
Abstract
Assistive technology (AT) devices are designed to help people with visual impairments (PVIs) perform activities that would otherwise be difficult or impossible. Devices specifically designed to assist PVIs by attempting to restore sight or substitute it for another sense have a very low uptake rate. This study, conducted in England, aimed to investigate why this is the case by assessing accessibility to knowledge, awareness, and satisfaction with AT in general and with sensory restoration and substitution devices in particular. From a sample of 25 PVIs, ranging from 21 to 68 years old, results showed that participants knew where to find AT information; however, health care providers were not the main source of this information. Participants reported good awareness of different ATs, and of technologies they would not use, but reported poor awareness of specific sensory substitution and restoration devices. Only three participants reported using AT, each with different devices and varying levels of satisfaction. The results from this study suggest a possible breakdown in communication between health care providers and PVIs, and dissociation between reported AT awareness and reported access to AT information. Moreover, awareness of sensory restoration and substitution devices is poor, which may explain the limited use of such technology.
Keywords
Introduction
Visual impairments, or vision that cannot be corrected with lenses or surgery and blindness, affects a large proportion of the human population. Globally, it is estimated that 285 million people, or 3.7% of the population, are living with visual impairment (He et al., 2020; National Health Service, 2018; World Health Organization, 2021). Visual impairment affects interactions with the physical world (West et al., 2002), interactions with others, and can result in poor mental health (Demmin & Silverstein, 2020). Chia et al. (2004) found that visual impairment significantly decreased one’s quality of life, on physical, social, emotional, and mental factors, compared to those without visual impairment and those with correctable vision. Thus, there is great potential for assistive devices in aiding people with visual impairments (PVIs) and improving quality of life.
The United Kingdom’s Medicines & Health care products Regulatory Agency (2021) defines assistive technology (AT) as any product designed to assist individuals with impairments with actions that would otherwise be difficult or impossible. As this report is focusing on visual impairments, further references to ATs refer to those designed specifically to assist with visual impairment. AT can be classified into low-tech, medium-tech, and high-tech devices: low-tech ATs require no electricity to operate, medium-tech devices require electricity but are not computerised, and high-tech devices require both electricity and are computerised (Kaye et al., 2008). Examples of popular “low-tech” devices for PVIs include canes and guide dogs or Braille (Illinois Library, 2020). Medium-tech devices for PVIs are less common, an example being electricity powered cassette tape readers (Varghese, 1996). Technological advances have facilitated the use of computer processing in ATs to provide more advanced assistance for PVIs through the development of high-tech devices (Bhowmick & Hazarika, 2017). High-tech ATs include sensory restoration devices and devices that utilise sensory substitution technology, either within a dedicated device or integrated into existing devices such as a mobile phone.
Sensory restoration devices for PVIs aim to restore functionally useful visual perception through stimulation of visual neural pathways (Lewis et al., 2015). Most devices are invasive, requiring surgical implantation, though some non-invasive techniques are currently being investigated (Sabel et al., 2020). Four Conformitè Europëenne (CE) marked sensory restoration devices, all retinal prostheses, are: Argus II (Luo & Da Cruz, 2016), Intelligent Retinal Implant System (IRIS) II (Pixium Vision, 2016), Alpha IMS (Stingl et al., 2013), and Alpha AMS (Daschner et al., 2018). All devices produced better performance on visual tasks, such as object localisation, shape recognition, and letter reading, with the devices on rather than off (Bloch et al., 2019). However, their effectiveness in helping PVIs during spatial navigation and wayfinding remains unclear (e.g., Garcia et al., 2015).
Unlike sensory restoration devices, sensory substitution devices do not require surgery. Sensory substitution technologies for PVIs communicate visual information via another, intact sensory modality (Ward & Wright, 2014); for example, playing different sounds to communicate different visual features, such as elevation and horizontal location, within the visual field. The technology is grounded in the understanding that the brain can interpret sensory information from one modality (e.g., sound) as information from a different modality (e.g., visual) (Shimojo & Shams, 2001; Solomon-Harris et al., 2013). Numerous devices designed specifically for sensory substitution have been developed (Scheller et al., 2018), such as The vOICe (visual-to-auditory) (Meijer, 1992), and BrainPort (visual-to-tactile) (Fale et al., 2016). Many devices designed specifically for sensory substitution have been successful in improving functional outcomes where sensory restoration devices have struggled (Erickson-Davis & Korzybska, 2021; Garcia et al., 2015). For example, sensory substitution devices have been found to improve spatial competence (Chebat et al., 2020; Jicol et al., 2020), object recognition (Arnoldussen & Rhode, 2010) and object localisation (Proulx et al., 2008).
Despite encouraging results from clinical tasks, sensory restoration and substitution devices are rarely used outside of the laboratory (Elli et al., 2014; Griffin-Shirley et al., 2017; Lloyd-Esenkaya et al., 2020). This may be because the devices do not improve processes such as object identification and navigation enough to support daily life. For example, statistically significant improvements on object identification may not represent large-enough benefits for use in everyday life. Luo et al. (2014) presented photos of three-dimensional objects and asked patients using the Argus II to identify the objects. They found a significant improvement in object identification when the device was switched on. However, correct identification with the system on was only 35.7% on average (SD = 14.6%), which may not be accurate enough to be useful in identifying objects in everyday life. With regards to navigation, retinal prostheses provide little useful spatial information (Horne et al., 2015), and some evidence suggests that users may not utilise the perceptual experiences provided by a sensory restoration device to aid in navigation (Garcia et al., 2015). The most popular assistive device used for navigation and mobility by PVIs to date is the long cane (Batterman et al., 2018; Dahlin-Ivanoff & Sonn, 2004). Sensory restoration and substitution devices may not replace the long cane because of the greater need for training and cognitive effort (Hamilton-Fletcher et al., 2016), in exchange for little additional benefits. Moreover, low-tech devices are difficult to surpass because of their reliability, lack of reliance on electricity, and relative inexpensiveness (Manduchi & Coughlan, 2012). Thus, the limited benefits of sensory restoration and substitution devices compared to low-tech ATs may explain their poor uptake.
On the contrary, research that has taken into account PVIs’ opinions suggests that the low uptake of sensory restoration and substitution devices may not be related to device functionality at all. Some PVIs have expressed disappointment about the neglect of user experience in such devices (Lenay et al., 2003). For example, in Hamilton-Fletcher et al.’s study (2016), while participants reported optimism for some visual-to-auditory sensory substitution devices’ potential in aiding everyday life, some devices were also criticised for the unpleasant auditory aesthetics. Others were highly praised for their focus on providing PVIs with sensory information beyond function, such as colour; a feature absent from most sensory substitution devices. This highlights the crucial distinction between a functionally effective device, and a device that PVIs like and want to use; a distinction often neglected in the development of ATs (Manduchi & Coughlan, 2012). Accordingly, another essential feature of ATs is subtlety. Many PVIs refrain from using ATs such as the cane due to the feelings of shame and stigmatisation that arise with being identified as visually impaired (Hayeems et al., 2005). Some sensory substitution devices are characterised by the same limitation. For example, part of the BrainPort device is placed in the mouth (Wicab Inc., 2010) and has been criticised for being indiscrete as well as impractical (Upson, 2007). Moreover, sensory restoration and substitution devices are often very expensive, thus rendering these devices inaccessible. A survey by Manjari et al. (2020) assessed a wide range of sensory substitution devices and concluded that seven of the 37 devices assessed were economic, and all but two were user-friendly. However, this study did not involve PVIs in drawing these conclusions, thus these conclusions should be regarded cautiously. This highlights the need for the inclusion of PVIs’ voices in research regarding ATs to refocus the industry on PVIs’ needs and desires, rather than on bioengineering solutions which may have contributed to the low uptake of such devices (Manduchi & Coughlan, 2012).
Another barrier to AT access may be awareness. Low-tech ATs, such as the cane, have existed for many decades (Strong, 2009) and are established as common assistive tools, as well as symbols of visual impairment (Due & Lange, 2018). Hence, PVIs are more likely to be aware of such technology (Senjam et al., 2020). As many high-tech ATs are relatively new, it is possible that PVIs are unaware of the existence of sensory restoration and substitution devices. Senjam et al. (2020) found that the majority of participants in a sample of visually impaired students in Delhi had awareness of Braille-related devices and long canes, but much fewer were aware of more high-tech devices such as electronic magnifier aids, talking calculators and mobile applications. However, visually impaired students showed high awareness for talking watches and screen readers. Almost all devices investigated by Senjam et al.’s (2020) study were designed to aid with very specific aspects of life; namely school life. Similarly, Okonji and Ogwezzy (2019) studied PVIs’ awareness of older ATs that specifically aid access to computers. Thus, a better understanding of AT awareness, especially for more recent devices in a wider range of contexts, is lacking. Furthermore, the studies by Senjam et al. (2020) and Okonji and Ogwezzy (2019) did not address possible barriers to accessing AT information, which could limit AT awareness. Hence, this study aimed to examine specifically: how accessible AT information is to PVIs, the extent of PVIs awareness of AT (particularly of sensory restoration and substitution devices), and how satisfied PVIs are with their AT (particularly with their sensory restoration or substitution device).
Method
Participants
Visually impaired participants were recruited via volunteer sampling by distributing the survey link to Facebook support-groups and through the Royal National Institute of Blind People. In total, 25 participants completed the study (11 males, 13 females, and 1 unspecified), ranging from 21 to 68 years old (M = 44.91, SD = 17.27). The sample included a range of visual impairments: 7 participants were completely blind, 12 were severely sight impaired, and 6 were sight impaired. Study information was provided and electronic consent was obtained prior to study initiation. Ethical approval was granted by the University of Bath’s Psychology Research Ethics Committee (reference no: UG 19-038). The study was carried out in 2019/2020.
De-sign, material, and procedure
This study was an online questionnaire study made and published using Qualtrics (2021). The data were analysed in three domains: Accessing AT information, awareness, and satisfaction. No validated measures of awareness of ATs, or accessing AT information, exist yet. Thus, a set of questions and measures were created for this study. The accessing AT information questionnaire comprised questions about sources of AT information and the extent to which PVIs actively searched for information (Table 1). The awareness questionnaire comprised questions about general knowledge of sensory restoration and substitution devices, and questions probing the depth of such awareness (Table 3). These items were measured on a 5-point Likert-type scale with “1” = strongly agree and “5” = strongly disagree (Nadler et al., 2015).
Questionnaire items included in the accessing information analysis.
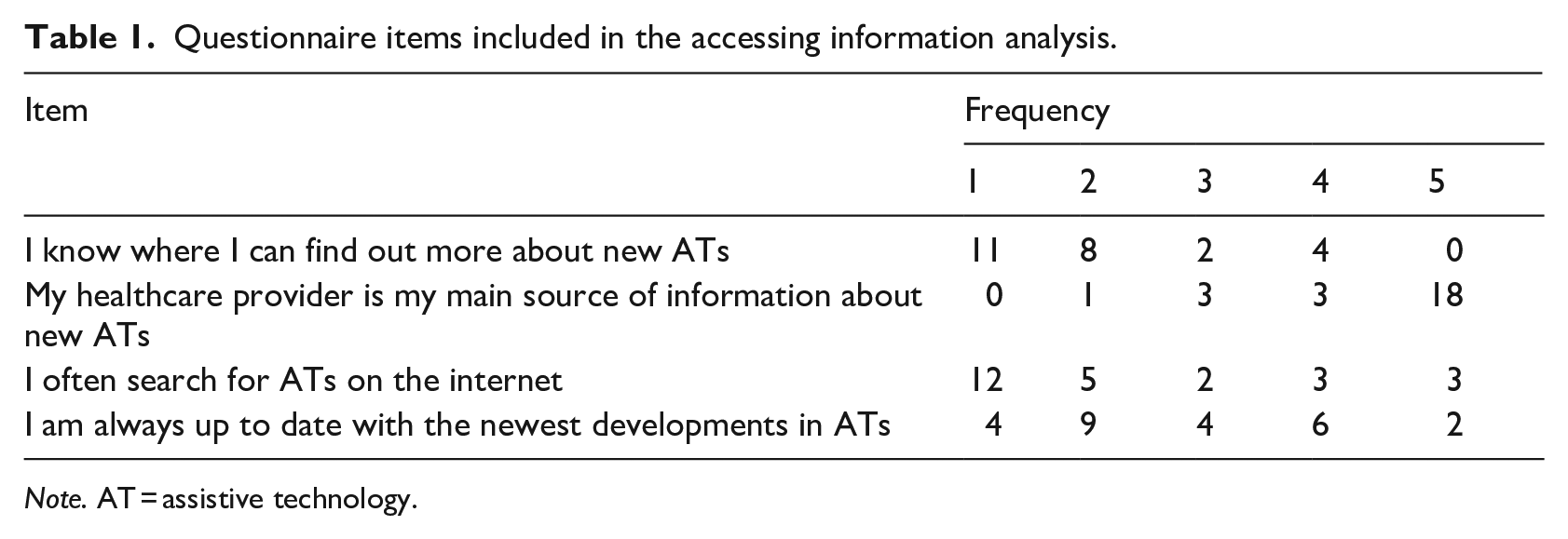
Note. AT = assistive technology.
Participants who answered “yes” to the additional question “Do you currently use an assistive sensory restoration or substitution device?” were further invited to complete the satisfaction and preference questionnaires. The satisfaction and preference questionnaires were analysed in conjunction with the qualitative responses collected on the same topics. The Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0) (Demers et al., 2000) was used to assess device and service satisfaction. Previous studies have shown this scale to have excellent test–retest reliability (Demers et al., 2002) and robust internal consistency (Galeoto et al., 2018). The Assistive Technology Device Predisposition Assessment for device users (ATDPA) (Scherer, 2005) assessed satisfaction with positive impact made to different aspects of participants’ lives. This scale also has an excellent test–retest reliability and a relatively high internal consistency (Koumpouros et al., 2017). Both questionnaires used a 5-point Likert-type scale where ‘1’ = extremely satisfied and ‘5’ = extremely dissatisfied. The five questions regarding AT preferences used a 3-point Likert-type scale with “1” = yes, “2” = maybe, and “3” = no, and can be found in the Supplemental Material.
Results
One-sample Wilcoxon’s signed rank tests were used to compare the hypothetical median (“3,” or “neither agree nor disagree”) against the observed median. This was done as the data were on an ordinal scale and mostly non-normally distributed (W[21] ⩽ .868, p ⩽ .009), as assessed by Shapiro–Wilk tests. All p values were Bonferroni corrected to account for familywise error, with this results section reporting the corrected p values.
Accessing AT information
Frequency distributions can be found in Table 1, results from the Wilcoxon tests are shown in Table 2, and boxplots for the data are presented in Figure 1. Reponses in this domain indicated that participants significantly agreed that they knew where to find information about new AT but strongly disagreed that their health care provider was their main source of information. No significant difference from “neither agree or disagree” was found for the items regarding often searching the internet for ATs and for always being up to date with the newest developments in ATs.
Test statistics for the domain accessing AT information.
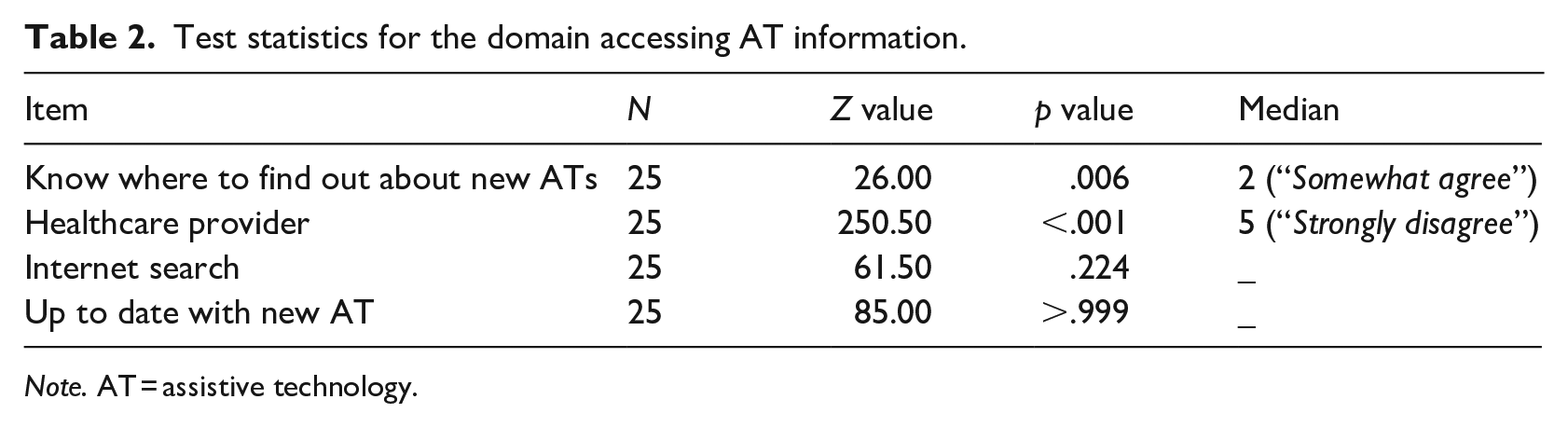
Note. AT = assistive technology.
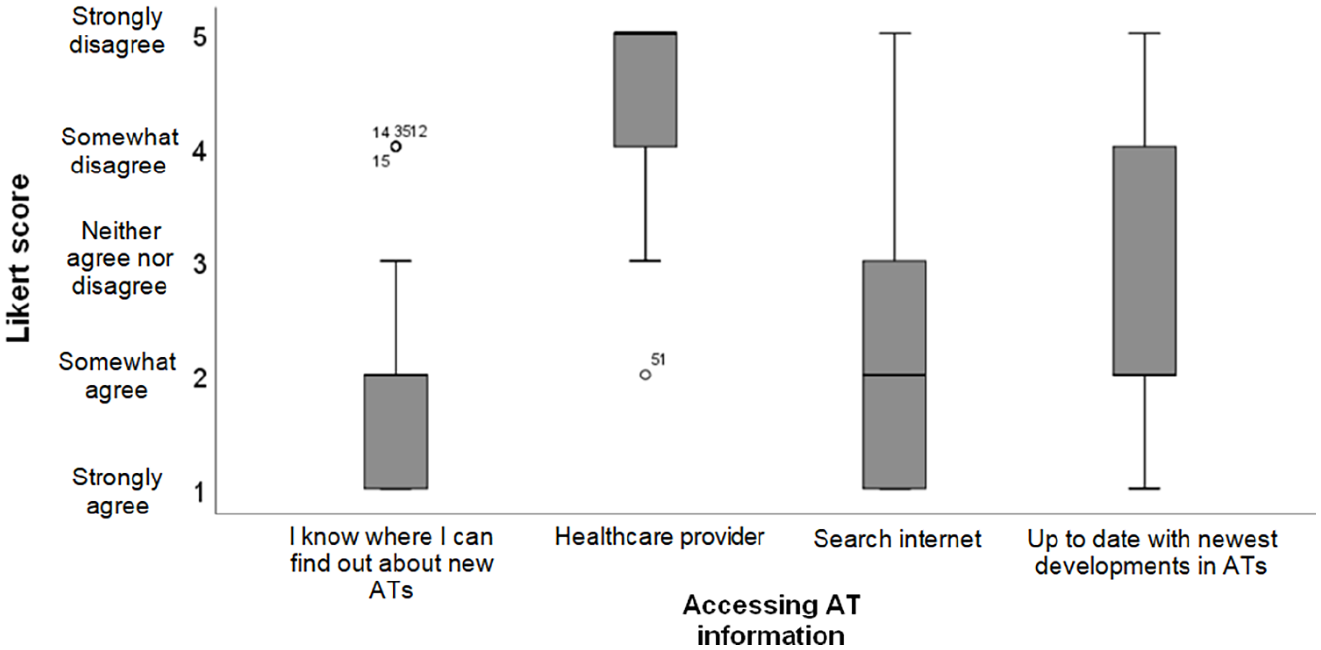
Box plots of the median and interquartile range of Likert-type scores for items regarding accessing AT information.
Awareness
Frequency distributions of the responses in the domain of AT awareness can be found in Table 3, results from the Wilcoxon tests are shown in Table 4, and boxplots for the data are presented in Figure 2.
Questionnaire items included in the awareness analysis.
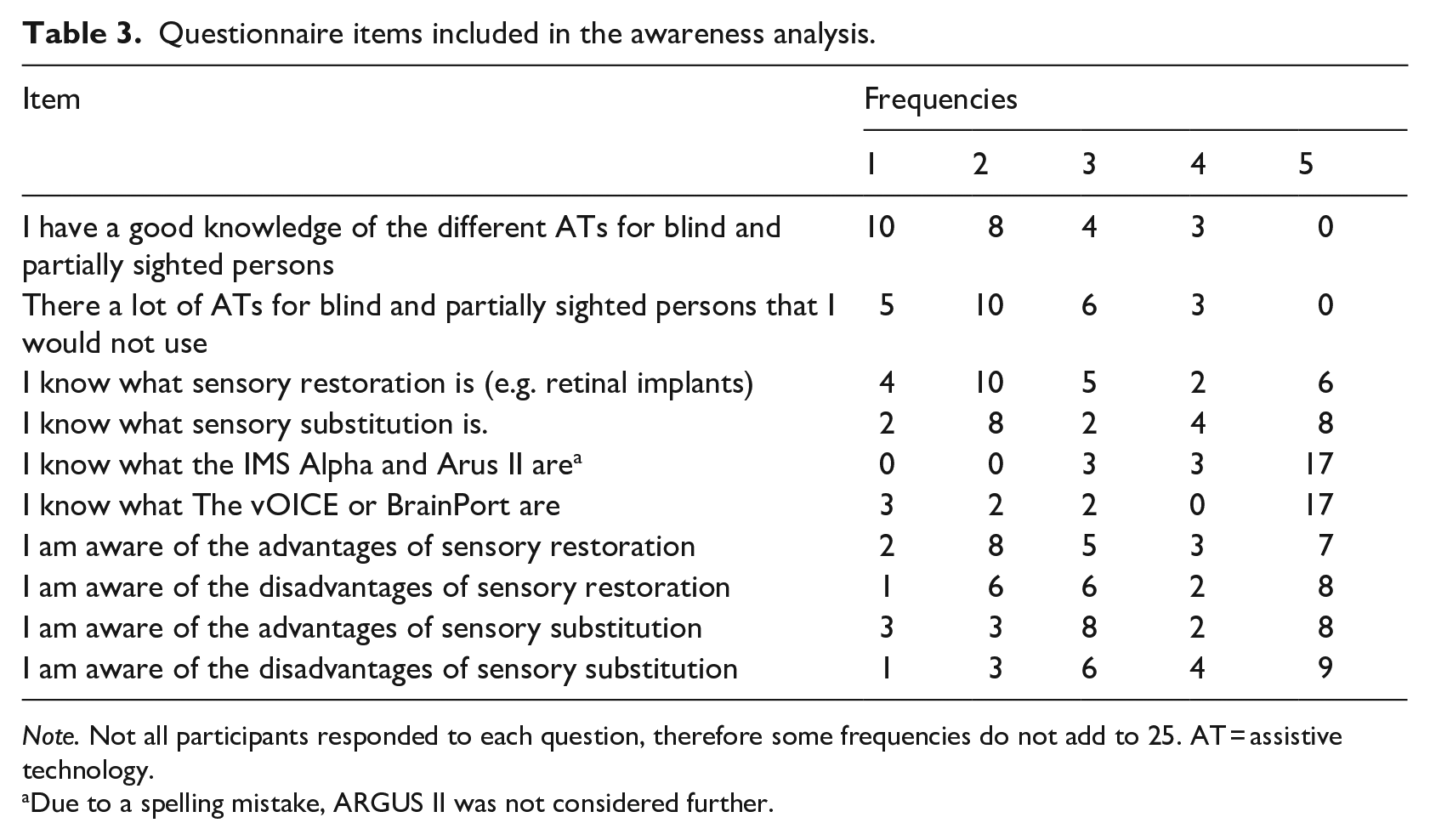
Note. Not all participants responded to each question, therefore some frequencies do not add to 25. AT = assistive technology.
Due to a spelling mistake, ARGUS II was not considered further.
Test statistics for the domain ‘awareness of ATs.
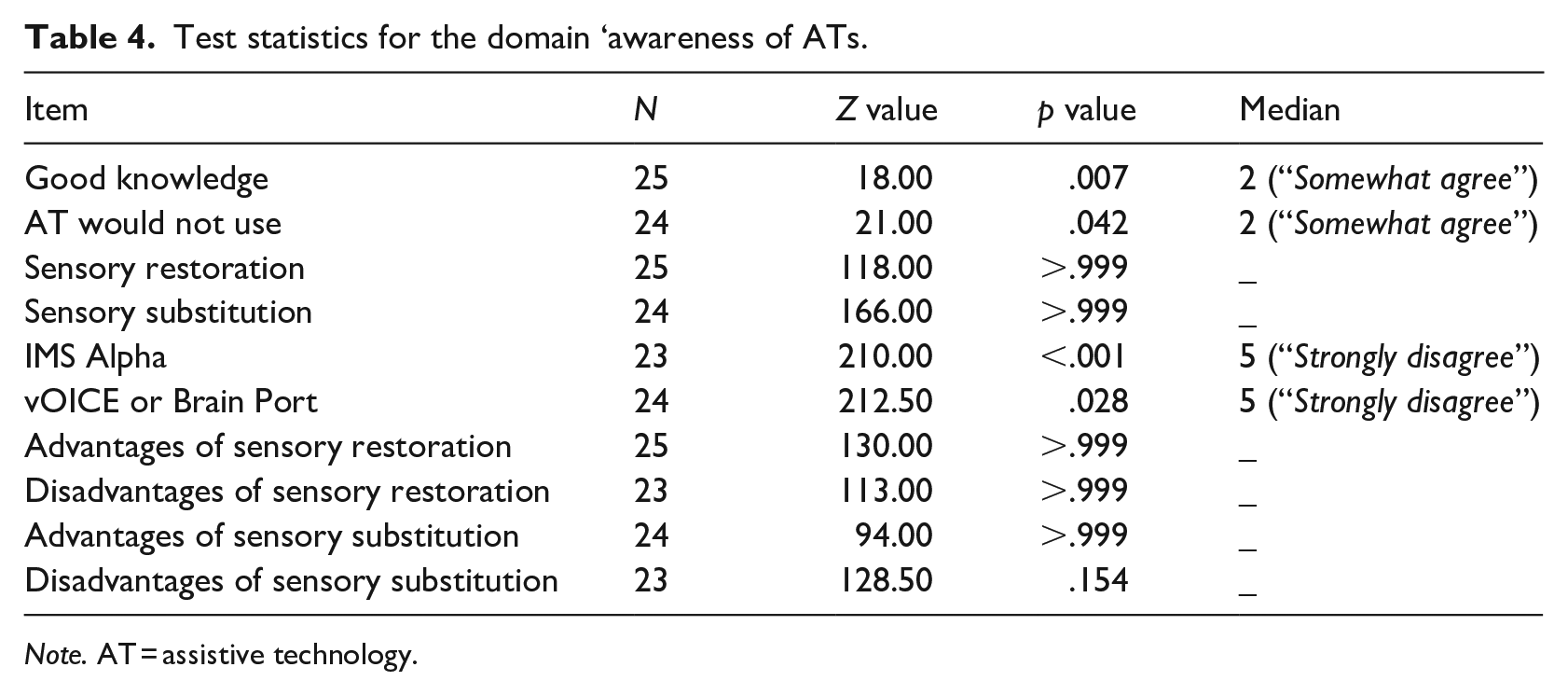
Note. AT = assistive technology.
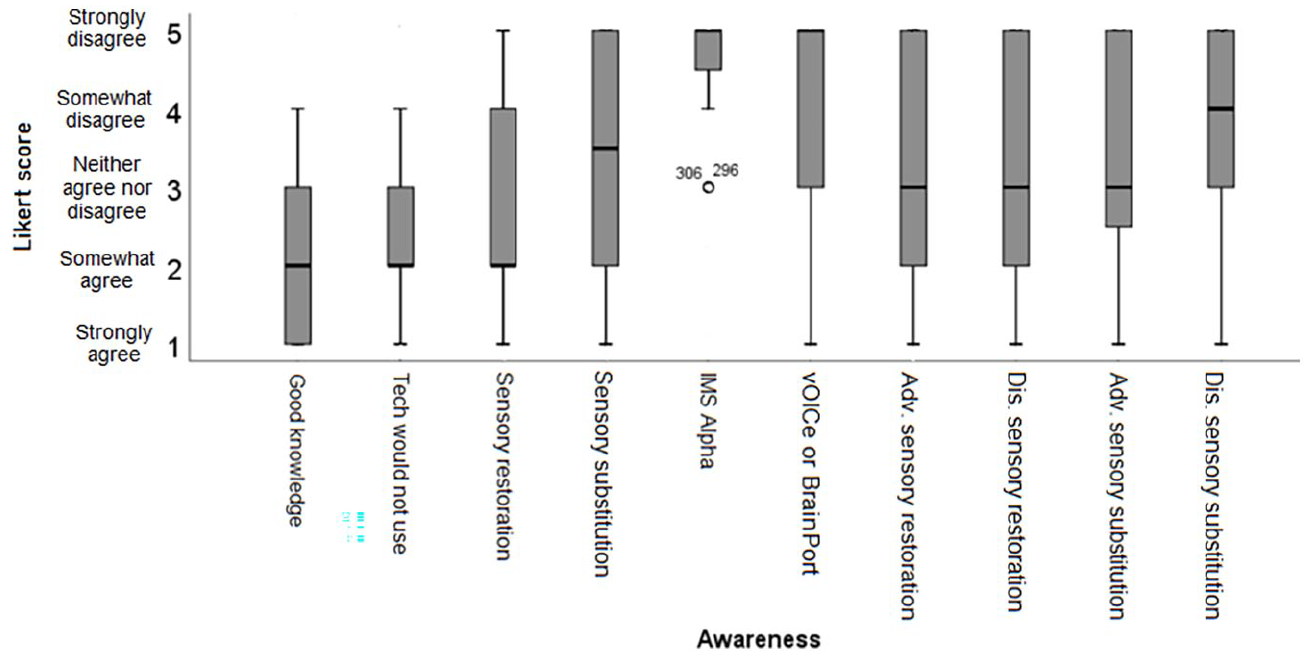
Box plots of the median and interquartile ranges of Likert-type scores for items regarding awareness.
The observed medians for four out of ten items for awareness were significantly different from the hypothetical medians. The results found that participants were significantly more aware than ambivalent of different ATs and technologies they would not use. Participants also reported significantly poorer level of awareness than neutral for the specific sensory restoration and substitution devices.
Satisfaction
Only three participants reported using high-tech AT for visual impairment, these were an iPhone/laptop, a Miniguide (Hill & Black, 2003) and BrainPort Vision Pro; the latter two being sensory substitution devices. With only three participants reporting using an AT for visual assistance, group analysis was not possible. However, Table 5 shows the individual satisfaction scores for device, service, and positive impact.
Satisfaction scores.
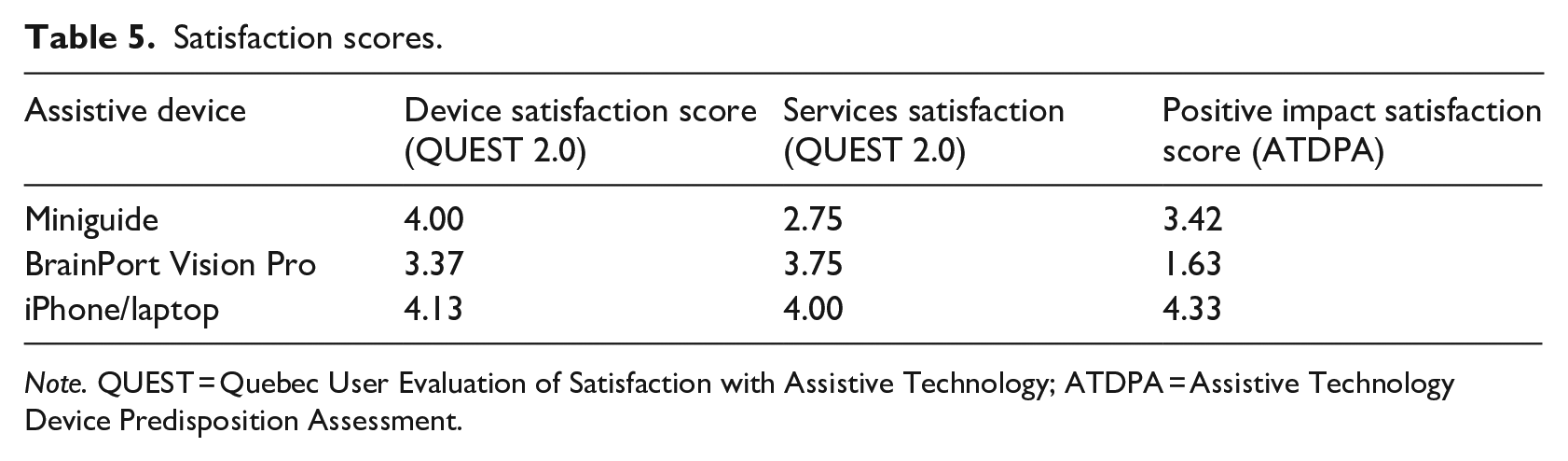
Note. QUEST = Quebec User Evaluation of Satisfaction with Assistive Technology; ATDPA = Assistive Technology Device Predisposition Assessment.
One participant reported using a bone-anchored hearing aid which is a sensory restoration device for auditory impairment, hence the data for this participant were not further analysed (but can be found in the supplemental material).
Device satisfaction measured the satisfaction with practical aspects of the device such as comfort, size, and effectiveness. Services satisfaction measured satisfaction with the customer service received for the device. Positive impact satisfaction measured the device’s ability to improve different areas of the users’ life.
The Miniguide user reported good device satisfaction, but was ambivalent regarding service and positive impact satisfaction. The BrainPort user reported ambivalence for device satisfaction, ambivalence/slight satisfaction for the services but expressed dissatisfaction for its positive impact. The Miniguide user reported that they would recommend their device, but the Brainport user reported that they would not.
In the preferences domain, the iPhone/laptop user and Miniguide user reported that they were disappointed by the promises made by companies developing new ATs. Both sensory substitution device users reported that they would prefer sensory restoration over substitution, and would invest time and effort into training for an AT they knew would improve their daily life. However, while the Miniguide user reported that they strongly agreed that they knew what sensory restoration was, the BrainPort user reported strongly disagreeing. This suggests that the BrainPort user’s reported preference for sensory restoration over substitution may be poorly informed and instead possibly due to interpreting sensory restoration as full visual recovery, as the name suggests.
There was not enough data to conduct a thematic analysis, with only the Miniguide user and iPhone/laptop user responding to open-ended questions. In response to how the device helped with their day-to-day life, the Miniguide user emphasised the enhanced spatial awareness regarding other people as useful (Extract 1), and later suggested that this resulted in a higher confidence and an increased sense of safety (Extract 2). Conversely, the iPhone/laptop user reported using their device to support with interactions with digital content more so than facilitating engagement with the physical world (Extract 3), though they did refer to Global Positioning System (GPS) use.
Question: How does this device help your day-to-day life? “Helps me to be aware of people entering my space.” Question: What reasons do you have for using your assistive device? “Increased awareness of surroundings resulting in higher confidence and security.” Question: How does this device help your day-to-day life?
Emailing, using GPS, watching videos onLINE and much more
Discussion
This study examined how participants source information about AT information, their awareness of high-tech AT, and how satisfied they are with high-tech AT. Results showed that participants knew where to find information about ATs, but their health care providers were not their main source of this information. It is unknown whether this is due to the existence of more prominent sources of information, a limited awareness of different devices from health care providers, or barriers to PVIs accessing the information or health care services. There are numerous challenges that hinder PVIs’ access to health care services and communication between PVIs and health care providers. These include, information being communicated via printed text (Cupples et al., 2012), limited information and assistance about health care entitlement (Sharts-Hopko et al., 2010), and a lack of sensitivity to PVI needs (Withers & Speight, 2017). Thus, these factors may not only prevent good communication between PVIs and health care providers, but limit access to the health care services altogether (Cupples et al., 2012). Understanding why health care providers are not the main hub of information about new ATs for PVIs and finding a targeted solution could be an easy barrier to overcome for PVIs, possibly increasing the uptake of some of available high-tech ATs.
Participants also remained neutral in agreeing or disagreeing with whether they often searched the internet for information about ATs and with whether they were always up to date with the latest developments in AT. Thus, despite knowing where they could obtain information from, they were not accessing it. One possible explanation is that there may be accessibility issues creating barriers to information. Lüchtenberg et al. (2008) found that 82% of 139 websites containing medical information were not fully accessible to PVIs. Since 2008, issues with accessibility seem to have somewhat improved, with the implementation of text-to-speech functions on major web browers (Ebden & Sproat, 2015). However, accessibility remains a barrier for accessing health information through difficulties in searching the internet (Sahib et al., 2012; Xie et al., 2018). Alternatively, Okonji and Ogwezzy (2019) found that some participants did not use high-tech AT because they had no need (29%) and lacked interest (22%), which may suggest a disinterest in AT. Lenay et al. (2003) found that PVIs were disappointed by ATs due to the expectations created around them. Similarly, the Miniguide user in this study expressed disappointment at the promises made by companies developing new ATs. Thus, this could contribute to the lack of interest. It is important to determine why participants are not seeking information about ATs as it indicates what PVIs want from ATs, if they want them at all, so that resources and research can be focused where they will be most useful (Hamilton-Fletcher et al., 2016). As this study found that participants were not particularly responsive to open-ended questionnaire questions, future research could involve interviewing PVIs to understand why they do or do not look for information on ATs.
The need to develop our understanding of why PVIs are not seeking AT information, nor receiving AT information from their health care providers is highlighted by the fact that, despite agreeing that they had good knowledge of different ATs, participants reported poor awareness of the IMS Alpha, The vOICe and BrainPort devices. While this suggests that participants may have good awareness of ATs other than those asked about, it also highlights the failure for information about specific relatively new high-tech ATs to reach PVIs. As participants are not receiving AT information primarily from health care providers and are not keeping up to date with AT development, this is perhaps unsurprising, further highlighting a need to understand why PVIs are not seeking or receiving as part of their health service AT information.
As only three participants reported using an AT device, limited generalisations about satisfaction with devices can be made; however, the findings are in line with previous research. The Miniguide user reported good device satisfaction. This is in line with Roentgen et al.’s (2012) findings that other users were satisfied with the device’s qualities such as discrete size, lightweight nature, and the ability to switch between visual-to-auditory and visual-to-tactile substitution. The Miniguide user in this study reported that their device was used for spatial awareness, particularly awareness of other people to provider a higher sense of confidence and security. This sentiment is echoed by other PVIs as a reason for AT use (Hersh, 2015).
The BrainPort user’s notable dissatisfaction with the positive impact of their device reflects criticism that despite being able to significantly improve ability on laboratory tasks (Grant et al., 2016), it does not aid functioning in daily life (Manduchi & Coughlan, 2012; Upson, 2007). The BrainPort user reported ambivalence towards device satisfaction, suggesting that the more physical aspects of the device were neither satisfying nor dissatisfying. BrainPort has been criticised for being uncomfortable (Upson, 2007), though some users noted that the discomfort is not insurmountable (Kastrup et al., 2009), perhaps explaining the user’s ambivalence.
While iPhone/laptop are not specific sensory substitution devices, this participant’s report of their use as AT is valuable within the wider context of AT research, particularly regarding the integration of sensory substitution technology into existing devices. The iPhone/laptop user’s satisfaction with their mobile devices reflects the findings of previous studies indicating that AT on mobile devices has been well received. Griffin-Shirley et al. (2017) found that 95% of PVIs used a mobile device, and that more than 90% of these participants reported using specialised applications. Of those individuals, 95.4% considered the applications to be useful, and 91.1% considered them to be accessible. This rate of uptake far exceeds that of rare dedicated sensory restoration or substitution device use (Elli et al., 2014; Griffin-Shirley et al., 2017). The participant in this study used their devices mostly for interaction with the digital world, but also for GPS navigation. Previous research has found that independence in mobility is highly valued by PVIs (Quinones et al., 2011). Thus, the fact that mobile devices can integrate this accessibility feature as well as others is highly beneficial; especially as PVIs prefer AT on their smartphones to integrate multiple assistive functions into one device (Hamilton-Fletcher et al., 2016). This benefit makes smartphone AT convenient (Senjam, 2021), economical, and relatively discrete in comparison to sensory substitution and restoration specific devices.
The benefits and popularity of integrating AT with common mobile devices, such as smartphones (Vailshery, 2021), indicate a valuable direction for AT development. Advances in computer science have created a rise in artificial intelligence (AI) AT applications for smartphones, often for free (Kugler, 2020). These aim to assist with functions such as object identification, facial identification, emotion identification, typed and handwritten text reading, and scene description (Parikh et al., 2018; Qureshi et al., 2021). Moreover, AI technology is being used to create ATs to assist with social interaction (Microsoft, 2021; Salido et al., 2016). This is particularly beneficial as sensory substitution devices are currently limited in their ability to assist with social interaction and aesthetic subtlety (Phillips & Proulx, 2018). Furthermore, these AI systems focus on providing practical aids to PVIs without struggling to follow through on promises of sensory experiences (Lenay et al., 2003), as sensory substitution and restoration devices do. While sensory substitution and restoration devices continue to improve to meet the needs of PVIs, a focus on the development of AI smartphone applications for PVIs may be highly valuable and preferable in the near future. The AI applications are simple in operation (Kugler, 2020), requiring less cognitive effort than sensory restoration and substitution devices where experiences have to be interpreted. Moreover, many applications with different purposes can be downloaded onto one device, which many PVIs already have: the smartphone (Griffin-Shirley et al., 2017). Much of these AI applications are new, thus little research has been conducted on user experiences of them. Therefore, future research should compare the functional capabilities and user satisfaction of these AI applications.
However, the results for AT satisfaction needs to be viewed cautiously as only three participants out of 25 reported using a high-tech AT device and were thus able to complete the satisfaction domain. Furthermore, only two participants reported using a sensory restoration and substitution device. While this highlights the limited uptake of sensory substitution and restoration devices (Elli et al., 2014; Griffin-Shirley et al., 2017), it does limit our understanding of PVIs’ attitudes towards the devices on a wider scale, thus limiting the generalisation of our conclusions. In particular, these participants reported using their ATs for various functions, such as online access, navigation and spatial awareness; however, inferences cannot be made regarding the functions PVIs find useful due to the small sample size. Therefore, future research aiming to further investigate device satisfaction should sample from a target population of device users, such that PVI preferences around AT functions can be determined to guide future AT research and design. In addition, it is acknowledged that 25 participants is a small sample size, thus the proportion of AT users to non-AT users may not be representative of the PVI population. Moreover, a larger sample size would allow more confident conclusions to be drawn about the levels of awareness and of access to AT information within the PVI population.
Despite this limitation, this research still provides important insight into PVI perspectives on ATs and a basis for future. The strong disagreement of PVIs about health care being a main source of AT information may indicate a breakdown in communication between PVIs and health care providers that should be further investigated and improved. With PVIs reporting a lack of seeking new AT information yet reporting good knowledge of AT devices, future research could also investigate the dissociation between awareness and accessing of information. Focus group studies may be valuable in further investigating these findings, as PVI experience with accessing AT information and interactions with health care services are complex topics. Thus, the opportunity to engage in discussion with others may help PVIs to dissect their experiences and attitudes towards high-tech ATs.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196221131746 – Supplemental material for Assessing people with visual impairments’ access to information, awareness and satisfaction with high-tech assistive technology
Supplemental material, sj-docx-1-jvi-10.1177_02646196221131746 for Assessing people with visual impairments’ access to information, awareness and satisfaction with high-tech assistive technology by Isabelle Liang, Ben Spencer, Meike Scheller, Michael J Proulx and Karin Petrini in The British Journal of Visual Impairment
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.