
Abstract
Charles Bonnet syndrome (CBS) is a condition associated with sight loss, characterised by vivid, spontaneous visual hallucinations. Currently, it is unclear whether CBS presents challenges to participation in physical activities, in addition to barriers attributed to sight loss alone. The purpose of this scoping review was to establish the extent of the literature, and gaps in the knowledge base, concerning the impact of CBS on older adults’ engagement in physical activities. Review conduct was informed by Arksey and O’Malley and Levac et al.’s scoping review methodologies. Six academic databases were searched during May 2021, yielding 2709 results: eight articles met eligibility criteria. Two additional sources were located via a reference check of included papers and stakeholder consultation. Quantitative cross-sectional studies (n = 3) indicate that CBS may interfere with the ability to move around, while qualitative sources (case report/series n = 6; autobiography n = 1) show that sudden presentation of hallucinations in a person’s pathway, or threatening content, may jeopardise safety while walking. Moving to avoid a hallucination could present a fall risk if attention is diverted from environmental hazards. One case report stated that CBS did not affect personal care activities. Due to a limited evidence base, further empirical research is needed to achieve a comprehensive understanding about how CBS affects older adults’ participation in physical activities.
Introduction
Nearly a fifth of the UK population is aged 65 years or over (Office for National Statistics, 2021). With increasing age, eye disease becomes more prevalent, and an estimated 20% of people aged 75 or older plus currently live with non-correctable sight loss (Royal National Institute for the Blind, 2019). Impaired vision can adversely impact older adults’ ability to move around safely (Ehrlich et al., 2019). In addition to age-related changes in gait and postural stability (Menz et al., 2003; Woollacott & Tang, 1997), reduced visual input compromises balance, particularly on compliant surfaces (Chen et al., 2012; Wood et al., 2009), and hinders visual detection and negotiation of environmental hazards (Patla, 1997). Negative consequences of sight-related constraints to mobility include falls - older adults with sight loss are 1.7 times more likely to fall compared with fully sighted peers (Legood et al., 2002) - and reduced engagement in physical activities (Ong et al., 2018; Smith et al., 2017).
People with impaired vision are known to restrict their activities (Smith et al., 2017), with fear of falling being a key influential factor (Wang et al., 2012). Potential outcomes of activity limitation include decline in physical, cognitive, and mental health (World Health Organization, 2018), and increased susceptibility to falling due to a decrease in lower limb muscle strength (Hopewell et al., 2019). A condition associated with visual impairment that may add a further layer of complexity to activity participation is Charles Bonnet syndrome (CBS).
CBS
CBS affects some people with sight loss, causing spontaneous external visual hallucinations (Ffytche et al., 1998) that the individual realises are unreal, although initially, contextually relevant percepts may be difficult to differentiate from reality (Menon, 2005). The nature of CBS varies from person to person: visual hallucinations are typically complex (people, distorted faces, animals, and whole scenes) (Hamedani & Pelak, 2019), static or dynamic (Schultz & Melzack, 1991), and can last for seconds or present continuously (Esteves Leandro et al., 2020). Duration from symptom onset varies, but a large-scale survey found that three quarters of respondents with CBS had experienced visual hallucinations for 5 years or longer (Cox & Ffytche, 2014). CBS is not associated with a particular eye pathology (Gilmour et al., 2009) although severity of vision loss increases susceptibility (Gordon, 2016). Potential triggers for exacerbation of CBS include living alone (Teunisse et al., 1995), feeling lonely (Teunisse et al., 1999), and stress (Vukicevic, 2010).
Recent inclusion of CBS in the 11th revision of the International Classification of Diseases (ICD-11) (World Health Organisation, 2019) has helped to standardise diagnostic criteria: partial or complete loss of sight; hallucinations are exclusively visual, complex, and usually temporary; and symptoms are not attributable to another aetiology. The leading explanatory theory for CBS is deafferentation: reduced sensory input leads to changes in neuronal activity within the visual areas of the brain, resulting in hyperexcitability and the release of visual hallucinations (Burke, 2002; Marschall et al., 2020).
CBS may affect 7.2%–60% of people with sight loss (Gordon, 2016; Menon, 2005; Niazi et al., 2019; Scott et al., 2001; Subhi et al., 2021) with low estimates primarily attributed to reluctance to disclose symptoms due to fear of stigma (Menon, 2005; Ord et al., 2018). Different screening approaches (Gordon, 2016) and variability in diagnostic criteria used in CBS research may also affect reported prevalence. Currently, there is no evidence-based treatment to manage CBS symptomology (O’Brien et al., 2020), and the success of self-help techniques is variable (O’Brien et al., 2020).
To help understand the potentially debilitating effects of CBS on function, this review aimed to (1) describe the extent of the literature concerning the impact of visual hallucinations on participation in physical activities and (2) identify gaps in the existing evidence base (Arksey & O’Malley, 2005; Munn et al., 2018). For the purpose of this scoping review, physical activity refers to ‘any bodily movement produced by skeletal muscles that results in energy expenditure’ (Caspersen et al., 1985), and level of intensity is categorised as light (cleaning, carrying rubbish, yoga), moderate (walking, shopping), or vigorous (dancing, swimming) (Department of Health and Social Care, 2019).
To the authors’ knowledge, a previous review focusing on this topic area has not been conducted (search conducted 27 May 2021, Medline [Ovid online] and CINAHL Plus [EBSCO]).
Materials and methods
A study protocol developed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews checklist (PRISMA-ScR) (Tricco et al., 2018) was prospectively registered on Figshare (27 May 2021, doi:10.48420/14686002).
Arksey and O’Malley’s (2005) and Levac et al.’s (2010) scoping review frameworks guided the conduct of this review: (1) identify the research question; (2) locate relevant studies; (3) select studies for analysis; (4) chart the data; (5) collate, summarise, and report the results; and (6) stakeholder consultation. Reporting criteria were informed by the PRISMA-ScR (Tricco et al., 2018).
Identify the research question
Primary question
What is known about the impact of CBS on older adults with sight loss’ engagement in physical activities?
Sub-questions
What effect do CBS-associated visual hallucinations have on susceptibility to falls?
What is the impact of CBS on fear of falling?
Which methodologies have been used to investigate/explore the effect of CBS on participation in physical activities?
Locate relevant studies
Eligibility criteria
The Population, Concept, and Context mnemonic was used to structure eligibility criteria for the review (Peters et al., 2020; Table 1). Theoretical papers (without data), protocols, conference abstracts, and personal opinions not written by someone living with CBS (editorials, commentaries, and letters to the editor) were excluded, as these sources were deemed unlikely to present primary data from people with CBS.
Eligibility criteria for papers included in the scoping review.
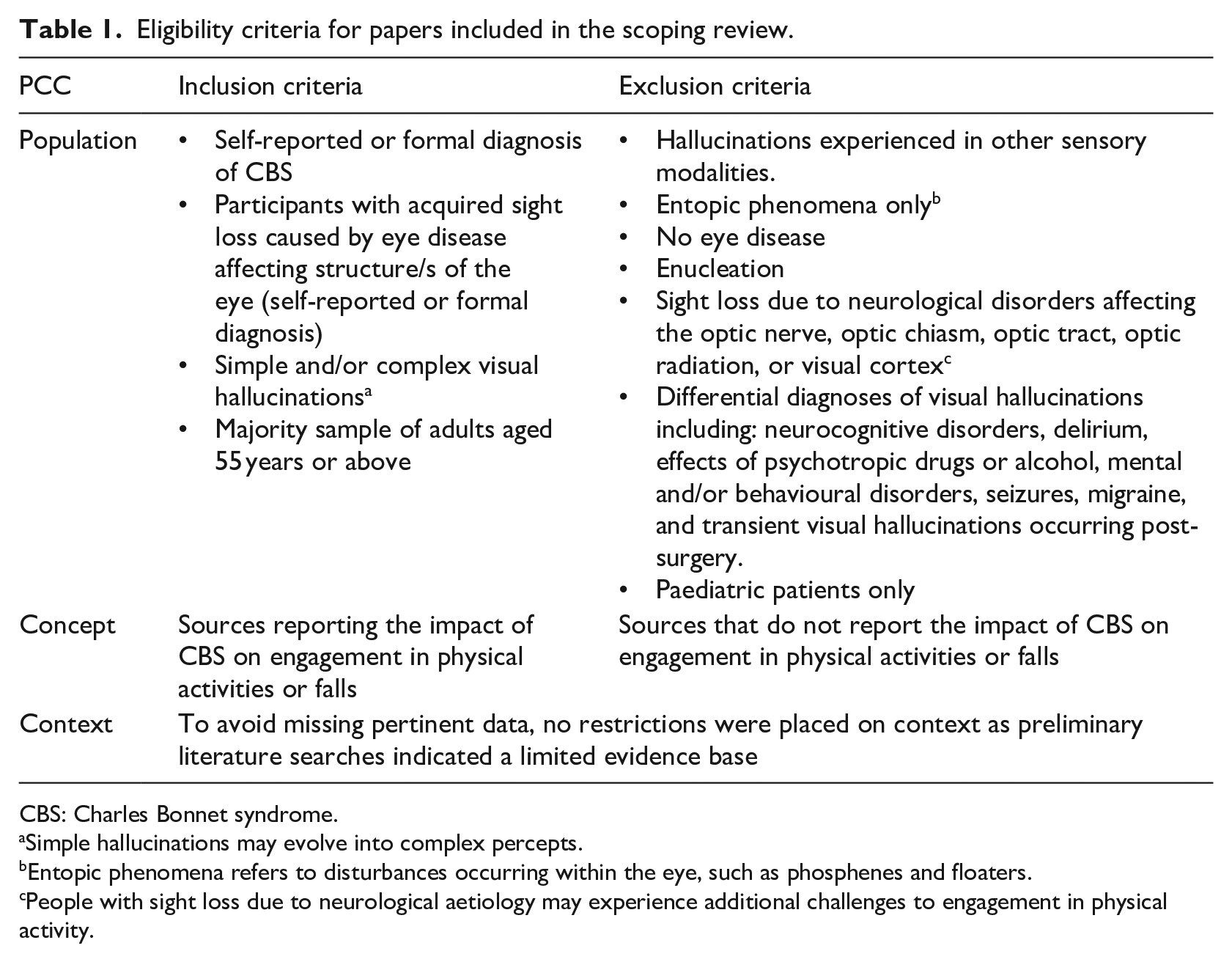
CBS: Charles Bonnet syndrome.
Simple hallucinations may evolve into complex percepts.
Entopic phenomena refers to disturbances occurring within the eye, such as phosphenes and floaters.
People with sight loss due to neurological aetiology may experience additional challenges to engagement in physical activity.
Search strategy
The following electronic bibliographic databases were searched during May 2021: Medline (Ovid online), CINAHL Plus (EBSCO), PsychINFO (Ovid online), and Embase (Ovid online). British Nursing Index (ProQuest) and Web of Science were also checked to locate papers that may have been omitted by the four key health databases.
Search terms included ‘charles bonnet*’ OR ‘visual hallucinations’ AND ‘sight loss’, plus database-specific subject headings and synonyms for free text terms. An initial search of Medline and CINAHL Plus revealed that inclusion of ‘physical activity’ or related concepts such as Activities of Daily Living (ADLs) in the search string returned a narrow set of results, risking relevant data being missed: these terms were therefore excluded. A specialist subject librarian provided advice regarding database selection and checked the final search strategy for each database prior to its application. An example search strategy can be found in Appendix 1.
To identify studies missed by electronic databases, bibliographies of included papers, plus key CBS literature reviews, were checked. A citation search of final papers was also undertaken (Arksey & O’Malley, 2005) using the Web of Science Citation Index, and key authors were contacted for further information. The Grey Matters Lite search checklist (Canadian Agency for Drugs and Technologies in Health, 2019) was used to locate relevant unpublished literature (search conducted 28 May 2021).
Due to limited resources, only papers in the English language were included. No restrictions were placed on time frame for publication, or context, due to the limited evidence base. One author (K.F.) conducted the literature search.
Select studies for analysis
All references located were uploaded to EndNote X9 reference management software. Following automatic removal of duplicates, any omissions were manually deleted (Rathbone et al., 2015). The final list of references was transferred to Rayyan (Ouzzani et al., 2016), a web-based tool to facilitate the literature review screening process by a research team. Source selection was completed in two stages:
One researcher (K.F.) excluded papers that were obviously irrelevant based on title alone, and two reviewers (K.F. and E.S.) screened the abstracts of remaining papers against eligibility criteria (Levac et al., 2010). Any discrepancies relating to eligibility criteria, or papers shortlisted for full-text review, were discussed and referred to a third reviewer (C.S.) for resolution. Studies were selected for full-text review if (i) the source appeared relevant, (ii) eligibility was unclear from the abstract, or (iii) case study or case series was mentioned in the abstract.
Two researchers (K.F. and E.S.) reviewed full-text papers, and any disagreements were discussed and referred to a third party (C.S.) to achieve consensus.
The study selection process, including reasons why full-text papers were excluded, was recorded on a PRISMA flow diagram (Tricco et al., 2018).
Chart the data
A bespoke data extraction form was developed that initially included: (1) author, (2) year of publication, (3) study design, (4) area of functional impact, and (5) summary of key findings. One reviewer (K.F.) tested the form by extracting data from two articles, and potential amendments were discussed with the research team. Agreed revisions entailed removal of ‘Functional impact’ – this information was already incorporated within reported findings – and addition of location and participant demographics to contextualise included sources. Due to potential variability in diagnostic criteria adopted in CBS research, these data were noted separately to help identify limitations in the findings. Using the finalised chart, one researcher (K.F.) transferred data from all included studies, which was then checked and verified by a second reviewer (E.S.).
Collate, summarise, and report the results
As pertinent literature was anticipated to be limited, a descriptive overview of quantitative results was undertaken, and qualitative data were analysed using conventional qualitative content analysis (Hsieh & Shannon, 2005): basic coding enabled identification of similarities and differences in content, and broad categories were formed to facilitate a summary of findings.
Stakeholder involvement
Stakeholder consultation comprised two stages: (1) pre-review to ensure questions are meaningful and relevant to people living with CBS and to help identify additional evidence sources (Arksey & O’Malley, 2005) and (2) following review completion to help validate and enrich findings (Levac et al., 2010). Esme’s Umbrella – a charity promoting awareness of CBS – and a society for people with sight loss, supported stakeholder recruitment. Discussions with stakeholders were scheduled to take place face-to-face, or via telephone.
Results
In total, ten articles were located: three cross-sectional studies, five case reports, one case series, and an autobiography written by a person who has experienced CBS. The scoping review flowchart is shown in Figure 1. Most studies were conducted in the United States (n = 4) followed by the United Kingdom (n = 3). Patients with a range of eye conditions were represented, with macular disease being the most common (n = 5). Both light and moderate intensity physical activities were reported: ADLs and Instrumental Activities of daily living (IADLs) (n = 1); walking (n = 6) or both (n = 3).
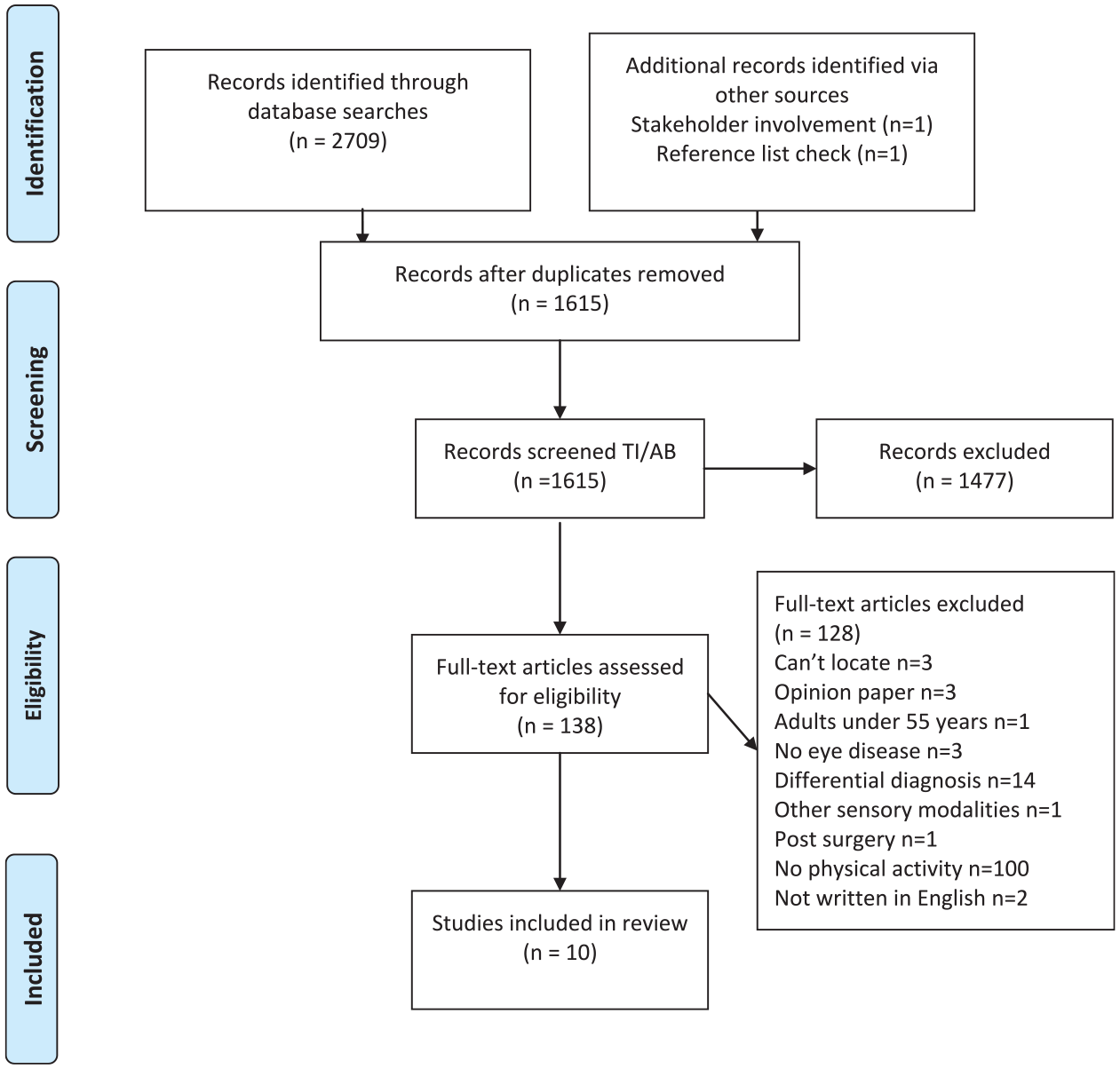
Scoping review flowchart.
Input from stakeholders
Three stakeholders provided input prior to commencing the literature search: one person living with CBS, a member of staff at a sight loss charity (both conducted face to face) and a volunteer working with people with CBS (via telephone). First and secondhand accounts of CBS and its negative impact on independence while walking confirmed the relevance of the topic, and during discussions, the staff member identified an additional source that met review eligibility criteria. Review findings were discussed in person with the author of the included autobiography who verified that they were plausible in relation to his own experience of CBS.
Quantitative sources
Quantitative findings are presented in Table 2. Three cross-sectional studies investigated the effect of CBS on daily activities, including moving around. Cox and Ffytche (2014) identified factors associated with negative outcome CBS (visual hallucinations that have a fairly, or very, negative effect on a person’s life). A random sample of 4000 Macular Disease Society members received a structured postal questionnaire: 1294 surveys were returned, and 492 people indicated that they had CBS. Forty-six percent of individuals living with CBS felt hallucinations interfered with their daily activities, including ‘moving about’. A third of people surveyed reported negative outcome CBS (n = 156), and the authors found a significant association between this status, and CBS affecting one or more daily activities (x2 = 75.3, p ⩽ 0.000001).
Quantitative sources.
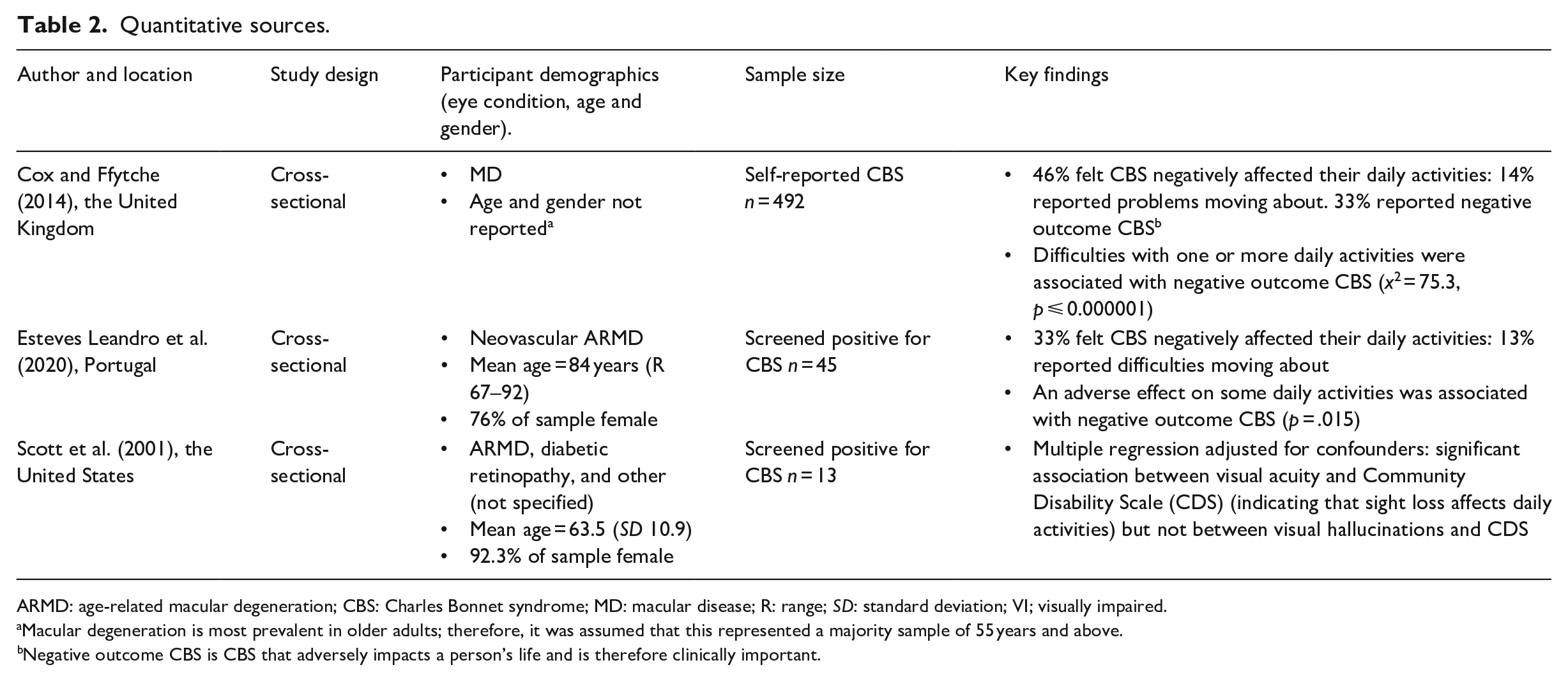
ARMD: age-related macular degeneration; CBS: Charles Bonnet syndrome; MD: macular disease; R: range; SD: standard deviation; VI; visually impaired.
Macular degeneration is most prevalent in older adults; therefore, it was assumed that this represented a majority sample of 55 years and above.
Negative outcome CBS is CBS that adversely impacts a person’s life and is therefore clinically important.
Esteves Leandro et al. (2020) also looked at the clinical impact of CBS, focusing on patients with neovascular age-related macular degeneration. Out of 500 eligible patients attending an eye clinic, 45 screened positive for CBS and completed a structured, face-to-face questionnaire based on Cox and Ffytche’s (2014) survey items. Thirty-three percent reported that visual hallucinations interfered with daily activities, and 13% indicated difficulties ‘moving about’. This study also found that 33% of CBS patients had negative outcome CBS. A statistically significant association was reported between some effect on daily activities and negative outcome CBS (p = 0.015).
Scott et al. (2001) used the Community Disability Scale (CDS), which incorporates a mobility subscale, to investigate the association between CBS and functional status in patients with retinal disease (n = 86). Visual hallucinations were associated with a higher CDS score (higher scores indicate worse functional status), but adjusted multiple regression showed that CBS was not a significant independent predictor of variation in CDS score (p = 0.42).
Qualitative sources
Qualitative findings are presented in Table 3. Seven references provided either verbatim quotes from people living with CBS (Needham & Taylor, 1992; Skipworth, 2021) or described an individual’s account about the effect of visual hallucinations on one’s ability to move around (Issa & Yussuf, 2013; Lomo et al., 2021; Needham & Taylor, 2000; Paulig & Mentrup, 2001; Richardson, 2007).
Qualitative sources.
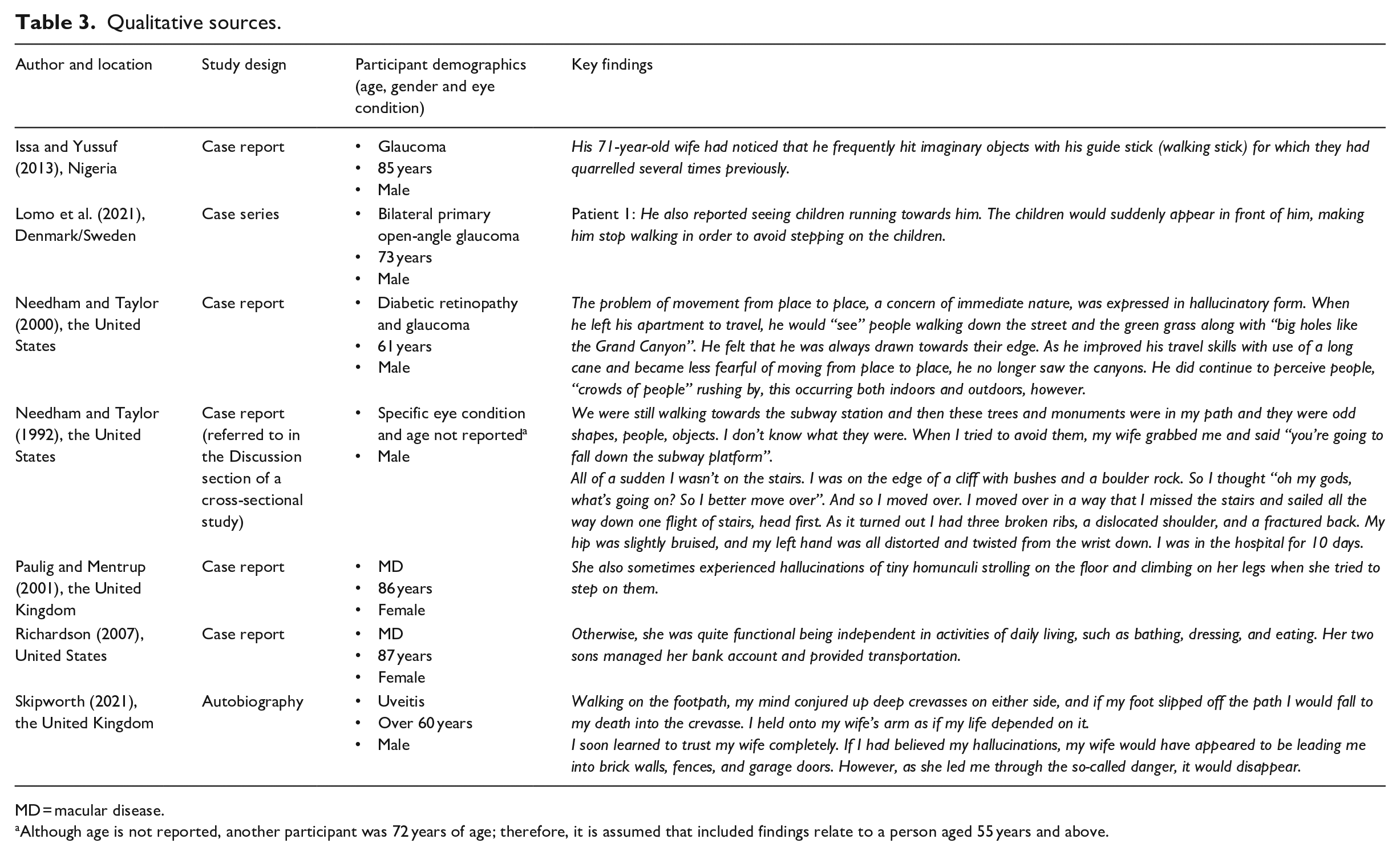
MD = macular disease.
Although age is not reported, another participant was 72 years of age; therefore, it is assumed that included findings relate to a person aged 55 years and above.
Hallucinations presenting an obstruction
Four sources detail how hallucinations may hinder the ability to walk efficiently and independently. One person stopped walking to avoid treading on children who spontaneously appeared in his pathway, while another described small human figures climbing onto her legs after she attempted to step on them. A mobility aid was used by one man to strike the hallucinations. For one person, a sighted guide was necessary to confirm that it was safe to continue walking through static hallucinations of brick walls, fences, and garage doors: while moving past, the hallucinations disappeared.
Hallucinations, falls, and fear of falling
One case report describes how a sighted guide physically intervened to stop a man from falling off a subway platform after he stepped aside to avoid trees, monuments, and other objects in front of him. The same person fell down an internal stairway when he moved away from an apparent cliff edge, resulting in hospitalisation.
In a different source, fear of falling was reported by a man who sought support and reassurance from his wife while experiencing hallucinations of deep crevasses alongside a footpath. Another report described how a man who was fearful walking outside perceived holes resembling the Grand Canyon: these particular hallucinations ceased after his confidence increased following long cane training.
Daily activities
One source stated that visual hallucinations did not interfere with a patient’s self-care activities, but assistance was needed with transportation.
Discussion
This review located ten eligible sources that included the effect of visual hallucinations on physical activity. The majority of identified studies indicate that CBS may potentially hinder the ability to move around safely and independently and could increase susceptibility to falls and fear of falling.
Quantitative data specific to CBS and its effect on physical activity is sparse. Two cross-sectional studies included one survey question about the perceived effect of CBS on everyday abilities, and from six fixed responses, ‘moving about’ was the second most frequently selected. Both surveys found a similar proportion of people with CBS who felt visual hallucinations interfered with their mobility (13% and 14%). These results show that CBS could present unique challenges while walking, in addition to those posed by sight loss alone.
As ‘moving about’ was not analysed as a discrete entity, it is not possible to identify an association between CBS and mobility difficulties via existing studies. Cox and Ffytche (2014) and Esteves Leandro et al. (2020) grouped mobility and other comparatively sedentary activities such as watching TV, under the over-arching category ‘abilities’: a significant association between one or more daily abilities affected by CBS and negative outcome CBS was found. Scott et al. (2001) used the composite CDS score incorporating ADLs, IADLs, and mobility subscales to measure functional status. Interestingly, following multiple regression analysis, visual impairment – not CBS – was found to be a significant predictor of CDS score. This result may be attributable to the small sample size, plus it is unclear whether the CDS is sufficiently sensitive to detect a difference between visually impaired people with, and without, hallucinations. Findings indicate that further quantitative studies which control for confounders are needed to fully investigate the relationship between CBS and mobility.
There is a paucity of qualitative data concerning how CBS affects physical activity. Currently, descriptive evidence is predominantly restricted to brief references in medical case reports. One book source (Skipworth, 2021) did offer a more extensive account about how CBS affects walking outdoors. Overall, included literature indicates that spontaneous or threatening visual hallucinations may affect safety while moving about.
Sudden visual hallucinations could trigger a response comparable to encountering an unanticipated, tangible hazard: step aside to avoid an obstruction, or stop walking. Threatening content may also trigger the fight or flight response, causing someone to stop in fear, or move away before assessing actual fall risks in the environment. When confronted with an unexpected external object, maintaining stability is vital to prevent a fall (Berg et al., 1989; Patla, 1997), but this may be affected by age-related changes in reactive balance control mechanisms (Gerards et al., 2021; Woollacott & Tang, 1997) and reduced visual input (Osoba et al., 2019). Strategies to manage automatic response to hallucinations may be problematic, as this process does not appear to be overridden by insight, even when hallucinations are not contextually relevant, such as a cliff edge in a house.
Included sources suggest that changes in emotion triggered by external events may alter hallucination characteristics. One case report described how a man who felt anxious during orientation and mobility training found that disturbing hallucinations ceased after his confidence increased. Changes in CBS content linked to a stressful situation have also been reported in the literature: a woman living with CBS experienced terrifying hallucinations following bush fires in Australia (Vukicevic, 2010). This apparent interaction between intrinsic and extrinsic factors may explain why CBS experiences differ (Carpenter et al., 2019; Scott et al., 2001) and symptoms fluctuate. Interestingly, a survey conducted during the COVID-19 lockdown in the United Kingdom found that older adults with CBS self-associated imposed restrictions in movement with symptom exacerbation (Jones et al., 2021). This finding indicates a potentially complex and dynamic relationship between physical activity and CBS symptomology.
One case report found that CBS did not interfere with daily function, reflecting findings in other studies – not everyone experiences difficulties linked to visual hallucinations (Cox & Ffytche, 2014; Esteves Leandro et al., 2020). As the purpose of medical case reports is to detail the diagnostic process, in-depth exploration about how CBS effects everyday function is not a priority, or may not be reported.
To enhance understanding about how CBS affects physical activity, high-quality empirical research is needed. In particular, studies adopting qualitative methodology would help clarify if, and how, CBS affects motivation and willingness to take part in physical activity, and whether a CBS component should be included in mobility, vision or falls assessment tools. Findings could also inform development of a comprehensive CBS assessment or outcome measure to help quantitatively evaluate the relationship between CBS and mobility. Although a CBS screening tool has been developed (Cantin et al., 2019), it does not incorporate the functional impact of visual hallucinations. Due to wide variation in CBS prevalence, a high-quality epidemiological study to determine the scope of this clinically important condition would be advantageous.
Implications for sight loss professionals
The strength of recommendations for policy and practice is limited by the extent and quality of evidence concerning CBS and its impact on undertaking physical activities. Based on this review’s findings, sight loss professionals supporting older adults living with impaired vision and CBS need to be cognisant that spontaneous or threatening hallucinations may compromise safety while moving about. If hallucinations are particularly intrusive, or include threatening content, sighted assistance may be necessary to provide reassurance and/or minimise fall risk.
Awareness of CBS among health care professionals is low (Gordon & Felfeli, 2018), and therefore, how a client responds to visual hallucinations may be misinterpreted. For instance, hallucinations causing a person to pause or deviate from straight line walking may incorrectly be attributed to cognitive or physical causes, while reluctance to engage in activities may be interpreted as low motivation. If CBS is suspected, or a person is known to have experienced a sudden deterioration in vision, sensitive questioning and reassurance may encourage divulgence of symptoms (Menon, 2005). As medical assessment is advised to eliminate differential causes of visual hallucinations, a CBS leaflet aimed at family physicians can be downloaded from the Esme’s Umbrella website (charlesbonnetsyndrome.uk) to help prevent misdiagnosis.
Identification of factors that may trigger or exacerbate CBS could help inform condition management strategies (O’Brien et al., 2020). Independent travel can be anxiety provoking for people with sight loss, and professionals need to be aware that emotional status could negatively alter hallucination content. If someone is fearful about walking outdoors, prior use of relaxation techniques, such as meditation, may help minimise intrusive visual hallucinations that could preclude engagement in physical activity.
Strengths and limitations
A key strength of this paper is the use of a transparent and replicable methodological review process to identify gaps in the CBS knowledge base, but some limitations should be noted. Data from participants with differential diagnoses may be included due to variability in diagnostic and eligibility criteria adopted in CBS research. Also, it was not feasible in one study conducted via postal questionnaire, to carry out comprehensive CBS screening: this source was included as it represents the largest phenomenological study to date and is likely to include a significant proportion of people fulfilling CBS diagnostic criteria. Two papers did not report the participant’s age, risking inclusion of findings nonspecific to older people. In both instances, eligibility was assumed: one article focused on macular degeneration, the most prevalent age-related eye condition, while reported demographics in the second relating to other study participants, concurred with review inclusion criteria. Overall, due to described shortcomings, the scoping review findings should be interpreted with caution.
As recommended in the PRISMA-ScR guidelines (Tricco et al., 2018), the following protocol deviations are reported: the sub-question concerning the effect of physical activity on CBS symptoms was omitted as it did not relate to ability to engage in physical activity per se, and sources reporting ADLS and IADLS were included as they may represent light to moderate intensity physical activity, helping to maximise findings.
Conclusion
Evidence concerning how CBS affects physical activity is limited, but both stakeholder feedback and sources included in this review indicate it is a valid and important area of inquiry. Further research is therefore needed to achieve a more comprehensive understanding about how CBS affects ability to undertake physical activities. Without this knowledge, tailoring health and social care interventions to meet the needs of people living with CBS is problematic, hindering a person-centred approach. Until a more robust evidence base is established, CBS may continue to remain ‘invisible’ to many allied health professionals, but for someone living with visual hallucinations, the impact on everyday function is real and potentially debilitating.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196221112800 – Supplemental material for Impact of Charles Bonnet Syndrome on visually impaired older adults’ ability to engage in physical activity: A scoping review
Supplemental material, sj-docx-1-jvi-10.1177_02646196221112800 for Impact of Charles Bonnet Syndrome on visually impaired older adults’ ability to engage in physical activity: A scoping review by Katharine Fisher, Caroline Sanders and Emma Stanmore in The British Journal of Visual Impairment
Footnotes
Acknowledgements
The authors thank Judith Potts, founder of Esme’s Umbrella; Mike Bailey, Development Manager at Christopher Grange, Liverpool; members of Esme’s Friends CBS support group; Joy Waters at Sheffield Royal Society for the Blind, and Bill Skipworth, author of Now I See, for their invaluable input.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the Thomas Pocklington Trust (grant no. RES-212).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.