
Abstract
Children and adolescents with a functional neurological disorder (such as functional visual disorder [FVD]) experience a lower psychological quality of life with more mental health problems than healthy controls. While there is ample research about functional neurological disorder in general, there is also a general lack of research concerning FVD and the effectiveness of treatments given to children and adolescents suffering from it. Our aim was to provide a visual overview of common topics concerning treatments of children and adolescents with an FVD. VOSviewer is a programme that extracts information (terms) from the titles and abstracts of articles to generate bibliometric networks. The results show that common subject terms are paediatrics and children. The common diagnostic terms include conversion disorder, hysterical vision disturbance, somatoform disorders, hysterical disorders, and functional (psychogenic) visual loss. Common therapeutic terms are suggestion therapy, brief psychotherapy, hypnosis, psychiatry, therapeutic processes, and suggestibility. The results give insight into the treatments that children and adolescents with FVD currently receive. We also provide directions for future studies into the treatment of FVD in children and adolescents.
Keywords
Introduction
A person with a functional visual disorder (FVD) genuinely experiences visual impairment in the absence of pathophysiological causes (Yeo et al., 2019). Psychological factors are often important to observe in relation to functional and dissociative neurological symptoms, but the symptoms are not invented by the sufferer. Most experts believe that these symptoms exist at the interface between the brain and mind, between neurology and psychiatry (Ring, 2002). The symptoms being both ‘in the brain and in the mind’ complicate treatment immensely. Patients referred to psychiatrists with FVD often feel that ‘the doctor is just saying that it’s all in the mind’. They, understandably, may feel defensive when talking to a psychiatrist which can result in an unhelpful consultation. Because of this, patients with functional symptoms have often found themselves ‘falling through the gaps’ of the system.
The need to study functional neurological disorder in children and adolescents is therefore even greater than in adults, since there is little to no knowledge on the subject related to this group.
Patients with functional neurological disorder, such as an FVD, experience a lower psychological quality of life compared to controls and score higher on mental health concerns (Kozlowska et al., 2017). The disorder can lead to severe disability (Mental Health Care Standards, 2022). Children can be moderately to severely limited in their daily functioning which in turn affects their general development. It impairs areas such as biological, psychological, and social development and has a great impact on family life (Walker et al., 2006). There is also evidence suggesting that the presence of a functional neurological disorder in late adolescents may increase the chances of severe and chronic functional neurological disorder in adulthood (Brattberg, 2004). The need to study functional neurological disorder in children and adolescents is therefore even greater than in adults, as there is little to no knowledge on the subject related to this group.
Very few studies on treatment strategies of interventions focusing on FVD are published in peer-reviewed journals. Yeo et al. (2019) report a single case study using adults (N = 2) in which different kinds of treatments were combined and indicated. Publication on adequate treatment strategies and the efficacies thereof for children and adolescents are lacking and sorely needed. However, before treatment strategies and efficacies of therapies in children and adolescents can be fully studied, it is pertinent to take a step back. The first priority is to determine what treatments are given to children and adolescents with a functional neurological disorder. To gain insight into the available treatments, a bibliometric mapping study is conducted on the peer-reviewed databases. This information can guide future research in order to determine efficacies of these treatments and may contribute to an evidence-based intervention protocol for children and adolescents with an FVD.
Method
Literature search and inclusion/exclusion criteria
Searches were done in five databases, namely: Pubmed, Web of Science, Psychinfo, Scopus, and the Cochrane Library. A list of search terms was compiled to search for articles containing any reference to a therapy for FVD in children and/or adolescents (see Supplemental Material 1). If the database allowed this, the search terms were sought only in the title and abstract of the articles.
Inclusion criteria were English articles published until 15 March 2022. These articles had to include information about children and/or adolescents (under the age of 18 years) with an FVD and the treatment thereof. Any diagnosis of FVD (with or without comorbidities) was included.
Exclusion criteria were articles about adults older than 18 years and articles in which only medical treatments were described (operations, procedures, and/or medication). Another criterium to exclude an article was if the children and/or adolescents had accommodation spasms, since these often have a functional component. No further restrictions were set. This study was preregistered in OSF registries (Schraauwers et al., 2022).
Data extraction
The search resulted in 292 articles, of which 32 duplicate articles were removed. A further three articles were removed due to a missing title or abstract. Two researchers reviewed each title and abstract of the 257 articles independently to determine their inclusion based on the inclusion and exclusion criteria. They could also specify if they were in doubt and had not reached a decision. Intercoder-agreement was 82.6% after the first round.
For the articles that did not reach agreement, a third researcher determined their inclusion based on the inclusion and exclusion criteria in the second round. These articles were again only reviewed on the title and abstracts. They could still specify if they were in doubt and had not reached a decision. When two out of three of the researchers were in accord, the article was then included or excluded.
When a conclusion had still not been reached after independent review by three researchers, these articles were reviewed in full in a third round. An accord was then reached via discussion between the three researchers.
After this, all articles were fully reviewed; five articles were excluded due to only describing adults (see Supplemental Material 2 for the PRISMA flow-diagram).
A total of 31 articles were included and subsequently imported into VOSviewer (version 1.6.18) (see Table 1). VOSviewer is a programme that extracts information (terms) from the titles and abstracts of articles to generate bibliometric networks. Normally VOSviewer defaults to the use of terms with less than 10 occurrences. However, due to the low number of results, this was not possible. Only 60% of the most relevant terms were selected for the bibliometric map. This resulted in five terms that were deemed relevant. In our case, VOSviewer defaulted to use terms with less than two occurrences, resulting in five terms. We therefore chose to use terms with less than one occurrence to enhance the number of relevant terms found. These terms were then reviewed independently by two investigators to determine the inclusion based on the before-mentioned criteria. Intercoder-agreement was 83.0% after the first round. For the terms that did not reach agreement, a third independent researcher determined their inclusion based on the same criteria in a second round. When two out of three researchers were in accord, the term was then included or excluded. For all terms, an accord was reached during the second round.
Included articles.
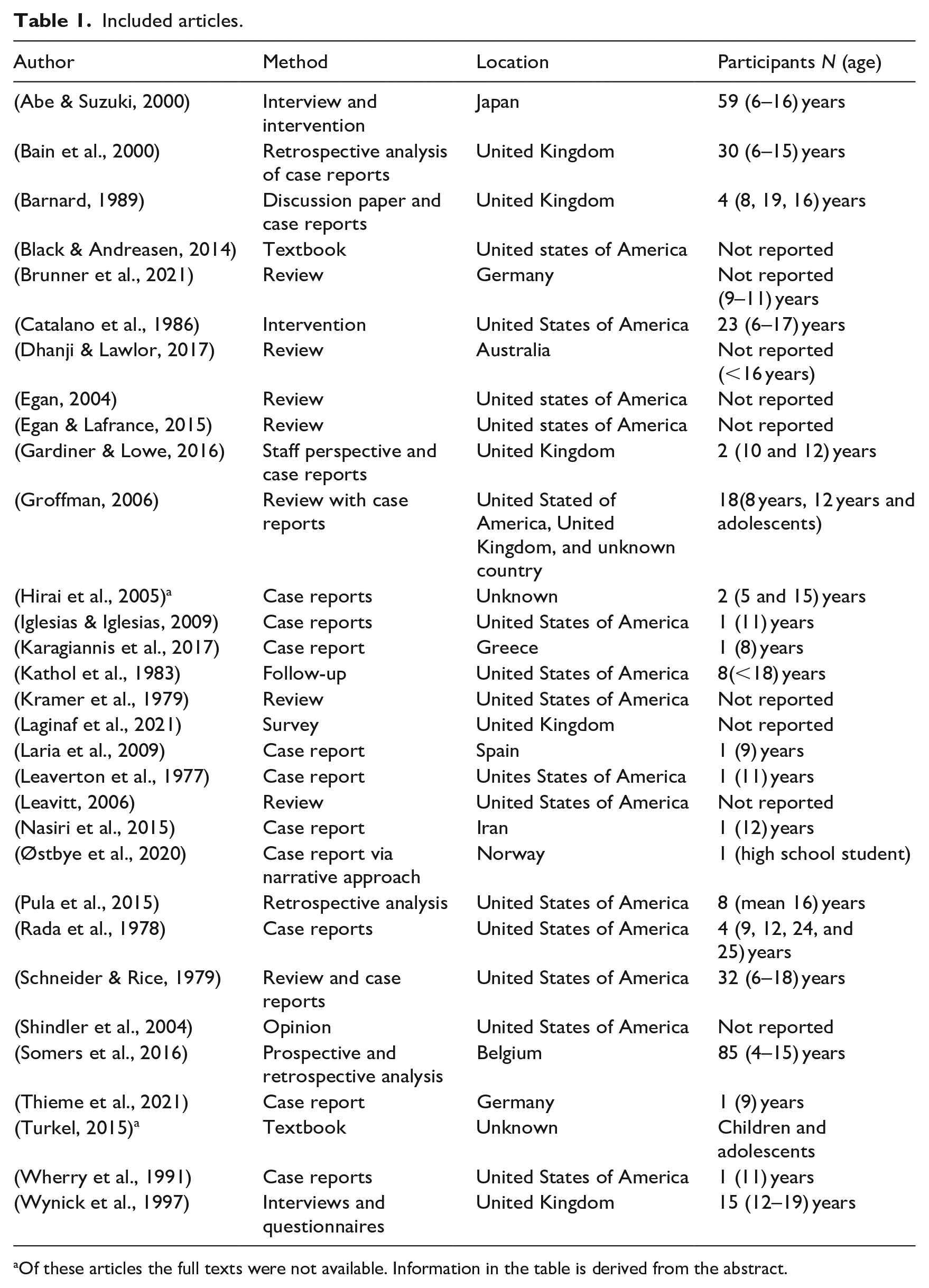
Of these articles the full texts were not available. Information in the table is derived from the abstract.
The following terms were excluded due to their generalist nature: paediatric nursing, functional magnetic resonance imaging, diagnostic and statistical manual, and case report. This resulted in a bibliometric network of 49 terms. Three terms were manually removed from the analysis because they occurred twice in the same cluster (suggestibility, vision disorders, and symptoms). One of the terms was also slightly altered, due to part of the term having been dropped by the programme, ‘Pervasive Refusal syndrome/pervasive arousal withdrawal’ changed to ‘Pervasive Refusal syndrome/pervasive arousal withdrawal syndrome (PAWS’). Two terms were merged together due to the only difference being the terms plurality/singularity. ‘Conversion disorders’ and ‘Conversion Disorder’ were merged to make the term ‘Conversion disorder(s)’. This resulted in a bibliometric network of 45 unique terms (see Figure 1).
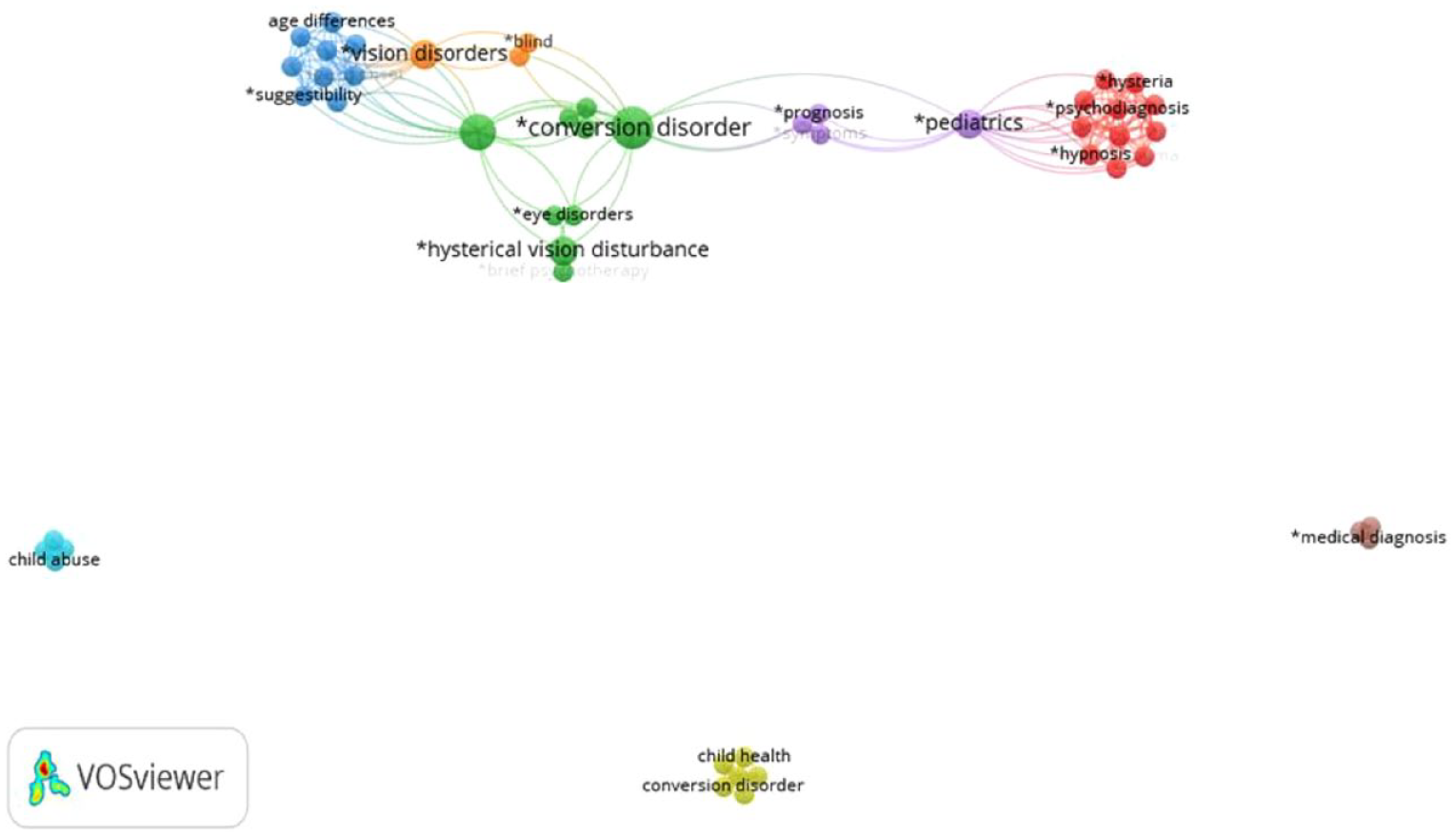
Bibliometric map of commonly used terms to describe interventions for functional visual disorders in children and adolescents.
Results
An overview of all included articles is presented in Table 1. All included articles were written between 1977 and 2021, with most articles being written after 2000. The most common forms to describe therapies for FVD in children and adolescents were via case reports or reviews. Other less-used methods that were follow-ups, interventions, interviews, questionnaires, surveys, opinion-articles, prospective and retrospective analysis, and textbooks.
The children and adolescent who were described in these articles were mostly between the ages of 4 and 19. Presumably no children younger than 4 was described in the included articles. However, for seven articles, the precise ages of the children or adolescents were not reported, while for another six articles, the age ranges were not clearly specified. Most articles were written about children from America or the United Kingdom. Other countries include Australia, Belgium, Germany, Greece, Iran, Japan, New Mexico, Norway, and Spain.
In Figure 1, the bibliometric network from VOSviewer is presented. This network consists of clusters of terms, represented by different colours. Each cluster consists of terms that are related to each other in which the difference between terms is a representation of how strong they are related (van Eck & Waltman, 2011).
Subject terms
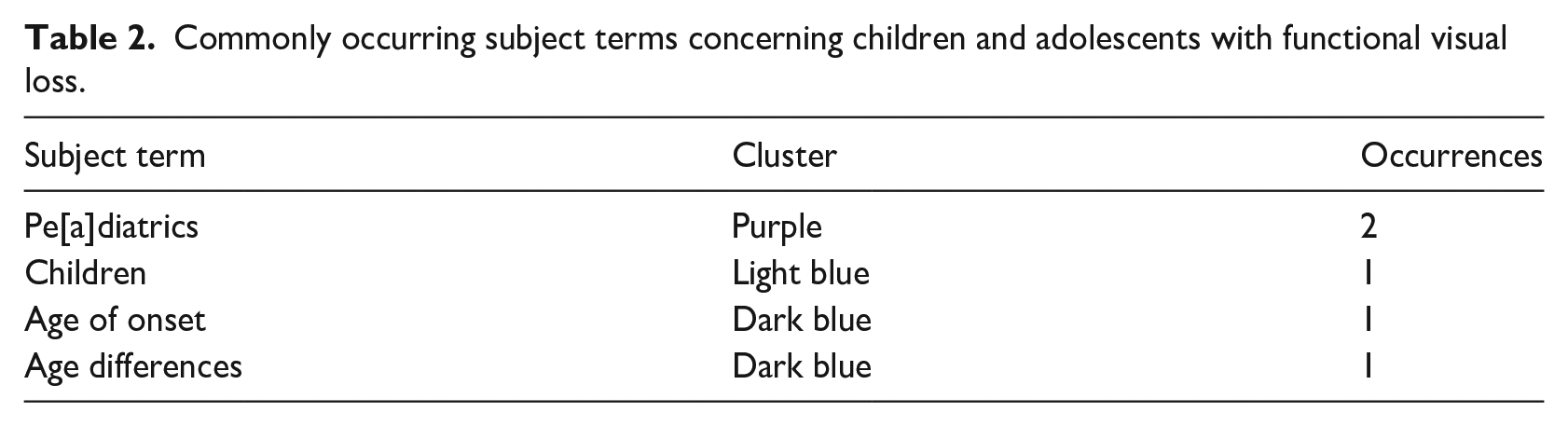
The purple cluster includes the term p[a]ediatrics. The light blue cluster includes the term children. The dark blue cluster includes terms concerning children’s ages, such as age of onset and age differences. In Table 2, we describe the categories of the subject terms and their occurrences. This shows that paediatric(s) and children are terms that are often used when describing treatments for FVD in children and adolescents, but that no specific terms to describe adolescents are used.
Commonly occurring subject terms concerning children and adolescents with functional visual loss.
Diagnostic terms
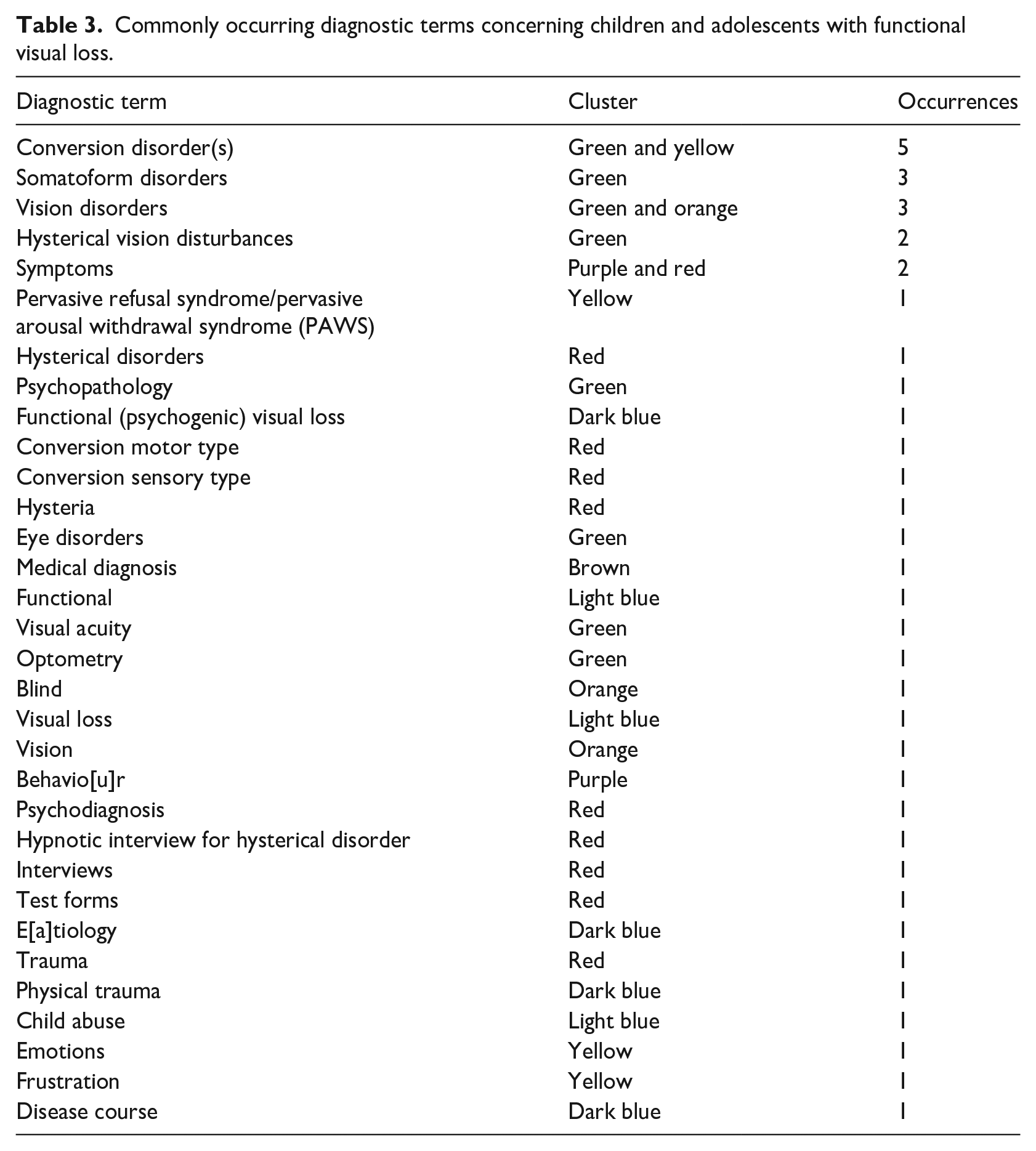
The green cluster includes terms that describe the diagnosis of FVD, such as conversion disorders, somatoform disorders, vision disorders, hysterical vision disturbances, psychopathology, eye disorders, visual acuity, and optometry. The orange cluster includes terms that describe the visual aspect of FVD, such as vision disorders, blind, and vision.
The purple cluster includes terms that describe the manifestation of FVD, such as symptoms and behavio[u]r. The red cluster includes terms that describe the diagnosis of FVD, its manifestations and the way to diagnose it, with terms such as symptoms, hysterical disorders, conversion motor type, conversion sensory type, psychodiagnosis, hypnotic interview for hysterical disorders, interviews, test forms, and trauma. The dark blue cluster focuses on FVD and its course, with terms including functional (psychogenic) visual loss, [a]etiology, physical trauma, and disease course. The yellow cluster includes other names for FVD and the emotional component of FVD such as pervasive refusal syndrome/PAWS, conversion disorder, emotions, and frustration. The brown cluster includes the term medical diagnosis. The light blue cluster includes terms that describe a possible cause for FVD and its expression in children, such as functional, visual loss, and child abuse. Some terms were present in two clusters, such as the terms conversion disorder(s), vision disorders, and symptoms. These terms also occurred often, meaning that they are important to describe FVD in children and adolescents.
In Table 3, we describe the categories of the diagnostic terms and their occurrences. This shows that conversion disorder, somatoform disorder, vision disorders, hysterical vision disturbances, and their symptoms were most often used to describe FVD in children and adolescents. Other terms used to describe FVD in children and adolescents can vary wildly and are not used often. At the same time, these terms make up the majority of the occurrences.
Commonly occurring diagnostic terms concerning children and adolescents with functional visual loss.
Therapeutic terms
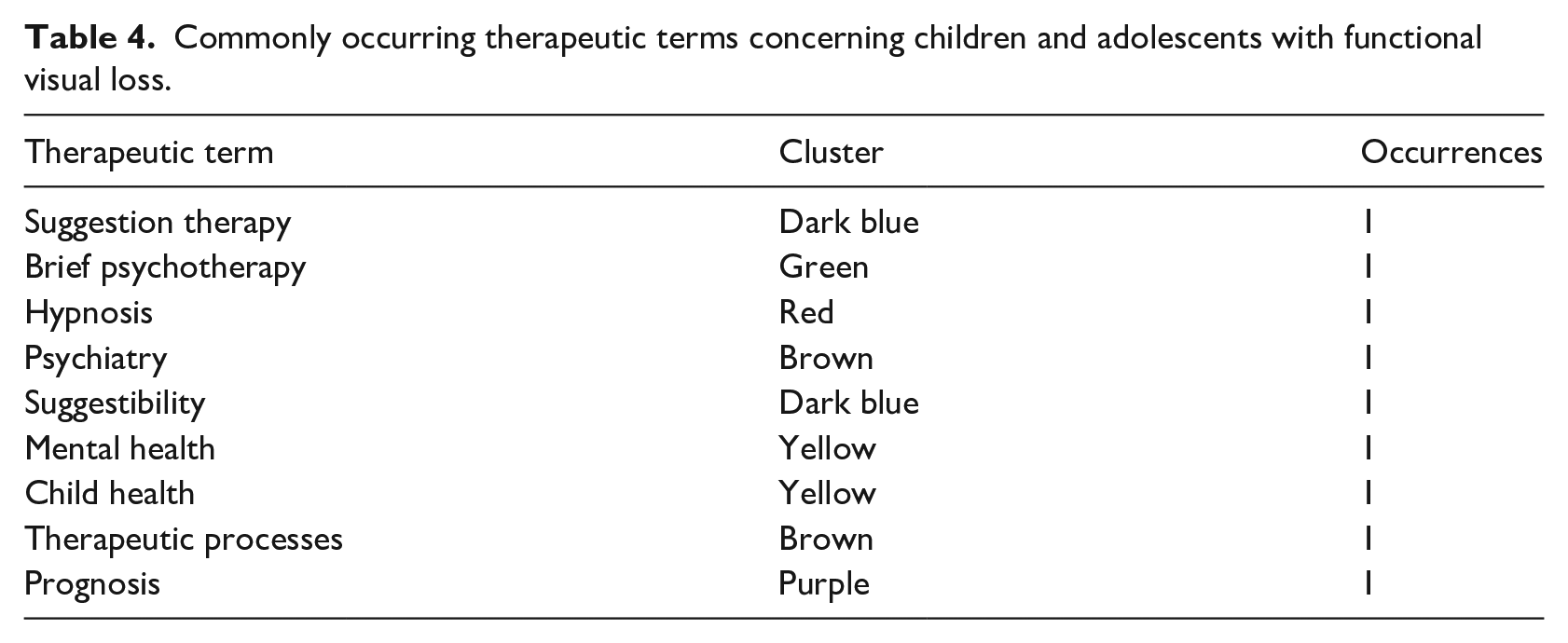
The nine therapeutic interventions were all mentioned once. The dark blue cluster includes terms that focus on the treatment of FVD, such as suggestion therapy and suggestibility. The green cluster includes the term brief psychotherapy. The red cluster includes the term hypnosis. The brown cluster also includes terms that focus on the treatment of FVD, such as psychiatry and therapeutic processes. The yellow cluster includes terms that focus on the general health of children, such as mental health and child health. The purple cluster includes the term prognosis. In Table 4, we describe the categories of the therapeutic terms and their occurrences. This shows that there is no single term that is primarily used to describe a therapy for children and adolescents with FVD. In most clusters, only one or two therapeutic terms are mentioned, which might show that there is no single therapy that is preferred by most health care professionals.
Commonly occurring therapeutic terms concerning children and adolescents with functional visual loss.
Discussion
The aim of this study was to provide an overview of terms describing children and adolescents with FVD and the therapies they have received. Generally speaking, the subject terms used for these children and adolescents with FVD are paediatrics and children, with extra consideration for the age of onset and the age differences. The mean age of the presentation of FVD in children is between 9 and 13.4 years (Bain et al., 2000; Lim et al., 2005; Mantyjarvi, 1981), but can occur as young as 4 years old (Wolpe, 1953). In adolescents, FVD occurs most often in 16- to 17–year olds (Lim et al., 2005). This coincides with the ages that were found in the bibliometric network, ranging from 4 to 19 years. The age of onset also seems important: functional neurological disorder (e.g., FVD) in late adolescence increases the chances of severe and chronic impairment during adulthood (Brattberg, 2004; Kashikar-Zuck et al., 2010; Thornton et al., 2015).
Many terms were related to the diagnosis of FVD, and these terms were kept separate from the subject terms. The most common diagnostic terms were conversion disorder, somatoform disorders, vision disorders, hysterical vision disturbances, and symptoms. However, a plethora of other terms are also used to describe FVD such as functional (psychogenic) visual loss, pervasive refusal syndrome/PAWS, and hysteria. This is in accordance with literature where a wide range of diagnostic terms are also used to describe FVD (Nicholson et al., 2011). Other diagnostic terms found focused on the diagnostic process, the cause of FVD and the expression of the symptoms. An important part of diagnosis is establishing that the child or adolescent has a visual impairment without a pathophysiological cause (Yeo et al., 2019). The terms in our bibliometric mapping associated with establishing a visual impairment and ruling out a pathophysiological cause are medical diagnosis, eye disorders, visual acuity, optometry, vision disorders, blind, vision, and visual loss. When a visual impairment is established and no pathophysiological cause is found for them, FVD can be diagnosed. Further examinations can then be done to determine the cause of FVD, as seen by terms such as etiology, psychodiagnosis, interviews, hypnotic interview for hysterical disorder, test forms, (physical) trauma, child abuse, emotions, and frustration.
Therapeutic terms that were associated with FVD in children and adolescents were suggestion therapy, brief psychotherapy, hypnosis, psychiatry, therapeutic processes, and suggestibility. Literature on FVD in adults shows that there is a focus on psychological therapies, reassurance, and follow-up as a treatment (Yeo et al., 2019). This focus on psychological treatments is also evident for children and adolescents with FVD in our bibliometric mapping. Associated terms for these therapies were mental health, child health, and prognosis. These terms make sense when placed in the context of rehabilitation, as the focus of the therapies is ultimately the child or adolescent’s (mental) health. Literature shows that the prognosis for children and adolescents with FVD is good (Pehlivanturk & Unal, 2002). However, a long-term follow-up is advised since children and adolescents can present with other psychiatric disorders even after recovery from FVD (Pehlivanturk & Unal, 2002).
Limitations and implications
This study had a few limitations. First, a search of grey literature was not performed in Google Scholar due to the restrictions posed by the database on the number of characters in a search string. A multitude of terms are used to describe FVD, and it was not possible to input all these terms for therapies and children/adolescents into the database.
Second, a plethora of terms are used to describe FVD in literature. As many terms as possible were included to describe FVD during the systematic literature search. However, it is possible that some terms for FVD were not included due to the authors not knowing these terms. This problem was addressed beforehand by reading literature pertaining to FVD and extracting terms from them to include in the systematic literature search. It can however not be ruled out that some terms were not included.
Third, not many therapeutic terms were found. This might be caused by the restriction posed by the VOSviewer programme, since this programme can only extract terms from the title and abstract of an article. It does not allow the insertion of full articles. A low number of articles were included in the bibliometric map because the therapy for FVD in children or adolescents had to be mentioned either in the title or in the abstract. It is therefore possible that therapies were not included in the bibliometric map because these were described in the full article as opposed to in the title or abstract.
Fourth, only a few terms had more than one occurrence in the included articles. None of the terms had more than four occurrences. This might be consistent with the lack of consensus of the term(s) used to describe FVD (Nicholson et al., 2011). It might also mean that there is no consensus over what treatment children and adolescents with FVD should receive.
The strength of this article is that the inclusion criteria were as broad as possible. Medical treatments (e.g., operations, procedures, and/or medication) were excluded. Next, accommodation spasms were excluded as these often have a functional component. All other treatments were included. Children or adolescents who had FVD together with other pathophysiological causes for visual impairment were not excluded. The portion of the visual impairment that cannot be pathophysiologically explained might be diagnosed as FVD and was therefore included. Due to these few exclusion criteria, we posit that this article gives a broad and thorough overview of the therapies that children and adolescents with FVD currently receive.
Conclusion
The aim of this article was to provide an overview of the themes related to therapies that children and adolescents currently receive. First, this study indicates that scientific studies into the treatment of children and adolescents with FVD are sparse. Second, the terms to describe FVD and its treatment in children and adolescents are few and seem to be not consistently applied in scientific research. These two issues give rise to several new directions for future studies into this field. First, there should be consensus about the terms used to describe and diagnose FVD. Second, a guideline should be constructed for the treatment of FVD in children and adolescents with clear names and definitions for the therapies. Third, therapies used to treat FVD in children and adolescents should be studied for their efficacy. It should not be assumed that the therapies that work for adults automatically work for children and adolescents. All these age-groups have different causes for the FVD.
It is of great importance that scientists in the field of visual impairments or in the field of functional neurological disorders see the need for further studies. At the moment, there are too many unknowns that do not benefit the children and adolescents suffering from FVD.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196231195703 – Supplemental material for Bibliometric mapping of current therapies for children and adolescents with a functional visual disorder (FVD)
Supplemental material, sj-docx-1-jvi-10.1177_02646196231195703 for Bibliometric mapping of current therapies for children and adolescents with a functional visual disorder (FVD) by R Schraauwers, ME Ketelaar and PS Sterkenburg in British Journal of Visual Impairment
Supplemental Material
sj-docx-2-jvi-10.1177_02646196231195703 – Supplemental material for Bibliometric mapping of current therapies for children and adolescents with a functional visual disorder (FVD)
Supplemental material, sj-docx-2-jvi-10.1177_02646196231195703 for Bibliometric mapping of current therapies for children and adolescents with a functional visual disorder (FVD) by R Schraauwers, ME Ketelaar and PS Sterkenburg in British Journal of Visual Impairment
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by ZonMW, grant no. 637005108.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.