
Abstract
In this autoethnography, the experience of being a patient in an ophthalmology clinic is explored, within the context of the Five Stages of Sight Loss Model. The author describes her lived experience of diagnosis and critically examines her experience of receiving treatment and care within an ophthalmology clinic. The literature focusing on supporting patient mental wellbeing in an ophthalmology clinic is considered, and a patient perspective on improving support for mental wellbeing is proposed. Consistent care, clinical skills, the interpersonal skills of the ophthalmologist, and shared decision-making with patients emerge as important factors. The concept of ‘embedded counselling’ is considered.
Keywords
Introduction
It is 1999. I am 6 months pregnant with my third child, and I am working full-time as a primary school teacher while managing a 3-year-old and a 2-year-old. Life as a working mom is incredibly busy. I am referred to the ophthalmology department after a routine visit to the optician, who has noticed some scarring on my retina and decides it is best for me to have it checked out.
Following a series of tests, the ophthalmologist delivers the news. I have a sight condition called Retinitis Pigmentosa (RP). I have never heard of it. I ask about potential treatments, only to be informed that there is no cure. It is a degenerative sight condition that will eventually lead to the complete loss of my sight. The timeframe for this loss is uncertain, as I have no family history on which to model a trajectory.
After the appointment, I go straight back to work. When my headteacher, who has been covering my primary three class, nonchalantly asks about the visit, I tell her, ‘I think I’ve just been told I’m going blind and there’s no cure’. She promptly has the classroom assistant take over, and she takes me to her office, where I break down and cry. The magnitude of my diagnosis began to hit me at that moment. My life, subsequently, implodes.
Methodology
This article is an autoethnography of my experience of being a patient in an ophthalmology clinic, within the context of the Five Stages of Sight Loss model (Thurston, 2010). In autoethnographic research, the researcher reflects on and analyses their own autobiographical experiences so they can contribute new knowledge to the research subject. Goodall (2000) describes it as, ‘the process of personally and academically reflecting on lived experience in ways that reveal the deep connection between the writer and her or his subject’ (p. 137). In compiling this autoethnography, I chose to include memories which were significant points in my sight loss journey, aided by written reflections and a scrap book of items collected over the years. Such introspection shares an intimate knowledge, which is based on lived experience, with others. This methodology was chosen then as it could facilitate a depth of engagement from me as both researcher and participant, allowing me to fully explore my unique perspective as a person with lived experience of severe sight impairment (blindness), a Reader in Counselling and Psychotherapy with a research interest in vision impairment and mental health, a counselling trainer in Higher Education and an ophthalmology patient. In addition, I am a cis-gendered, White, middle-class, educated, professional, Scottish woman. The complexity and uniqueness of these viewpoints inform my understanding. I hold both insider and outsider perspectives (Bukamal, 2022). There is currently a concerning paucity of patient perspectives informing ophthalmology treatment and care. Deans et al. (2017) discuss how the patient is uniquely placed to understand the impact of the disease and can use that position to transform ophthalmic care at the individual and collective level, from research to care delivery. Greenhalgh et al. (2015) assert that evidence-based medicine’s hierarchy of evidence tends to devalue the patient’s or carer’s experience. Fricker (2007), in her explanation of epistemic injustice, talks about, testimonial injustice, which occurs when prejudice causes a hearer to give a deflated level of credibility to a speaker’s word; and hermeneutical injustice which occurs at a prior stage, when a gap in collective interpretive resources puts someone at an unfair disadvantage when it comes to making sense of their social experiences. (p. 2)
I recognize both testimonial injustice in the experience of living with vision impairment and in trying to have my patient voice heard in an academic forum. The inaccessibility of the journal submission process alone provides an additional barrier. I also recognize hermeneutic injustice in the wider implications of a community whose voice is underrepresented in society. Overall, this autoethnography created a space for me to tell a silenced story that ‘need[ed] to be heard’ (Shoemaker in Adams et al., 2013).
Key ethical challenges with this methodology involve protecting the researcher’s privacy and confidentiality and protecting the confidentiality and privacy of nonactive participants. In considering my own privacy, I took note of Tolich’s (2010) warning to consider the permanency of what I might commit to sharing in this paper by presenting initial versions of my experience of sight loss to a range of audiences to see how it felt. I also shared early drafts of this paper to trusted colleagues to trial my comfort with it being read publicly. Guided by relational ethics (Ellis, 2007), the nonactive participants were consulted prior to writing starting, were able to read the paper before publication, and consented to being included in potentially identifiable ways in the study. The project received ethical approval from the university ethics committee.
The structure of this autoethnography follows a timeline of my diagnosis, as I describe my lived experience and critically analyse my experience of receiving consistent and compassionate care from my ophthalmologist. I explain the development of the Five Stages of Sight Loss Model (Thurston, 2010) and use it to frame my own lived experience, with reference to literature. The literature on supporting patient mental wellbeing in ophthalmology clinics is considered and suggestions for improving support for patient mental wellbeing are proposed. My voice is represented in passages of italics.
2001: decimation
Within a year of diagnosis, I have:
Stopped driving.
Stopped working.
Stopped socializing.
Stopped functioning.
Stopped mothering.
Lost my earnings.
Lost my house.
Lost my identity.
Lost hope.
I lose years to a deep depression, for which I’m prescribed anti-depressants. Despite the practical support offered to me during that time, like a liquid level indicator and a long cane nobody asks me how I’m feeling. Reflecting on that now, it seems inconceivable that the focus of support was entirely function-orientated, given the annihilation of my life that followed my diagnosis.
2004: wanda
Four years later, I am partnered with a guide dog called Wanda. Training with Wanda is perhaps my lowest point. Before then, I have been able to conceal my blindness. I am reluctant to use my white stick, hiding it in my handbag or in the pram hood when I am out and about. A guide dog means that I become publicly ‘blind’. I can no longer hide my lack of sight. The initial months prove tough as I adapt to the routine of harnessing Wanda before setting out. In some ways, I feel like I am the one wearing the harness, as the spontaneity of just getting up and going has become a thing of the past. I try counselling at this time, but I am unable to articulate the magnitude of what has happened to me, and I feel like a failure.
However, with time, a remarkable transformation unfolds. I notice that people are not just accepting of Wanda, they are drawn to her, warmly anticipating our presence during our outings. Wanda seamlessly integrates into family life, participating in disco dancing classes and swimming lessons with the kids, skilfully navigating me through the bustling school playground during nursery drop-offs. Her exceptional qualities are recognized when she becomes the first UK Guide Dog of the Year. The resulting media attention plays a pivotal role in the restoration of my confidence. I start a night class in counselling, figuring that this might be a career that will not be sight dependent. I can listen to people. I go on to complete an MSc Counselling, winning British Association for Counselling and Psychotherapy New Researcher prize (2009) for a qualitative project about the emotional impact of sight loss. Subsequently, I discover a new career in academia, securing a full-time lecturing post in Counselling (2010) and completing a PhD (2016).
2010: the emotional impact of sight loss project
My first research project lays the foundation for the development of my subsequent research career. I interview 18 adults to explore the emotional impact of their sight loss, focusing on four core areas: mood, self-concept, social connectedness, and loss (Thurston, 2010). I am keen to know if others had a similar experience to me. The key themes that emerge from the interviews include the challenges of receiving a diagnosis, coping with degenerative sight, undergoing a change in identity, engaging in rehabilitation, encountering others, and experiencing multiple losses. The findings of this study provide insights into the emotional experiences of individuals facing sight loss and show me that my experience of the emotional impacts of sight loss has not been unique. From the findings, I am able to identify a model which offers a way to make sense of the process of acquiring sight loss (as opposed to being born without sight). The model consists of five distinct stages. Initially, I call the model, ‘The transition from sight to blindness’ (Thurston et al., 2010). However, after many presentations, it becomes commonly known as, ‘The Five Stages of Sight Loss’, which is a more accessible and useable title. Since its conception, there have been more recent studies (Boagey et al., 2022; Ferrey et al., 2022, 2024; Partow et al., 2021; Rai et al., 2019) which support each stage of the model. Future research is needed to understand if and how intersectionality is accommodated by the model and to develop a model of acquired sight loss for children and young people.
The five stages of sight loss
Stage 1: the diagnosis
The model begins with the diagnosis of an eye condition, resulting in serious visual impairment. Whether this is out-of-the-blue or whether it has been long awaited, the common emotional responses include shock, panic, and fear. People look to health care professionals for information, practical insights, and emotional reassurance, such as finding out about the origins and prognosis of the condition, symptoms, treatments, ongoing research, practical lifestyle adjustments, and how to cope emotionally with life with a visual impairment. Ferrey et al. (2022) explored the impact of diagnosis by interviewing 18 visually impaired people in England. Four themes related to patients’ experience of diagnosis were identified: the convoluted process of being diagnosed, the impact of clinicians’ words, and the search for information and reflections on what could be improved (Figure 1).
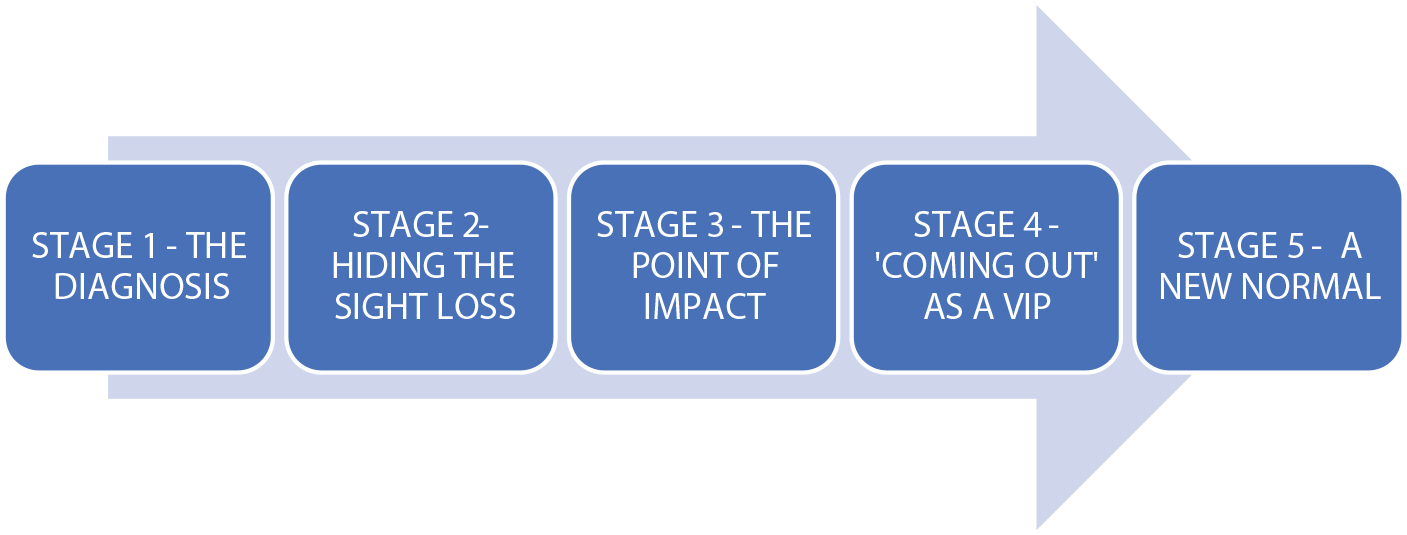
Five stages of sight loss model (adapted from Thurston, 2010).
Stage 2: hiding the sight loss
During this stage, a person uses strategies to hide their sight loss, rejecting or resisting using visible aids such as a ‘white stick’. There is a desire to carry on with life ‘as normal’. Engagement with rehabilitation services is typically unsuccessful during this phase, as using low vision aids signifies an acceptance of the visual impairment, which, in turn, means a profound redefinition of identity from a sighted person to a blind person. Ferrey et al. (2024) concur that a person’s identity needs to be renegotiated after receiving the diagnosis of a condition leading to vision loss and that, unlike many other disabilities, people with a vision impairment can choose whether to disclose their disability to others. They may choose to avoid any chance of disability-related stigma and attempt to maintain their identity continuity by presenting as nondisabled as much as possible. Boagey et al. (2022), in a qualitative study examining the psychological impact of sight loss, also identified denial as a subtheme of coming to terms with the diagnosis, but the challenge to identity continuity is a more nuanced explanation of the reason behind denial.
Stage 3: the point of impact
Stage 3 signifies a point where the impacts of sight loss start affecting the person’s life tangibly, leading to enforced lifestyle changes, such as the loss of a driving licence or being no longer able to get out and about. Losses at this stage can be practical, emotional, and aspirational. Consequently, the person grapples with the challenging realization that life can no longer be lived as it once was. Socially and emotionally, the point of impact is an exceptionally demanding phase, given the enforced alterations to life due to visual impairment. In a qualitative study about the psychological impact of vision loss, participants identified a range of losses associated with their vision loss, such as loss of purpose in life, loss of hobbies, and loss of career prospects, all of which negatively impacted their mood (Boagey et al., 2022). The following poem illustrates the point of impact. It was compiled verbatim from anonymised transcripts (Thurston, 2010) where nine visually impaired people shared their experiences of loss: There is a great loss and it’s like a bereavement. You know it’ll never be there again. It’s gone forever. You feel as though someone’s chipped a bit out of your heart and your soul. You think something’s gone and you’ll never see it again. It’s like when you lose someone close to you because you are losing a sense. You go through the anger, you go through the bitterness and then you come out of that and you do, you grieve over what you are losing. I was grieving, but I kept it into myself. As your sight gets worse, you are losing all the time, because you are losing your independence and you’ve got to have help which makes you lose your pride, and that takes down your self-esteem. I think driving is still the biggest loss, you know the independence of driving. The freedom to say, Oh well, let’s just go off to the Lakes or the Highlands for the weekend. You know, You’ve lost that. You don’t have the freedom to jump in the car and drive somewhere. So often you are waiting for somebody to come and give you a lift somewhere. You do spend time sitting there. Not being able to read to the grandchildren is a huge loss. I just can’t do the things I used to do. That’s it every day’s the same. I’m bored. I would like to be able to work in a charity shop, but I can’t because I can’t see the money. I was intending to go away to work in Asia first and then on to New Zealand. I was going to take my partner and my kid over, but that got hit on the head. I used to go to football and all that, but I can’t go there now. You do think from time to time, Oh yes, this would have been a lovely day, or I could just be cantering up here, you know a nice grassy path. I used to love going to see the opera, but I didn’t go this year because, I can’t see a damn thing. It’s not the same when you can’t see it. So what’s the point? You don’t see your grandchildren or places you visit. It makes you depressed if you think about it You lose everything in a oner It’s just life itself is loss. To know what the heck to do. You know, you get bored stiff in your own four walls. You say to yourself, What can I do? and you look at yourself and you say Sit there and shut up because you can’t do anything. You know it’s frustrating With disabilities, people say, They’ll get a few quid in benefits, but I mean it is nothing to what you’ve lost.
Stage 4: coming out as a visually impaired person
When there is engagement with rehabilitation services, such as using a white cane, a guide dog, or other low vision aids, the person enters a challenging phase, both socially and emotionally. This transition involves accepting a new public identity as a visually impaired person (VIP), which can lead to firsthand encounters with disability discrimination or societal marginalization. People, generally, display awkwardness in their interactions with those who have sight loss, which can make the person with sight loss feel like they no longer belong to society, in the way they once did. This may also trigger their own internalized societal prejudice about visual impairment. In a qualitative study by Partow et al. (2021), participants reported a lack of control and feelings of hopelessness and helplessness over stigma-related encounters.
Stage 5: establishing a new normal
This stage signifies an acceptance of sight loss. This may be through the re-conceptualization of one’s identity or perspective on the vision impairment, resulting in the establishment of a ‘new normal’. Various coping strategies can be employed, such as contextualizing the eye condition in comparison to life-threatening illnesses, adopting an optimistic outlook, or recognizing the unexpected positive life changes brought about by sight loss. Rai et al. (2019) found that people with vision impairment used multiple strategies to cope with their disability and that positive coping strategies were associated with a better general functioning and better psychosocial quality of life. Stage 5 also holds potential for personal growth and flourishing. Indeed, Barskova and Oesterreich (2009) suggest the possibility of post-traumatic growth in adaptation to chronic health conditions.
A flexible, nonlinear process
The model is not prescriptive; rather, it constitutes a flexible conceptualization of a process, which is not strictly linear in its progression, as implied by the graphic. For example, a person with a diagnosis might be advised by their consultant to stop driving. If they work, say, as a taxi driver, this will have an immediate impact on their employment, due to the loss of driving capability. There would be no ‘hiding’ stage, as ‘the point of impact’ would come simultaneously at diagnosis. Conversely, someone in a long-term relationship might experience a gradual onset of sight loss over several years, with the consequential impact significantly affecting their life only after the death of their partner. The point of impact for this person might come years after Stage 5 had been reached.
Emotional support
The Five Stages of Sight Loss model highlights the nuanced nature of emotional support required at distinct points in the process of sight loss. For instance, frontline support provided by an Eye Clinic Liaison officer, who is employed in hospital settings to provide emotional support, practical support, and signposting for patients, may prove instrumental in aiding individuals coping with the shock of diagnosis during Stage1 (Menon et al., 2020; Trott et al., 2023). Counselling emerges as a potential resource during Stage 3, aiding individuals in identifying and managing the multifaceted losses incurred (Thurston et al., 2013). In Stage 4, counselling may facilitate an exploration of feelings regarding the shift in identity, while peer or group support may impart practical coping mechanisms. Those who become ‘stuck’ in Stage 3 may be particularly susceptible to chronic depression or suicidal ideation. A Finnish study revealed elevated suicide levels among the visually impaired (Kim et al., 2023).
I will return to my own journey to further exemplify the cyclical aspect of the model and how ophthalmologists may have a role to play in supporting patient mental wellbeing.
2020: back to Stage 3
For many years, I have identified as being in Stage 5. I am living a rich and fulfilling life, which holds meaning and purpose for me. However, in 2020, I find myself catapulted back into Stage 3 (The point of impact). I am diagnosed with a basal cell carcinoma on my bottom eyelid. I fear the procedure and possible disfigurement which might result. The challenge of daily living with limited sight reduces my capacity to cope with this new health development, and I find myself fearful of my future. This is further compounded by the COVID-19 pandemic. Everything in my world changes. Routes I have previously learned about are decimated and replaced by one-way systems. Bus interiors are reorganized, using black and yellow hazard tape to block off seating. My lectures move to being delivered online, and I must learn to navigate a new virtual world. Societal changes, social distancing, and navigating a brand-new world, lead to my increasing vulnerability.
Amid this vulnerability, 2021 necessitates a decision about cataract surgery. RP cataracts can be complicated and, as well as fearing the procedure itself, I also fear the risk of further deterioration. It feels like a ‘stick or twist’ situation. There is no clear best option. If I do not have cataract surgery, I lose the little residual sight in that eye, but if I opt for cataract surgery and it goes wrong, I also risk losing the little residual sight in that eye. Navigating me through this impossible decision is my consultant ophthalmologist.
2021: consistent care and compassionate support
During the turbulence of the COVID-19 pandemic, my ophthalmologist supported me through the removal of two basal cell carcinomas, one from each eyelid, and a cataract removal with subsequent postoperative cystoid oedema. She performs all the surgeries herself. In understanding how ophthalmologists might better support patient mental health, I reflect on what makes her such an exceptional ophthalmologist and how might this be replicated in the treatment of other patients. From the perspective of patient and counselling trainer, I identify the clinical and interpersonal skills that positively support my mental wellbeing during treatment.
Collaborating over treatment options
She created a climate of collaboration during consultations, and I was actively involved in determining my treatment options. Options were meticulously explained, and the associated risks were clearly laid out for me to consider. Often, I vacillated between options, looking to her for guidance. On these occasions, the pace of the consultation slowed, so that I might have time to listen again to the options and have space to think. She created the illusion of time. Eye clinics are always busy, but she gave no sense of being time pressured. Sometimes another consultation was scheduled so that I had time to reflect on treatment options with my family and friends. This climate of collaboration helped empower me. I felt involved in my own treatment. She flattened the power differential between clinician and patient, where the patient is ‘done to’ not ‘done with’. We were a team. We were in it together. I got the feeling she cared about that.
Clinical skills
She was an exceptionally skilled clinician. After the removal of the carcinoma, every time I looked in the mirror, I was reminded of her handiwork. I had been most fearful of facial disfigurement, and her skilled reconstruction of my eyelid allayed this fear. Through extended dialogue, she had known how important a good cosmetic result was to me, and she was able to deliver this.
By the time it came to my cataract surgery, I had absolute trust in her clinical skills, and this got me through my fear barrier. During the cataract surgery, I was aware that she was using a variant of Emotional Freedom Technique (EFT) tapping techniques (König et al., 2019) to help alleviate my pain and anxiety. As she was administering the injection into my eye, she tapped on my eyebrow, the side of my eye, under my eye, under my nose, and on my chin. This technique has been used with some success in a variety of clinical settings (Stapleton et al., 2023). She understood my anxiety, and she cared about making the procedure as painless as possible for me.
Interpersonal skills
She was a skilled and empathic listener who was able to build a collaborative and trusting relationship in which I could explore my fears and distress about treatment options. When I was talking, she attended herself towards me using a SOLER model (Egan and Reese, 2019). This is where the listener sits positioned squarely to the talker, maintaining an open posture and leaning slightly in towards the talker, while maintaining eye contact in a relaxed way. This signalled that she was attending to what I was saying, rather than being occupied by reading notes or typing. She cared about listening to what I had to say.
She was warm, compassionate, approachable, and easy to talk to. She was unassuming and generous in her praise for her colleagues. The working atmosphere of the team around her was happy and relaxed. I have no doubt she created this.
Discussion
The mental health impacts of sight loss
A survey by Enoch et al. (2019) found people fear losing their sight more than any other of their senses. Therefore, the diagnosis of a sight condition can be a fearful prospect which significantly impacts negatively on mental health (Ferrey et al., 2022; Garcia et al., 2017). The link between depression and sight loss is a global issue. Holloway et al. (2018) found depression was common in low-vision rehabilitation clinics in Australia. An Italian study by Parravano et al. (2021) found depression in patients with visual impairment was a common problem that should be recognized and addressed by the health care professionals treating these patients. Hesterbeek et al. (2017) in the Netherlands found that the incidence of depression and anxiety in older adults with vision impairment is twice as high compared with older adults in general. Nollett et al. (2016) found that people in the United Kingdom with vision impairments are a high-risk group for depression. Three-quarters of those who screened positive for depression in a Low-Vision Clinic were not receiving any form of treatment, suggesting that depression is being routinely overlooked. In a USA study, Cimarolli et al. (2016) found significant numbers of older adults with AMD experienced depression and anxiety. Tantirattanakulchai et al. (2022) found a high prevalence of suicidal ideation among older people with vision impairments. Lee et al. (2022) investigated the association between visual impairment and suicidal ideation, plans, and attempts among 214,505 adults in the United States. Compared to their cited peers, a relatively high proportion of adults with vision impairment had serious thoughts about suicide, suicide, plans, or suicidal attempts in the preceding year.
Acquiring a guide dog
Sanders (2000) asserts acquiring and being assisted by a guide dog changes the identities of people with visual impairments. Guide dog owners report that the dog can increase their health and independence and facilitate social contacts (Glenk et al., 2019). A systematic review by Rodreguez et al. (2021) found that having an assistance, dog was associated with improved psychosocial functioning among individuals with disabilities. Positive findings were identified in all domains and subdomains of psychosocial, health, and wellbeing.
Cancer treatment
Deshpande and Ghooi (2017) concur that fear of possible disfigurement from cancer treatment is a concern for most patients, while Suzuki et al. (2016) report it may cause anxiety and depression.
The impact of the COVID-19 pandemic on people with vision impairment
Shalaby et al. (2021) interviewed individuals across the spectrum of vision impairment in a cross-sectional comparative study to assess the implications of COVID-19 for individuals with vision impairment compared to those without vision impairment. Serious concerns about general health, mental health, and essential activities were more commonly reported among individuals with substantial vision impairment, suggesting that this population was disproportionally affected by the COVID-19 pandemic.
Cataract surgery
Muley et al. (2020) used the Hospital Anxiety and Depression scale to attempt to quantify the patients’ anxiety about cataract surgery. They reported that increased anxiety preceded the first cataract operation and that female patients were marginally more anxious than their male counterparts.
Patient voice
Dean et al. (2017) argue for a greater value of the patient voice in medical research and clinical practice so that priorities might better align with the needs of those who have lived experience of the disease.
Ophthalmologists as a source of support
An analysis of survey data (Garcia et al., 2017) from patients with vision impairment supports the potential role of ophthalmologists in providing support for their patients’ mental wellbeing. More than half of the survey respondents (52.4%) identified ophthalmologists as a source of emotional support. However, the idea of emotional support varies among individuals, and the ways in which ophthalmologists offer such support differ. For example, emotional care from ophthalmologists could be direct, involving active counselling or attentive listening, or indirect, providing patients with clear answers and knowledge about their condition and perhaps signposting other sources of emotional support. The data from this survey show the significant potential for ophthalmologists to play a role in the emotional care of patients with sight loss, which may currently be overlooked in eye care clinics.
Shared decision making in ophthalmology
Bouaziz et al. (2022) reviewed the literature about shared decision-making in ophthalmology and reported that, although there are challenges to this, associations have been made regarding improved patient outcomes as a result of doing with the patient, not doing to the patient. Kuhn & Gryzbowski (2022) state that paternalistic medicine, where the doctor knows best and will tell you what treatment option they chose, has no place in contemporary practice and that any reasonable patient who has been properly informed about the condition, the risks and benefits of surgery, and the consequences of not undergoing surgery can make the correct decision for themselves.
Communication skills in ophthalmology
Walkden (2023) concurs that health care professionals should make every effort to listen to patients’ stories. There has been previous examination of the benefits of including communication skills in ophthalmology training. Vegni and Moja (2004) evaluated the efficacy of a communication skills course for ophthalmologists in a pilot study. After the training, their participants reported becoming more attentive to patients′ psychosocial needs, both in terms of general quality of consultation (patient-centeredness) and in terms of using specific interpersonal skills. In a survey of the Canadian Ophthalmological Society, Zakrzewski et al. (2008) found that most respondents believed it is important for ophthalmologists to communicate effectively when breaking bad news. A more recent review focuses on training ophthalmologists to break bad news (Hilkert et al., 2016); however, there is little research about the impact of the ophthalmologist’s interpersonal skills and personal qualities in relation to supporting patient mental wellbeing.
There are recommendations across the literature that counselling, emotional support, and mental health interventions can be helpful to people with vision impairment and that ophthalmologists and ophthalmology clinics may have a role to play in developing service provision for patients (Demmin & Silverstein, 2020; Garcia et al., 2017; Parravano et al., 2021; Rai et al., 2019). Integrating emotional support into ophthalmology clinics offers holistic care, which is more accessible to patients. Given the profound impact of sight loss on mental wellbeing, this critical aspect often remains overlooked within current service frameworks and provisions (Barrow et al., 2018).
To address this, an understanding of the psychological impact of sight loss could be introduced into ophthalmology training. Developing skills in effective communication, empathy, and recognizing signs of mental distress during patient interactions might also be beneficial in helping ophthalmologists better support patient mental wellbeing. McLeod and McLeod (2014) provide an overview of research evidence on the concept of ‘embedded counselling’, where counselling skills are used effectively within the context of other professions such as health care, teaching, or social work. There is much to be learned from this article. Using embedded counselling, the ophthalmologist might make use of windows of opportunity within clinical consultations to afford patients the opportunity to express their emotions and work through their fears about diagnosis or treatment.
In addition, consistency of care, through allocating patients to one named clinician, might support the development of a trusting relationship where patients feel comfortable expressing their fears, concerns, and emotional challenges and can collaborate over treatment options.
Encouraging collaboration between ophthalmologists and researchers in the field of mental health and sight loss might contribute to increasing evidence-based practices in this area.
Limitations
I shared a draft of this article with some ophthalmology consultants, who recognized the stages of sight loss and felt moved by my patient account. They thought it would be good for their colleagues to read, and they acknowledged the challenge of implementing such changes. They commented on the two-way nature of the patient–ophthalmologist relationship, recognizing that certain relationships worked better than others, depending on the match between patient and ophthalmologist. They highlighted the broader team around the ophthalmologist (nurses, photographers, porters, support workers, etc.) and likened it to ‘a big family’, each of whom possessed a different and yet valuable skill set and, all of whom might have a part to play in supporting the mental wellbeing of patients. They also questioned if compassion/empathy could be taught, or whether it was an innate personal quality. Further consultation with ophthalmologists, nurses, support workers, and patients should be sought so that all perspectives might inform a compassionate and effective model of supporting patient wellbeing within ophthalmology clinics.
Conclusion
I have used the Five Stages of Sight Loss as a lens through which to view my lived experience of acquiring a visual impairment and my experience of being a patient in an ophthalmology clinic. From a patient perspective, I have highlighted the emotional complexities inherent in diagnosis and treatment. Consistent care in ophthalmology clinics, combined with clinical skills, the interpersonal skills of the ophthalmologist and shared decision-making with patients emerge as important factors in supporting patient mental wellbeing. The concept of ‘embedded counselling’ may also be helpful.
Footnotes
Acknowledgements
The author acknowledges Dr Helen Murgatroyd for her consistent and compassionate care, which was the inspiration for this paper. The author also acknowledges Dr Paul Johnstone, Professor Tariq Aslam, Amanda Hawkins, Fiona Stirling, Julia McLeod, Professor John McLeod, and Professor Andrew Reeves for their encouragement and support in shaping her ideas.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Abertay University, School of Applied Sciences Ethics Committee gave full ethical approval for this project on 19 October, 2023 (approval no. EMS7395).