores the need for nuanced, case-by-case assessments to accurately identify each child’s unique profile of strengths and challenges across the different domains of SESs.
The findings showed a positive correlation between SES scores reported by students and parents, suggesting shared perceptions likely shaped by their home-based experiences, where emotional behaviour and relationships are more easily observed. In contrast, teachers’ ratings differed, reflecting differences in both context and evaluative frameworks. Teachers observe students in structured classroom settings that emphasize self-regulation, cooperation, and academic-related social behaviour. As a result, their evaluations may be shaped by more performance-based or normative standards. These differences highlight how context shapes SES assessments and support using multiple informants for a more complete understanding (Martinsone et al., 2022).
Parents perceived children and adolescents with ‘mild VI’ as having better SESs, particularly in Social Awareness and Relationship Skills, than those with ‘moderate VI to blindness’, which differed from the SES perceptions of students and teachers. This suggests that while compensatory strategies may help, more severe VI still affects SES development, complicating the awareness of one’s surroundings and social relationships (Dale & Salt, 2007; Klauke et al., 2022; Tadić et al., 2009). The findings indicate that certain SEL domains are more sensitive to VI severity, emphasizing the need for a detailed analysis of each subdomain to guide targeted interventions (Elliott & Gresham, 2021).
Furthermore, gender and age differences emerged: parents and teachers reported higher SES scores for girls and perceived SESs to have a positive association with age, whereas students did not. Gender differences in SESs, with girls exhibiting better social-emotional functioning, are consistent with findings in the general population (Romer et al., 2011). This may result from gender socialization (Stockard, 2006), where girls and boys are encouraged to adopt gender-specific roles. For girls, these roles often promote emotional expressivity and better social-emotional functioning (Brody & Hall, 2010). Regarding age, the findings are consistent with previous reports that compensatory strategies and SESs improve with increasing age (Peterson et al., 2000). The lack of change in students’ reports may reflect the consistency in their self-image and SES perceptions over time (Augestad & Elmer, 2017).
Finally, higher SES scores were assigned to children and adolescents with VI participating in inclusion-based activities, which is consistent with findings of previous studies on extracurricular activities (Jessup et al., 2017; Zebehazy & Smith, 2011) and sports (Alcaraz-Rodríguez et al., 2021). These activities have been associated with the development of SESs in all individuals (Cortellazzo et al., 2021), as they may contribute to enhancing SESs by fostering social interaction, self-confidence, and a sense of belonging – all of which are critical for social-emotional development in youth with VI (Roe & Webster, 2002).
The study used the French version of the SSIS-SEL RFs (Elliott & Gresham, 2021), opening up a broader discussion on the use of standardized assessment tools for individuals with VI (Hill-Briggs et al., 2007; Joyce et al., 2022; Loftin, 1997; Minks et al., 2020; Slykerman, 2022). First, comparing children and adolescents with VI to a normative sample without VI raises concerns (Slykerman, 2022). Hannan (2007) advocates for the development of measurement tools with normative data that include students with VI, but this approach must account for the significant heterogeneity within this group, including variations in age of onset, visual functioning, aetiology of vision loss (Joyce et al., 2022), and environmental influences (World Health Organization, 2001). Second, the items in standardized tools may not fully capture the specific behaviours of children and adolescents with VI (e.g., gaze direction or stillness as a sign of attention). To address this, supplementing standardized tools with those specifically designed for students with VI is crucial (e.g., Social Competence Assessment and Social Skills Assessment Tool for Children with Visual Impairments: Revised; Loumiet & Levack, 1992; Sacks, 2014). Considering these arguments, a comprehensive assessment should consider factors such as aetiology, age of onset, and degree of VI while also integrating functional vision assessments. It should recognize the limitations of normative samples and include multiple tools, respondents, and contexts to offer tailored recommendations based on each child’s unique strengths and challenges (Minks et al., 2020; Slykerman, 2022). In addition, alternative assessment methods such as systematic direct observation (Whitcomb, 2018) and dynamic assessment (Bøttcher & Dammeyer, 2016; Haywood & Lidz, 2006) should be explored to gain a deeper understanding of the child’s social-emotional development.
While these findings provide valuable insights, several limitations should be addressed. First, the sample included children and adolescents with VI as well as other disabilities (e.g., SLD, ADHD, DLD, and ASD), which may have introduced bias. In future studies, the sample could be refined by excluding comorbid conditions to facilitate a more focused analysis. Second, although comparing SES scores in children and adolescents with VI with those in the general population is informative, it remains an artificial comparison. To improve accuracy, future studies should include a control group with similar sociodemographic characteristics but without VI. Third, sociodemographic variables such as socioeconomic status, ethnicity and family support, which are likely to influence SESs, were not considered in this study. Future research should include these variables to provide a more comprehensive understanding. Finally, self-perceptions may not fully reflect actual SES performances in daily life. To address this, future studies should incorporate direct assessment methods (Whitcomb, 2018).
Future studies should explore the following areas of research in more detail. Longitudinal research is essential to better understand the acquisition and development of SESs in children and adolescents with VI (Veldhorst et al., 2022). Investigating ecological factors, such as school climate (Thapa et al., 2013), classroom climate (Wang et al., 2020), and parental socialization of emotions (Edler & Valentino, 2024) may provide valuable insights into the environments that foster SES development. It is also important to investigate how individual factors such as gender (Robinson & Lieberman, 2004) and executive functions (Heyl & Hintermair, 2015) influence SESs. Finally, expanding assessment methods to include dynamic assessment protocols (Haywood & Lidz, 2006; Norris, 2018) would offer a more comprehensive understanding of SESs, leading to better guidance for professionals.
Conclusion
Understanding social-emotional development and compensatory strategies of children and adolescents with VI is crucial for designing effective interventions. This study explored the SES profiles of children and adolescents with VI, comparing SES perceptions from different respondents (students, parents, and teachers) with the SES scores of the general population. It also investigated how SESs vary with VI severity, gender, age, and participation in inclusive extracurricular and sports activities.
The findings showed no significant differences in SESs between children and adolescents with VI and their sighted peers; however, perceptions varied across respondents. However, individual analyses indicated that a considerable proportion of children and adolescents with VI were rated as ‘below average’ by both parents and teachers. Students and parents generally reported similar SES scores, whereas teachers’ assessments differed. In addition, unlike students and teachers, parents assigned higher SES scores to children with ‘mild VI’, particularly regarding Social Awareness and Relationship Skills. Gender differences emerged, with girls being rated higher by parents and teachers; however, students did not share this perception. SES scores reported by parents and teachers increased with age, but this trend was not reflected in students’ self-reported SES scores. Finally, participation in inclusive extracurricular and sport activities was associated with higher SES scores reported by parents and teachers.
While a comparison of SESs between children and adolescents with VI and the general population remains debated, the findings confirm that the French version of the SSIS-SEL RFs (Elliott & Gresham, 2021) is an effective tool for assessing SESs in this population. However, the assessment process requires further refinement. A comprehensive assessment should consider psychometric results as well as factors such as aetiology, age of onset, severity of VI, and functional vision assessments. In addition, recognizing the limitations of normative samples and using various assessment tools, respondents, and contexts is crucial in gaining a more complete understanding of each child’s strengths and challenges regarding SES development.
In conclusion, adopting a comprehensive approach to assessment and accurately identifying each child’s unique profile of strengths and challenges across the different domains of SESs deepens the understanding of social-emotional development in children and adolescents with VI, paving the way for more tailored and effective interventions that promote social participation.