
Abstract
Paediatric vision impairment is a significant public health issue because of the associated health and economic consequences. This study aimed to determine the clinical characteristics and causes of vision impairment in paediatric patients who presented to a university-based low vision eye clinic in KwaZulu-Natal. The study used a retrospective design and included all paediatric patients with vision impairment who were younger than 18 years and presented to the university-based low vision eye clinic between January 2015 and December 2019. The sample consisted of 156 children with vision impairment with a similar proportion of males (n = 82) and females (n = 74). The mean age of the children was 13.5 ± 2.8 years, with a range of 5–17 years. Based on the best-corrected visual acuity (VA), most of the children (n = 111) had moderate vision impairment (VA worse than 6/18 to 6/60). The most common causes of paediatric vision impairment included albinism (n = 54), refractive error (n = 11), cataract (n = 10), and glaucoma (n = 10). The retina (n = 74) and normal globe (n = 26) were the most affected anatomical sites. Spectacles were prescribed to almost half of the sample (n = 76). A total of 126 optical and non-optical devices were recommended with telescopes (n = 43) and sun-protective measures (n = 20) being the most common. Paediatric vision impairment can have a negative impact on the quality of life. Local data related to the characteristics of children with vision impairment can be used to enhance the services provided in this university-based low vision clinic. This is important as efforts aimed at early identification, management, and rehabilitation will help minimise functional limitations and improve the quality of life of affected children.
Introduction
Recent estimates from the World Health Organization (WHO, 2019c) indicate that 2.2 billion people have vision impairment (Bourne et al., 2021). Of this number, 295 million have low vision (visual acuity [VA] <6/18 but ⩾3/60 in the better eye) and 43.3 million people are blind (VA <3/60 in the better eye) (Bourne et al., 2021; World Health Organization, 2019c). The global prevalence of vision impairment in children younger than 14 years is 2.8%, with earlier studies estimating that approximately 19 million have vision impairment (17.5 million with low vision and 1.4 million with blindness) (Abdolalizadeh et al., 2021; Gilbert & Foster, 2001; Pascolini & Mariotti, 2012). Despite children accounting for a small proportion of the global estimate, paediatric vision impairment was recognised as an important public health issue and included in the VISION 2020: The Right to Sight programme (Courtright et al., 2011; Gilbert & Foster, 2001). This is because paediatric vision impairment poses significant health and economic burden as the earlier onset of vision impairment and the greater number of disability-adjusted life years in children can have more profound consequences (Abdolalizadeh et al., 2021; O’Sullivan et al., 1997). Furthermore, some of the conditions that result in childhood blindness also cause death where high rates of childhood mortality have been observed within the first few years of becoming blind (Gilbert & Foster, 2001; Ozturk et al., 2016). Therefore, the VISION 2020: The Right to Sight programme aimed to achieve a 0.35 per 1000 children reduction in the global prevalence of avoidable childhood blindness in 2020 by planning and implementing strategies to better screen, diagnosis, and manage ocular conditions that have the potential to contribute to paediatric vision impairment (Gilbert & Foster, 2001). Despite the considerable efforts and successes over the last two decades to reduce the global burden of vision impairment, the eye care sector has now moved into the post VISION 2020 era that is also experiencing the COVID-19 pandemic and will have to plan and implement new strategies to address adult and paediatric vision impairment (Ung et al., 2021).
Even though paediatric vision impairment is a global public health issue, there are differences in the prevalence figures and distribution of conditions that cause vision impairment across the different regions. These variations are likely a result of several factors including income level, area of residence (rural vs urban), socioeconomic status, availability of eye care services, and demographic factors such as age and gender (Chandna & Gilbert, 2010; World Health Organization, 2019c). Consequently, there is no single condition that is responsible for global paediatric vision impairment, but literature shows certain trends that have been associated particularly with the socioeconomic levels in the different regions (Courtright et al., 2011). In high-income countries, cerebral visual impairment is the commonest cause of paediatric vision impairment (Gilbert et al., 2017; Solebo & Rahi, 2014). Retinopathy of prematurity is emerging as the leading cause in middle-income countries and urban parts of low-income countries (Courtright et al., 2011; Gilbert et al., 2017). The trend in low-income countries is changing as the rate of corneal scarring has substantially decreased over the past few years, and this has been attributed to improvements in measles immunisation coverage and vitamin A supplementation in these countries (Courtright et al., 2011; Gilbert et al., 2017). Despite this, the overall number of children with vision impairment in low-income countries has not reduced as childhood cataracts have become the most common cause of paediatric vision impairment (Gilbert et al., 2017). In all countries and similar to the trend observed in adult populations, uncorrected refractive error is a significant cause of avoidable vision impairment in children (World Health Organization, 2019a).
The University of KwaZulu-Natal (UKZN), which is located in KwaZulu-Natal, South Africa, is one of four higher education institutions that provide optometry education and training in South Africa. As part of the facilities and aligned to the community engagement and teaching and learning agendas of UKZN, the university-based eye clinic aims to provide affordable eye care services to the public, especially previously disadvantaged communities, throughout the academic year (Mashige, 2010). The clinic serves as a referral centre for patients from KwaZulu-Natal and surrounding areas. Consequently, the university-based eye clinic provides low vision examination and management services to enable individuals with vision impairment to use their residual vision more effectively and thereby increase their participation. It is estimated that 11 million individuals across all age groups in South Africa have vision impairment (International Association for the Prevention of Blindness, 2022). This study aimed to determine the clinical characteristics and causes of vision impairment in paediatric patients who attended the university-based low vision eye clinic. In this way, local data from the study can be used to re-evaluate and enhance the current examination and rehabilitation services to better address the needs of children with vision impairment who present to this clinic. This is important as vision impairment in children has the potential to significantly affect their development, education, and future employment activities (Ozturk et al., 2016; Solebo & Rahi, 2014). Consequently, efforts aimed at early identification, management, and rehabilitation will help to minimise functional limitations and improve the quality of life of affected children (Gao et al., 2016; Uprety et al., 2016).
Methodology
This was a retrospective research study involving a review of the clinical record cards of all patients attending the university-based low vision eye clinic from January 2015 to December 2019. Referral to the university-based low vision clinic is usually through schools (mainstream and special), eye care personnel (optometrists, ophthalmic nurses, and ophthalmologists), and other health care practitioners. Following the United Nations Convention on the Rights of the Child, a child was defined as any individual younger than 18 years (United Nations International Children’s Emergency Fund [UNICEF] UK, 1989). Therefore, only record cards of children during the study period were included in the study. Ethical approval (reference number 1052/2020) was obtained from the Biomedical Research and Ethics Committee at UKZN and the study was undertaken according to the tenets of the Declaration of Helsinki. Gatekeeper approval to access the clinical record cards in the eye clinic was obtained from the Academic Leader of the Discipline of Optometry at UKZN.
Data extracted from the record cards included demographic (age and gender) and ocular characteristics (main reason for visit, source of referral, spectacle and/or low vision device use, presenting and best-corrected distance VA and primary cause of vision impairment) and management recommendations (spectacles, optical low vision devices, non-optical devices, and referrals). Distance VA, using age and cognitive-level appropriate Early Treatment Diabetic Retinopathy Study (ETDRS) charts, was recorded in the logarithm of the minimum angle of resolution (LogMAR) notation and converted to Snellen notation. Objective refraction using retinoscopy and/or an auto-refractor was performed on all patients and subjective refraction was attempted. Magnification and device trial at distance included the use of telescopes and at near included hand-held, stand, and spectacle magnifiers. The types of optical low vision devices recommended for distance and near were based on the patient’s visual demands and goals, ease of use, dexterity, and preference during the device trial. The types of non-optical devices recommended were based on the patient’s visual demands and goals, functional limitations, and cause of vision impairment.
The 11th revision of the WHO International Classification of Disease was used to classify the level of vision impairment. In this classification, there are four categories of distance vision impairment, and these are defined according to VA as follows: mild vision impairment (VA worse than 6/12 but better than or equal to 6/18), moderate vision impairment (VA worse than 6/18 but better than or equal to 6/60), severe vision impairment (VA worse than 6/60 but better than or equal to 3/60), and blindness (VA worse than 3/60) (World Health Organization, 2019b). The cause of vision loss was classified according to the anatomical sites outlined in the WHO/Prevention of Blindness eye examination protocol for children with blindness and low vision (Gilbert et al., 1993). The different anatomical sites included the cornea, lens, uvea, retina, optic nerve, normal globe, whole globe, and others. Specific conditions such as amblyopia, refractive error, cerebral vision impairment, and nystagmus were included in the normal globe category while glaucoma, phthisis bulbi, and microphthalmos were included in the whole globe category (Gilbert et al., 1993). In most of the clinical record cards, the cause of vision impairment was a single condition. However, where two or more conditions were noted, the most preventable/treatable condition or the condition that resulted in the last event that rendered the child with blindness was selected following the WHO recommendation as has been used previously (Bamashmus & Al Akily, 2010; Uprety et al., 2016).
Data were captured on Microsoft excel and exported to the Statistical Package for Social Sciences (SPSS) version 27 for analysis. Descriptive statistics were computed and data are presented as frequencies, percentages, means, and standard deviations. The chi-square test was used to test the association between gender and the anatomical sites of the conditions causing the vision impairment. A p-value of .05 or less was considered statistically significant. For standardisation, only one researcher was responsible for screening the record cards against the study criteria and capturing the data. The researcher double-checked each data entry at a subsequent interval to verify the accuracy of data capturing. Any inconsistencies in data capturing were cross-checked against the patient record card and resolved before data analysis.
Results
Demographic characteristics
Overall, 170 clinical record cards were obtained for children who presented for examination and management at the university-based low vision eye clinic. Of these, 14 patient records were excluded as these children achieved VA of 6/12 or better after examination and were classified with no vision impairment. Therefore, the sample included in the analysis comprised 156 children with an almost equal proportion of males (n = 82) and females (n = 74). The mean age of the children at presentation was 13.5 ± 2.8 years (range = 5–17 years). The majority of children were older than 9 years (n = 144, 92.3%). Approximately one-quarter (n = 41, 26.3%) were wearing spectacles at the time of the examination. The majority were referred from schools that cater to children with vision impairment (n = 127, 81.4%) while others were referred from hospitals (n = 6, 3.8%), mainstream schools (n = 7, 4.5%), eye care personnel (n = 3, 1.9%), or the source of referral was not recorded (n = 13, 8.3%). Most reported blurred or reduced vision at distance, near, or both (n = 117, 75.0%), followed by general check-up (n = 26, 16.7%), assessment for spectacles or low vision devices (n = 7, 4.5%), symptoms including photophobia, itchy eyes, or headaches (n = 3, 1.9%), advise on eligibility for disability pension (n = 1, 0.6%) as the main reason for presenting to the low vision clinic while the record cards of two (1.3%) children did not specify the reason for the visit.
Visual acuity
Based on the presenting distance VA, 3 (1.9%) patients were classified with mild vision impairment, 100 (64.1%) with moderate vision impairment, 35 (22.4%) with severe vision impairment, and 18 (11.5%) with blindness (Table 1). Based on the VA measurements after subjective refraction, the number of patients classified with mild (n = 11, 7.1%) and moderate (n = 111, 71.2%) vision impairment increased with a corresponding decrease in the number of patients in the severe vision impairment and blindness categories (Table 1). Thirty-four children (21.8%) were legally blind according to the South African VA criterion for blindness (best-corrected VA in the better seeing eye worse than 6/60 or 1.0 LogMAR).
Distribution of WHO categories of VI based on presenting and best-corrected distance VA in the better eye among children (n = 156).
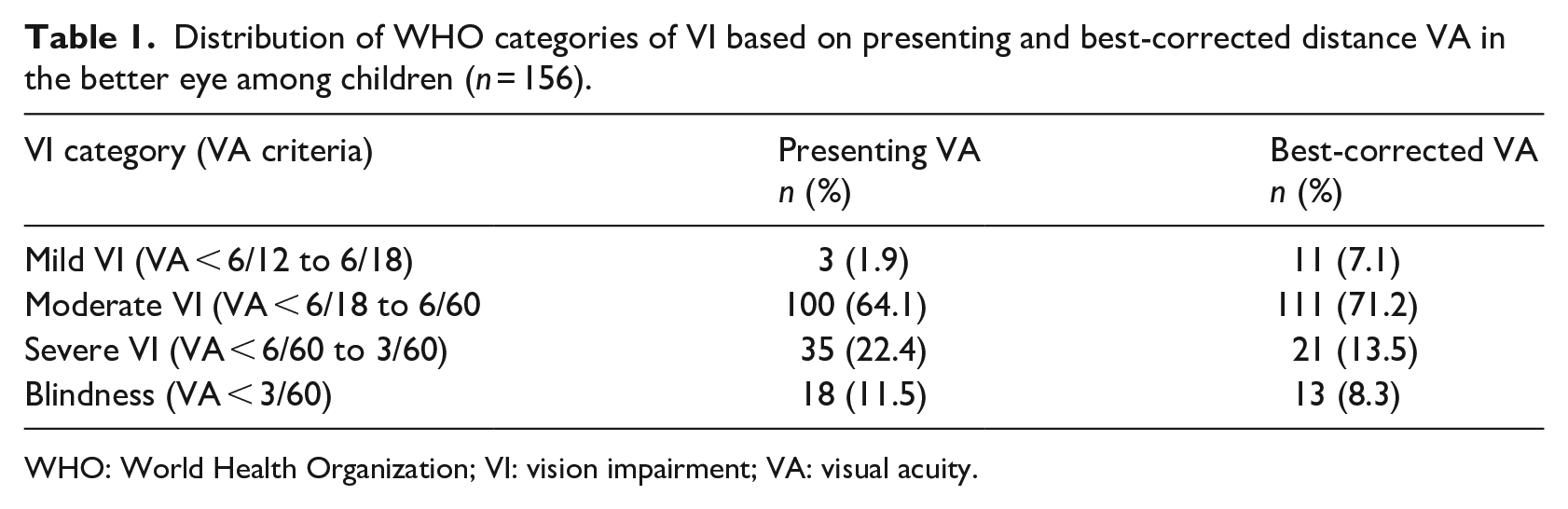
WHO: World Health Organization; VI: vision impairment; VA: visual acuity.
Cause of vision impairment
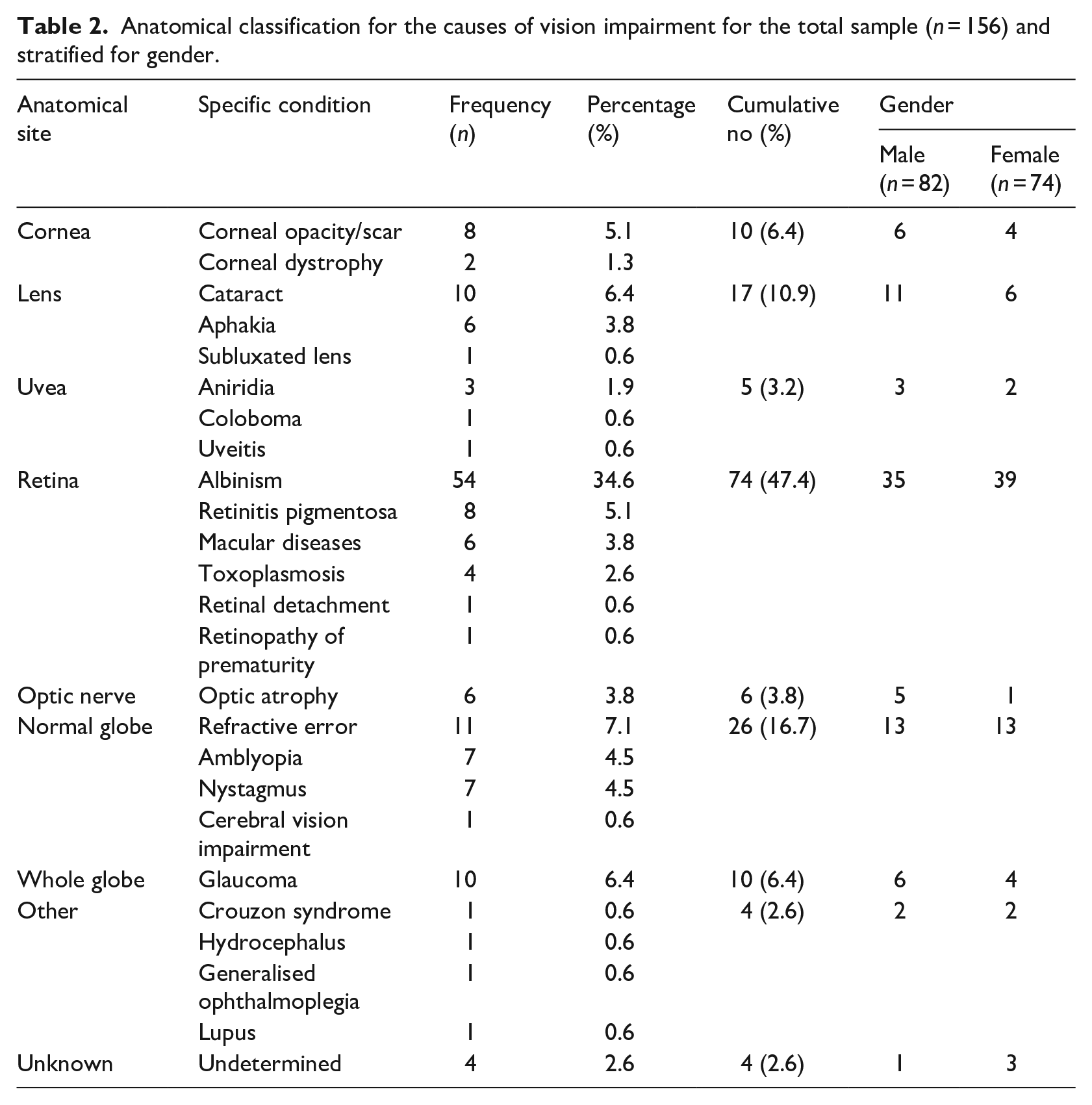
Table 2 shows the anatomical classification for the causes of vision impairment among children. The retina (n = 74, 47.4%) and normal globe (n = 26, 16.7%) were the most common anatomical sites causing vision impairment. In terms of the specific condition causing the vision impairment, albinism was the most common condition and was observed in more than one-third of the children (n = 54, 34.6%). This was followed by refractive error (n = 11, 7.1%), cataract (n = 10, 6.4%), and glaucoma (n = 10, 6.4%). Retinitis pigmentosa and corneal opacity/scar were noted in eight children each (Table 2). The specific condition causing vision impairment could not be determined in four children, and they were subsequently referred for further assessment. In terms of gender, there were either more males or an equal number of males affected in all anatomical sites except for the retina and unknown (Table 2). Despite this gender trend, there was no significant association between the anatomical site of vision impairment and gender (p = .652).
Anatomical classification for the causes of vision impairment for the total sample (n = 156) and stratified for gender.
Management recommendations
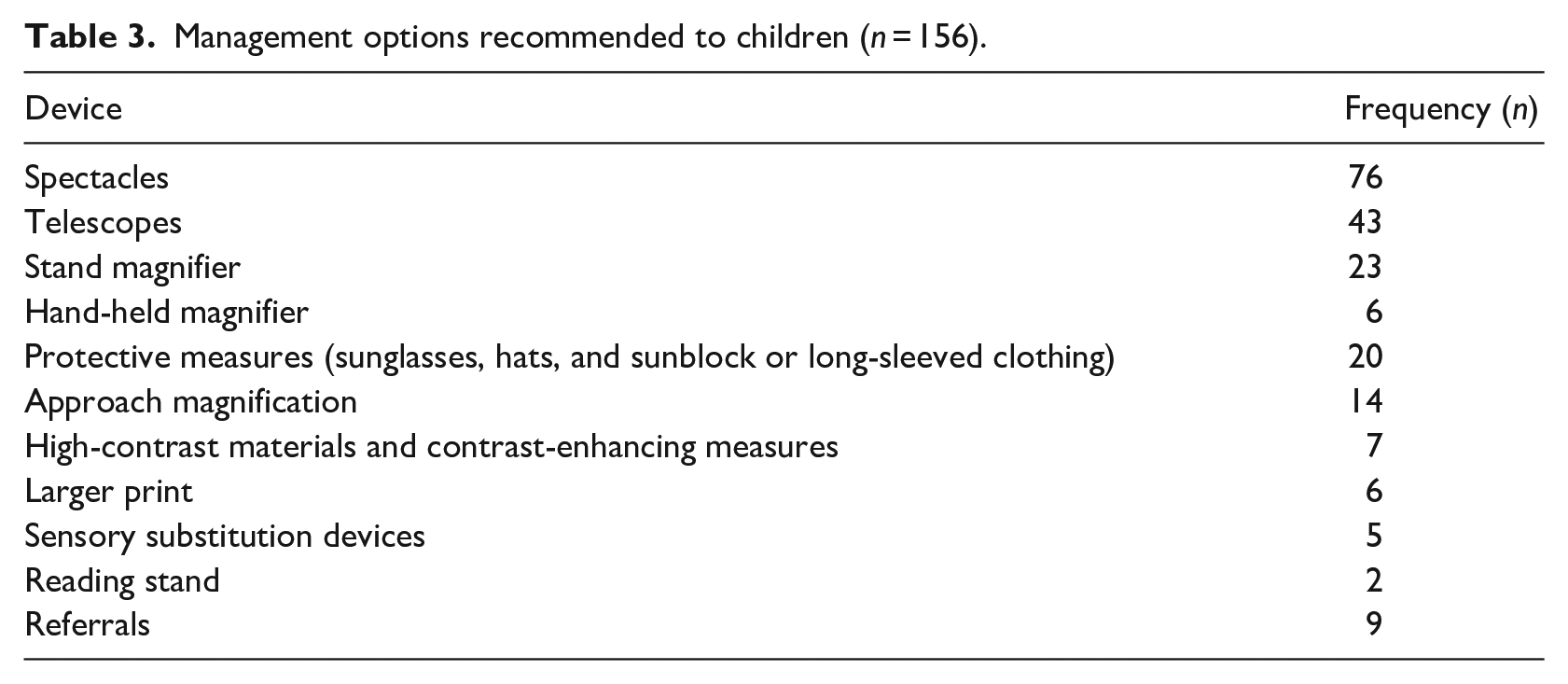
Spectacles, for distance and/or near, were recommended to about half of the children (n = 76, 48.7%). A total of 126 devices were recommended and comprised more optical (n = 72) than non-optical (n = 54) devices. Telescopes were the most common optical device recommended (n = 43) followed by stand magnifiers (n = 23). For the non-optical devices, protective measures (including sunglasses, hats, sunblock, and/or long-sleeve clothing) and approach magnification were the most common recommendations (Table 3). Nine children were referred to either ophthalmologists (n = 4, 2.6%), special schools that cater to children with vision impairment (n = 2, 1.3%), psychologists (n = 2, 1.3%), and/or occupational therapists (n = 1, 0.6%) (Table 3).
Management options recommended to children (n = 156).
Discussion
Vision is important for early learning, development, socialisation skills, self-esteem, and self-confidence in children (Augestad, 2017; Chandna & Gilbert, 2010). Consequently, vision impairment in children can have educational, developmental, emotional, social, and economic consequences for the affected child, their family, and society (Solebo & Rahi, 2014). The WHO and the International Association for the Prevention of Blindness identified the need to control for paediatric vision impairment, more specifically childhood blindness, as a key priority more than two decades ago (Gilbert & Foster, 2001). Accurate data on the prevalence, magnitude, and causes of vision impairment in children is necessary to plan and implement appropriate activities at primary, secondary, and tertiary levels of care to reduce the impact of paediatric vision impairment and minimise any functional limitations (Khanna et al., 2019). To this end, some studies have reported on children with vision impairment in population-based studies (Lu et al., 2009; Pandey et al., 2021). However, population-based epidemiological studies on paediatric vision impairment require large sample sizes and therefore significant human and financial resources are needed to execute these studies (Gyawali & Moodley, 2017; O’Sullivan et al., 1997). Other studies have reported on children in schools for the blind as a means to better understand the causes of vision impairment in children (Esra & Mayet, 2020; Gyawali & Moodley, 2017; O’Sullivan et al., 1997). Despite the usefulness of information from these studies, their samples may be subjected to selection bias and may not always include preschool children, affected children from rural areas, and children with multiple disabilities (Gilbert & Foster, 2001). Other clinic and hospital-based studies have reported on children with vision impairment in Nepal (Uprety et al., 2016), Eritrea (Gyawali et al., 2017) Australia (Du et al., 2005), England (Theodorou & Shipman, 2012), China (Gao et al., 2016), and Yemen (Bamashmus & Al Akily, 2010). In such studies, information about children with vision impairment can be obtained from clinical records with minimal human, financial, and time resources (Gyawali et al., 2017). Aligned with the research design used in the latter group of studies, this study identified the clinical characteristics and causes of vision impairment in paediatric patients who attended a university-based low vision eye clinic in KwaZulu-Natal, South Africa. In this way, this study provides detailed baseline data on the profile of children presenting for low vision examination and management services at this university-based clinic. Furthermore, this study contributes to the literature on vision impairment in younger individuals as there is a relative paucity of literature on paediatric vision impairment than adult vision impairment (World Health Organization, 2019c).
Albinism was the leading condition accounting for vision impairment and was observed in just over one-third of the sample (n = 54, 34.6%). There is a high prevalence of albinism in Africa than elsewhere in the world with rates varying from 1 in 5000 to 1 in 15,000 (Kromberg et al., 2020). Specifically for South Africa, it is estimated that 14,000 individuals have albinism and that the condition is more common in the Black population where 1 in every 4000 people have albinism (Kromberg et al., 2020). Other recent studies conducted in South Africa have also noted albinism as a common condition in their samples of individuals with vision impairment. For example, Esra and Mayet (2020) noted that 28 (15%) of the 189 children in a blind school in Johannesburg had albinism while Xulu-Kasaba et al. (2020) noted that 96 (47%) of the 204 individuals younger than 20 years attending a university clinic in a resource-limited setting had albinism. Albinism is an inherited genetic disorder and affected individuals often experience several visual symptoms (decreased vision, photophobia, impaired depth perception, and reduced contrast sensitivity) as well as discrimination, ridicule, and social challenges (Coleman, 2018; Kromberg et al., 2020). Genetic counselling services have been available in South Africa since 1997, and these services are intended to help affected individuals and their families to better understand the characteristics of albinism in terms of its prognosis, diagnosis, mode of inheritance, implications on the visual system, management options, and risk of recurrence (Coleman, 2018). Like other genetic conditions, albinism is not preventable, but genetic counselling can help to assess the risk of recurrence. For this reason, affected children and their parents should be encouraged to seek genetic counselling services that are available at the South African government departments. In addition, it would also be useful to investigate the effectiveness of the genetic counselling services that are currently being offered to people with albinism as such studies could provide opportunities to better understand the nature and usefulness of these services.
After albinism, the second most common cause of vision impairment was refractive error (n = 11). When this is considered with the proportion of children with amblyopia (n = 7), it suggests that greater emphasis should be placed on refractive services for children and provides further evidence for eye care policymakers to prioritise and implement more school screening programmes to earlier identify children with vision impairment in South Africa. This is because early identification of refractive error and correction with spectacles is an effective means to address the problems of reduced vision in children (Burton et al., 2021). Cataract and glaucoma were noted in 10 children each (6.4%) followed by retinitis pigmentosa and corneal opacity/scar that was observed in 8 children each (5.1%). Even though the number of children affected with cataracts and glaucoma in the present study (n = 20) compares favourably to that reported in other studies involving South African samples (Esra & Mayet, 2020; O’Sullivan et al., 1997) (n = 23–53), these conditions are potentially avoidable causes of vision impairment. This finding reinforces the need for early identification and referral to specialist paediatric care facilities to provide timely and appropriate surgical and/or medical treatment. Together with regular monitoring and provision of low vision rehabilitation services that cater for the changing visual demands because of progression throughout their schooling, these services can help to minimise the impact of conditions such as cataracts and glaucoma on affected children. In a recent study, Esra and Mayet (2020) reported that corneal scarring was found in 16 children and accounted for 8% of vision impairment in their sample. In an earlier study involving children enrolled in blind schools across South Africa, O’Sullivan et al. (1997) reported that corneal scarring attributed to vitamin A deficiency and/or measles infection accounted for avoidable vision impairment in 27 children (5%). The percentage of cases due to corneal opacity/scarring in the present study and previous studies in South Africa are lower than the percentages reported in studies in other developing countries (Gyawali et al., 2017; Gyawali & Moodley, 2017; Ilechie et al., 2020; Panda et al., 2020) (12%–24%) and may reflect the better levels of perinatal care and success of primary health care interventions aimed at measles/rubella immunisation and vitamin A supplementation in South Africa (Baker, 2010; du Plessis et al., 2007).
In the present study, the retina (n = 74, 47.4%) was the most common anatomical site causing vision impairment which is consistent with the trend noted in previous studies involving children in South Africa (Esra & Mayet, 2020; O’Sullivan et al., 1997). This finding differs from other studies where it was noted that the most common site was the lens mostly as a result of cataracts and aphakia in Eritrea (n = 55, 22.1%) (Gyawali et al., 2017) and Ghana (n = 75, 29.8%) (Ilechie et al., 2020). A study conducted in India noted that the most common site was the whole globe category mostly as a result of phthisis bulbi and microphthalmos (n = 83, 32%) (Panda et al., 2020). These findings corroborate the trend that specifically cerebral visual impairment in the normal globe category is not often observed in samples of children with vision impairment in developing countries. This contrasts with reports from developed countries such as Turkey (Ozturk et al., 2016), Australia (Du et al., 2005), and New Zealand (Chong et al., 2019) where cerebral visual impairment in the normal globe category was noted as most frequent. The difference between the site and associated conditions causing vision impairment between developing and developed countries may be attributed to factors including geographical area, socioeconomic status, and access to and availability of neonatal and/or eye care services (Chandna & Gilbert, 2010; World Health Organization, 2019c). The latter factor is particularly important for cerebral visual impairment as the provision of timely and efficient neonatal care is critical to the survival of low birth weight and preterm children.
Optical and non-optical low vision devices allow for better functioning in identified tasks through effective use of the device aimed at maximising the residual vision of the individual with vision impairment (Gao et al., 2016; Haddad et al., 2006). In this study, more optical (n = 72) than non-optical (n = 54) low vision devices were recommended confirming the trend that optical devices are more commonly prescribed (Theodorou & Shipman, 2012; Uprety et al., 2016). Telescopes were the most frequently recommended optical device and this suggests that visually demanding school tasks that require object recognition at distance (Theodorou & Shipman, 2012), such as reading the chalkboard and locating objects in the classroom, were more important for children. For near, stand magnifiers were the most commonly recommended optical low vision device as has been noted in other studies (Gao et al., 2016; Haddad et al., 2006; Uprety et al., 2016). Stand magnifiers are indicated for fluent reading tasks such as reading textbooks and worksheets that children often undertake as part of their academic activities at school. Participants likely preferred the stand magnifiers as they allow for hands free work which is important for near tasks that require turning pages and writing (Gao et al., 2016). The frequent recommendation of telescopes and stand magnifiers in the present study is not surprising as children with vision impairment reported that copying from the chalkboard, seeing details across the road, and reading printed textbooks at an arm’s length were the most challenging tasks at school (El Byoumi & Mousa, 2010). Consequently, as the telescopes and stand magnifiers would help to engage in visually demanding tasks at school, they would allow children with vision impairment to improve their participation and perform better in school-related tasks (Gao et al., 2016; Haddad et al., 2006). In the present study, only a few hand-held magnifiers were recommended (n = 6), and this may be explained by the optics of hand-held magnifiers that have to be held at a specific distance away from the object, corresponding to the focal length of the lens in the magnifier, for optimal focus and magnification (Jackson & Wolffsohn, 2007). Consequently, it may be more difficult for children with vision impairment to use hand-held magnifiers than stand magnifiers for prolonged fluent reading tasks at near.
Several non-optical devices and recommendations can assist individuals with vision impairment to improve their function and quality of life (Jackson & Wolffsohn, 2007). In this study, protective measures (n = 20) and approach magnification (n = 14) were the most commonly recommended non-optical devices. The high frequency of protective measures is likely explained by albinism being the most common condition causing vision impairment in this sample. As a result of the impaired melanin synthesis, individuals with albinism are susceptible to skin cancer and damage due to solar and ultraviolet radiation (Kromberg et al., 2020). This highlights the importance of appropriate advice on skin and eye protection in individuals with albinism which includes the use of long-sleeved shirts, sunglasses, long skirts or trousers, hats, and sunblock with an adequate sun protection factor (Kromberg et al., 2020). Approach magnification was the second most common non-optical recommendation and likely preferred when the distance magnification requirement was low and could be compensated for by children moving closer to the object being viewed. For example, children can sit in the front row of the classroom to better view the chalkboard without relying on any optical devices. Furthermore, children often have adequate amplitudes of accommodative and decreasing the object to eye distance at near can result in magnification (Haddad et al., 2006) without necessarily using an optical device. In this way, advice on approach magnification is a relatively easy and cost-effective way to provide magnification particularly for low amounts of magnification (2–2.5×). It is interesting to note that no electronic devices, which include closed-circuit televisions, desk-based and portable electronic magnifiers, were recommended to participants. This suggests that there may be limited availability or awareness of the usefulness of these types of devices as has been observed in low vision clinics in developing countries (Uprety et al., 2016). Furthermore, no recommendations regarding awareness, demonstration, or training on the accessibility features in devices such as smartphones, desktops, and laptops were noted. Consequently, the low vision curriculum at UKZN should be investigated to determine whether aspects related to electronic devices are included and necessary amendments made if needed.
Spectacles were the most common recommendation and prescribed to almost half of the sample (n = 76). This may be attributed to the finding that after refraction many of the children showed improvement in VA, compared with the presenting VA, and were classified with a different category of vision impairment using the WHO classification. Only 26.3% (n = 41) of children presented with spectacles at the time of the examination while spectacles were recommended to 48.7% (n = 76) suggesting that many children could potentially benefit from using spectacles. Other studies have also noted that spectacles are the most common management option used for children with vision impairment (Burton et al., 2021; Chong et al., 2019). These results indicate that refraction has the potential to make a difference in the VA and functional vision in children with vision impairment. This re-affirms the importance of accurate refraction and correction of distance refractive error and/or provision of near additions in children with vision impairment. Sometimes there is a tendency to omit refraction in individuals with vision impairment as the cause of reduced vision is often due to ocular and/or systemic pathology (Sunness & El Annan, 2010). The results of this study imply that correction of the refractive error would be the first step in the rehabilitation process as this can sometimes result in improved performance of tasks that involve recognition of details and navigation (Sunness & El Annan, 2010). Thus, refraction should be an integral part of the low vision examination as refractive error is common in children with vision impairment (Du et al., 2005; Pandey et al., 2021; Uprety et al., 2016). Furthermore, VA measurements are necessary for determining the distance and near magnification requirements needed for specific tasks. Using the VA measurements after best correction allows for accurate estimation of magnification without unnecessarily reducing the field of view with the latter occurring when magnification is overestimated. Therefore, it is important that eye care personnel, even those with limited training in the field of low vision, do not rule out the importance of refraction and provision of spectacles in children with vision impairment, especially as refractive services are relatively more accessible and affordable than low vision services.
The sample consisted of a similar number of males (n = 82) and females (n = 74) which is in contrast with other studies that noted a higher number of males in their samples (Bamashmus & Al Akily, 2010; Chong et al., 2019; Du et al., 2005; Gyawali et al., 2017; Uprety et al., 2016). Possible reasons for the gender difference noted in the latter studies include that parents of male children may give them more priority and therefore access eye care and educational services, females with vision impairment may have a higher mortality rate or males may be at a higher risk for some of the conditions that result in paediatric vision impairment (Bamashmus & Al Akily, 2010; Gao et al., 2016; Uprety et al., 2016). More than 92% of the sample were older than 9 years implying an older age at presentation for low vision examination services as has been noted previously (Gyawali et al., 2017). The older age of presentation could be accounted for by some of the conditions of vision impairment such as refractive error (in cases of pathological myopia) and retinitis pigmentosa that have a later onset. Furthermore, the higher number of older children may be explained by more than 80% of the sample being from schools that cater to children with vision impairment. Consequently, the requirements for undertaking visually demanding school activities such as copying from the chalkboard and reading at near (El Byoumi & Mousa, 2010) in these children may have prompted them to present for examination and management at the low vision eye clinic. The youngest child was 5 years and together with the low proportion of children under 9 years (n = 12, 7.7%) strongly suggests a limitation in the examination and management services offered at this university-based low vision eye clinic. Therefore, greater efforts are needed specifically targeting parental awareness campaigns and education as well as preschool vision screening to facilitate early identification, diagnosis, and management of children with conditions that have the potential to contribute to paediatric vision impairment.
Limitations of this study include the use of a clinic-based rather than population-based sample and therefore may not represent the entire population of children with vision impairment in KwaZulu-Natal. It is also possible that some children with vision impairment, possibly those with mild vision impairment, are being examined and managed by other optometrists and therefore would not need to present to the university-based low vision clinic. Furthermore, incomplete record cards with missing information and multiple examiners in a clinical setting can sometimes lead to information bias in retrospective studies. Despite these limitations, this study provides useful information that can be used to review and enhance the examination and rehabilitation services at this university-based clinic to better address the needs of paediatric patients with vision impairment that present to this clinic. Furthermore, it is recommended that this study be repeated at a subsequent interval of 5–10 years as this may help to assess for changes (if any) in the causes of vision impairment and/or clinical characteristics of children with vision impairment that present to this clinic. This information would be important for planning and implementing evidence-based services to continue to meet the needs of children that present to this university-based clinic.
Conclusion
This study provided local data on the clinical characteristics and causes of vision impairment in paediatric patients attending a university-based low vision clinic in KwaZulu-Natal. The findings indicated that the majority of the children were older than 9 years and from schools that cater to children with vision impairment. Albinism, refractive error, glaucoma, and cataract were the main causes of vision impairment. Overall, spectacles, telescopes, and stand magnifiers were the most common management recommendations. These results would be useful to eye care personnel involved in planning and providing services to improve the facilities offered for patients with vision impairment at this university-based low vision clinic. Consequently, university eye care authorities (clinicians, clinic committee members, and policy makers) involved in the monitoring and maintenance of the low vision eye clinic should use these results to ensure that the examination and management services provided are appropriate to the needs of children with vision impairment that present to this clinic. This is because early identification and effective management of children with vision impairment can help them to use their residual vision more effectively and improve their participation and quality of life.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.