
Abstract
The COVID-19 pandemic resulted in changes to low vision service provision across the UK. The main aim of this study was to investigate service providers’ (SPs) experiences of, and views on, the impact of the COVID-19 pandemic on provision of low vision (LV) assessments, and future provision post-pandemic. A mixed methods approach employed two surveys (S1 and S2) and one-to-one semi-structured phone interviews. SPs were invited for S1 (LV assessments before and during the pandemic) between June and August 2021, and S2 (post-pandemic services) in July 2022. Eleven purposively recruited SPs gave telephone interviews, assessing changes to LV assessments during the pandemic and how experiences could inform future services. Survey responses were tested for significant differences between proportions, and interviews analysed using thematic analysis. Eighty SPs, comprising clinical and non-clinical professionals, responded to S1, 27 to S2. Two themes emerged from interviews and surveys: early pandemic modifications and remote services. From S1, during the pandemic there was a significant increase (p < .001) in the proportion of SPs providing LV assessments remotely (either alongside face-to-face provision, or remotely only), compared with pre-pandemic. S1, conducted while some COVID restrictions remained, also identified an increase in the proportion of LV assessments expected to be provided remotely post-pandemic compared with pre-pandemic (p < .001). However, for S2, conducted after all restrictions were lifted, the increase in the proportion of LV assessments actually provided remotely post-pandemic was not statistically significant (p = .20). Advantages (e.g., reduced risk of infection) and limitations (e.g., issues for hearing-impaired users) of remote LV assessments were highlighted. Remote LV assessments increased significantly during the pandemic and remained more common post- than pre-pandemic, though less common than anticipated. Many advantages were perceived, but guidance may need to be developed before remote services are more widely adopted.
Keywords
Introduction
Vision impairment (VI) is an important issue world-wide, with an estimated 1.93 million people living with sight loss in the United Kingdom (Pezzullo et al., 2018). A greater proportion of older people experience VI (Jackson et al, 2021). Challenges faced by individuals with VI can significantly impact daily living and quality of life (Man et al., 2021). Multi-disciplinary LV support and rehabilitation services form an essential part of managing everyday life for individuals with VI and their caregivers (Binns et al., 2012; Ryan, 2014) and are provided by a range of professionals including optometrists, eye clinic liaison officers (ECLOs), and rehabilitation officers – visual impairment (ROVIs 1 ). UK LV services may be stand-alone, but are more often provided within a multi-agency system. Services are provided in different settings, both statutory (National Health Service (NHS), Local authorities) and third sector organisations (e.g., charities). LV assessment is one of the support services which may involve assessing visual function; carrying out a refraction; supplying LV aids, such as magnifiers and telescopes; and providing information about other support organisations. Other organisations will, for example, provide equipment to help with daily living activities, for example liquid level indicators, and mobility and orientation training including teaching ‘white cane’ skills for navigation outdoors. In the United Kingdom, the Care Act 2014 (Care Act 2014, 2014) requires local authorities to establish and maintain registers of people in their area with VI. Registration as sight-impaired (SI) or severely sight-impaired (SSI) may help the individual to gain timely access to some of these services.
As a result of the global COVID-19 pandemic (referred to as ‘pandemic’ hereafter), the first UK lockdown was imposed in March 2020. Many other countries also imposed restrictions to try to reduce the spread of this disease (Ayouni et al., 2021). In the United Kingdom, the degree of restrictions in different geographic areas varied depending on the pressure on the NHS and the level of infection (Government UK, 2022; The Health Protection (Coronavirus, Restrictions) (England) Regulations, 2020). These limited, for example, travel, work and access to ‘face to face’ activities to ‘essential’ contacts. Within the devolved governments there were variations in guidance and regulations leading to differences in approach between England, Scotland, Wales and Northern Ireland, with the pandemic restrictions finally lifted across the United Kingdom in May 2022.
During the pandemic, hospital activity fell greatly, for example, ophthalmology saw a 35.1% fall in outpatient clinic appointments and 44% reduction in elective surgery admissions for March–December 2020 compared with the previous year (Bottle et al., 2021). Ophthalmology departments re-evaluated their practices (Safadi et al., 2020), with some introducing virtual (video) consultations. For example, Moorfields Eye Hospital NHS Foundation Trust used the ‘Attend Anywhere’ platform as they introduced video consultations for virtual Accident and Emergency clinics (Kilduff et al., 2020). Similarly, optometric practices also adapted and altered the ways in which their professional services were provided (Nagra et al., 2021). Taking account of the restrictions, NHS England, the College of Optometrists and the professional representative bodies amended and updated guidance and regulations as the pandemic progressed and risk levels changed (Allen et al, 2021).
Changes in LV support services introduced during the pandemic included greater use of remote elements, however there is currently little evidence of evaluation of these services or how they are accepted by patients (Jones et al., 2022; Wilson et al., 2021). The scoping review by Wilson et al concluded that more research is needed into reasons for older people not accessing e-health, research which addresses both actual physical and psychological barriers. This research investigated services for a predominantly older population from the perspective of both service providers (SPs) and service users and was designed to provide more insight into the acceptability of remote services for older people.
The overall aim of this study was to investigate the impact of the pandemic on a range of LV services and their likely future provision post-pandemic. The study was informed by the views of SPs, service users, and their carers. This paper focuses on one aspect of the overall research: the effect of the pandemic on LV assessments, with the aim being to provide more evidence of what happened to LV assessments and SPs’ views on the resulting impact. In the United Kingdom, service provision of LV assessments is variable (Codina & Rhodes, 2023; Dickinson et al., 2011) and, although these are typically carried out in a hospital setting, in certain areas LV assessments are performed in community optometric practices.
Methods
A mixed methods approach was taken, with data collected using surveys and semi-structured phone interviews. A literature search failed to find any similar surveys, presumably because of the specific nature of the topic. Various formats of surveys have previously been used in the low vision literature, many of which have contained questions with multiple and yes/no options (e.g., NEI-VFQ 25; Mangione et al, 2001). We therefore designed a survey that incorporated these principles alongside the addition of free-text boxes that allowed respondents to provide further information if they wished. The survey was developed in conjunction with a small group of experts (academics and SPs) who advised on survey design and the structure of the phone interviews. They also helped pilot the survey.
The multiple-choice questions and free-text boxes were constructed to seek demographic and other data designed to provide a picture of the user and their mode of practise. All authors endeavoured to ensure that the choices offered for each MCQ item covered as many likely answers as possible. Questions included requests for details of the format (face-to-face, remote, or both) in which the services were provided before and during the pandemic; and the format expected to be provided post-pandemic (S1) or actually provided post-pandemic (S2). A topic guide was devised to steer the phone interviews, which further expanded data collection on SPs’ experiences of service provision during the pandemic. See Appendices 1, 2 and 3 in the supplemental material which contain the complete surveys and topic guide.
Ethics approval was obtained from the Optometry Proportionate Review Committee, City, University of London (ETH2021 01722) and the protocol conforms to the tenets of the Declaration of Helsinki. All participants in surveys received participant information and provided consent online, or were sent the information sheet and informed consent form. Interviewees were sent an information sheet and provided consent, either in writing or verbally (see Appendices 4, 5, 6 and 7 in the supplemental material).
SPs based in the United Kingdom and aged 18 years or over were invited to participate in the initial survey (S1). Invitations were e-mailed between June and August 2021 to SP organisations known to the researchers or found on the internet. These included personal contacts in LV support services, local and national VI charities, and professional bodies. Surveys were available online via Qualtrics (Qualtrics XM – Experience Management Software, n.d.) or through an accessible Word document, for completion by anyone who provided LV support services.
SPs from various professional backgrounds (e.g., Optometrist, ECLO, and ROVI) from the four nations of the United Kingdom were purposively invited to participate in the semi-structured phone interviews, completed between July 2021 and February 2022. The interviews focussed on similar topics to S1 and were designed to gain a more in-depth understanding of the influence of the pandemic on LV services across the United Kingdom. Interviews were conducted via telephone, audio recorded, and the anonymised recordings transcribed by one author (ECF). Two pilot interviews were conducted, and minor alterations made to the topic guide based on their feedback. As a result of the pilots a further question was added to the topic guide, asking about any changes the SPs expected to see in their future services.
Results from S1 and the interviews informed the follow-up survey (S2) assessing the pandemic’s longer-term impacts on service provision, including what services were actually being delivered remotely post-pandemic. S2 was developed in a similar way to S1, with input from the expert group and piloting. In July 2022, at least 5 months after all UK pandemic restrictions had been lifted, S2 invitations were sent to those who had completed S1 and indicated a willingness to participate in a further survey. Some SPs forwarded the invitation to colleagues who also completed S2.
Data analysis
Thematic analysis of qualitative data was undertaken using NVivo software (NVivo, n.d.). Anonymised phone interview transcripts and free-text comments from both surveys were uploaded into NVivo. Researcher ECF listened to each interview twice before undertaking initial coding. These codes were re-organised to find developing topics, from which emerging themes were identified by assessing recurring or interesting comments and ideas. The anonymised transcripts and survey comments were reviewed by researcher AS, who agreed common emerging themes and subthemes and appropriate working titles with ECF. A third researcher (DFE) assessed the transcripts and survey comments for appropriateness of the themes, and disagreements were discussed to reach consensus (Nowell et al., 2017).
Quantitative data were analysed using MedCalc Software Ltd (Schoonjans, 2024). Differences between proportions were calculated using the ‘N-1’ Chi-square test as recommended by Campbell (2007) and Richardson (1994). Confidence intervals (CI) were calculated using the method recommended by Altman et al. (2000), and 95% CIs are reported. For all tests p < .05 was considered significant. No imputations have been made for missing data.
Results
Quantitative results
Out of 112 individuals who read the participant information online and consented to participate, 71% (79/112) SPs completed at least part of S1 between June and November 2021. One SP completed S1 in Word document format.
Twenty eight percent (22/80) of the respondents were optometrists, 20% (16/80) ECLOs and 18% (14/80) ROVIs. Fourteen percent (11/80) were other eyecare professionals (e.g., Orthoptists, Advisory Teacher for Children with Vision impairments) and 15% (12/80) worked in other roles (e.g., charity outreach, service co-ordinator). Six percent (5/80) did not answer the question about their professional role. Services were provided from several sources, for example, hospitals, local authorities, charities, optical practices. Several respondents worked in more than one setting (Table 1).
Demographics of those taking part in Survey 1, Survey 2, and interviews.
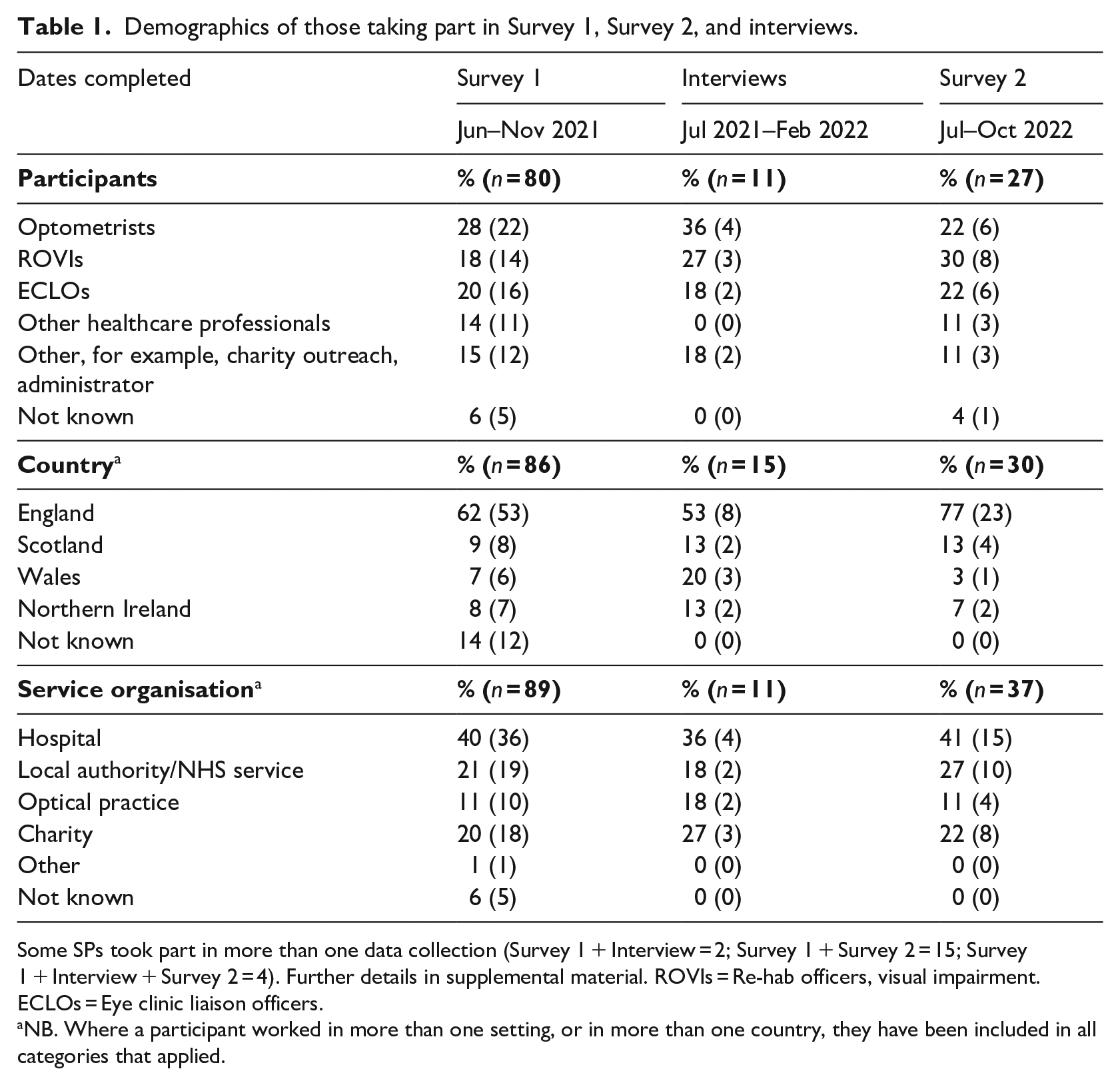
Some SPs took part in more than one data collection (Survey 1 + Interview = 2; Survey 1 + Survey 2 = 15; Survey 1 + Interview + Survey 2 = 4). Further details in supplemental material. ROVIs = Re-hab officers, visual impairment. ECLOs = Eye clinic liaison officers.
NB. Where a participant worked in more than one setting, or in more than one country, they have been included in all categories that applied.
Sixty one percent (49/80) of SPs gave information about LV assessments; 93.9% (46/49) reported LV assessments undertaken pre-pandemic face-to-face and the remaining 6.1% (3/49) providing them both face-to-face and remotely (Table 2). Forty SPs reported providing LV assessments during the pandemic, of which 15% (6/40) were face-to-face only, 22.5% (9/40) both face-to-face and remotely, and 62.5% (25/40) remotely only. The increase from 6.1% to 85.0% (22.5% ‘both’ + 62.5% ‘remote only’) in the proportion of SPs who provided LV assessments remotely during the pandemic (78.9%, CI = 61.4% to 87.8%) was statistically significant (p < .001, df = 1, Chi-square = 55.81). Forty eight SPs responded to the question asking what services they expected to provide face-to-face or remotely post-pandemic, with 54.2% (26/48) who previously provided only face-to-face services expecting to be still working face-to-face only post-pandemic. The remaining 45.8% (22/48) expected to provide both face-to-face and remote services (Table 2). Compared with the 6.1% (3/49) of SPs who provided both face-to-face and remote assessments pre-pandemic, there was a 39.7% (CI 22.9% to 54.1%) increase post-pandemic in the proportion of SPs who expected to provide LV assessment remotely (alongside face-to-face provision, none expected to provide them only remotely), which was statistically significant (p < .001, df = 1, Chi-square = 19.78).
Percentage of SPs who were providing low vision assessments face-to-face, remotely, or both face-to-face and remotely, pre-pandemic, during the pandemic, and expected to be provided (Survey 1) or actually provided (Survey 2) post-pandemic, based on survey responses. The final column shows the differences in remote provision before compared with during, and expected after pandemic (Survey 1 (top)) and before compared with during, and actual after pandemic (Survey 2 (bottom)).
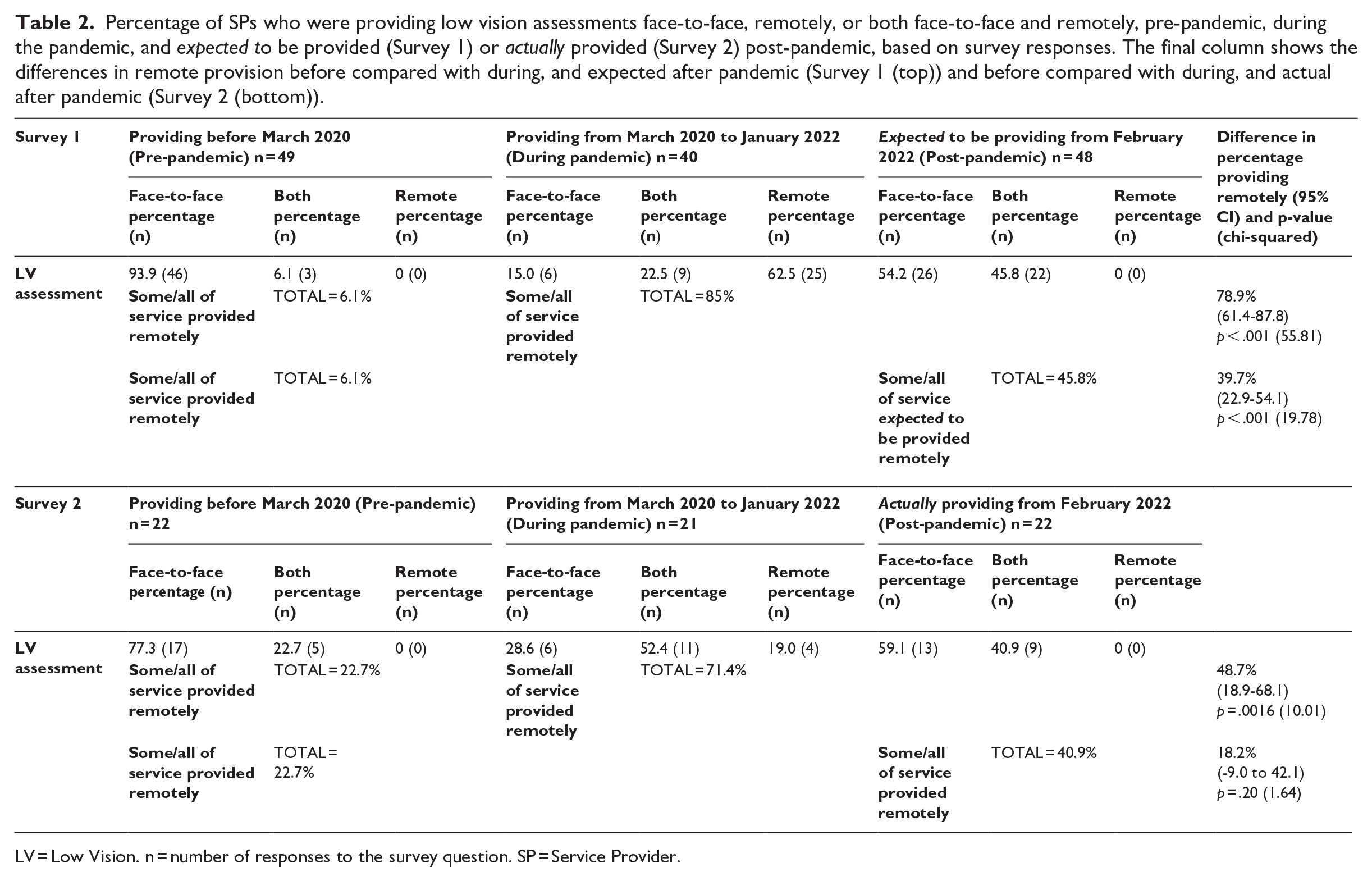
LV = Low Vision. n = number of responses to the survey question. SP = Service Provider.
Ninety six percent (47/49) of participants indicated which platforms were used for remote assessments, with several using more than one platform, giving a total of 99 responses. The most widely used platforms were phone (39% (39/99)), Zoom (19% (19/99)) and Microsoft Teams (18% (18/99)). Other platforms were WhatsApp (9% (9/99)), AttendAnywhere (7% (7/99)), Skype (4% (4/99)), BABL (2% (2/99)) and Doctorlink (1% (1/99)).
Of the 31 (out of 33) SPs who personally provided LV assessments, 32% (10/31) reported no difference in success for new or follow-up remote assessments. A total of 58% (18/31) felt follow-ups were more successful and 10% (3/31) felt new assessments were more successful. To assess the perceived advantages and disadvantages of remote LV assessments SPs were provided with a list of statements and asked to indicate all they agreed with. Eighty five percent (28/33) responded, several citing multiple statements (Table 3). The three most frequently selected advantages were: ‘There is no risk of spreading infections (COVID-19 or other)’ (75% (21/28)), ‘Clients are less stressed because they have no travel issues’ (61% (17/28)), ‘Clients are more relaxed in their own homes’ (46% (13/28)). The three most frequently selected disadvantages were: ‘Unable to pick up non-verbal clues when meeting remotely’ (82% (23/28)), ‘Some clients have difficulty engaging because they are hard of hearing/deaf’ (71% (20/28)), ‘Some clients have difficulty using remote platforms’ (64% (18/28)).
SPs’ level of agreement with statements about the advantages and disadvantages of remote LV consultations.
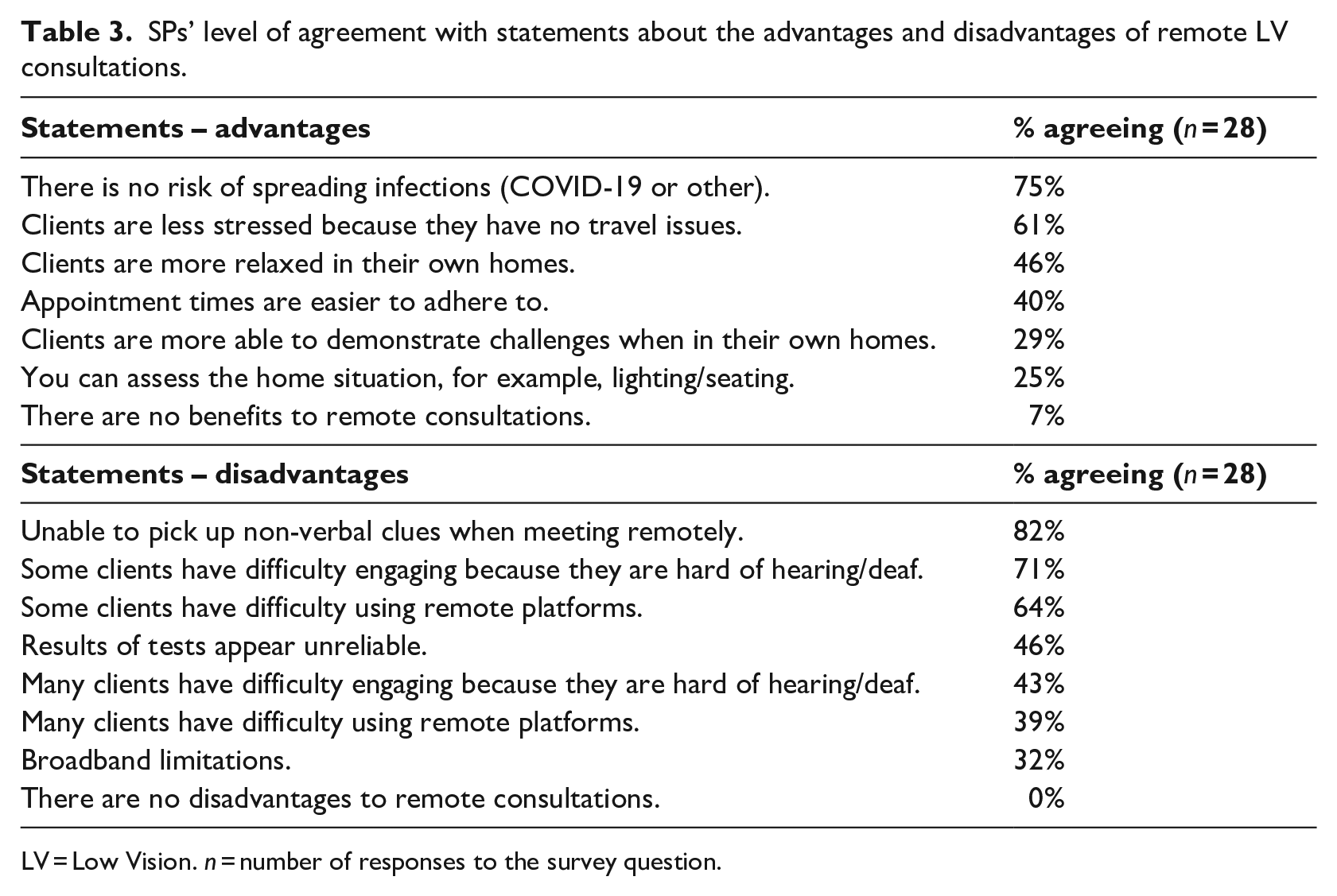
LV = Low Vision. n = number of responses to the survey question.
For the 28 (out of 33) SPs who personally provided LV assessments, one respondent felt remote assessments were not beneficial for any age group, and another SP felt they did not benefit those aged 80 + (Figure 1). The majority of SPs felt that remote assessments were beneficial ‘sometimes’, ‘frequently’, or ‘always’ for those in every age group, and that they benefitted those who were SI or had mild/moderate sight loss more than those with more advanced vision loss (Figure 2). Asked whether a caregiver’s presence at a remote LV assessment was helpful, 56% (14/25) responded ‘always’ or ‘frequently’, 40% (10/25) responded ‘sometimes’, 4% (1/25) responded ‘occasionally’, with none responding ‘never’.
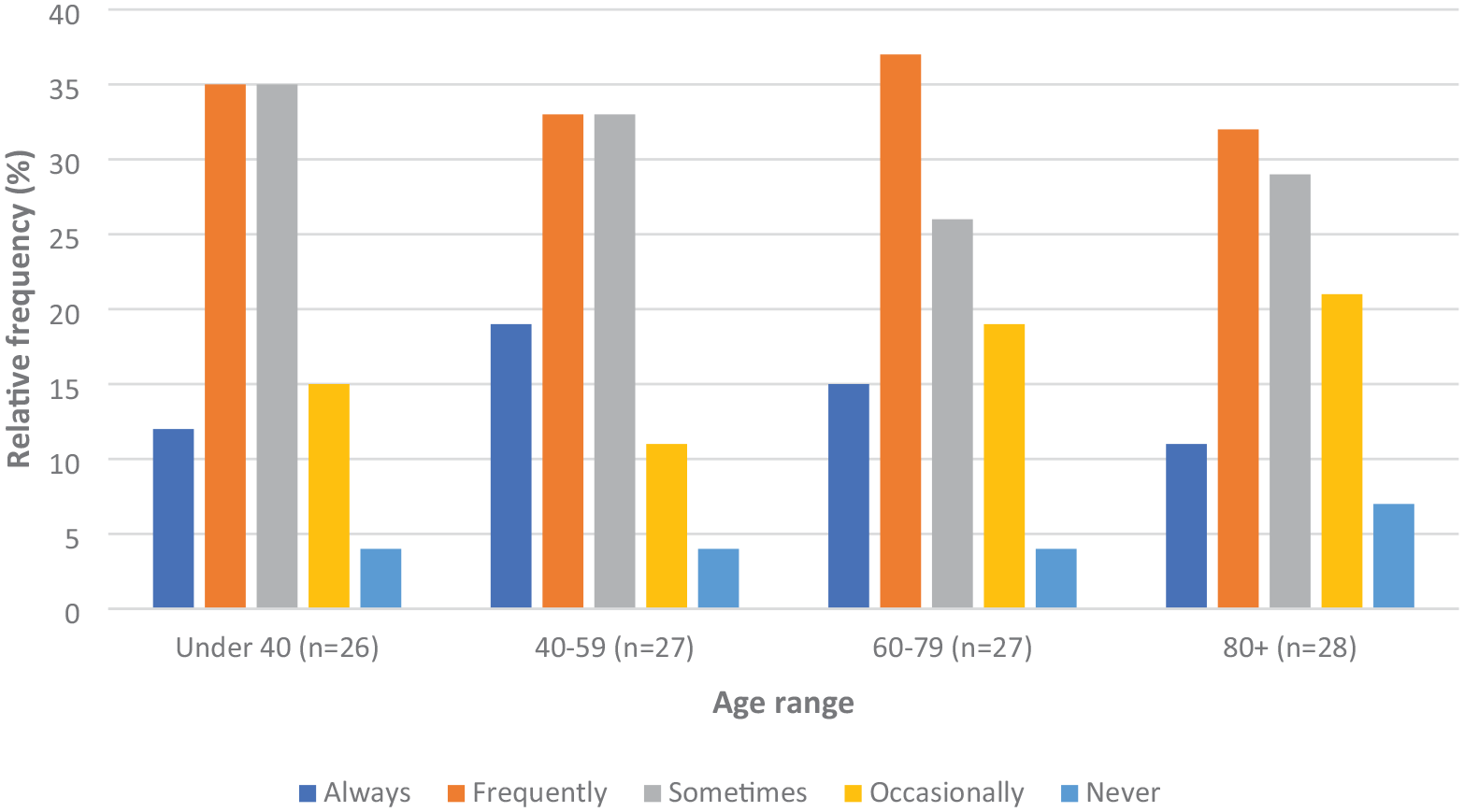
Percentage of patients perceived to benefit from remote LV Assessments across differing age ranges.
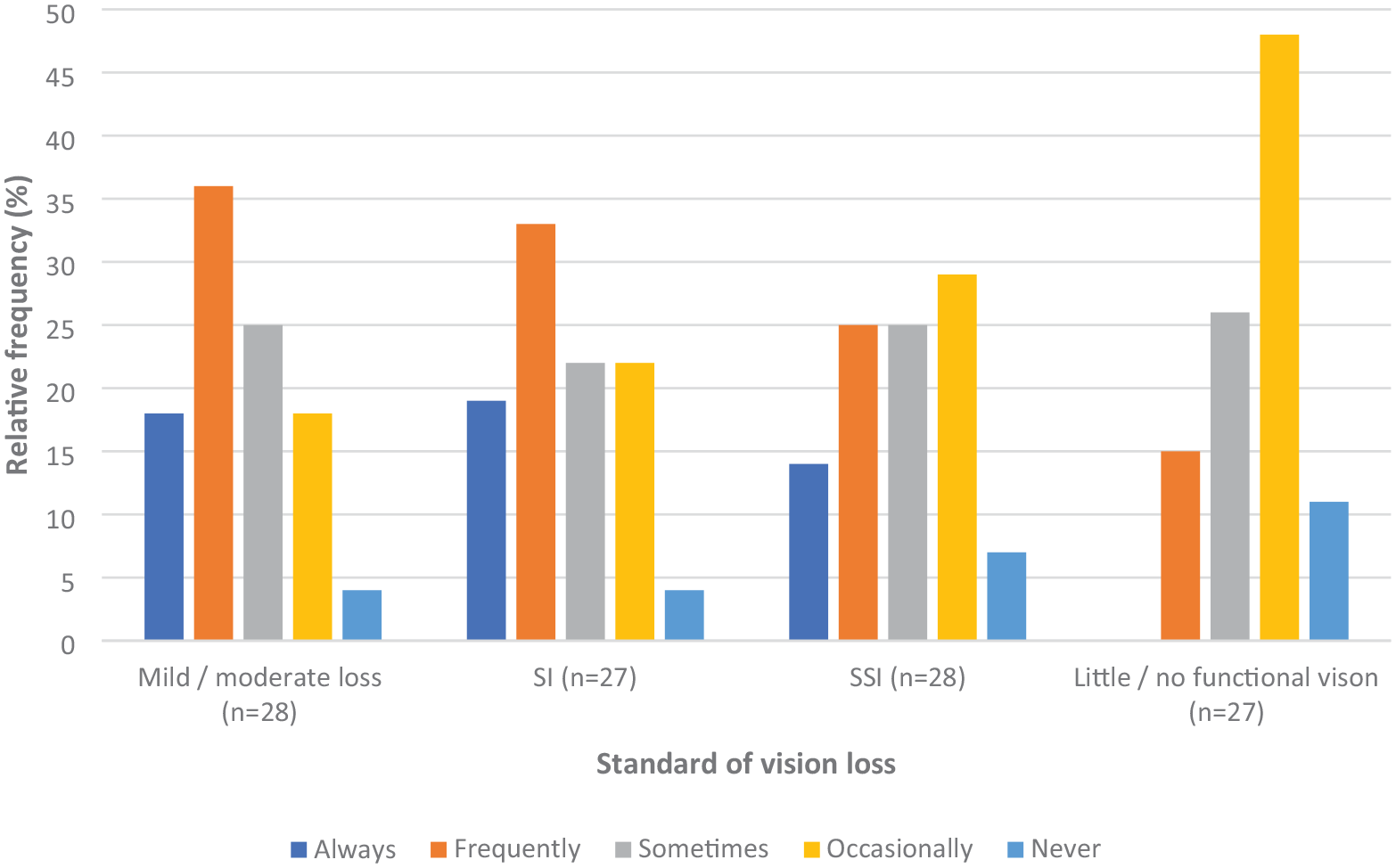
Percentage of patients perceived to benefit from remote LV Assessments across differing standards of vision.
SPs were asked whether they provided test charts when they wanted to assess vision during a remote LV assessment. Seventy nine percent (26/33) responded, with 69% (18/26) of respondents either posting chart(s) to the patient or sending a download link, citing 42 charts used. The most widely used charts (used either ‘usually’, ‘often’ or ‘sometimes’) were a reading chart (
Out of 29 individuals who read the participant information online and consented to participate, 27 (93%) completed S2 between July and October 2022. There were some differences in the distribution of participants’ professions between S1 and S2, notably a greater proportion of ROVIs took part in S2 (30%) than S1 (18%). Seventy percent (19/27) of S2 participants had also taken part in S1 (Table 1 and supplemental material). For these 19 SPs, the mean interval between completing the surveys was 361 days (CI 338 to 383 days), and the median 364 days (IQR 340 to 374 days, range 241 to 456 days). LV assessments were provided by 81.5% (22/27) of respondents. During the pandemic, the trend for remote LV assessments was, as expected, similar to S1, with an increase from 22.7% (5/22) pre-pandemic to 71.4% (15/21) (52.4% both + 19% remote only) in the proportion of SPs who provided the service remotely (either alongside face-to-face provision or remotely only) (Table 2). This difference in proportions (48.7%, CI 18.9% to 68.1%) was statistically significant (p = .0016, df = 1, Chi-square = 10.01)
However, a smaller proportion of SPs actually delivered services remotely post-pandemic than respondents completing S1 had anticipated. From S1, 45.8% (22/48) of SPs expected to provide LV assessments remotely post-pandemic compared with 6.1% (3/49) who provided services remotely pre-pandemic, and this difference in proportions of 39.7% (CI 22.9 to 54.1) was statistically significant (p < .001, df = 1, Chi-squared = 19.78). However, in S2 40.9% of SPs (9/22) actually provided LV assessments remotely post-pandemic compared with 22.7% (5/22) pre-pandemic (Table 2), and this 18.2% increase in the proportion of SPs providing remote services was not statistically significant (p = .20, df = 1, Chi-squared = 1.64) (Table 2). Analysis of the paired data for the 19 SPs who participated in both surveys shows that only 53% (10/19) of those expecting to provide LV assessment remotely post-pandemic (S1) actually provided them remotely (S2).
Respondents were asked to select options from a drop-down list to describe specific changes made to services post- compared with pre-pandemic, and the reasons for them. Twenty SPs responded, and more than one option could be selected. The changes introduced most frequently involved a phone call in advance of an appointment to decide whether a face-to-face appointment was necessary (75% (15/20)), or to collect more background information before an appointment (60% (12/20)). Fifteen percent (3/20) of the respondents reported some or all of their services had moved to a different address, and all the changes of location were reported to be for cost saving reasons. There were a total of 50 responses covering all the service change options. Thirty four percent (17/50) had made the changes for cost savings; 54% (27/50) felt that the changes made better use of their staff/volunteer time; and 66% (33/50) felt that the changes were an improvement on their pre-pandemic services (see supplemental material).
Qualitative results
Participants for the semi-structured phone interviews comprised four optometrists, two ECLOs, three ROVIs, a charity outreach worker and an optical technician (Table 1). Four provided services from a hospital setting, two worked for Local Authorities, three for charities and two for optical practices (one a fixed practice and one providing purely domiciliary services). One held a strategic/management role and another represented their profession nationally. Six provided services in England, one in Scotland, one in Wales, one in Northern Ireland, one in both England and Wales, and one UK-wide. Six of those interviewed had also completed S1 (see supplemental material). This section includes quotes from both surveys (indicated by the prefix SPQD) and semi-structured interviews (SPT). For interviewees, the type of organisation providing services is included in the reference suffix. For survey responders, this was often not possible because several worked for more than one organisation and the organisation to which their responses applied was unknown.
Two themes emerged: Early pandemic modifications and Remote services, with the sub themes of: LV consultations; Provision of LV aids; New and follow-up appointments.
Theme 1: early pandemic modifications
Early in the pandemic, with many services suspended, there was little indication about the duration of the disruption or how patients were managing. Several SPs phoned as many low vision patients as capacity allowed. These were often safety and well-being cheques rather than low vision assessments.
In some instances, serious well-being concerns were identified, for example patients struggling to feed themselves because of pandemic restrictions:
SPT01 ‘We discovered a gentleman who hadn’t eaten for nearly 2 weeks properly because his main meal was from a day centre and they’d closed the day centre and hadn’t really put in place any support for the people’. (Optometrist – Charity)
Initially calls were not prearranged and there were no protocols:
SPT06 ‘[We] decided to go to everybody who was on the waiting list and do like a telephone assessment’. (ROVI – Local authority)
Gradually SPs developed clinical protocols to facilitate provision of remote LV assessments, which became more targeted and were by appointment:
SPT01 ‘We worked on adapting the College of Optometrists’ teleconsult template to make it appropriate to low vision and then we rolled that out very very quickly so we were speaking to 4 or 5 patients a day by teleconsult’. (Optometrist – Charity)
Adaptations were also gradually applied to in-person settings, including provision of PPE and better infection control measures, which allowed more patients to be seen face-to-face in addition to providing remote appointments, but appointment numbers did not reach pre-COVID levels:
SPT07 ‘We weren’t able to see the same number of patients because of the cleaning and the PPE and the restrictions . . . there was the rigid capacity in the waiting area, . . . the patients were pre-screened, Covid screening, before they came for the service and again we had screens on the slit lamps – everything was really well set up’. (Optometrist – Hospital)
Theme 2: remote services
LV consultations
Once clinical protocols were established there was greater emphasis on triaging patients through remote consultation (usually via a phone call) followed by a face-to-face appointment if needed. This was felt to be beneficial by reducing chair time and enabling support to be started sooner; and increasing the number of patients who could be contacted:
SPT07 ‘One of the good things that we did, I felt, was that we would have phoned some of the patients prior to their appointment and undertaken some of the discussions, the history and symptoms prior to them coming in’. (Optometrist – Hospital) SPQD002 ‘We can cover a lot of information in advance of a face-to-face which shortens chair time in clinic and gets them started on support quicker’. (Optometrist)
Some providers indicated that they wanted to continue this approach post-pandemic because of the perceived benefits, for example, patients preferring remote consultations based on convenience, costs and not requiring assistance to take them to appointments:
SPT07 ‘Even when we came back to being able to see them face-to-face, some of these patients were quite content with the telephone assessments because there was no travel’. (Optometrist – Hospital)
Others felt that remote services filled a need during the pandemic but they were not a long-term option, pointing out the limitations of the tests that could be undertaken remotely:
SPT01 ‘I think it served a purpose . . . I think you can probably do a good three quarters of a low vision assessment over the phone, but you’re always going to need to do magnifier assessment, training, most of the eye examination, the objective tests, subjective test, the eye examination [face-to-face] . . . so you’re saving maybe fifteen minutes by doing a teleconsult . . . it’s still better to see them face-to-face, and I think once we started getting people back in you realise how much better it is’. (Optometrist – Charity)
Problems engaging with patients with hearing or cognitive issues were felt to be a major limiting factor to remote provision:
SPT07 ‘So for example the telephone assessment . . . wasn’t good for those with hearing loss and a lot of our people have hearing loss’. (Optometrist – Hospital)
SPs also highlighted that some patients were less accepting of remote services especially if they required a video link and the standard of remote services was not the same as a face-to-face appointment which caused concern to some SPs:
SPQD002 ‘Many of our service users couldn’t use video consult’. (Optometrist) SPT01 ‘They [the patients] might have been happy with the [virtual] assessments, but we weren’t very happy with them’. (Optometrist – Charity)
Provision of low vision aids
During the pandemic some low vision aids were prescribed following remote consultations. Several advantages and disadvantages of remote prescribing were highlighted.
Advantages included being able to help a good majority of patients remotely by prescribing them aids, including helping those struggling at home who were unable to attend in person due to being vulnerable and pandemic restrictions:
SPQD034 ‘The majority of optical aids delivered by virtual care were appropriate, maybe 75%’. (Optometrist) SPQD088 ‘Useful to help patients struggling at home’. (ECLO)
Remote prescribing was particularly useful if the patient already used a magnifier and required a ‘stronger’ aid:
SPT11 ‘So if a patient says ‘I want to try the next one up in this magnifier’, I would probably order them the next power up without really saying to them ‘well, do you want to come in and try it first?’, I’d just order it’. (Optometrist – Optical practice)
It was also a useful option if patients had broken or damaged their existing aid. These were often replaced following phone consultations, where previously a further assessment might have taken place. SPs felt this ensured individuals with VI were not left without aids:
SPQD031 ‘Good – opportunity to continue to support those with magnification needs’. (Sight loss adviser)
Disadvantages included the inability to supply more ‘complex aids’ (e.g., telescopes) and limitations imposed due to being unable to assess optimal aid type and magnification when the patient was unable to try aids during the assessment:
SPT07 ‘We couldn’t do any complex low vision aids, we kept to very simple aids. We didn’t even think about telescopes. Maybe posted out a pair of Max TV glasses which are a bit easier to cope with, but no telescopes during the pandemic’. (Optometrist – Hospital) SPQD088 ‘Difficult as unable to assess face-to-face to ensure the best magnifier’. (ECLO)
SPs also felt that because of limitations imposed on the type of aids that could be prescribed following a remote consultation only a few patients were removed from waiting lists for face-to-face LV assessments:
SPT04 ‘In terms of solving any problems as to any visual aids there were only a few patients we could take off the waiting list’. (Optometrist – Hospital)
Training individuals to use magnifiers and verify proper use was also felt to be problematic:
SPT03 ‘I did try and demonstrate how to use a magnifier on Zoom with someone, but not great at all’. (ROVI – Local authority)
New and follow-up LV appointments
SPs expressed mixed views about whether new or follow-up appointments lend themselves better to a remote format. Reasons for feeling that follow-up remote assessments were more successful included that the SP had baseline information taken at a previous face-to-face appointment:
SPQD010 ‘Certain measures are required for a satisfactory baseline appointment that would be tricky to deal with in a new case without face-to-face first’. (Optometrist)
SPs who reported no difference between new and follow-up appointments generally felt that benefits depended on the patient and where they were in their sight loss journey:
SPQD034 ‘It was perhaps easier to predict magnification and aids for review pxs [patients]. However, the holistic experience for the new pxs and referral for sensory support/ RNIB contact as well as information was for some more relevant than magnification’. (Optometrist)
Some of the reasons for preferring remote LV assessments for new patients related specifically to the situation during the pandemic when face-to-face appointments were suspended, so a remote assessment enabled the patient to understand the resources available and receive aids that would make a difference to them quickly; whereas follow-up assessments often resulted in only minor changes:
SPQD034 ‘The new patients benefitted from the quicker contact possible by phone and the information provided as well as getting magnification/ aids. With review patients . . . when magnification/ aids were fine, there was perhaps less intervention needed’. (Optometrist)
Discussion
This mixed methods research offers new insights into UK LV assessment provision before, during and after the pandemic. In general, the proportion of remote LV assessments increased significantly during the pandemic, with some services transitioning to fully remote delivery. Respondents to S1, conducted before all restrictions were lifted, expected the proportion of LV assessments provided fully or in part remotely to increase significantly post-pandemic. The actual increase in provision of remote LV assessments, assessed in S2, was not statistically significant post-pandemic, although the increase of 18% (from 23% to 41%) represents a notable shift towards hybrid provision. There could be several reasons for this marked difference between expectations in S1 and reality in S2. S2 was completed approximately one year after S1 and priorities for many SPs may have changed, with remote LV assessments no longer a priority once regulations restricting face-to-face services had been fully lifted. Often SPs are not in control of the format of services they provide, being largely dependent on their managers for making service level decisions. Some managers may be change-averse and would not favour a move to hybrid delivery. Also, some providers may still have been awaiting approval for change, as approval processes are often protracted. Remote services may become more widely used and accepted once more evidence is gathered about their effectiveness. Currently the evidence is limited, however a 2013 Manchester initiative (Parkes et al., 2013) demonstrated that a telephone follow-up for patients issued with LVAs was useful to address problems and determine how soon an in-person appointment should be scheduled. Some remote LV services had been successfully implemented in the USA before the pandemic, but they were primarily focused on ongoing rehabilitation rather than initial vision assessment and LV aid provision (Ihrig, 2014). Bittner et al (2018) carried out a literature review on remote LV rehabilitation and found only one completed clinical trial and two more underway. A scoping review by Jones et al (2022) found that more research is needed into the long-term benefits from LV telerehabilitation, and that currently patients varied in their ability and willingness to take part.
Our study highlighted different approaches to LV assessment provision during the pandemic; some SPs ceased all services while others provided a full service, similar to pre-pandemic levels. Similarly, different policies were highlighted across the optometry sector, where 42% of practitioners were reported to be furloughed during the pandemic (Nagra et al, 2021). Although not specific to LV services, it was noted that there were differences in patient pathways in England, Scotland, Wales and Northern Ireland. The Clinical Council for Eye Health Commissioning (College of Optometrists, 2021) surveyed eyecare professionals from different backgrounds and providing LV services for a variety of organisations. It reported 52.6% of LV assessment services were suspended during April–June 2020, with 36.8% reporting all services restored by March 2021 (20.6% respondents did not know). Our survey found 18% of SPs did not report any services available during the pandemic (until January 2022). Several reported initially suspending services and re-introducing them from September 2020. A survey by the London Eye Health Network, based on the work of ECLOs (London Eye Health Network, 2023) showed all but urgent face-to-face LV clinics cancelled and re-hab mainly restricted to remote services using phones. Several practitioners in our surveys worked in more than one setting, and so it was not possible to deduce whether services were more disrupted or returned to normal more quickly in one setting compared with another, for example, hospital, optometric practice. These differences are perhaps unsurprising given that even pre-pandemic, UK LV services demonstrated variations in service type, provision and funding. For example, in Wales, there is a country-wide LV assessment and aid provision service funded through optical practices (Ryan et al., 2013). In England, the NHS funded LV services are provided through hospital contracts and charities rather than independent optical practices, although provision varies (Codina & Rhodes, 2023; Dickinson et al., 2011)
During the pandemic, instead of meetings, discussions, protocols and pilot studies before new services were commissioned, SPs worked more independently and at speed. New services were rolled out much faster, for example, the COVID-19 Urgent Eyecare Service (CUES) was commissioned within a month (Kanabar et al., 2022). Although this environment encouraged SPs to introduce new, innovative services, there was insufficient time to research them thoroughly or to access resources and training. Consequently, although SPs felt remote services had been successful during the pandemic, many reverted to face-to-face format post-pandemic, with some remote elements retained. Some SPs regarded remote services as an excellent ‘stop gap’, but felt they were less effective than face-to-face and, therefore, once the pandemic restrictions were lifted, services reverted to those previously commissioned.
Some SPs identified benefits from elements of remote services, for example a phone appointment before a face-to-face clinic visit. These enabled SP and patient to be better prepared for the face-to-face appointment, for instance having the required equipment or information to hand. Responses to S2 suggested that several respondents who used pre-clinic calls did not regard them as being a ‘remote’ service, reporting that they only provided the service face-to-face. These differences in interpretation by SPs make it more difficult to compare and evaluate services and suggest that the proportions of those reported as offering remote services could be underestimates. Limitations of replacing face-to-face services with fully remote ones were also found in other health-related services, for example, physiotherapy (Saaei & Klappa, 2021), although the benefits of a hybrid model with some parts provided face-to-face and other elements provided remotely were also highlighted.
Our findings highlighted that SPs felt that some patients were less likely to benefit from remote services than others. Several barriers were cited; those with greater vision and hearing loss and cognitive impairment were more likely to struggle when using remote services. Similarly, a survey of Occupational Therapists (OT) (Almog & Gilboa, 2022) highlighted that 9% of respondents found remote OT services inadequate for those with cognitive decline, significant vision impairment or hearing loss. Wilson et al (2021) concluded that hearing impairments and memory problems (e.g., remembering passwords), were barriers to accessing e-health consultations. Jones et al (2024) suggested that those with hearing loss found remote phone services challenging. Although previous researchers have also highlighted age as a barrier to benefitting from remote services (Almog & Gilboa, 2022; Jones et al, 2024; Wilson et al, 2021), a majority of SPs (approximately 60%) in our study felt that all age groups could benefit, either ‘always’, ‘usually’ or ‘sometimes’ from remote LV services. A small minority (7%) suggested that they were never beneficial for those aged 80 plus. Technological barriers such as Wi-Fi access and difficulty using remote platforms were also cited. Lack of access to reliable Wi-Fi particularly impacts older people, those on lower incomes, and those with a disability (Office for National Statistics, 2020). People with a VI are disproportionately represented in this population. Although numbers of older and disabled people with internet access are increasing, this remains a potential barrier. People with VI are also more likely to have difficulties using technology. Encouragingly, several interviewees reported that more IVIs started using technology (iPads, etc.) during the pandemic, often with encouragement from family members keen to remain in contact. Patient and public safety is another potential barrier. One interviewee commented that the safety implications of remote LV assessments should be considered when advising individuals with early vision loss about driving standards when VA cannot be measured accurately during the remote appointment and face-to-face VA measurements are not recent. Despite these barriers, many SPs pointed to the benefits of remote services, including no risk of infection and removing the need to travel, both of which can cause difficulties whether or not there is a pandemic.
Interestingly, many of the platforms used for remote LV assessments, for example, Zoom (Zoom, 2023) and WhatsApp (WhatsApp Web, n.d.) were not designed for e-health consultations, raising security concerns when confidential information was discussed. Although some SPs used an NHS approved platform, Attend Anywhere (AttendAnywhere video consultations guidance for patients, n.d), specifically designed for e-health consultations, concerns have been raised over platform accessibility issues, especially for the elderly (British Geriatrics Society, 2021). Future studies should identify platforms suitable for remote LV assessments, bearing in mind security and accessibility issues for IVIs. Platforms such as Zoom and WhatsApp are likely to be acceptable for social meetings, such as peer support groups, but not for more confidential health appointments.
Most SPs felt remote LV assessments were better for follow-up appointments than for new patients as follow-ups already possessed an aid and supplying a stronger equivalent might suffice. On average, SPs completed S1 17 months (SD = 1.3) after the pandemic restrictions had been introduced. During this period, most routine services, such as follow-up appointments, had been delayed. Most follow-up appointments would therefore relate to patients for whom the previous assessment had been face-to-face and the SPs would have access to some information regarding the patient. New appointments were more difficult without an accurate measure of VA. Surprisingly, some SPs did not provide any charts to assess vision/VA during a remote assessment. For the telephone-based LV assessments at Moorfields during the pandemic both distance and near charts were sent to patients (Patel et al., 2021). In future, protocols should be developed for LV assessments stating which charts should be used to allow appropriate assessment of patients’ needs. Other charts are available for home testing of vision, such as SpotChecksTM (Bianchi et al., 2024) to measure contrast sensitivity, raising the possibility of expanding the investigation of vision remotely.
Several SPs felt remote LV assessments did not reduce waiting lists as only ‘simple’ aids (reading or Max-TV) could be dispensed, rather than more complex aids (hand-held telescopes). However, hand magnifiers for reading are the most commonly prescribed LV aids, with more complex aids not usually prescribed even in face-to-face clinics (Lindsay et al., 2004). A 2022 audit of LV aids usage confirmed that simple magnifiers are the most accepted devices long-term (Gothwal & Sharma, 2023). This indicates that the way forward may be to offer simple aids remotely and only provide more complex aids face-to-face where there is a perceived need and the patient is felt to be suitable, rather than routinely. The audit of LVA usage (Gothwal & Sharma, 2023) also found that patients are more likely to abandon aids due to a lack of training in their use. Several SPs had commented on the importance of training and how difficult this is in a remote setting. An American study by Bittner et al (2022) found remote training in the use of magnifiers to be well accepted and successful. However, the subjects all used video links and had been seen in person for initial training in using the aid. This suggests that initial in-person assessments and training followed by remote follow-ups to be a way forward. Future research into remote LV assessment should investigate which LVAs can be successfully prescribed remotely and which models of low vision assessment work well, for example an initial in-person appointment with further remote appointments for training/refining the LVA prescribed.
It was noted that remote services provision initiated during the pandemic and as a direct result of it were instigated in haste. This caused several challenges for providers. There were few protocols for undertaking remote services and the regulatory bodies were silent on this scope of practice. Conducting remote services was not part of the core training for optometrists, dispensing opticians, ROVIs, and so on. Some professional body organisations have started to address these issues, but more work would benefit the future provision of remote LV services.
There were several study limitations. Our intention was to distribute S1 after all pandemic restrictions had been lifted, however, when ethics approval was granted in June 2021 some restrictions remained in place, with no definite end-date available. It was decided to distribute S1 without further delay, before memories became less reliable. However, the timing made it impossible for SPs to give definitive answers regarding post-pandemic services. Therefore, the questions asked were about services provided, and their format, before and during the pandemic; expectations about services to be provided post-pandemic; and SPs’ views about the appropriateness of the provision and format. This uncertainty meant that we carried out a second survey S2 when all restrictions were lifted but this may have created survey fatigue with only 27 participants taking part in the second survey despite efforts by all investigators to boost recruitment. It was also difficult to calculate response rates – alongside S1 being distributed to known contacts, we also advertised on the social media platform Twitter, therefore it was not possible to identify how many SPs had access to the survey but decided not to participate. Throughout both surveys, SPs were asked to indicate whether they provided specific services face-to-face, remotely, or both. There was no option (apart from on a paper Word version) to state that the service was not provided. Where the answers to these questions were left blank, the researchers could not establish whether the service was normally provided but temporarily suspended; whether it had never been provided; or whether the participant had inadvertently missed the question. As a result, we treated answers left blank as missing data. In retrospect, the options ‘temporarily suspended’ and ‘never provided’ should have been included.
The sample who completed S2 was small (27 and only 19 of these completed both surveys) and may not be representative of LV SPs as a whole, limiting generalisability of our results. The survey length may have deterred potential participants. Another factor with potential to contribute to the low completion rate of S1 was that many SPs themselves have VI (personal experience) and use software which is incompatible with currently available survey platforms.
Conclusion
This study has gathered useful data on the benefits of, and barriers to, remote LV assessment service provision. The increase in remote provision during the pandemic was statistically significant and, although remote services remained more common post- than pre-pandemic, the increase was not statistically significant and remote provision was less common than providers anticipated. Further research is required before remote services are more widely adopted. The documented learnings from the expansion of remote LV assessment provision during the pandemic will provide useful information in the event of another pandemic; an event designated as ‘pandemic X’ (New Scientist 2024; World Health Organisation 2022) for which the WHO is already planning. Documenting findings about SPs’ experiences during the pandemic will likely increase preparedness of LV SPs for another pandemic event.
This study demonstrated the potential for providing elements of LV assessments and the provision of aids remotely. However, when introducing remote services, the following guidelines and factors should be considered -
The benefits of remote services are not currently well understood, and more evidence is needed. Our research suggests that an initial face-to-face appointment followed by remote services may be the best option for managing LV support. However, current limitations of aspects of remote vision assessment, and the awareness that pathology could develop after the initial face-to-face assessment, suggest that further periodic face-to-face appointments would be required.
Practitioners should consider an initial phone/video appointment to gather information, and provide the patient with initial information and reassurance, before a new face-to-face low vision clinic appointment. This should reduce, and make better use of, the time spent in the clinic.
Not all patients would be suitable for remote services, and consideration should be given to factors such as their level of VI; other challenges such as hearing or cognitive impairment; and, if necessary, the presence of a ‘carer’ to assist with the IT. Reliability of Wi-Fi should also be a consideration.
Protocols for remote services would be beneficial to assist commissioners. These should indicate which patients are best suited for remote assessments, the types of test chart that should be used, and the most suitable platforms for conducting remote assessments.
To initiate the development of protocols for commissioners the authors intend to highlight the results of this research to the professional bodies who influence regulation, clinical practice and commissioning of LV support services; and to organisations commissioning research into relevant areas of health and social care. These include, but are not limited to the following UK organisations: College of Optometrists, General Optical Council, LOCSU (Local Optical Committee Support Unit), Rehabilitation Workers Professional Network, UKRI (UK Research and Innovation).
Supplemental Material
sj-docx-1-jvi-10.1177_02646196241298207 – Supplemental material for Service providers views on changes in low vision service provision during and after the COVID-19 pandemic
Supplemental material, sj-docx-1-jvi-10.1177_02646196241298207 for Service providers views on changes in low vision service provision during and after the COVID-19 pandemic by Elizabeth C Frost, David F Edgar, Christine Dickinson and Ahalya Subramanian in British Journal of Visual Impairment
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.