
Abstract
Cerebral visual impairment (CVI) is a leading cause of childhood visual impairment in Western countries. This complex condition impacts affected children’s ability to see and process visual information, affecting their learning and development. Although early intervention is beneficial, many children with CVI live with this condition without this being identified. This is, in part, due to unfamiliarity with the condition among health care and education professionals. In recent years, more information has become available, and attempts have been made to explain this condition in accessible formats, such as educational videos. For this study, students and professionals in health care and education were asked to rate their knowledge about CVI, to watch three short educational videos about CVI, and to complete a survey about the use of these videos as a tool to raise awareness and to increase understanding of the condition. The study shows that educational videos can be used effectively to raise awareness of CVI among educational and health care students and professionals. Furthermore, the study shows that there is a mix of understanding, confidence and learning styles across the key professionals supporting children with CVI. As a result, different videos are effective for different audiences and therefore no one size fits all.
Keywords
Introduction
Cerebral visual impairment (CVI) is a significant cause of sight impairment and severe sight impairment among children in the Western world (Boonstra et al., 2012; Bunce et al., 2017; Chong et al., 2019; Rahi, 2007; Rahi et al., 2003; Sahli et al., 2021; Teoh et al., 2021). The prevalence of CVI among children appears to be increasing, related to the improved survival rate of premature children and improved treatment of other types of brain injury (Kozeis, 2010; Philip & Dutton, 2014). Children can have different functional presentations, depending on the affected brain area (Dutton & Bax, 2010, pp. 65–66). Some children experience visual dysfunctions despite relatively good visual acuity, while other children have profound visual impairment involving primary visual functions as well as higher visual processing dysfunction (Chokron et al., 2020; Williams et al., 2021). Children with additional support needs are more at risk of having CVI than typical children (Donaldson & Karas, 2020; Gorrie et al., 2019). In order for children with CVI to function optimally in a classroom or school environment, their CVI needs to be understood, so that learning material can be adapted and strategies to minimise the effect of their visual dysfunction can be taught (Oakland et al., 2000). It appears that many children in both special and mainstream education experience visual dysfunctions not previously identified (Black et al., 2019). Teachers value information-sharing from medical professionals, to tailor their teaching approach to the individual needs of their pupils (Black et al., 2019; Chokron et al., 2021; Davies, 2013; Goodenough et al., 2021; Pease et al., 2021). A basic knowledge about the subject would improve their general understanding of the topic, so that specific needs are appreciated in context. Effective management of CVI requires a team effort from medical and education professionals as well as the caregivers (Erickson et al., 2007; Fellenius et al., 2001; Hyvärinen, 2009; Sahli et al., 2021). Children benefit from early intervention as vision plays an important role in developing cognitive, language, social and motor skills (Baird et al., 1997; Erickson et al., 2007; Hyvärinen, 2009; Lueck & Dutton, 2015; Micheletti et al., 2022; Morgan et al., 2021; Sahli et al., 2021; Spolidoro et al., 2009). However, it appears that many families struggle to get a timely diagnosis for their children due to a lack of familiarity with CVI among relevant professionals (Goodenough et al., 2021). CVI is not systematically taught in undergraduate programmes for eyecare professionals, and therefore the responsibility to identify and manage CVI may not be assumed to be part of their job role (Harpster et al., 2022; Mazel et al., 2019; Pilling et al., 2023).
The aim of this study was to evaluate three short videos on the topic of CVI in terms of their use as a tool for raising awareness and increasing understanding of the condition among students and professionals in health care and education. Participants’ level of self-perceived knowledge was documented before and after watching the videos.
Methods
The study used the following three videos:
The Tale of the Curious Mechanic (TCM); courtesy of Rachel Pilling, Bradford University
CVI Virtual Reality Simulation (VRS); courtesy of Andrew Blaikie, St. Andrew’s University
CVI Formal Lecture (FL); produced by Cirta Tooth (2022)
The TCM video explains the concept of CVI through an analogy whereby a person is having difficulties driving their car. It turns out that the driver is healthy but that the car has many defects, leading to difficulties with navigating and controlling the car. Similarly, a person with CVI has visual dysfunctions related to brain damage or malfunction, while their eyes may be healthy.
The VRS video explains CVI through video simulations of visual dysfunctions in the classroom setting and in a beach scene. Explanation is given about brain areas that serve vision. In the end, the effect of decluttering is demonstrated.
The FL video explains CVI systematically, whereby the visual pathway from the eyes to the brain is described, as well as the higher visual processing centres in the brain. Common visual dysfunctions related to damage or malfunction of the primary cortex, occipital, and parietal lobes are explained using images.
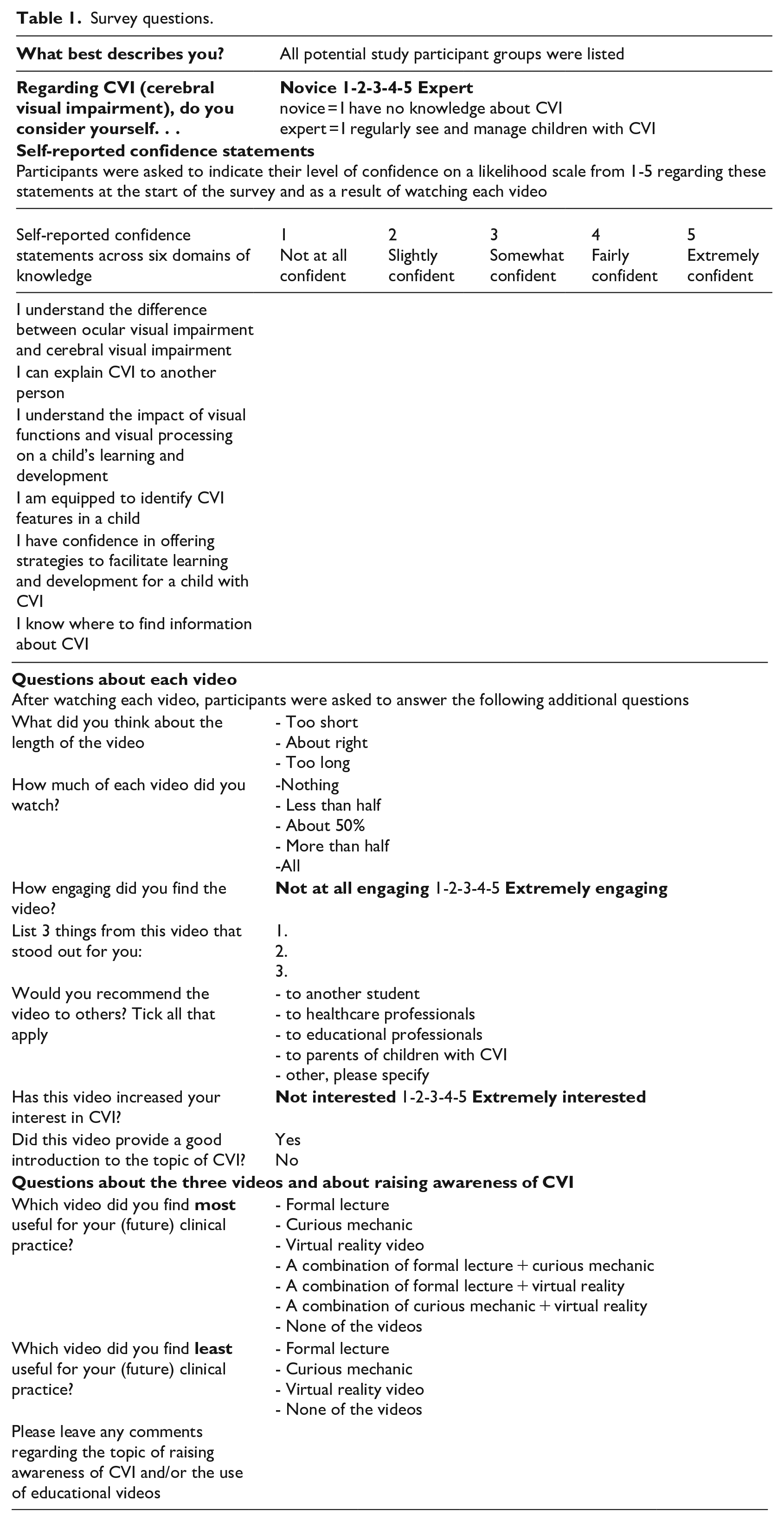
The three videos were embedded in an online questionnaire for which participants received a link. Videos were watched in a random order. Participants were recruited via email, social media posts, and university platforms in England, Scotland, and Wales. Responses were collected from ophthalmologists, optometrists, orthoptists, qualified teachers for the visually impaired (QTIV), teachers, learning assistants, and students of optometry, orthoptics and QTVI. Responses were anonymous. The survey questions are listed in Table 1. For this study, SPSS (version 27) was used for quantitative data analysis and thematic analysis was carried out for qualitative data.
Survey questions.
Results
The survey link was provided to 162 potential participants, of whom 80 completed the survey. Three participants were excluded from the study as they did not provide details about their role (student or professional group). Data were analysed for the remaining 77 participants, including 14 ophthalmologists (2 trainees and 12 consultants), 21 optometrists, 9 orthoptists, 7 QTVIs, 12 students (7 optometry, 1 QTVI, and 4 orthoptics) and 14 education professionals (6 mainstream teachers, 4 teachers in special education, 3 mainstream learning assistants, and 1 learning assistant in special education).
Group characteristics
Respondents were asked to rate their general level of experience and knowledge about CVI before viewing the videos. Figure 1 shows that orthoptists and ophthalmologists rated themselves significantly higher than educational professionals and that optometrists’ ratings were significantly lower than the ratings from ophthalmologists (Wilcoxon, p < .05 analysis and Bonferroni post hoc analysis, p < .003).
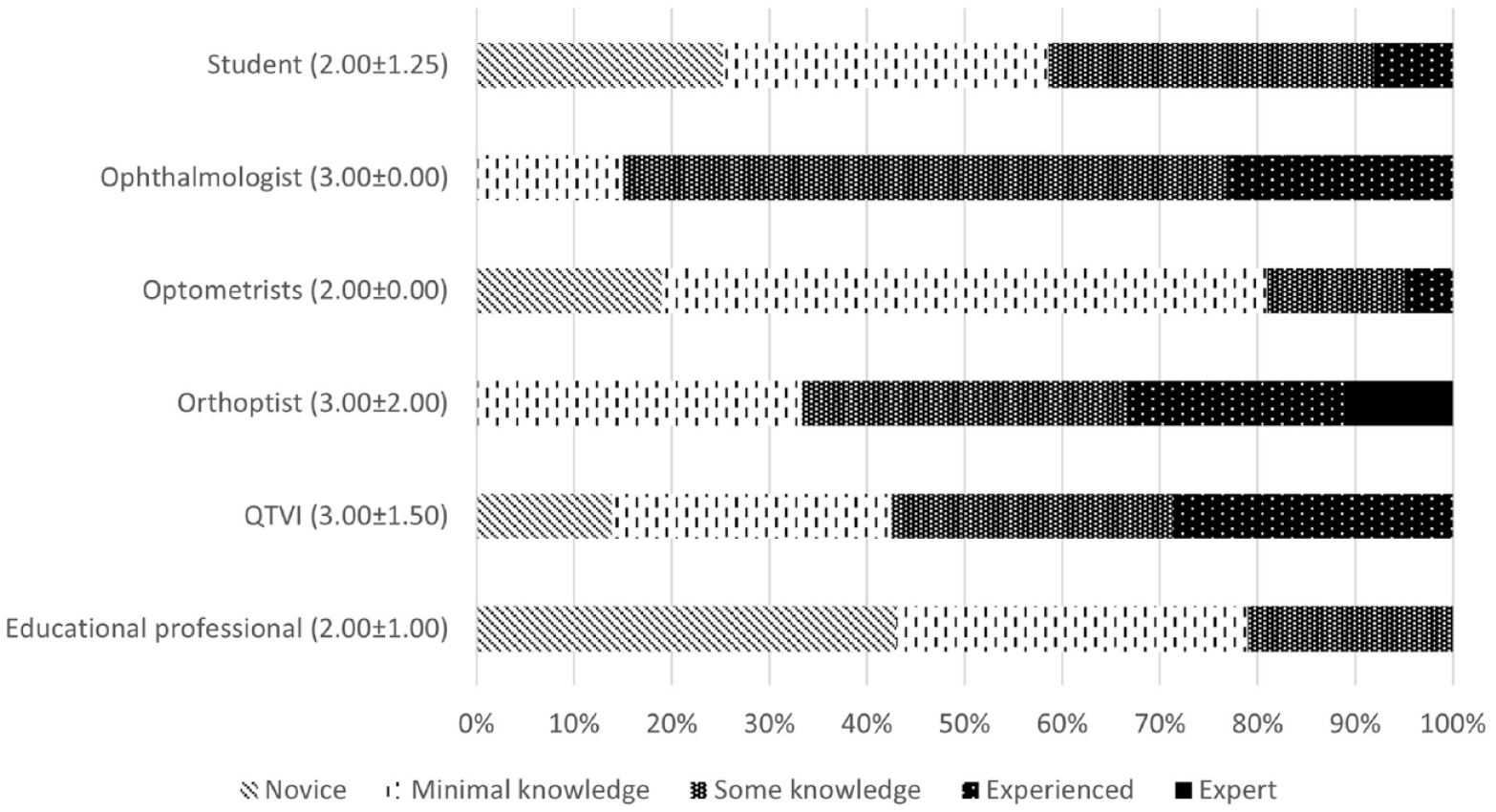
Self-perceived level of experience and knowledge about CVI prior to watching videos. Median and IQR (inter quartile range) are indicated for each group in brackets. Patterned bars provide a breakdown of ratings within groups (%).
Next, respondents were asked to rate their confidence across six domains of knowledge on a likelihood scale from 1 to 5, documented as the ‘Domain Score’ (DS). An average score across the six domains was calculated to derive an Average Domain Score (ADS). This showed that QTVIs rated themselves the highest (ADS = 3.60 ± 1.09), followed by orthoptists (ADS = 3.20 ± 0.88), students (2.93 ± 0.88), ophthalmologists (2.90 ± 0.62), optometrists (2.22 ± 0.98), and education professionals (2.04 ± 0.80). Education professionals were more confident about the impact of CVI (3.21 ± 0.97), compared to other domains. Ophthalmologists had confidence in understanding (DS = 3.86 ± 0.77) and explaining CVI (DS = 3.79 ± 0.70), but felt less confident about identifying CVI (DS = 2.50 ± 0.94) or offering strategies (DS = 1.86 ± 0.77). Orthoptists (DS = 3.22 ± 1.09) and QTVIs (DS = 3.00 ± 1.41) were more confident about identifying CVI, compared to other groups.
Domain scores before and after watching videos
Friedman (p < .05) and post hoc Wilcoxon (Bonferroni correction 0.05:6 = 0.008) tests showed that there was a statistically significant increase in ADS after watching each video for ophthalmologists, optometrists, and education professionals. For the students, QTVIs and orthoptists, the improvement was not statistically significant (see Figure 2). Friedman (p < .05) and post hoc Wilcoxon (Bonferroni correction 0.05:3 = 0.015) analysis for the whole sample showed that the FL video (ADS = 3.73 ± 0.70) had a significantly higher score for ADS than the TCM video (3.31 ± 0.87) and the VRS video (3.57 ± 0.78). Friedman (p < .05) and post hoc Wilcoxon (Bonferroni correction 0.05:3 = 0.015) analysis showed that the VRS video and FL video had significantly higher scores compared to the TCM video in the domains of ‘Impact of CVI’, ‘Identifying CVI’, and ‘Strategies for CVI’. In addition, the FL video scored higher than the other videos in the domain of ‘Information about CVI’ (see Figure 3). Of note is that the ophthalmologists’ rating for ‘identifying CVI’ increased from 2.5 ± 0.94 before watching videos to 3.21 ± 0.97 after TCM, 3.36 ± 1.15 after VRS and 3.5 ± 1.09 after FL.
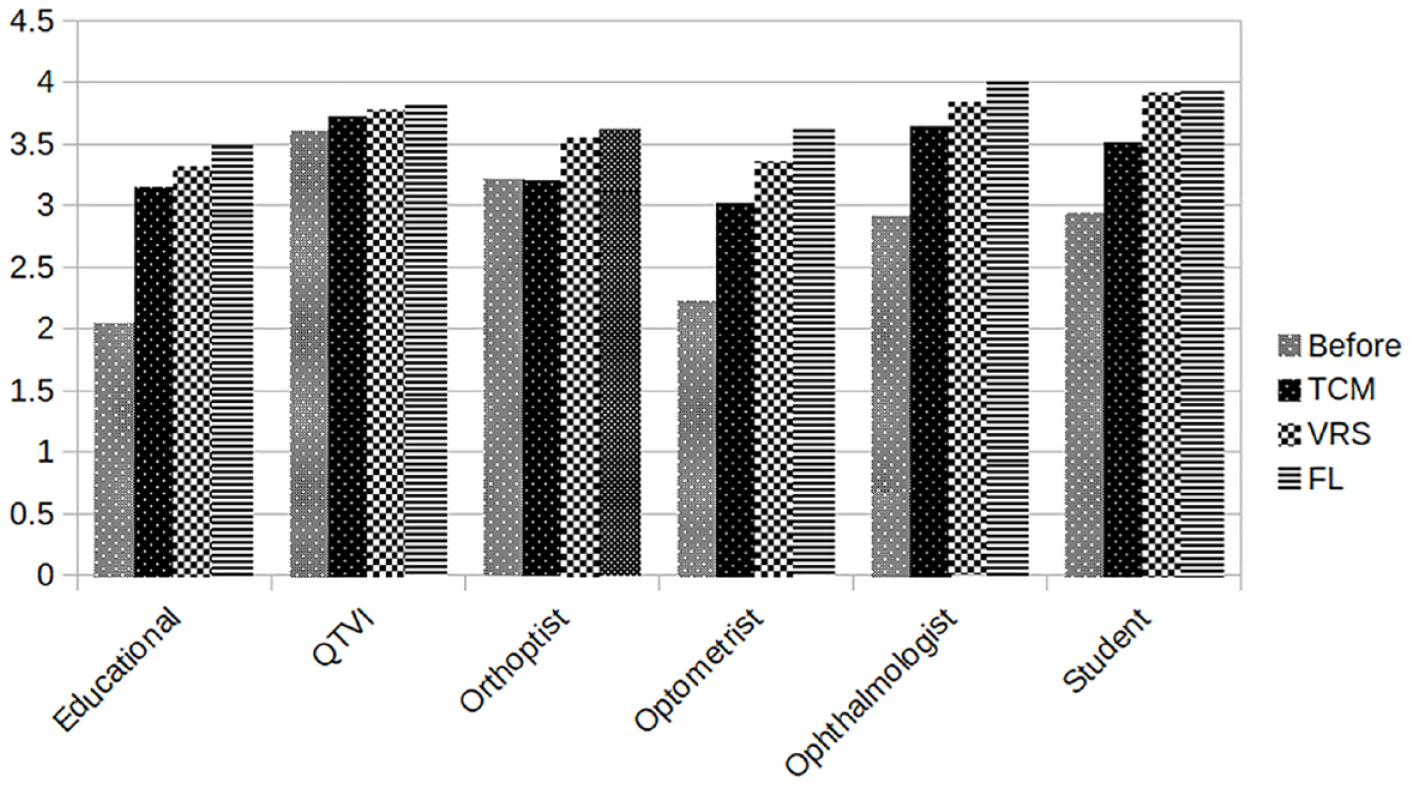
Average domain scores (ADS) across the six domains of knowledge from each group before and after watching the videos. The orthoptists and QTVI’s gained the least benefit from watching the videos.
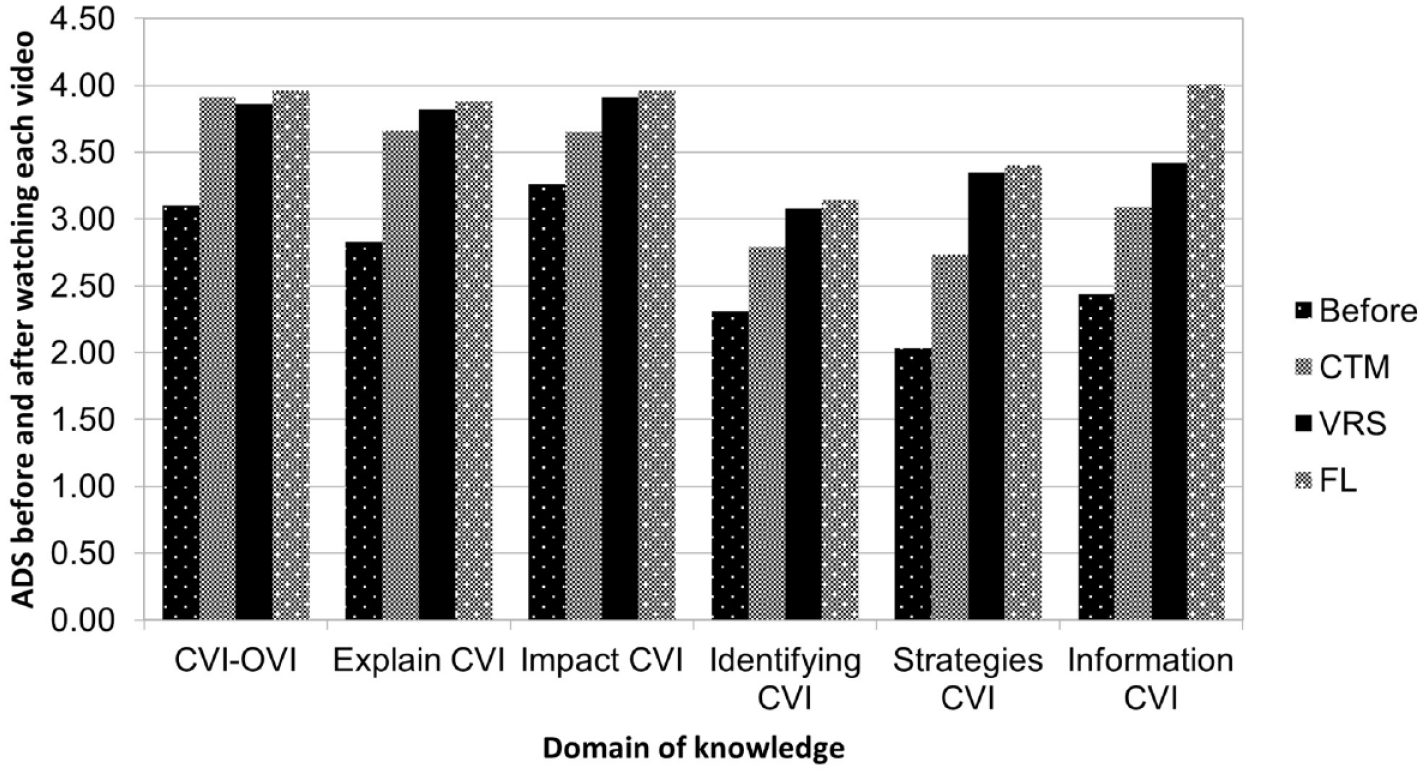
Scores per domain of knowledge before and after watching each video for the entire sample.
Video characteristics
The majority of respondents watched the videos from start to finish (TCM = 89%, VRS = 89%, FL = 96%) and considered the length of the videos to be appropriate (TCM = 70%, VRS = 93%, FL = 88%). Each video was deemed suitable as a tool to introduce CVI (TCM = 82%, VRS = 89%, FL = 97%).
On a scale from one to five, with five being ‘not at all engaging’ and five being ‘extremely engaging’, the average scores were 3.78 ± 0.98 for the TCM, 4.12 ± 0.99 for the VRS and 4.06 ± 0.69 for the FL video. Scores for ‘increased interest’ were 3.67 ± 1.04 for the TCM, 4.03 ± 0.89 for the VRS and 4.05 ± 0.84 for the FL video. Friedman (p < .05) and Wilcoxon post hoc analysis (Bonferroni correction 3:0.05 = 0.015) demonstrated that the VRS video was deemed more engaging than the other videos, and the TCM video triggered the least interest in CVI. Respondents were more likely to recommend the videos to adults than to children. The TCM and VRS videos were thought to be more suitable for patients with CVI than the FL video, while the FL and VRS videos received more recommendations for professionals in health care and education. The FL video appeared most suitable for students. Respondents were asked which video(s) they found most and least useful for their own practice. The FL video was thought to be most useful on its own or in combination with one of the other videos, while the TCM video was thought to be least useful (see Figures 4 and 5).
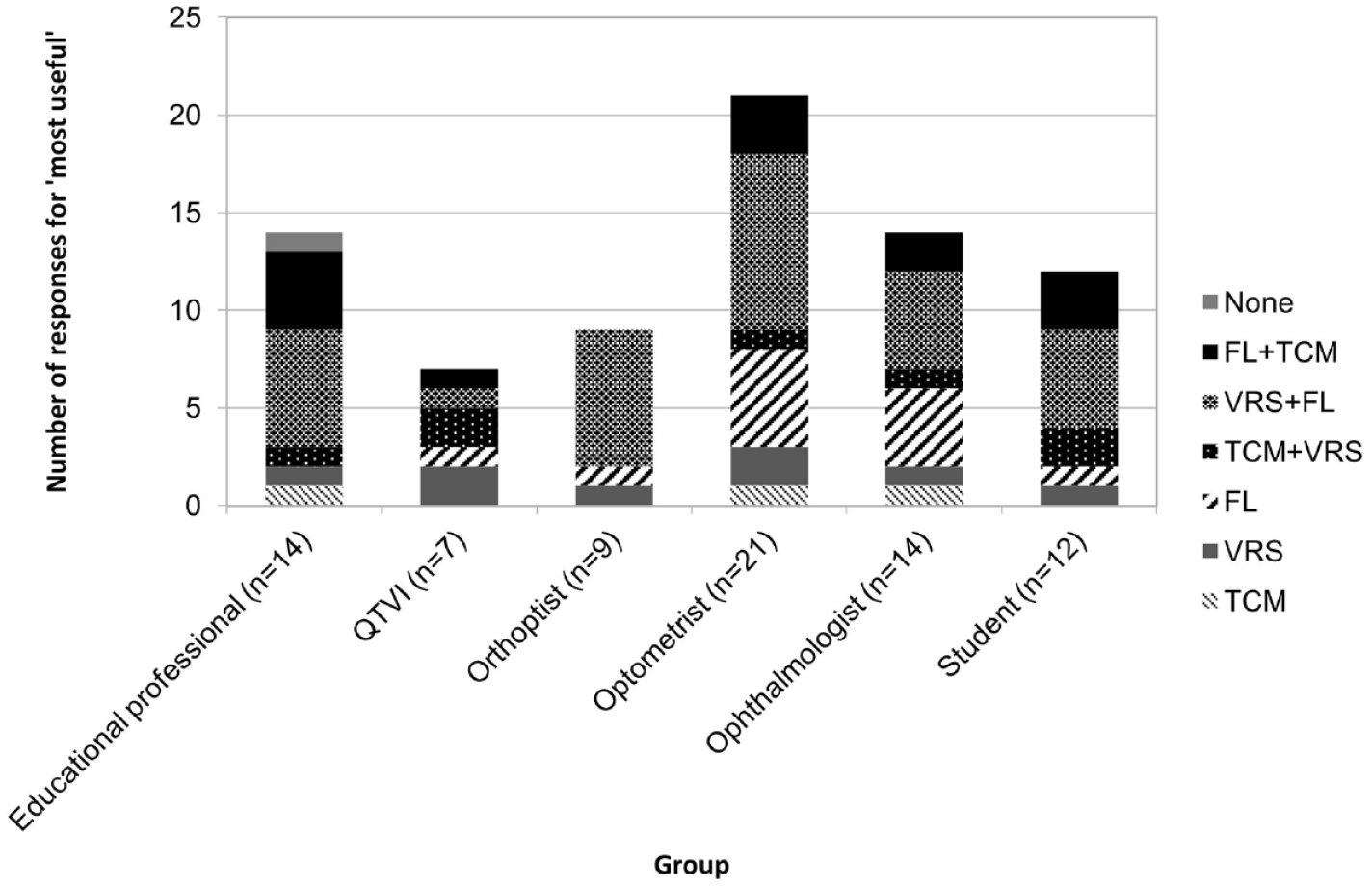
Most useful video(s) for future practice per group of respondents (number of responses per video or video combination for each group).
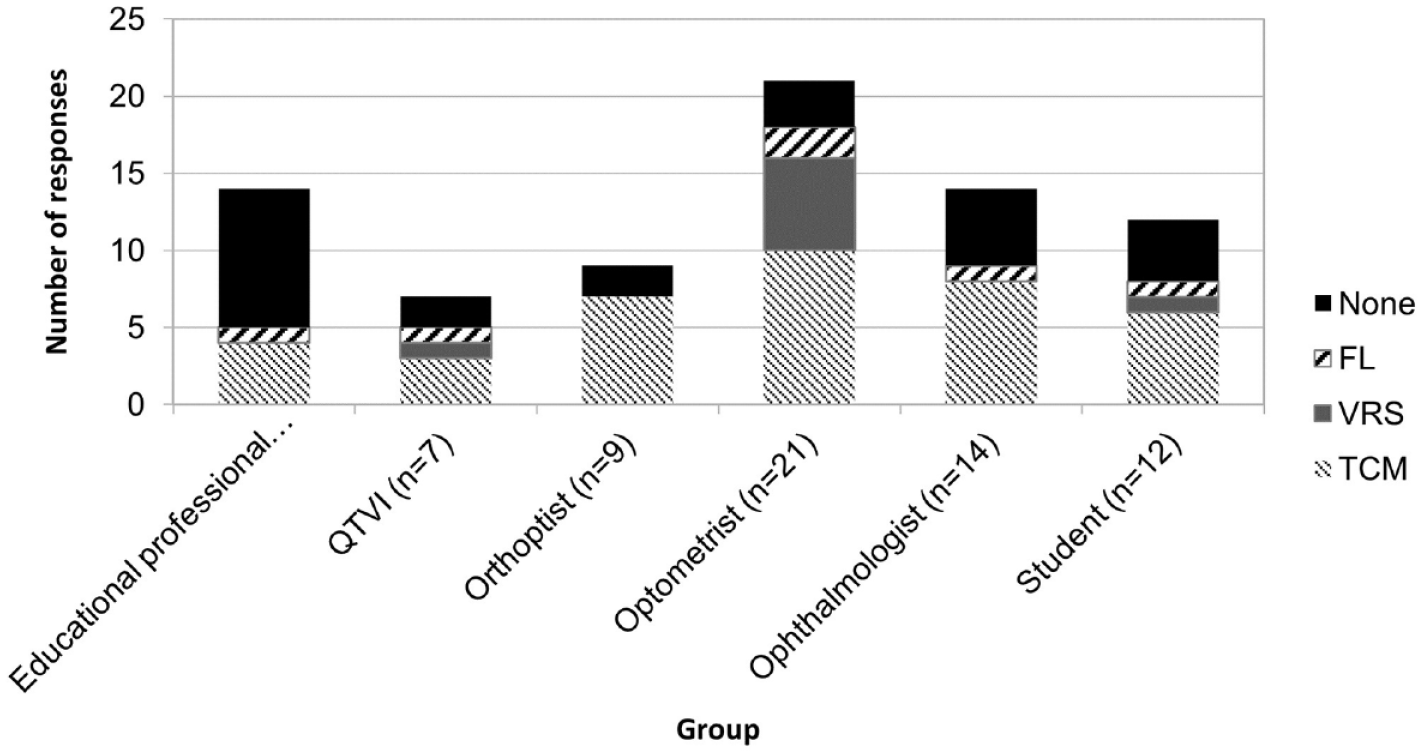
Least useful video for future practice per group of respondents.
Thematic analysis
The six main themes which emerged from the analysis of the responses to open questions were:
Presentation style;
Use of analogy/virtual reality simulations/images;
Facts and statistics;
Assessment and management;
Recommending the videos to others;
The use of videos to raise awareness.
Although each video had a very different presentation style, they were all considered to be easy to understand, well-structured, and engaging by the majority of respondents.
A significant number of respondents appreciated the analogy of the TCM video and found it ‘memorable’ (mainstream teacher) and a good way to communicate the information (orthoptist). However, a small number of respondents found it ‘confusing’ (e.g., optometrist, orthoptic student) or a ‘weird premise’ (teacher in special education). Overall, the analogy was perceived to explain the difference between ‘seeing and processing’ well (teacher in special education). The simulations in the VRS video made the concept of CVI easy to understand. ‘Seeing through the eyes of the child was very impactful’ (teacher special education). The use of images in the FL video was appreciated by a number of respondents as it helped them to ‘visualise what the patient sees’ (optometry student).
Many comments were made about the facts and statistics presented in all three videos. The TCM video emphasised the difference between OVI (ocular visual impairment) and CVI and the particular problem with processing visual information. The VRS video clearly explained dorsal stream dysfunction, visual field impairments, and reduced contrast sensitivity. The FL video explained the visual pathways and the unique combination of visual dysfunctions in every child and how these impacted on everyday function. Each video mentioned the estimated prevalence of CVI within schools. Overall, respondents were surprised about the high prevalence.
The TCM video communicated well that history taking is important in children with suspected CVI, and in particular, the types of questions that need to be included, as a QTVI explains: The need to ask the right questions with CVI: The need to ask how someone sees and not just what they see
The VRS video appeared to be effective in explaining that conventional strategies, such as making things larger, do not always work for children with CVI and that decluttering is often a more effective strategy.
The FL video presented a range of visual dysfunctions, which explained children’s visual behaviour. An optometrist commented that this video presented ‘more tips on how to help. . .[children]. . . cope with various impairments, compared to other videos’. A number of respondents commented on the simplicity of some of the strategies mentioned in the FL video. Participants appreciated the slide with websites for further information.
Recommendations were made for each video to be watched by others, including patients, carers, professionals in health care and education as well as policymakers. The TCM video was particularly thought to be accessible for people without prior knowledge about the condition, including patients and parents. The VRS video was recommended for researchers. An orthoptic student felt that the FL video was perfect for anyone wanting to genuinely see what it would be like to see and know about CVI. The images and phrasing make it easy to understand and digestible and offer exactly what we need to know and want to know at an introductory level
Professionals and students with different background knowledge and skills commented on the benefit of having the topic explained from different angles: ‘All three videos were useful, really. The Car Mechanic is really good for explaining what CVI is using an analogy. The formal lecture is really good at a quick comprehensive sweep of the many different ways CVI can present. And the virtual reality is a good way of getting people to see how some people with CVI actually engage with the world visually. More people should see any and all of these videos’. (teacher special education)
After watching the videos, respondents recognised the need to raise awareness of CVI: I believe it’s really important for teachers to know about CVI in children since they might well have a child in their class with undiagnosed CVI (teacher special education) Need to educate particularly the health professionals and teachers (ophthalmologist)
Discussion
The use of educational videos to raise awareness of CVI
We set out to investigate the use of educational videos to raise awareness of CVI among education and health care students and professionals, and to aid their education. Overall, the videos were well received. They created an interest in CVI and were judged to be suitable means for bringing this topic to the attention of the target groups. The study also provided data concerning self-perceived knowledge about CVI among the study groups.
In our study, ophthalmologists, orthoptists, and QTVIs rated themselves higher than optometrists, teachers, and students on a number of domains of knowledge and experience of CVI. However, even within these confident groups, the level of knowledge was not consistent. Only 23% of ophthalmologists, 22% of orthoptists and 29% of QTVIs rated themselves as ‘experienced’ in the topic. In the majority of respondents, their confidence in understanding and explaining CVI to others did not translate into confidence in identifying CVI or to implementing habilitation strategies. These findings are similar to other studies, which have reported that health care and education professionals have limited knowledge about identifying and managing CVI in children (Blackstone et al., 2021; Harpster et al., 2022; Maitreya et al., 2018; Oliver et al., 2023). Each child with CVI has a unique combination of visual strengths and difficulties, which need to be carefully considered to ensure that appropriate support is offered. Diagnosis and management of CVI are complex clinical skills which are too complex to be addressed in an introductory video.
The ophthalmologists, optometrists, and education professionals benefitted the most from watching the videos in terms of self-rated knowledge, especially true for the FL video. Videos with high information content, such as the FL video, tend to enhance self-perceived conceptual knowledge (Wijnker et al., 2019). In terms of explaining the difference between CVI and OVI and providing the facility to explain CVI to another person, the three videos were equally effective. However, the TCM video scored lower than the other two videos in the domains of understanding the impact of CVI, ability to identify and manage CVI, and ability to offer strategies. These domains are examples of procedural knowledge, which can be developed using key feature scenarios and problem-solving tasks (Schmidmaier et al., 2013). It is possible that the simulations of real-life scenarios through videos and images in the VRS and FL videos were responsible for this difference in self-rated confidence in these domains of knowledge, as the use of video animations can be effective in improving knowledge among health care professionals (Knapp et al., 2022). In recent years, the use of virtual reality in ophthalmic education, diagnostics, and therapeutics is becoming more common and appears to have potential, although more studies are required to evidence its effectiveness (Iskander et al., 2021; Ong et al., 2019). Similar to other educational videos (Hurtubise et al., 2013), the videos used in this study provided a concise and simplified explanation of the topic in an engaging manner. Novelty increases the chance of getting the message across (Wijnker et al., 2019). The analogy in the TCM video and the virtual reality simulation in the VRS video employed this principle. The video animations in the VRS video and the images in the other videos served to aid visualisation of the concepts and make the videos more engaging and entertaining. Respondents found the VRS video the most engaging, while the TCM video triggered the least interest. The FL and the VRS video (to a lesser extent) were deemed to be most useful for future practice, which may be due to their practical content in terms of recognising CVI in a child and learning potential habilitation strategies.
The use of online videos can potentially reach a wide audience. However, the downside is that they are not tailored to the individual needs of learners. Wijnker et al. (2019) recommend the use of specific videos for explicit aims. The videos in the present study were evaluated by different groups of students and professionals in terms of their own benefit and recommendations for others. For students, the FL video appeared most suitable as it was most frequently recommended to students by all respondents, and the students also rated this video most suitable for their own future practice. For medical and education professionals, the FL and VRS videos were most frequently recommended by the respondents. Our study found that, although medical professionals felt that they understood the difference between OVI and CVI reasonably well, their confidence in identifying CVI and managing the condition was low. Ophthalmologists are expected to provide an eye examination and vision tests to identify children with reported and observed verifiable visual dysfunction suggestive of CVI (VINCYP [NHS Scotland], 2021a, 2021b). Although an introductory video cannot address this issue, the FL video improved their confidence ratings in these domains the most. Optometrists also favoured the FL video in terms of increasing their confidence in domains of knowledge and in terms of usefulness for their own practice. The TCM video received the highest number of votes for being suitable as an introduction to CVI and triggered more interest among education professionals than the other two videos. However, the FL video had the most impact on improving their self-perceived knowledge, was deemed most useful for their practice (in combination with the VRS video) and was found to be most engaging. From these findings, it appears that the TCM video may be most suitable as an initial introduction but that teaching professionals do appreciate a lecture-style video for acquiring more in-depth knowledge and understanding. Education professionals appeared to appreciate the impact of CVI with similar ratings to the ophthalmologists and higher ratings than the optometrists in this domain. Teachers are likely to encounter children with CVI in their classrooms and could potentially gain great benefit from understanding the individual needs of children. The TCM video was most frequently recommended to children and adults with CVI. The VRS and TCM videos were most frequently recommended to parents and carers. A further study could explore the use of educational videos for these groups to acquire views from these groups.
Limitations
Due to the difference in professional groups and the differences between videos, some questions were more relevant to particular videos and/or particular groups of subjects, but every effort was made to make the questionnaire as broad as possible. The participants were not required to watch each video from start to end. This was a deliberate choice to mimic a ‘real-life’ situation. The downside is that some participants answered the questions without having watched the entire video, leading to inaccurate assessments of the videos. This effect is thought to be minimal as the vast majority watched the entire video. Although the participants watched the videos in a random order, the effect of learning from each video could not be eliminated and may have caused a degree of bias. The study relies on self-reported knowledge and subjective responses, rather than measured competencies. This does not provide evidence of participants’ actual understanding of the subject or the impact of these videos on their practice. Therefore, the effect on domains of knowledge needs to be interpreted with caution. Although the survey was anonymous, a number of respondents entered a prize draw and therefore, their names were revealed to the researcher. This may inhibit the respondents from offering constructive criticism and thereby leading to positive bias. The professional and student groups were small. Therefore, while the study has provided some interesting results, no firm conclusions can be made for the entire population of the respective groups. This study was limited to optometrists, orthoptists, ophthalmologists, QTVIs, teachers, learning assistants and students of optometry, QTVI and orthoptics. A further study could explore the use of educational videos among other groups, such as occupational therapists, speech and language therapists, educational psychologists, children and adults with CVI and their carers, as well as policymakers in the areas of child health and education.
Conclusion
This study shows that educational videos can be used effectively to raise awareness of CVI among education and health care students and professionals. The simulation in the VRS video was perceived to be particularly effective in explaining what it is like to experience dorsal stream dysfunction. While the TCM video was deemed least useful for the students and professionals in the study sample, it was recommended as a suitable introduction to CVI for affected families. A further study is required to confirm if these groups would indeed prefer the TCM video over the other videos. Overall, the FL video resulted in the most significant improvements in self-perceived knowledge, especially in the domains of impact of, identifying and managing CVI across all groups and was perceived as the most useful for their practice. A combination of videos was perceived as beneficial. Due to the different starting points in terms of knowledge and confidence in the topic and the different learning styles and learning goals across the key professionals supporting children with CVI, different videos are effective for different audiences and therefore no one size fits all.
Footnotes
Ethical approval
The study was approved by the School Research and Ethics Committee (SREC) from the School of Optometry and Vision Sciences at Cardiff University and by the City of Edinburgh Council (for the purpose of recruiting schools).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.