
Abstract
Over the past decade, there has been increasing interest in advanced secondary mobility aids for people with low vision, such as sensory substitution devices (SSDs) and electronic travelling aids (ETAs). However, these new modalities have not been able to reach end-users in significant numbers. We conducted an online survey to investigate the current uptake of mobility aids, as well as perspectives on emerging technologies from people with inherited retinal disease (IRD). The cross-sectional survey received 74 complete responses from Australians that self-reported as legally blind from IRD. Approximately half (57%) of respondents were aged over 55 years, with the cohort exhibiting above average education levels (with half holding a bachelor’s degree or above). Long canes (54%) are currently the most used primary mobility aids in this cohort. However, around half of the respondents have used ETAs or SSDs (51 %) for additional help. Respondents reported that their choice of mobility aid was often based on whether they were in a familiar or unfamiliar environment. Most respondents showed interest in SSDs, but were concerned about usability and aesthetics. This cohort of people living with IRD in Australia was interested in advanced technologies and showed willingness to try novel mobility aids if the device was easy to use and the quality of training was guaranteed. Respondents indicated a preference for devices which were portable, and had a minimally intrusive form-factor. Our results can inform the research and development of emerging assistive devices. They serve as valuable guidance for selecting aids tailored to the needs of individuals with visual impairments. Future assessments on the effectiveness of low vision aids should include not only the functional improvement, but also participant-reported assessments regarding usability and portability, as these aspects dictate integration of the device into regular use.
Introduction
In Australia, a person is considered legally blind if they have best corrected visual acuity of less than or equal to 6/60 in the better eye or a visual field of less than 10° from fixation. Inherited retinal diseases (IRDs) are ocular disorders that are passed down from one generation to the next through genetic inheritance and are the most common cause of legal blindness in the working-age population in Australia (Heath Jeffery et al., 2021). IRD may lead to a wide range of visual impairments or abnormalities, including night blindness in retinitis pigmentosa (RP) and central vision loss in Stargardt disease. Vision loss is also the third highest-ranked reason, after arthritis and heart disease, that people need assistance with their activities of daily living (Şahlı & İdil, 2019). Many aspects of daily life may be affected by impaired vision, including orientation and mobility, participation in social activities, and remaining productive in work and personal development.
Mobility aids are devices designed to help people with visual impairment to navigate their physical environment more safely and independently. To date, long canes and guide dogs are still the most used primary mobility aids (Markoski, 2019). A primary mobility aid is a stand-alone device capable of detecting drop-offs independently, whereas a secondary mobility aid requires use in conjunction with a primary mobility aid to detect drop-offs. Long canes are often thought of as ‘obstacle detectors’, whereby people with visual impairment can use the cane to identify and hence avoid objects in their path. Conversely, guide dogs work as an ‘obstacle avoider’, where the dog will guide the person around objects and to desired locations in a safe manner. However, users have reported limitations for both of these primary mobility aids, including the fact that the long cane is unable to detect head height obstacles (Manduchi & Kurniawan, 2011) and that guide dogs need intensive training and maintenance (Jackson, 1995). There is room for improvement for both aids; for example, high-tech add-ons for canes and enhanced training programmes for guide dogs could be helpful.
Recently, a growing number of individuals with impaired vision have tried electronic travel aids (ETAs), such as smartphones and ultrasonic guides, as secondary mobility aids (Tapu et al., 2020). These devices offer additional information about the environment when used in conjunction with their long cane or guide dog. For example, the GuideCane™ is equipped with ultrasonic sensors for detecting obstacles ahead. Smartphone applications, such as Google Maps™, are very popular within the Australian low vision community, offering additional navigation information, including route planning and bus schedules (Deverell et al., 2023).
Sensory substitution devices (SSDs) are a new generation of ETAs. SSDs capture visual information in the environment and deliver it to the user via another intact sensory modality (e.g., auditory; Dakopoulos & Bourbakis, 2009). Generally, SSDs can be categorized by how the visual information is acquired and how the information is then conveyed to the user. The most widely used input sensors are optic cameras and ultrasound transducers (Bourbakis, 2008; Bousbia-Salah et al., 2007; Dakopoulos & Bourbakis, 2009). The information then can be delivered to the user via auditory or tactile feedback. For example, a software called ‘vOICe’ converts the video feed from a camera into corresponding ‘soundscapes’ (Ward & Meijer, 2010). Another commercially available SSD, BrainPort™, transforms images captured by the camera into electro-tactile stimulation via an electrode pad placed on the tongue (Danilov & Tyler, 2005). One advantage of SSDs is that all major components (i.e., visual-capture device, processing unit, and human–machine interface) can be upgraded as required, to improve overall performance as well as provide a personalized experience for users.
SSDs have been investigated in the lab environment for studying neural plasticity (Bubic et al., 2010). However, there exists a substantive gap between a research prototype and a commercially viable mobility aid. The life cycle of such research prototypes tends to be short, and many are never commercialized, hence little is known about the end-users’ attitudes towards such prototypes. It is therefore important to understand the current uptake of mobility aids, and end-user perspectives on emerging mobility assistance technologies, to inform not only rehabilitation services, but also to appropriately direct resources into the mobility aids that people will want to use.
The aim of this study was to capture information on currently used mobility aids (both primary – such as long canes and guide dogs, and secondary – such as ETAs), and user perspectives on emerging SSD technologies (which are not yet available commercially). Cohort selection was restricted to people living with IRDs in Australia, to ensure there were no significant differences in visual aid access, funding, and health systems. We focused on those who are defined as ‘legally blind’, since certain supports such as government welfare (e.g., the Disability Support Pension and the National Disability Insurance Scheme) are only accessible to those with best-corrected visual acuity of less than 6/60 or visual field restricted to less than 10° (Luu et al., 2020).
Methods
Survey development
We formed a multidisciplinary team, including two optometrists (R.J. and L.N.A.), a biomedical engineer (M.A.P.), a computer scientist (C.D.M.), a physiotherapist (J.L.M.), and a qualitative researcher (F.F.), to develop a survey. It was used to investigate current uptake of standard low vision mobility aids and end-users’ acceptance level of new SSDs. We started our questionnaire development by conducting an extensive literature review regarding low vision and mobility aids. We adapted mobility questions from an existing Australian instrument, which was previously used to report use of technology by low vision cohorts (Deverell et al., 2023), and Likert-type scale scoring (Nemoto & Beglar, 2014). The questionnaire was designed for a maximum duration of 15 min and was only available in English. Survey questions were developed with input from our multidisciplinary research team, and then assessed for face validity by a small group of Australians classified with legal blindness from IRD (n = 3).
The questionnaire contained four sections: (1) demographics, (2) currently used low vision mobility aid/s, (3) perceived advantages/disadvantages and important features of commercially available low vision mobility aids, and (4) attitudes to emerging SSD designs. The SSD design options were selected to cover a wide range of technologies, including audio and tactile output. We included characteristics of both commercial devices and those still in research and development stages. The survey was included as Appendix 1. After reviewing the piloted data, some of the questions were modified. The resulting survey was conducted online using Qualtrics survey software (Qualtrics, Provo, UT).
Respondents
Between May and August 2021, the Qualtrics survey link was distributed via email to the support and advocacy services of Vision Australia and Retina Australia. Other potential respondents were identified through an IRD registry led by L.N.A. (Britten-Jones et al., 2022) and also invited to participate via email. Inclusion criteria included being an Australian resident (to ensure healthcare systems were similar), having a diagnosis of an IRD, and having been classified as legally blind (<6/60 or less than 10° of visual field). These criteria were explicitly asked in the survey, and we relied on self-report of the respondents. Ocular diagnosis and visual status were not independently confirmed. No other criteria were applied. We used an anonymous online survey, which included a study in plain language statement and informed consent form on the first page. Respondents could choose to complete or not and were given no incentive for participation and could only complete the survey once.
The majority of surveys were completed online (n = 73, 98.6%), but we did offer the option to complete the survey over the telephone for one respondent who preferred this modality. In both cases, informed consent was obtained before data collection commenced. The survey was open for 12 weeks. The project was approved by the University of Melbourne Human Research Committee (reference ID 2021-21234-15988-3).
Data analysis
We applied mixed-method analyses to the data. The online survey data were exported to Excel and SPSS from Qualtrics. Missing data were checked, and descriptive statistics were generated for demographic data. Inferential statistics were used to identify differences between different devices. Thematic methods were applied to process free-text answers (Tuckett, 2005). First, we identified the segments of raw data (i.e., survey free text answers) and assigned descriptors (i.e., codes) to text segments. Based on these segments, we further generated categories and grouped initial codes into categories which hold together a group of similar codes. This process was recursive and initially done by the first author (R.J.), and then independently by an experienced qualitative researcher (F.F.), with any difference in coding discussed and resolved.
For answers to self-rating and Likert-type-scale questions, the central tendency was determined by the average rating of all respondents. For each statement, their degree of agreement was computed by the average rating number of all respondents. The absolute value of number indicated how strongly the view was towards that opinion. The study’s reporting followed the Checklist for Reporting Results of Internet E-Surveys, commonly known as ‘CHERRIES’ (Eysenbach, 2004).
Results
Demographics and mobility aids status
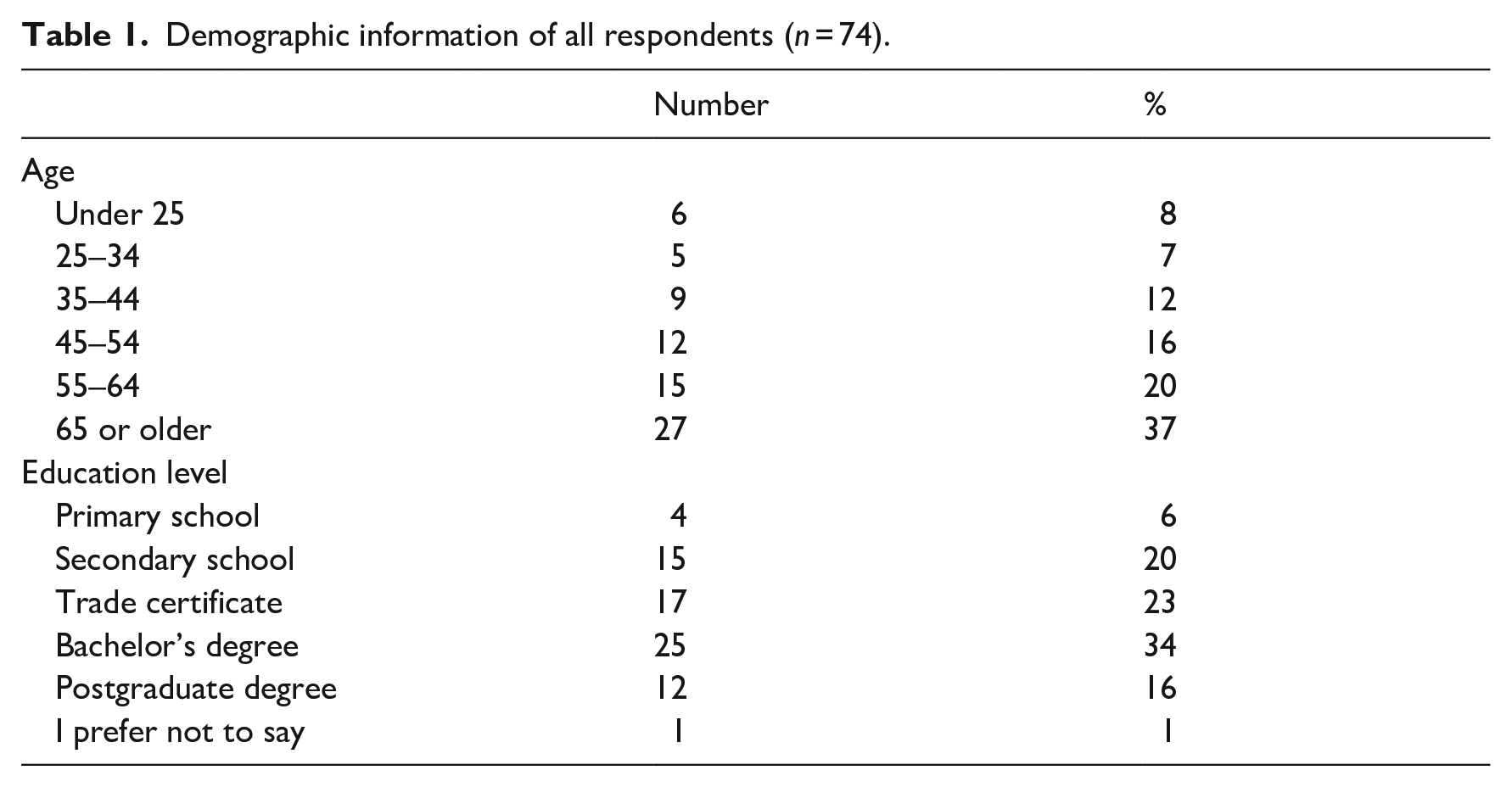
Seventy-four respondents completed the survey, and demographic details are as summarized in Table 1. Approximately half (n = 43, 57%) of respondents were aged over 55 years, with the cohort exhibiting above average education levels (with 50% holding a bachelor’s degree or above). A long cane was the most popular primary mobility aid among respondents (n = 40, 54%). Most respondents (n = 47, 63%) used their mobility aids multiple times per day (Figure 1(a)). More than half of respondents (n = 39, 54%) rated their confidence using their mobility aid as higher than 4, on a scale of 1 (e.g., poor confidence) to 5 (e.g., very confident) (Figure 1(b)). A one-way ANOVA showed that respondents who use guide dogs are significantly more confident than people who use other aids, F (3,65) = 5,48, p = .002. There were no differences between the other types of aid.
Demographic information of all respondents (n = 74).
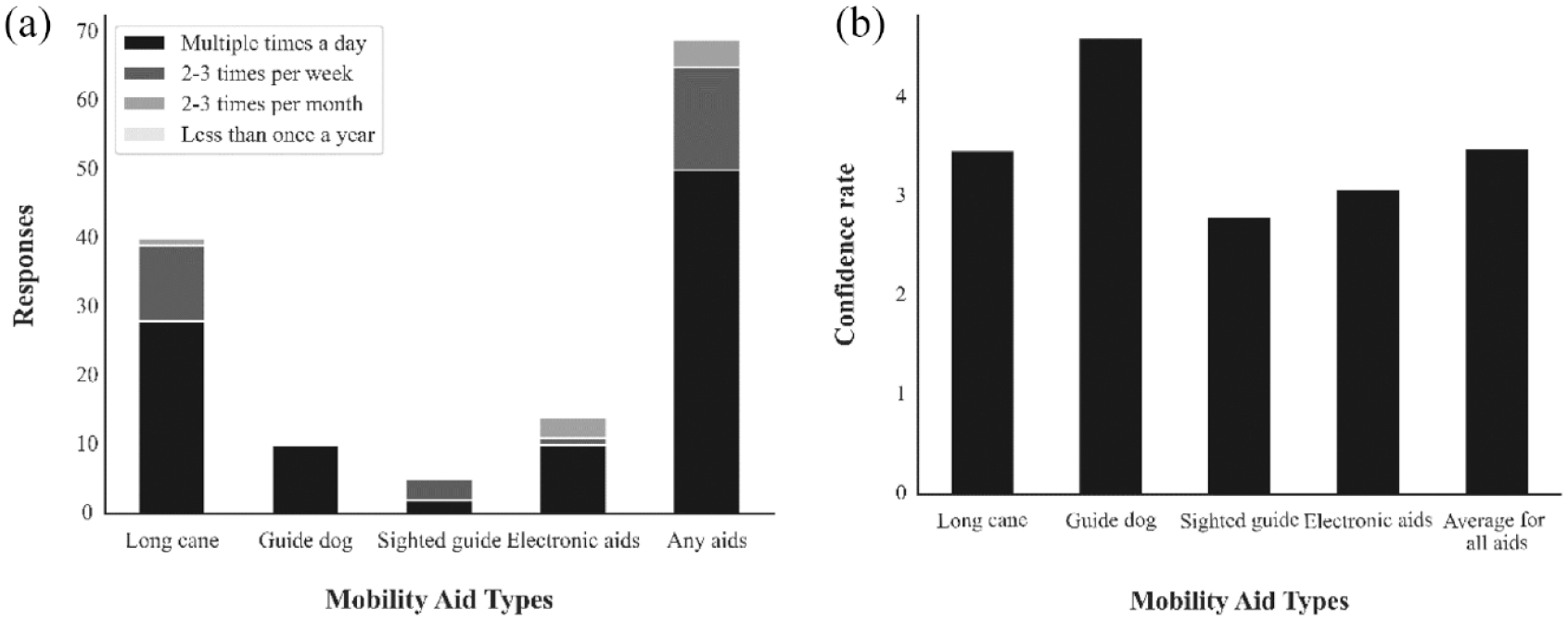
Mobility aids usage and confidence level.
Over half (n = 38, 51%) of the respondents reported that they do use ETAs as a secondary mobility aid or have tried ETAs. Only 2% of respondents (n = 5) reported that they did not use any mobility aid at all (including sighted guide), despite having legal blindness. For those who reported they had used an ETA, the devices listed were smartphone (n = 22), MiniGuide (gdp research, UK) (n = 14), Head torch (n = 2), Satnav (n = 1), and Sunu band (Sunu, USA) (n = 2).
Experiences with mobility aids
Participants were not given a preset list of features to choose from; instead, they were free to provide their own likes and dislikes based on their experiences with the aids. Table 2 summarizes the findings from thematic analysis which listed the most frequently mentioned categories for the free-text question; more than half of respondents (n = 38) found their current mobility aid most useful in familiar places, with statements such as navigating known destinations and familiar surroundings and the situations and environments I’m familiar with. Respondents’ answers also highlighted situations in which they found their current mobility aids were not helpful.
User experiences of different mobility aids.
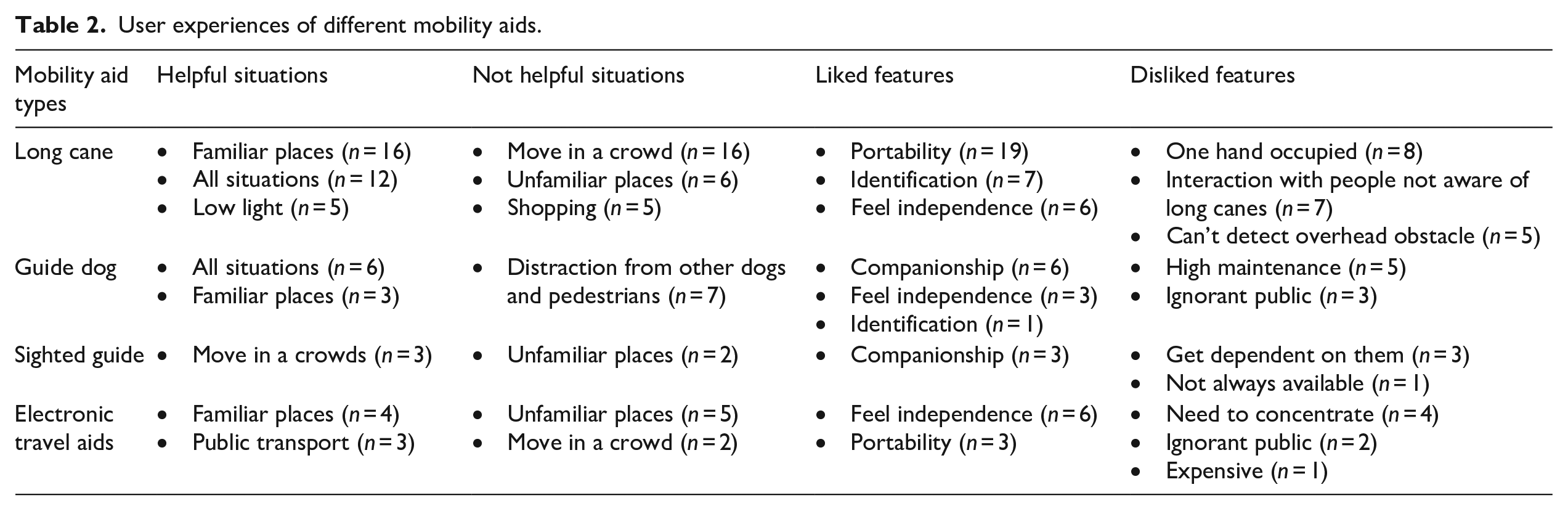
Crowded (n = 29) and unfamiliar places (n = 20) were of significant concern, as reflected by statements such as crowded places and large places like airports and city railway and city shops and large malls noise is distracting . . . also do not feel safe and In situations where there are a lot of people moving around quickly or where the ground is uneven.
Liked and disliked features of different aids are summarized in Table 2. Respondents valued the identification role of primary aids (e.g., long cane, guide dogs), but also found the convenience of ETA very helpful (e.g., smartphone, MiniGuide). For primary aids, respondents responded that their long cane was good at finding low ground obstacles but struggled with overhanging obstacles. Responses also indicated that guide dogs were very good companions but often distracted in crowded spaces.
Desired features in mobility aids
Respondents were provided with a list of features of mobility aids and asked to score on an importance scale of 1–5, with 1 being not important at all and 5 being of greatest importance. The features were ease of use, cost, quality of training, availability of training, multifunctionality, and that the device ‘does not interfere with other senses’. Averaged scores for the different features, for different aid users, are as summarized in Figure 2. Individuals’ data were pooled and averaged. The highest scored feature for all respondents was ‘Easy to use’ (M = 4.3), followed by ‘Quality of training’ (M = 4.1) and ‘Availability of training’ (M = 3.9). Lower scores were given to the device not interfering (M = 3.5) and has multifunction (M = 3.4). Cost was the least important (M = 3.2). There were no statistically significant differences observed between users of different types of mobility aids, except for the statement regarding the device not interfering with other senses. Users of a long cane rated this statement as significantly more important compared with individuals who use a guide dog or an electronic aid, F (65,3) = 2.89, p = .042.
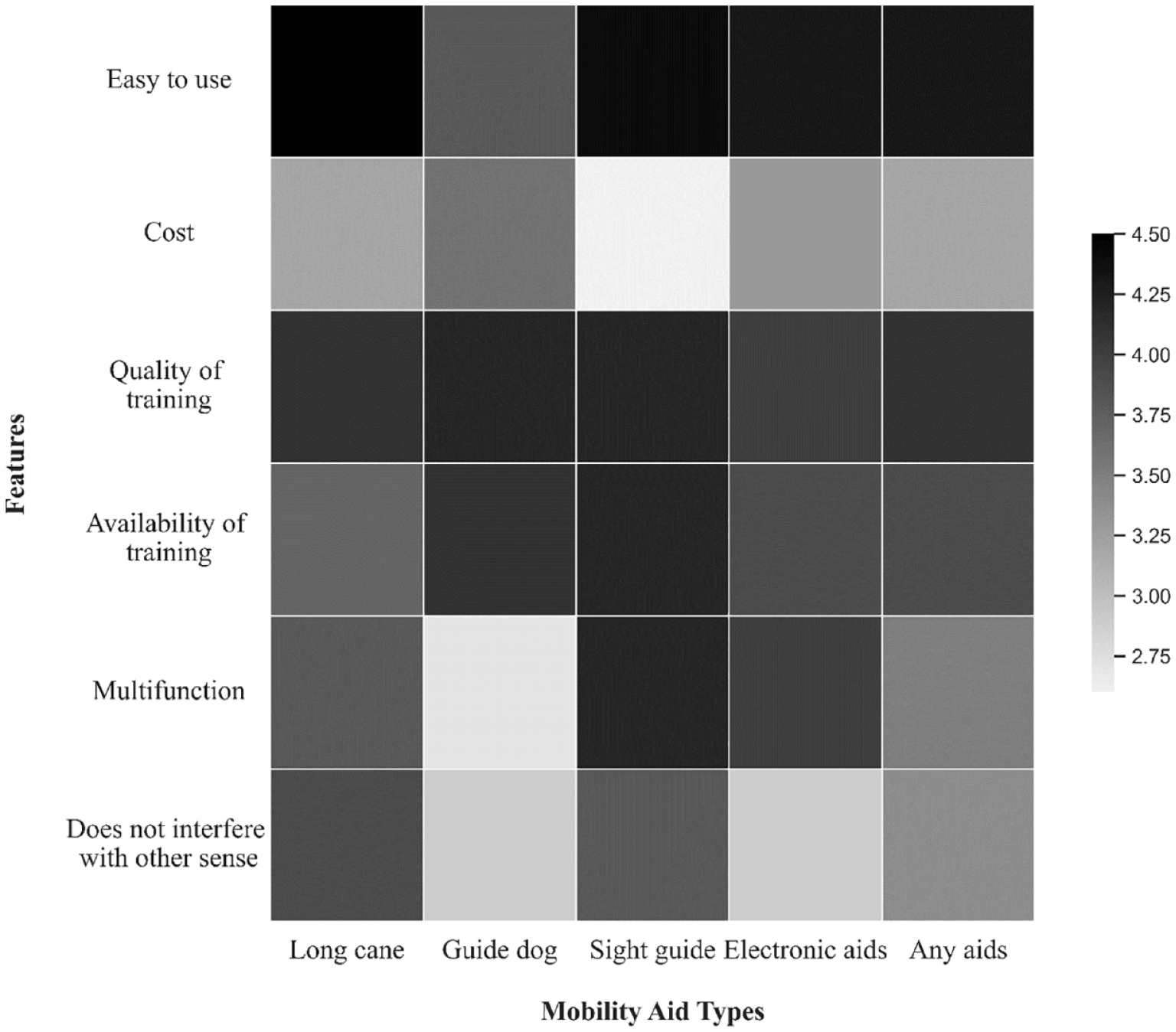
Desired features in mobility aids.
Attitudes to SSD
Almost two-thirds of the respondents (n = 48) had heard of SSDs prior to this survey, and one-third (n = 24) had used an SSD in the past. Respondents’ degrees of agreement for different SSD designs are as summarized in Figure 3.
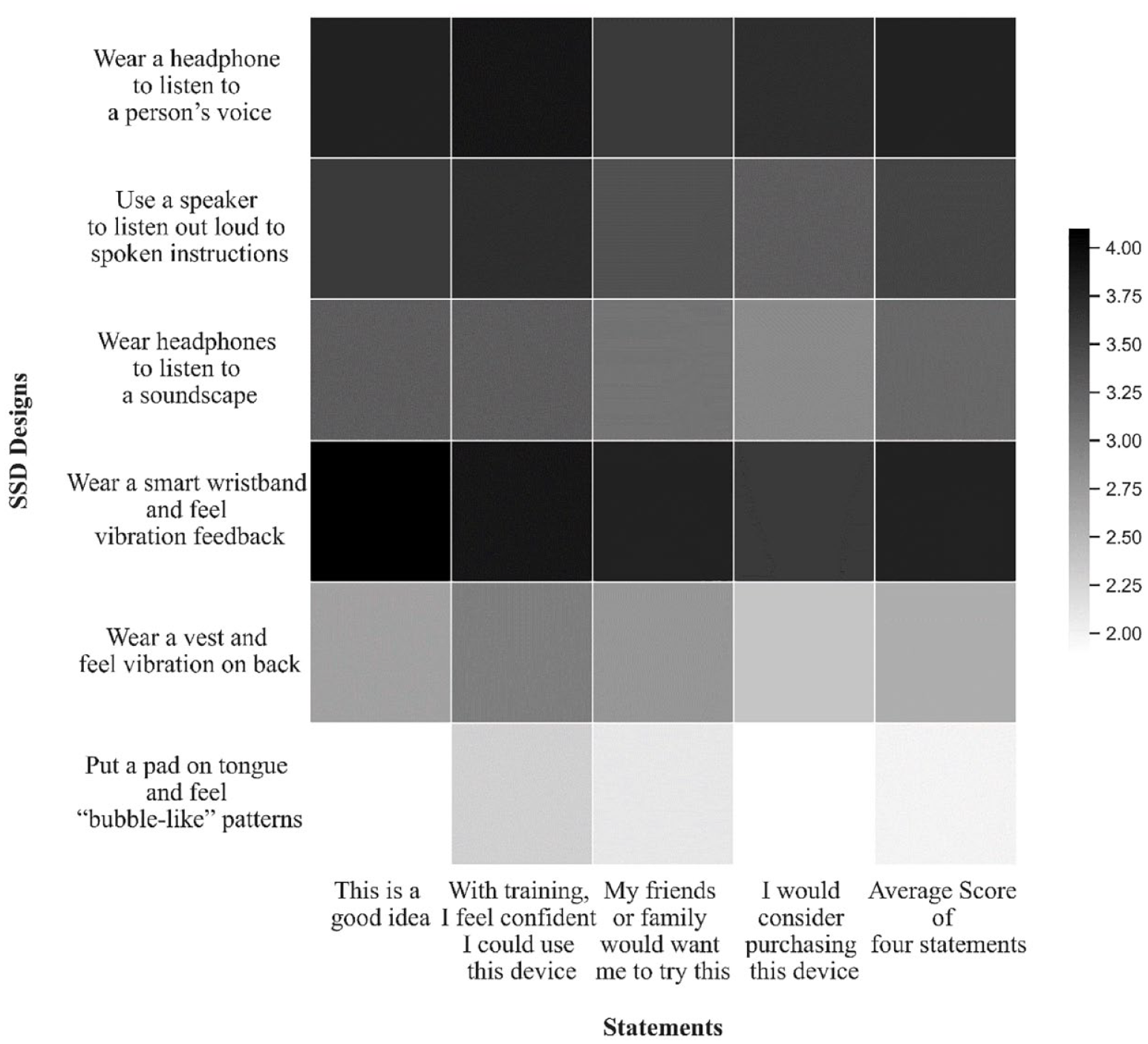
Attitudes to SSD.
Respondents’ attitudes varied with respect to different designs of SSDs, including within the category of visual-to-audio or visual-to-tactile. The least accepted designs were the vibration vest (M = 2.6) and vibration pad on tongue (M = 2). The most accepted designs were spoken instructions over headphone (M = 3.8) and the vibration wristband (M = 3.8) for audio and tactile modalities, respectively. A repeated measures ANOVA showed that the vest and tongue vibration devices and the headphones to listen to soundscapes were less accepted than all other devices, F (5) = 38.17, p < .001. Respondents also reported feeling less confident in their ability to use these three devices, F (5) = 26.94, p < .001), that their friends and family would be less likely to want them to try them, F (5) = 27.63, p < .001, and that if they were in their price range they would consider purchasing them, F (5) = 32.43, p < .001. Respondents showed a stronger preference for the wrist band over the vibration vest or tactile tongue display.
Discussion
The results demonstrated that most people (n = 54, 73%) still rely on primary mobility aids (e.g., long cane, guide dogs). Interestingly, over half of the respondents (n = 39) had used or tried an ETA as a secondary aid, and one in three (n = 24) reported that they had tried an SSD. This confirmed that this cohort of respondents were interested in advanced mobility aids. When it comes to the design of new mobility aids (i.e., SSD), people preferred the idea of audio feedback compared with tactile feedback. Respondents ranked ‘easy to use’ and ‘quality of training’ as the two most desired features of mobility aids.
In agreement with a previous report from Deverell et al. (2023), the ETA has become a standard travel aid in Australia. Many ETA users (n = 22) from our survey reported using smartphones as travel aids, which is testament to the inclusive software design that many smartphones now come with as a standard feature. Smartphones have natural advantages of a short learning curve, compact designs, and high acceptability (as most Australians now own a smartphone; Garrett et al., 2021). Applications like Google Maps and Uber have become increasingly more accessible to the low vision community. They typically assist in macro-navigation, aiding individuals in navigating long-distance routes or wayfinding, while primary aids could detect drop-offs and changes in the terrain to ensure safety. Like all electronic devices, user experiences of ETAs can be affected by the length of battery life and the quality of training instructions. While manufacturers such as Apple Inc. have led the incorporation of accessibility features into mainstream devices, the cost of smartphone devices with these features is still a challenge (Morrice et al., 2017).
Aside from smartphones, other ETAs have been designed to assist people with mobility and visual needs. For example, the MiniGuide and Sunuband were both specifically designed to negotiate with obstacles (Hill & Black, 2003; Smith et al., 2022). They provide an additional detection range and angle when used in conjunction with primary mobility aids. The results of our study may help in the research and development of more ETAs, in addition to guiding device selection for individuals with visual impairment.
The second half of our survey focused on SSDs, which aim to map the visual environment to other sensory modalities. However, due to the complexity of real-world environments, interpreting tactile or visual feedback could be cognitively demanding and have a steep learning curve. Previous studies have suggested that prolonged concentration makes SSD users tired, and that frustration can arise by the sometimes unreliable feedback (Elli et al., 2014; Maidenbaum et al., 2014). Our results suggested that users would prefer a familiar form of feedback (e.g., person’s voice, vibration) to more novel forms of sensory input (e.g., soundscape, bubble-like patterns over tongue). Future study could incorporate open-ended questions and offer a deeper understanding of the practical implication of SSD usage in real-world settings. To improve future devices, developers may wish to consider depth algorithm and attention loci algorithms, which could improve the quality of feedback by selecting only the most salient subset of information from preprocessing of the video input (Maidenbaum et al., 2014). Our study also agreed with earlier work that users desired a well-designed training programme for their mobility aids; see Figure 2 for details (Elli et al., 2014).
Other barriers to adoption of novel mobility aids (e.g., SSD) were highlighted in the current study, such as the need for portability. In line with previous studies in rehabilitation ergonomics (Lenay et al., 2003), all components should be small in size to be as unobtrusive as possible, since they need to be carried for long time periods. Regardless of the type of mobility aid, respondents’ user experiences were highly impacted by the environmental factors (e.g., familiar places, or not) and the designs of the product (e.g., portability and usability). In the free-text sections of our survey, respondents gave clear examples of the limitations of some of the existing mobility aids. For example, people commented that long canes are challenging to use when moving through a crowd or detecting overhead obstacles. Regarding ETAs and SSDs specifically, the small-scale manufacturing and high research and development costs could result in a high price tag. Additional costs could be incurred if rehabilitation training is required. To lessen these costs, commercially available SSDs could benefit from a closer collaboration between academia, low vision service, and manufacturers, to ensure devices are designed with the end user and manufacturing processes at front of mind.
Limitations
Our study also has limitations. Most importantly, many of the respondents (n = 50) had never tried the SSDs outlined in the survey. As such, they were basing their opinions on a small paragraph of text, rather than lived experience. Future studies could investigate how the responses change after trial exposure to all the SSD options, to gather information on real-world experiences, rather than theoretical decisions. Several new tools now have emerged since the time of our survey, including smartphone applications like OKO (AYES, USA) and BeMyAI (Be My Eyes, USA). Both were designed to use artificial intelligence to recognize the user’s environment and provide audio narratives. Future research should include these mobility aids. Moreover, we surveyed people with IRD meeting the definition of legal blindness without identifying their specific visual pathology and their visual acuity. People with different pathologies (e.g., rod-cone, maculopathy) and remaining vision could have totally different issues regarding mobility and affect their choices for a secondary mobility aid. It will be important in future work to capture data on visual acuity, duration of vision loss, and other disease specifics for more detailed correlation of disease state with mobility aid preferences. For example, people with macular degeneration are often challenged when travelling at night due to their poor dark adaptation, and so may benefit from a device which does not need good lighting (like a cane; Wu et al., 2016). Further studies could investigate the relationships between ocular disease subtype and a respondent’s desired features in mobility aids. Our recruitment strategies were also biased towards people who have access to internet, as we used an online survey, which may bias our findings towards people who are engaged and interested in technology. Our respondents were also recruited through research databases and community advocacy groups, suggesting they were likely interested in research and the IRD community. The lack of data on respondents’ cultural backgrounds is a significant limitation of our work. While our study primarily focused on the user perspective of mobility aids, it is important to consider cultural factors in future research and device development efforts, as they have been shown in Gallimore et al. (2016). This is crucial for ensuring that emerging technologies meet the diverse needs of individuals with impaired vision.
Interestingly, a small group of respondents (n = 2) managed their daily activity (e.g., commuting to work) without the help from any mobility aid. This highlights the fact that there is no ‘one-size-fits-all’ solution for mobility and supports the continued research and development into devices and other interventions for people with visual impairment. Moreover, respondents in this ‘legally blind’ category may still retain sufficient residual vision to perform daily tasks without the need for mobility aids.
Conclusion
In conclusion, our study aimed to gain insights into the perspectives on current mobility aids and emerging technologies like SSDs within the Australian low vision community affected by IRDs. Through an online survey and mixed-method analysis, we found that traditional mobility aids are still the most commonly used; novel mobility aids (ETAs and SSDs) also have the potential to significantly improve the travelling experiences of people with impaired vision. The results indicated that respondents expressed a preference for the wrist band over other tactile feedback options at first impression of SSDs, highlighting the importance of user preferences. Therefore, ergonomics and well-designed training programmes are essential considerations when developing such aids. While our study focused on individuals with IRDs, it is important to acknowledge the potential variation in experiences among those with different causes of vision loss and varying levels of remaining vision. Future evaluation studies of low vision aids should consider more than functional improvements, also ensuring they investigate user experience and barriers to uptake. Both are critical to transforming a novel idea (e.g., SSDs) into a commercially available product, thus offering those with impaired vision more options for assistance and independent travel.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196241253514 – Supplemental material for Perspectives on traditional and emerging mobility aids amongst Australians with inherited retinal disease
Supplemental material, sj-docx-1-jvi-10.1177_02646196241253514 for Perspectives on traditional and emerging mobility aids amongst Australians with inherited retinal disease by Rui Jin, Matthew A Petoe, Chris D McCarthy, Jennifer L McGinley and Lauren N Ayton in British Journal of Visual Impairment
Footnotes
Acknowledgements
The Bionics Institute and the Centre for Eye Research, Australia, acknowledge the support they received from the Victorian Government through its Operational Infrastructure Support Programme. The authors also thank Fiona Fylan (Leeds Sustainability Institute, Leeds Beckett University, Leeds, UK) for her input into the survey development.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Health and Medical Research Council Investigator Grant to L.N.A. (grant nos. 1195713 and 2022-26), University of Melbourne Driving Research Momentum Fellowship to L.N.A. (2019-23), 2021 Retina Australia Grant to L.N.A., M.A.P., C.D.M., and J.L.M. and a 2020 Melbourne Disability Institute Grant to L.N.A., J.L.M., M.A.P., C.D.M., and R.J.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.