
Abstract
Smartphones and applications (apps) are replacing traditional assistive technology devices for people with vision impairment (PVI) to support their mobility and independence in daily life. However, training and learning support to enable PVI to use this technology to its full advantage requires further research. A better understanding of what, and how, training and learning support is currently being provided is required to inform the future development of training and best practice in the area. This study, using an interpretive descriptive qualitative approach, aimed to explore the perspectives of trainers on the current provision of smartphone training in Australia, Canada, and Singapore. Semi-structured interviews with 22 trainers, including 13 trainers with a vision impairment, discussed how training is currently conducted, the challenges, and their ideas on what would constitute a high-quality or ideal training programme. The data were analysed using thematic analysis and six themes emerged: structure and content of training; training provides hope, independence and connection; trainers’ approach and attributes influence training; informal support and other avenues for learning; challenges associated with providing training; and suggestions to improve training. Participants highlighted that smartphone training was a source of hope for PVI and that it enabled independence. The importance of responding to clients’ emotional needs, in addition to their learning needs in an individualised and graded approach, was discussed as critical to the success of training. Trainers with vision impairment who weaved their lived experience into the training sessions found this to be beneficial to their clients’ learning and adjustment to vision loss.
Introduction
Around the globe, the number of people with vision impairment (PVI) is increasing (World Health Organization [WHO], 2022). PVI include those who are either blind or have low vision, as defined by The International Classification of Diseases 11 (2018) (WHO, 2022). In developed counties such as Australia, Canada, and Singapore, focused on in this study, the number of PVI remains high. In Canada, the percentage of PVI is estimated to reach 4% in 2023 (Asare et al., 2019), and in Australia, the number of PVIs is predicted to rise to 564,000 by 2030 (Vision Australia, 2022). In Singapore, while there is no national registry for PVI, it is estimated there are about 50,000 PVI (Wong, 2020). The provision of assistive technologies (ATs) is essential to support PVI in their participation in life (Hakobyan et al., 2013). Recent advancements in smartphone technologies have turned smartphones and applications (apps) into a useful and core AT for PVI (Borges & Mendes, 2018; Senjam, 2021). Yet, support to use smartphones by PVI has yet to catch up to the technological developments that smartphones can offer PVI.
Prior to the development of smartphones and apps, PVI relied on a myriad of AT to navigate the environment and be independent (Balata & Mikovec, 2016; Bhowmick & Hazarika, 2017; Fok et al., 2011). These AT included closed circuit televisions (CCTVs), handheld magnifiers, and Braille GPS (Irvine et al., 2014). On average, PVI could use up to six devices each, for their everyday needs (Fok et al., 2011). Smartphones have now replaced many of these devices, due to their in-built accessibility features (Martiniello et al., 2019).
These in-built accessibility features, such as screen readers, voice assistants, and zoom text, have made it possible for PVI to use smartphones as a core piece of AT (Crossland et al., 2014). Prior to smartphones, these features were only available if additional software were purchased for particular functions, thereby increasing the cost (Martiniello et al., 2019). Comparatively, coupled with abundant free or low-cost apps, such as apps for navigation and reading, smartphones can be an economical AT option because they are also an everyday technology device (Senjam et al., 2021). However, like other traditional AT, PVI need to learn how to use smartphones to optimise their functionalites to best support their participation and independence (Sankhi & Sandnes, 2020).
PVI learn to use smartphones and apps in a variety of ways, the most common method being self-teaching, followed by support from friends and family, and training sessions with an organisation (Martiniello et al., 2019; Robinson et al., 2017). Martiniello et al. (2019) reported that 69% of their 466 international participants surveyed relied on self-learning to use smartphone and only 7.5% received training from vision rehabilitation professionals. In an Australian study, 65% of participants reported that they would like to see more training being provided by their vision support organisations (Locke et al., 2021). Research in low- and middle-income countries also indicates the need for more training resources, with a study in Nepal stating that smartphone training materials should be made easily available to schools to support students with vision impairment (Sankhi & Sandnes, 2020). Some previous research have reported the value of formal training as they generally increase proficiency and promote increased use of smartphones as AT (Celusnak, 2016; Locke et al., 2021; Miskin et al., 2021; Sankhi & Sandnes, 2020; Senjam et al., 2021; Wong & Tan, 2012). However, what training is currently being provided to PVI is relatively unknown, and there is limited evidence to guide its provision, with insufficient research on the topic.
To date, two studies have specifically evaluated smartphone training programmes for PVI. Miskin et al. (2021) in the United States showed that all 337 veterans who participated in their 35-hr professional training for smartphones and tablets, became more proficient in using them, thus needing less or no help post-training. In Norway, Fuglerud et al. (2021) found that improving the provision of training and organising good post-training support are important in reaching and motivating older PVI to learn to use smartphones and apps. However, a lack of research to understand the provision of such training globally warrants further investigation to inform best practices in this area. This article, therefore, aimed to understand the perspectives of trainers on the current training landscape in Australia, Canada, and Singapore. The study aimed to answer the following research questions:
What support and/or training is being provided to PVI on the use of smartphones and apps?
What are the challenges experienced by trainers in training PVI?
What improvements would trainers like to see in the current training/support available for PVI?
Methods
Design
A qualitative approach using interpretive description (ID) was used, with in-depth semi-structured interviews conducted (Teodoro et al., 2018). ID originates from phenomenology, ethnography, and data-based theory and provides solutions to real-life clinical problems (Teodoro et al., 2018; Thorne, 2016). This method of enquiry was developed by Thorne and colleagues in the 1990s as conventional qualitative approaches, including grounded theory, ethnography, and phenomenology, could not fully be applied to clinical questions. The ID approach aims to improve clinical practice by first understanding the practice well (Thorne, 2016). ID was therefore chosen as a framework to guide this study, as the research aimed to understand the complexities of smartphone training to work towards improving training for PVI. Ethical approval for the study was granted by the Singapore Institute of Technology’s Institutional Review Board (reference no. 2020133) and The University of Queensland’s Human Research Ethics Committee (reference no. 2021/HE002105).
Participants and recruitment
Participants, who were trainers employed by organisations or self-employed, were recruited via purposive and snowball sampling in this multi-site qualitative study. Multi-site studies are carried out to obtain rich data from people working in different contexts (Bower et al., 2021; Burgdorf et al., 2022). Targeted organisations that supported PVI in Australia, Canada, and Singapore assisted in recruiting participants through advertisements or inviting their trainers to join. Eligible participants had to be proficient in English and have provided training within the last 12 months. The first author recruited the first few participants who fit the criterion for recruitment via ‘key informants’ from those organisations. These participants then recommended other participants who met the recruitment criteria, hence materialising the ‘snowballing’ sampling as explained by Thorne (2016). Recruitment ceased when avenues for recruitment were exhausted. In qualitative research using ID, Thorne (2016) states that studies will have small sample sizes of between 5 and 30. A total of 22 trainers, with 4 from Canada, 8 from Australia, and 10 from Singapore gave their verbal or written informed consent before the Zoom interviews, which lasted between 2 and 4 hrs. These trainers were diverse in their academic backgrounds and experience, thus staying true to the ID approach of ‘maximal variation’ in theoretical sampling via purposive and snowballing sampling techniques (Thorne, 2016). Diverse views from participants of diverse backgrounds are key in multi-site research, as it increases its applicability to other contexts (Jenkins et al., 2018).
Data analysis
All interviews were audio-recorded, transcribed verbatim, and managed using NVivo 20 software for thematic analysis (Creswell & Poth, 2018). NVivo 20 was used to help us manage large data sets and improves efficiency (Leech & Onwuegbuzie, 2011). The inductive in vivo open coding, recommended for the ID approach, was carried out by the team (Burdine et al., 2020). The first three transcripts were coded by the first and second authors independently, before discussing and refining the codes together. Following this, a list of initial codes was generated, and the first author proceeded to code the remaining transcripts. For rigour of the analysis and member checking, the first author kept an audit trail, and the research team regularly reviewed and discussed the preliminary coded data. Codes that were disagreed upon were altered, merged with other codes, or discarded after discussion. A set of themes and subthemes were then derived and discussed iteratively to reach the final set of themes and subthemes.
Results
The trainers had diverse professional backgrounds from allied health, education to computer science and worked mainly in community-based settings (64%). The length of experience in providing training ranged from 3 months to 13 years (average: 5.3 years). More than half of those interviewed have vision impairment (59%). Table 1 provides further details of trainers and their backgrounds.
Characteristics of participants (N = 22).
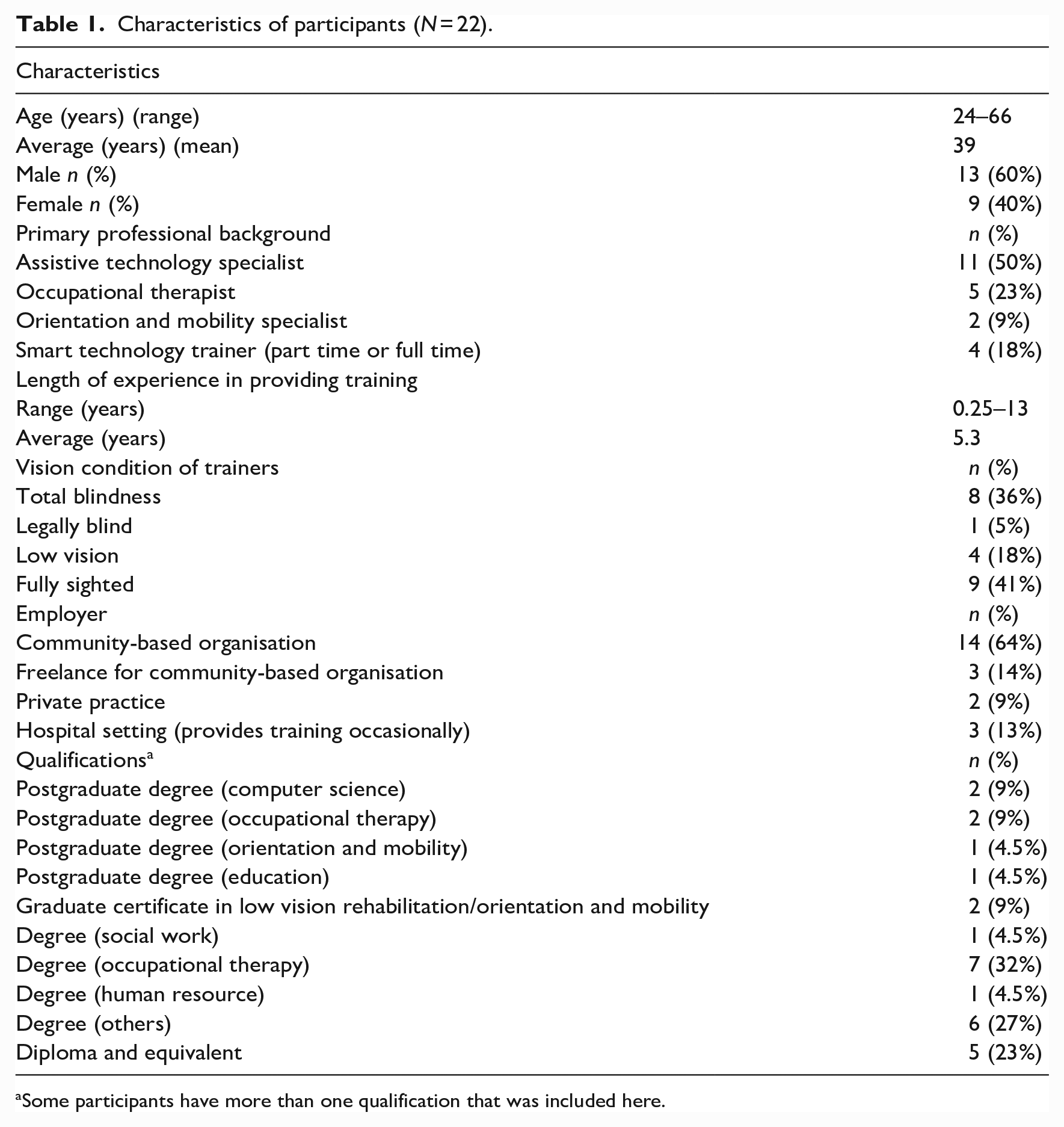
Some participants have more than one qualification that was included here.
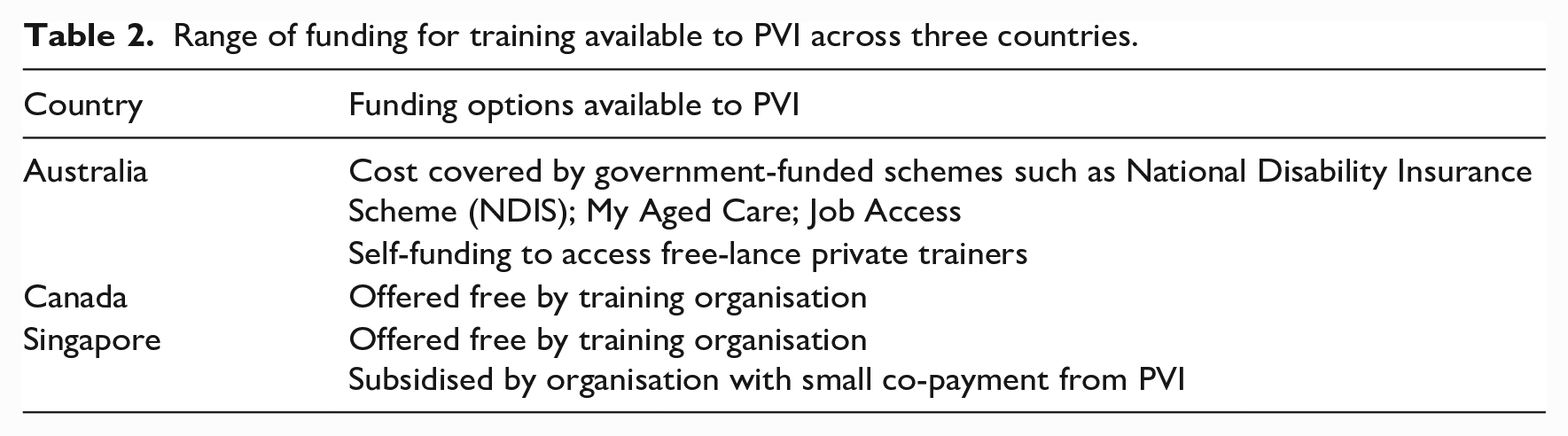
The most common clients the participants worked with were adults over 60 years old with a range of vision conditions. Their clients’ reasons for attending training differed, including recent loss of vision prompting them to learn to use the smartphones using voice control, upgrading phones, and wanting to learn new accessibility features. Training was funded by government-funded disability insurance schemes, subsidised, or offered free by organisations supporting PVI, and Table 2 shows the funding schemes in each country. Smartphones in the three countries were usually not funded, as they were deemed a mainstream device, rather than an AT device. Most trainers preferred to use iPhones because of their perceived superior in-built accessibility features for PVI.
Range of funding for training available to PVI across three countries.
The analysis derived six main themes and subthemes, as shown in Figure 1, describing the experience of providing training, including the challenges and positive outcomes. All participants, regardless of their backgrounds and roles at work, are referred to as ‘trainers’, and alphanumeric information listed before or after participants’ quotes are code names, for example, A1 denotes participant 1 from Australia.
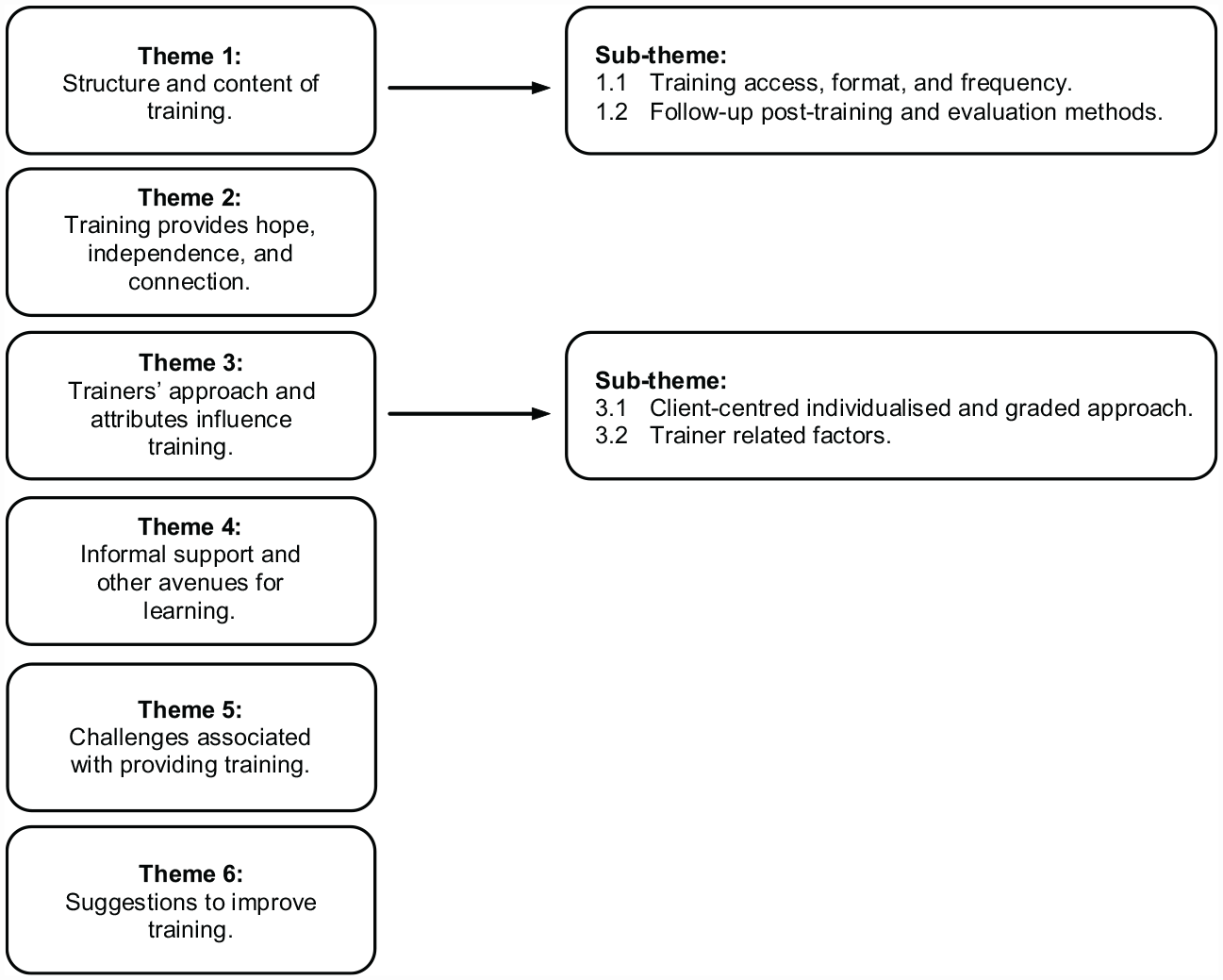
Six main themes and subthemes derived.
Theme 1: structure and content of training
This theme describes how training is currently being provided, including access to training, what clients want to learn, the format, the importance of follow-up, and what measures some trainers use to evaluate the outcomes.
Subtheme 1.1: training access, format, and frequency
In all countries, participants reported that PVI learned about training via websites or word of mouth from other PVI. Waiting lists varied, from as short as a week in Canada to a few months in Singapore. The training took place in the organisations or the homes/workplaces of PVI or occasionally in public spaces, such as cafes; or over the phone and video calls via the Zoom platform. Individual training was often preferred by the trainers as the needs of clients were deemed to be too varied to be addressed in group settings. However, group settings were seen as important for peer support as described in Theme 2.
Trainers reported that sessions were usually 60–90 min long, to suit clients’ concentration span and lessons occurred weekly or fortnightly, to allow time for practice in between sessions. The training frequency was determined by various factors, such as funding systems and trainers’ workload. Face-to-face sessions were preferred as it was more effective to use hand-over-hand guidance to teach gestures to use smartphones.
All trainers discussed that younger clients tended to want to learn to use smartphones and apps to browse the Internet and join social media while older clients wanted to learn for communication, such as receiving and making voice or video calls; texting or using voice messages and emailing. Teaching print access apps was also common, since ‘a lot of information these days are in print format’ (A1). Generally, most trainers reported that they start with teaching clients the basic skill to use in-built voice assistants such as Siri. C1 identified three basic skills he always taught before delving into more complex skills – ‘how to add a contact, how to text, and how to email’. A7 explained why these basic skills are important, ‘Once people learn, the basic use of the phone, and once they know how to navigate around . . . they can put that into practice . . .’.
Subtheme 1.2: follow-up post-training and evaluation methods
The value of follow-up post-training was endorsed by most trainers. They opined it was essential to keep clients motivated. Many trainers found it useful for clients to have training notes to practise in between sessions. Most trainers provided notes via texting platforms; email or printed notes in large print format and some would email audio recordings of the training sessions. In addition, trainers might send other resources to clients, to consolidate learning. To reinforce learning, some organisations have weekly ‘drop-in clinics’ run by volunteers. A Canadian trainer described that they would assign a volunteer (sighted or non-sighted) to teach clients for five sessions after three individual sessions with a trainer.
Some trainers measured the outcomes of training via goals set out collaboratively with their clients at the commencement of training. Other evaluation methods reported included asking clients post-training verbally or through a short-written survey, their perception of training. More extensive or standardised outcome assessments were not used due to time constraints and a lack of relevant outcome measures.
Theme 2: training provides hope, independence, and connection
This theme describes how training can provide hope for PVI, independence, and help to connect PVI to a wider community of support with peers. Trainers described that training has indirectly provided a channel to address the sense of loss commonly experienced by PVI and facilitated their acceptance of their vision loss. They reported that through their interactions with clients, they found that the smartphone training gave their clients ‘hope for the future’, that they could still participate in life, and do the things that were important to them. As S1 stated, ‘there are still a lot that they can keep up and their schedule, their routines don’t need to change’. Clients were reported by trainers to be more independent overall after training, and that they were able to get ‘out and about’ and navigate in their communities. Similarly, C2 described that her client said she can ‘know what’s around me with soundscape or I can do this independently with Be My Eyes [an app]’. A4 shared that after learning to use smartphones and apps, clients can ‘do a lot of the ticketing . . . online shopping’ and A6 said his clients can ‘bank independently . . . catch public transport’. He added, ‘the changes are phenomenal . . . how it [skills to use smartphones and apps] can provide people independence’.
Learning in groups was seen as beneficial in offering clients support from others with ‘shared experiences’, as C3 explained: ‘ . . . people can vent about the same things and laugh about things and not feel alone. You could set up buddies . . . so they call each other in between sessions to check in with each other . . .’.
Many trainers agreed that a form of support group for clients during and after lessons would enhance the effectiveness of the training sessions. Being connected to a community would provide valuable opportunities for clients to support each other emotionally and a chance to socialise. As C4 shared, ‘to be able to bring blind people together and support each other is such a powerful thing in any community’.
Theme 3: trainers’ approach and attributes influence training
This theme illustrates how different factors impact the delivery of training. This includes the value of taking an individualised approach, and trainer-related factors, including their preference for phone brands, their attributes, and perceptions of what constitutes good training. Trainers also highlighted how their lived experience helped their clients during training.
Sub-theme 3.1: individualised graded approach
All trainers discussed that they did not follow a fixed curriculum but took an individualised approach and adapted their training to fit the clients’ experience, technology skills, and learning needs. For example, they adjusted their pace of teaching and use of jargon during training, so as to not overwhelm clients. S7 shared, ‘. . . not every training will fit everyone . . . we do look in terms of . . . working out different options, or different packages to suit the clients’ requirements . . .’.
Trainers also emphasised the importance of understanding their clients from the beginning. Some trainers commented on the importance of understanding clients’ motivation and purpose for learning, in addition to what operating systems or phone models they would like to base their learning on. C1 said, ‘. . . that’s why I ask so many questions to get an understanding, of the individual and their condition and what they’re facing, and then work around that . . .’.
Trainers were also mindful to acknowledge clients’ difficulties when learning and tried to build in small successes during sessions so that clients stay motivated, as A2 explained the graded approach makes it easier: . . . we sort of get intimidated by something that’s tricky to learn . . . might not continue because we think it’s too hard to learn . . . but if we had been introduced step-by-step . . . in a bite-size, easy to learn and digest . . .
Sub-theme 3.2: trainer-related factors
Most trainers conduct training in one operating system only, most often iOS, but some would try to be well-versed in both systems, to meet the needs of different clients. Most trainers expressed that to be good trainers, they should be patient, respectful, empathetic, have good listening skills, and have a ‘passion to teach’. Other attributes discussed included regular updating of skills and knowledge, and reflecting on the training they provide to improve it. In addition, to some, a good trainer would work alongside clients to ensure that they have the skills to problem solve and troubleshoot after training, as shared by A8, ‘. . . you’re gonna learn how to solve it yourself, but I will give you my experience . . . because being a blind person, it’s a full-time problem-solving job . . .’.
The value of trainers having lived experience of vision impairment was discussed frequently. As both users and trainers, trainers with vision impairment were able to keep up with the technology updates easier than sighted trainers and they were also able to share their lived experiences and act as role models. A5 stated, . . . so many times, they come with frustration, stress, depression . . . and then I showed them what I can do with the technology . . . I said, look, if I can do it, you can do it too . . . we will work together . . . so you can achieve your independence . . . I always encourage them like that . . .
Theme 4: informal support and other avenues for learning
This theme discusses learning support outside of formal training. Trainers reported on how they made use of informal support systems, such as family members, and other avenues for learning, to enhance the training.
There was no consensus on if involving family and support persons during the training session was helpful. Some trainers perceived sighted family members and support persons hampered the progress of clients as they were judgmental and discouraging towards clients. However, others felt that it depended on the attitudes displayed by the family member or support person. Some found having sighted family members around as beneficial, where they could help with instructing the clients during sessions, especially during the COVID pandemic. Post-training, they could revise with clients the skills learnt, as C2 shared, ‘if someone is there, that’s also looking at how you would do things . . . it can help like in between lessons’.
While trainers reported that friends or family members might be able to teach PVI, they felt their help was often limited, as generally sighted people do not know how to use the accessibility features optimally or know the range of features and apps available. Trainers reported that there are other avenues available to PVI to learn. These included hotlines and websites about accessibility features from Apple, Google, and Microsoft. Aside from hotlines, some trainers commented that Apple stores can help PVI who need to learn some basic skills to use the accessibility features. Besides these, the trainers reported that some clients access list-serves, podcasts, or videos on YouTube.
Theme 5: challenges associated with providing training
There were a few key challenges encountered by trainers in their work. These included responding to clients’ emotions, managing resistance towards learning, and dealing with the impact of the COVID pandemic on training.
Trainers discussed that they give their clients time and space to grieve or express their ‘frustrations’ and ‘stress’ with their vision loss. Trainers with vision impairment would also share their lived experiences, which they described helped some frustrated clients feel empathised and heard. By sharing their lived experiences, some trainers discussed that they ‘counsel’ some clients as they have expressed suicidal thoughts to them. Some trainers reported that they have had ‘demanding’ clients who were ‘rude’ and tried to ‘belittle’ the trainers as they felt that trainers did not understand their situation, but the trainers with vision impairment reported that this could be turned around and A5 pointed out that ‘protective’ clients would ‘start to open up’ when he shared his lived experience.
Many trainers mentioned that clients with some residual vision tended to resist learning voice control, such as Siri, or screen readers like VoiceOver. If trainers were perceived to push their clients to learn these methods, some clients would lose interest and stop attending training completely. Other health conditions were reported to impact training, such as finger joint deformities from arthritis, which could make learning finger gestures difficult, and hearing impairments could make communication during training more challenging. For some clients, the trainers reported that declining cognitive abilities and fear of or resistance to technology, could also slow down learning.
Other challenges shared included the difficulty in keeping up with technology advancements, especially for sighted trainers, as they do not use the smartphones’ accessibility features daily. Even C4, who is a user himself, found it ‘impossible to stay on top of everything’. Some trainers also mentioned that due to funding cuts, there were staff shortages which resulted in long waiting lists for their services.
Lockdowns due to the COVID pandemic in all three countries meant a stop to all face-to-face services. All the trainers, however, adapted quickly and offered training online or over the phone which posed additional challenges. Some trainers reported finding it difficult to adapt in the beginning, as they had to pivot to online teaching quickly, and some clients did not have the skills and tools needed to attend online sessions. Without the ability to show clients physically some finger gestures or to correct the wrong use of gestures (tapping and swiping and so on), training was made more difficult as shared by C1: ‘. . . Voice Over especially, err with the gestures, that’s really hard to teach, over the phone . . .’.
Theme 6: suggestions to improve training
This theme presents what trainers perceived would improve the training they provide. This included more training and mentoring for trainers, incorporating group training as well as smartphones to be loaned out for trial by clients.
Some trainers suggested having improved resources, especially for new trainers. This included ‘user-friendly’ training resources from phone suppliers that are constantly updated, access to mentors, as well as better training materials developed within their organisations, such as training videos on accessibility features. In addition, some trainers discussed a need for more information on how to structure the training, so that there is consistency in what is provided to clients, including the assessment and training approaches and knowledge that is imparted. In S7’s opinion, a ‘framework’ for training will help as currently without a framework, ‘now it’s like everybody is offering – a bit here and there . . .’.
Some trainers expressed that group training could be offered in addition to individual training to provide more support to a wider group of PVI. A3 said: ‘group training is wonderful because it facilitates relationships between clients, and it can empower the clients, knowing that it’s hard for everybody’. Others specifically stated that group training should be offered before individual sessions to upskill people in the basic features of smartphones before individual training catering to unique needs.
Online training was suggested to be an option that should remain, and some trainers wanted to see a ‘hybrid format’, to be able to cater to those who are geographically remote. Some trainers discussed the value of having clients who ‘know how to use the technologies’ to volunteer to train others. This would mean that organisations would have ‘more support staff or teachers’, as explained by A3. Some trainers like A4 would like to see a ‘pool of equipment’, in both iOS and Android platforms be available to them for use in training and trial by clients, so clients would be able to try different types of phones before committing to purchase one model or platform. A8 felt that some PVI who lost their sight later in life, who are ‘not in the [blind] community’ would ‘fall through the cracks not knowing where to access training’. Because of this, he felt that organisation’s training should be marketed more to ophthalmologists and optometrists to create more awareness of training and provide hope for the person who has just lost their sight, stating, ‘. . . don’t send your bloody clients, crying, you know out of your door, because they’ve lost their sight. Give them some hope’.
Discussion
This research explored the current perspectives of trainers in Australia, Canada, and Singapore on the provision of formal smartphone training to PVI. International literature has previously discussed the importance of formal training to improve proficiency among PVI in the use of smartphones (Locke et al., 2021; Sankhi & Sandnes, 2020; Senjam et al., 2021). By understanding the perspectives of trainers on what constitutes good training, the study sought to inform evidence-based training support for PVI.
Key findings that inform future training support for PVI include the importance of incorporating an individualised and graded approach, as well as gaining a good understanding of clients’ emotional readiness to learn; trainers with lived experience of vision impairment help to motivate clients and provide inspiration, and smartphone training not only imparts skills and knowledge but instils hope and supports independence and connection in clients.
One important strategy espoused by trainers in this study was to use an individualised approach for training. Previous studies have also recommended this approach, discussing how each client is unique, and that each person’s visual function, learning capacity, and learning needs should always be considered before and during training, to develop an individualised training programme (Robinson et al., 2017; Senjam, 2021; Wong & Tan, 2012). Other strategies shared in this study, that support the individualised approach, include recommending suitable accessibility features to be used depending on the person’s vision conditions. For example, as explained by Robinson et al. (2017), those with low vision would benefit from learning the zoom function and magnifier apps while those who are blind will need to learn how to use screen readers and other tailored features.
Participants conveyed the importance of individualised training to meet clients’ individual needs. This is supported by previous work discussing taking an individualised approach, including taking a graded approach. For example, by first learning to be comfortable with the touchscreen; then being orientated to the phone; using voice commands to make calls, and then learning more complex skills, such as finger gestures.
The findings suggest the trainers guided the learning experiences of PVI by pacing the training and providing challenges by grading the lesson. Pacing training is recommended to cater to the abilities of clients to enable clients to succeed and keep them motivated (Pendleton & Schultz-Krohn, 2018). Their style of teaching closely aligns with the Universal Design for Learning (UDL) design principle of ‘multiple means of engagement’ (Center for Applied Special Technology [CAST], 2023; Cumming & Rose, 2022), which assisted the PVI with different abilities and experiences to stay motivated as they engaged in learning activities. The findings also indicate that the trainers have applied the UDL guideline of ‘multiple means of representation’ to their practice by understanding first how their learners learn and then adjusting their method of teaching accordingly. The trainers were able to offer different modes of learning that cater to individual needs. Acknowledging variability in learners is critical in using the UDL framework as well (Hartmann, 2015). Trainers shared that some learners demonstrate what they have learnt in different ways by practising in between sessions, attend ‘drop-in’ clinics, filling up informal surveys post-learning or verbally informing trainers on their learning outcomes, thus showing that trainers have also offered ‘multiple means of expression’, which is another guideline under UDL (CAST, 2023).
One of the important findings of this study was the need for trainers to have a good understanding of their clients’ experience of vision loss. The study findings indicate that trainers should be mindful of their clients’ situation, for example, whether their vision is declining further, and whether this is worrying them or they are experiencing grief related to this, trainers can then use appropriate communication strategies, such as empathy, to engage with their clients. Depression and vision loss are highly correlated, and risk factors, such as age, poor self-rated health, visual acuity, and time since vision loss, are associated with depression (Nollett et al., 2019). Therefore, it is recommended that professionals supporting PVI not only be mindful of such risk factors, but it may also be useful to screen clients for depression before commencing training (Nollett et al., 2019).
Demmin and Silverstein (2020) have found that some PVI experience anxiety and social withdrawal, feel frustrated, and at times, have suicidal ideation. In line with these previous findings, trainers in this study reported that they often encountered clients presenting with these experiences and feelings. The findings suggest that trainers may need more training, to appropriately respond to their clients’ emotional needs, and provide support and education about vision loss. Further research is needed to support trainers in this regard. Peer support has been found to be beneficial in providing empathy and validation for PVI and can be garnered via sharing of positive narratives by another PVI or in the form of group-based intervention (Barrow et al., 2018; Stitt, 2016). Trainers with vision impairment discussed that sharing their lived experiences on how to overcome challenges was especially valuable to motivate their clients to attain their personal goals, reflective of the value of employing PVI as trainers. Trainers also discussed the benefits of peer support, with group-based training reported by trainers to be helpful in providing peer support and connectivity to motivate clients to progress further together, in learning smartphones or in other areas of their lives.
The results of this study indicated that training in smartphones can foster hope in clients for the future, as well as enhance their independence and connection. Training facilitates hope for the future was also discussed in Spafford et al.’s (2010) study, which stated that a timely referral to low-vision services (which can include learning to use AT) by doctors was important in fostering hope (Spafford et al., 2010). However, this is often not the case for smartphone training with delayed referrals, due to a lack of awareness of the usefulness of smartphones and apps for PVI among health care professionals (Senjam, 2021). As suggested by one of the participants, awareness among health care professionals regarding training may need to be raised, for example, by marketing the training to ophthalmologists and optometrists. This may enhance referral to organisations providing training and ongoing support provided to PVI.
Limitations
While we endeavoured to capture a comprehensive sample, there were limited trainers from Canada, and more participants from there would have meant a more balanced perspective on training from the three countries. It would also have been beneficial if the research team had observed some training sessions, to add another source of data to enrich the data analysis. This study heard the voices of trainers, and while this included PVI, for future research, PVI who received the training should be included to understand their experience of training. For example, co-design approaches in the design of future training will be important. In addition, this study was conducted in high-income countries, and given the emerging demand for training in some low and middle-income countries such as Nepal and Ghana, with high incidences of vision impairment (Abraham et al., 2021; Sankhi & Sandnes, 2020; Senjam et al., 2021), research in these countries on the training needs of PVI and contextually relevant training development is recommended. Future research exploring the wider influences on the access and use of smartphones and training, such as nations’ disability support policies, may also offer important insights into the barriers to smartphone use for PVI.
Conclusion
Good training not only provides the skills and knowledge for PVI to use smartphones and apps to be independent, but it also provides connectivity and hope for the future. The findings have provided critical information to inform current and future training programmes towards establishing best practices. These include the importance of responding appropriately to clients’ emotional needs, and trainers having lived experience, as trainers with vision impairment found sharing their lived experiences was beneficial to their clients’ learning and adjustment to vision loss. Gaining a good understanding of clients’ existing skills and knowledge, and catering to their unique learning needs in an individualised and graded approach, were critical to ensuring success in teaching and learning as well. Future research could explore the support needs of trainers in managing the emotional needs of clients, as well as partnering with consumers to develop future training and learning support.
Footnotes
Acknowledgements
The authors thank Miss Ai Sun, Siow, from the Singapore Institute of Technology, for her assistance in formatting the manuscript. This research was completed as part of the first author’s PhD candidature, with The University of Queensland, Australia.
Data availability
Data of this study can be obtained by emailing the first author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: H.L.T.’s PhD studies were funded by the Singapore Institute of Technology. This research was funded by Seed Grant (HSS 05-May 2020) from the Singapore Institute of Technology.