
Abstract
Aim:
The present study aims to evaluate oral health knowledge and habits of children with visual impairment by comparison with their sighted counterparts and also evaluates parental knowledge and involvement in children’s oral hygiene routines.
Methods:
This observational and transversal study included the participation of 68 children (34 were visually impaired and 34 were sighted), from seven schools from Lisbon. The participants with visual impairment were age and gender-matched with their sighted counterparts to minimize variations in the analysis. In all, 52.9% of children were male, with average age of 11.15 (±3.413) years [6; 18]. The children and parents completed one survey each. Children were submitted to an oral examination to evaluate oral health.
Results:
Participants with visual impairment showed a non-significant increase in the decayed, missing, and filled teeth index (dmft), gingival, and oral hygiene indexes. Both groups’ gingival state was mostly classified as excellent, and oral hygiene was mainly classified as excellent/good. More children with visual impairment (85.7%) needed help with teeth brushing (p = .046) and were more likely to miss dentist check-ups more often (p = .025). Also, sighted children and their parents demonstrated more knowledge about oral health.
Conclusion:
Children with visual impairment and their parents showed less favorable results, justifying the need to promote oral health education to this demographic.
Introduction
A lot of children with special needs, especially with visual impairment, face many challenges during their daily tasks and, consequently, in their oral hygiene habits (Shahabudin et al., 2016).
According to the International Classification of Diseases 11 (2018), visual impairment can be classified into four main categories: mild, moderate, severe visual impairment, and blindness (World Health Organization [WHO], 2019).
Accordingly to the WHO (WHO, 2019), the number of children with visual impairment globally is approximately 1.4 million (4–5% of the overall population), with three-quarters living in impoverished regions in Africa and Asia. In Portugal, the number of cases has not been yet fully established, but according to the 2001 CENSOS, the incidence rate of visual impairment cases reached its highest value in practically every region in Portugal for the age groups of 0 to 15 and 16 to 24 years (Instituto Nacional de Estatística [INE], 2002).
In previous studies, children with visual impairment have shown difficulties in aptitude and perceiving the need for brushing, which leads to the presence of oral cavities (Dom et al., 2010; Nobre, 2015). It is extremely important that people with visual impairment understand the state of their oral health so that they can adopt hygiene and other habits that contribute to maintain and improve oral health (Filho et al., 2010).
Parents or tutors play a significant role in reducing the cavity risk by conveying the importance of maintaining oral health and supervising the child’s daily brushing habits. However, this follow-up does not always take place as parents assume too early that the child is able to care for their oral health independently (Albino & Tiwari, 2016; A. Fernandes et al., 2012).
Children with visual impairment often show greater difficulty in brushing their teeth. For that reason, the adult supervising the child’s dental check-ups plays a pivotal role in instructing and aiding the child at home with the recommended oral hygiene procedures (Lima, 2011).
Another problem associated in children with visual impairment developing oral cavity is dental trauma. Studies revealed that in children with partial sight and blindness, dental trauma in the maxilla and central incisors occurs with higher frequency. This is frequently a consequence of protrusion of incisors and inadequacy in labial border covering that reduces the effects of dampening (Agrawal et al., 2013).
The aim of the present study consists of comparing children having visual impairment with their sighted counterparts concerning their oral health, habits, and oral hygiene knowledge and parents’ knowledge and involvement in their children’s oral hygiene routine.
Materials and method
Study design
The following observational and transversal study covered a sample of 68 children, half of which were sighted participants and the other half of the children had visual impairment (blindness or partial sight). The parents of all children also participated in this study, with one tutor for each child.
The data collection was performed between October 2019 and March 2020.
Participants
This study includes 68 children, covered both genders (52.9% of individuals were male), without ethnic and social distinction, to allow as many participants as possible, seeing that the sighted group was matched with the visually impaired group. All children were school-aged (6 to 18 years old): 38 children attended elementary school, 20 middle schools, and the other 10 high school.
The criteria included a sighted group that did not suffer from any type of visual impairment and a partially sighted group in which children possessed at least one type of visual impairment (like blindness and low/poor vision). In the study, children were compared taking into account these criteria, with a group of children with visual impairment and a group of sighted children.
The parents also participated in this study (one for each child) by completing a survey, and the degree of relatedness verified in the majority was the mother (85.3%).
The parents of all children that participated in this study provided signed consent. The objectives of this study were explained in the consent forms and the authorization requests to the schools. The parents were also informed about the possibility of a request to drop their child’s participation in this study at any moment. Consent forms were sent to the parents of all students with visual impairment and some sighted students to match them up with counterparts of the same age, gender, and school class.
Ethical considerations
This study was approved by the Ethics Commission of the Faculty of Dental Medicine of the University of Lisbon and followed the Declaration of Helsinki’s international rules for people with special needs.
For this study, authorizations from seven schools from Lisbon inserted into the network of schools of reference for the education of students with visual impairment and low vision of the Governmental Department of Education of Portugal were obtained. Seeing as the choice of schools was due to convenience, the sample is not probabilistic.
Oral examination
An oral observation of the participants’ oral cavities was conducted in a classroom, with the participant sitting near a window to use natural light. Before the oral observation, the instruments subsequently used were shown to all participants and particularly felt by the children with visual impairment, in order to keep them calm and informed about the procedure that would follow. The oral observation consisted of a check-up where three indexes were evaluated: decayed, missing, and filled teeth index (DMFT/dmft) (WHO, 2013) for both dentitions, deciduous and permanent, including mixed, gingival index (GI) (Löe, 1967), and the simplified oral hygiene index (OHI-S) (Greene & Vermillion, 1964), to evaluate the participants’ oral health. At the end of each oral observation, the children completed a survey, and they were also educated about oral hygiene, with adaptations for children with visual impairment. It should be noted that the participation of children in the study through oral examination and survey completion was always done under the supervision of a teacher or a school staff member that the child was familiar with, who helped in the communication and relaxation of the children.
Survey questionnaire
Parents’ and children’s surveys were adapted from preexisting ones and included new questions by the authors of the present study (AlSadhan et al., 2017; Bizarra, 2016; M. Fernandes, 2017; Liu et al., 2019; Pan et al., 2017; Rodrigues, 2008). Both questionnaires mostly presented multiple-choice questions. The survey directed to the parents was filled in at home, while the children’s survey was completed by the observer through an interview conducted after the oral observation. Both surveys’ themes covered social demographic characterization, visual impairment medical history, oral hygiene habits, dependency, and oral health maintenance.
Data analysis
Data were analyzed using the SPSS® version 26.0, with a significance level of 5%.
Descriptive statistics were made of all variables to calculate the absolute and relative frequencies, and then an inferential analysis was conducted to associate oral health variables with the others. After checking the non-normality of variables with the Kolmogorov–Smirnov test, it was decided to use nonparametric tests. The chi-square independence test was used to analyze and compare the two groups about nominal variables, such as autonomy, type of help, and brush checking, and also those that were related to knowledge about oral health. In contrast, the Mann–Whitney U test was used to examine possible differences between the ordinal scale variables, such as parental education level, bushing frequency, and regularity of dental appointments, and also all those who evaluate oral health indexes.
Results
Analysis of social demographic data of children and parents
The sample had 68 participants, half of them had visual impairment, of which 13.2% were blind and 36.8% were partially sighted. From the sample, 52.9% of individuals were male, and the average age was 11.15 (±3.413) years (6; 18), being that between the groups, there were no significant statistical differences in gender and age.
The main causes of visual impairment were diseases (58.8%), such as congenital glaucoma (32%) and Leber Congenital Amaurosis (12%). Most of them were reported as congenital or happened until 1 year of age (85.3%).
The parents of children involved in this study had a wide range of level of education, but parents of children with visual impairment had in average lower qualifications. More parents of children with visual impairment had levels of education lower or equal to high school, and 73.3% of parents with a university education were of sighted children, showing significant differences (p = .013).
Analysis of oral hygiene habits of children
The analysis of the children’s survey showed that 10.3% of overall children (from which 85.7% had visual impairment) needed help with brushing (p = .046). The parents reported that 14.7% of all children (from which 70% had visual impairment) needed help. The referred sighted participants were between 6 and 8 years old and the visually impaired between 6 and 15 years old.
After brushing, 23.5% of participants (68.8% had visual impairment) reported that their parents check if their teeth are well brushed. However, 38.2% of parents (57.7% of them were parents of children with visual impairment) reported checking their children’s brushing efficiency (p = .034).
In all, 48.5% of participants used fluoride mouthwash, with participants with visual impairment (54.5%) reporting a slight preference for it. On the other hand, 23.5% (68.8% were sighted) reported using dental floss. Furthermore, most parents of participants with visual impairment expressed that their children used less of these products (p = .069).
As for the regularity of dental appointments, 42.6% of individuals were not regulars, and most of them had visual impairment (20; 69%), presenting a significant difference (p = .025) (Table 1).
Oral hygiene habits of children.
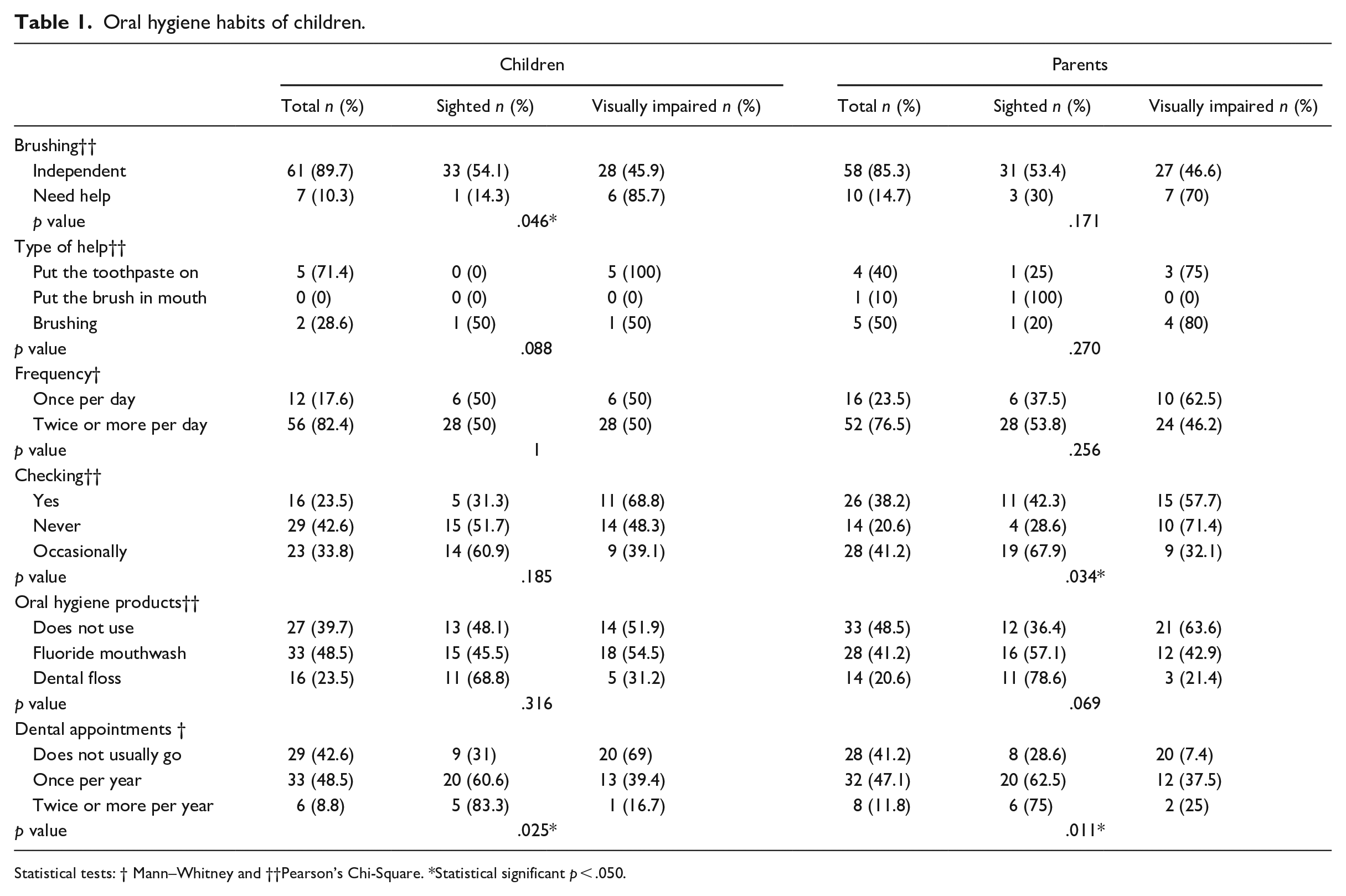
Statistical tests: † Mann–Whitney and ††Pearson’s Chi-Square. *Statistical significant p < .050.
Analysis of oral health knowledge of children and parents
In all, 82.8% of participants reported already having received oral health information from their parents and other relatives, whereas only 57.7% of parents reported it themselves.
Concerning the children’s knowledge about oral health, 47.1% (59.4% were sighted) considered it important that the toothpaste contains fluoride. Of these 47.1%, 84.4% of individuals (59.3% were sighted) said that it mainly aims to prevent dental caries (p = .975). The parents also considered this prevention as its main measure (82.6%), being that 47.4% of them have children with visual impairment (p = .611).
In all, 98.5% of participants (49.3% had visual impairment) stated that brushing prevents dental caries. Having a healthy diet (n = 65) and regular dental appointments (n = 64) was also considered by most participants as being essential prevention measures. In general, parents showed a greater lack of knowledge than their children given that sighted children’s parents selected more measures correctly (Table 2).
Knowledge of children and parents related to measures that prevent tooth decay.
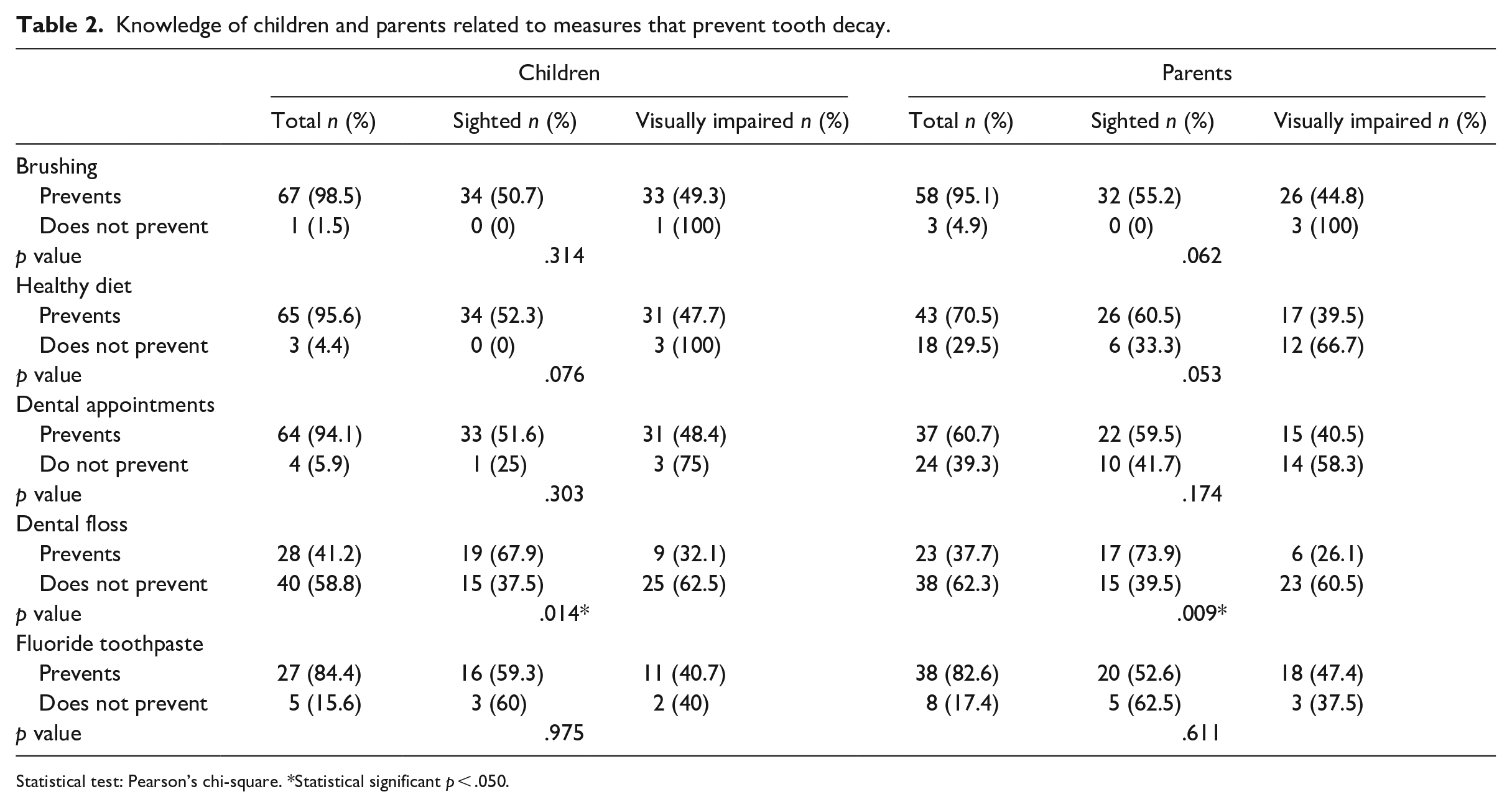
Statistical test: Pearson’s chi-square. *Statistical significant p < .050.
Analysis of oral health of children allowed by oral observation
Even with a greater number of teeth present in sighted participants (52.1%), it was verified that the deciduous dentition registered a mean (1.50 ± 2.86) of decayed teeth in children with visual impairment higher than sighted children’s (p = .183). The number of caries-free children was lesser for participants with visual impairment (12; 46.2%) (p = .245). In permanent dentition, children with visual impairment also presented a higher average of decayed teeth (0.21 ± 0.48). Of the 59 (86.8%) children free of caries, more sighted children (31; 52.5%) are in this situation. The dmft index for deciduous dentition was higher in children with visual impairment (1.60 ± 2.93), while for permanent dentition was higher in sighted participants (0.35 ± 0.77) (p = .917) (Table 3).
Decayed, Missing, and Filled teeth index for both dentitions (DMFT and dmft) of children.
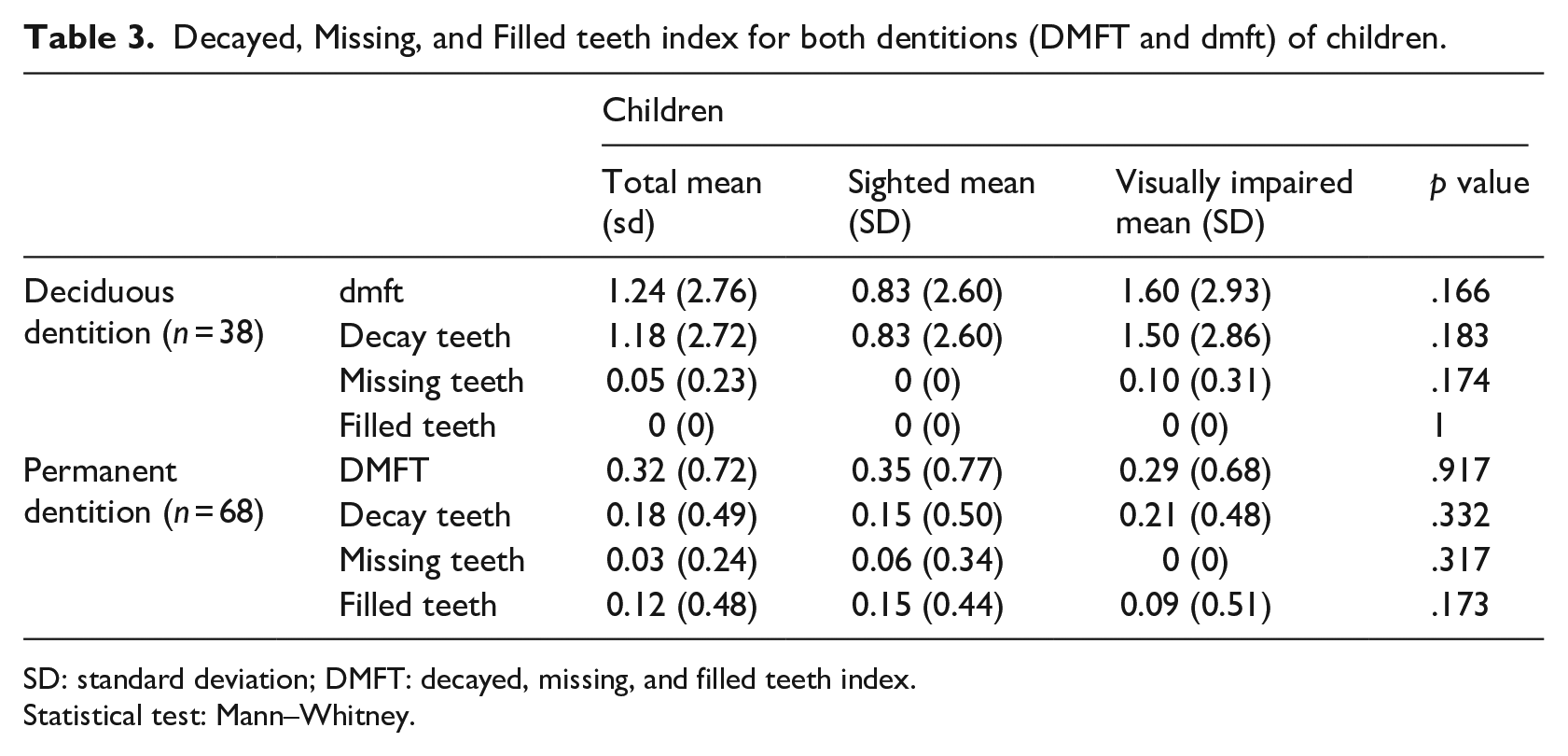
SD: standard deviation; DMFT: decayed, missing, and filled teeth index.
Statistical test: Mann–Whitney.
In the gingival index, children with visual impairment obtained a GI score of 0.18 (±0.25) (p = .251), and classification of the same index showed that 61.8% of participants (52.4% were sighted) were in an excellent level (p = .620). In all indexes to evaluate the oral hygiene (debris and calculus indexes, and posteriorly OHI-S), it was verified a greater average in children with visual impairment, however, without significant differences. In the OHI-S, most children (n = 65) scored excellent and good, with similar results for both groups (p = .558) (Table 4).
Gingival Index (GI), Debris Index (DI), Calculus Index (CI), and Simplified Oral Hygiene Index (OHI-S = DI + CI) of children.
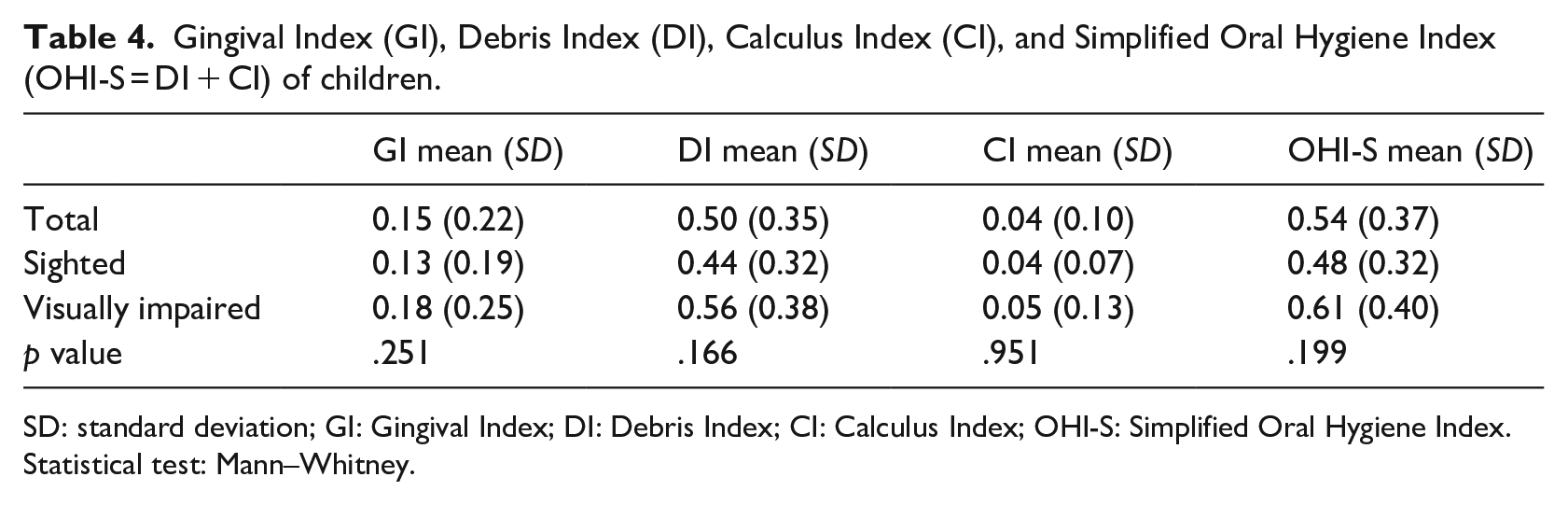
SD: standard deviation; GI: Gingival Index; DI: Debris Index; CI: Calculus Index; OHI-S: Simplified Oral Hygiene Index. Statistical test: Mann–Whitney.
The parents were questioned about their children’s history of dental trauma, having an incidence of 25% with 58.8% of sighted children.
Discussion
Few studies approach the theme of oral health in individuals with visual impairment, and the ones that do compare them with sighted people are even fewer. However, blindness can impact oral health due to physical barriers, social, and information related to this impairment, demonstrating the need for more studies (Ozdemir-Ozenen et al., 2012).
Most children (n = 56) reported brushing 2 or more times a day, and both groups presented the same value (50%), while in previous studies where a lesser percentage of children with visual impairment were in this frequency, justified by the lack of education on the oral health of children with visual impairment (Chang & Shih, 2004). This same frequency of brushing was still higher than the estimated value for the Lisbon region (69.3%) for the age gap of 12 (the average age in the present study was 11.15 years) (Calado et al., 2015).
On the other hand, the reduced number of children who use dental floss was similar to the previously mentioned study, which can relate to the lack of knowledge of this interproximal hygiene method. Seeing as in this study, a large majority of children and parents considered that the utilization of dental floss does not avoid tooth decay (Chang & Shih, 2004). The present study presented higher values than the estimated values for the region of Lisbon in terms of dental floss use, although the frequency of this utilization was not checked in the present study (Calado et al., 2015).
According to studies, oral hygiene can be substantially improved using practical teachings of brushing by oral health professionals during appointments (Kumar et al., 2020). However, this study corroborated others because it showed that most children with visual impairment (69%) did not usually go to dental appointments, contrary to sighted children, lacking vigilance and detection regarding oral diseases (Chang & Shih, 2004). According to AlSadhan et al. (2017), the lack of this regularity can be justified by the parents of children with visual impairment being more focused in appointments related to their disability, making dental appointments secondary. However, more factors may be associated with the lack of regular dental appointments, such as these families’ socioeconomic level. Also, the parents do not recognize that prevention is better than letting the situation evolve to a disease stage, which requires more complex treatments.
Oral health knowledge of sighted children was greater than children with visual impairment, revealing the necessity of education about oral health primarily for the last group. Few studies compared the knowledge of oral health of these individuals, focusing more on the state of oral health. Nevertheless, knowledge is fundamental, as it can contribute to better maintenance of it (Chang & Shih, 2004).
The acquisition of this knowledge depends a lot on the information about oral health received by those surrounding the children, such as the parents and other relatives, teachers, and oral health professionals. In this study, practically every participant (82.8%) reported having received general information. Regarding who supplied the information, children underlined their parents and other relatives, meeting results from the AlSadhan et al. (2017) study. However, in that same study, the sighted children reported receiving more information from their parents, contrary to children with visual impairment. Although not all parents from this study considered being an information source for their children, electing teachers and oral health professionals more than their kids. Perhaps because parents do not consider themselves safe sources and do not realize that they play such an essential role in transmitting this knowledge. Teachers are referred, as a minority information source by children, similar to the other study (Bekiroglu et al., 2012).
The parents were also evaluated regarding their knowledge, being that sighted children’s parents demonstrated, in general, superior knowledge, just like their children. This can show the importance of parents’ knowledge being influential on their kids,’ and consequently, in their habits and oral health, seeing as parents have an essential role in decision-making regarding their children’s health (Kenney et al., 2008).
Visual impairment is one of the risk factors that contribute to a higher prevalence of dental trauma (Munot et al., 2017). Furthermore, school-age was considered a risk of the occurrence of these traumatic injuries (Greene & Vermillion, 1964). However, when compared to similar studies, this study obtained different results, seeing as more sighted children presented a history of dental trauma (58.8%).
Various previous studies presented that children with visual impairment had worse oral health than their sighted counterparts (AlSadhan et al., 2017). The present study follows that evidence, seeing as in all evaluated indexes, except the DMFT index, the children with visual impairment presented higher values, even though there were no statistically significant differences.
The average of decayed teeth in both the dentitions was superior in children with visual impairment, contrary to the recent study by Kumar et al. (2020), in which the deciduous dentition of sighted children showed a higher decayed teeth rate. This can be explained by the fact that in that study, some children with visual impairment were institutionalized and had a more controlled diet and oral health habits. This way, it was verified that more sighted children were free of caries in both dentitions, meeting results from the other study (Ozdemir-Ozenen et al., 2012). Comparing the percentage of caries-free children in permanent dentition in the age group of 12 years old, the present study (80.9%) presented a substantially lower value than the estimated value for the Lisbon region (43.2%) (Calado et al., 2015).
The dmft index was higher in children with visual impairment (1.96 ± 2.93). Since the DMFT was higher in sighted children (0.35 ± 0.77), being as this trait was also observed in the study of AlSadhan et al. (2017). However, the average values of the present study were substantially lower when compared with the previous study. The dmft index was higher in comparison to the values of the DMFT index, and this can be related, according to Kumar et al. (2020), with the process of dentition change, seeing as deciduous teeth that are decayed end up suffering exfoliation.
It was observed that the gingival state was better in sighted children, such as in the study of AlSadhan et al. (2017). This can be related to the debris index, where it was also seen higher average value for children with visual impairment, which suggests a more inefficient brushing.
In general, most children (n = 65) presented good oral hygiene, evaluated through the simplified oral hygiene index. It was also possible to observe in this index a higher average value in children with visual impairment, such as reported by other studies (Kumar et al., 2020; Ozdemir-Ozenen et al., 2012).
In the study of AlSadhan et al. (2017), the authors referred that higher values for the GI, OHI-S, and DMFT indexes can be frequently related to parents’ school degrees. This hypothesis can also be inferred from this study. It was observed that the parents of children with visual impairment demonstrated a tendentially lower school degree and results demonstrated that children with visual impairment have the worst oral health.
Children with visual impairment can effectively have greater difficulty in brushing, which can influence its efficiency, as they do not possess a visual perception of dental and gingival anatomy. The present study corroborates this hypothesis because children with visual impairment reported a greater need for help during brushing (85.7%) and a check at the end by parents. These are, in fact, variables that can make a difference in bacterial plaque (AlSadhan et al., 2017).
Furthermore, a previous study (Jain et al., 2013) showed that children with visual impairment presented better oral hygiene than sighted children given that they were institutionalized and the brushing routine and caretakers’ supervision was regular. Showing that with training and consistent habits, children with visual impairment are able to maintain good oral health as sighted children (AlSadhan et al., 2017).
This study may have had some limitations, starting with the fact that it has a convenience sample. The data were collected in different schools, so the conditions and environments could differ slightly. Also, due to the current pandemic situation, it was not allowed to observe more individuals.
Conclusion
In the studied sample, it was verified, in general, more favorable results for sighted children. More children with visual impairment need help with brushing and more sighted children regularly go to dental appointments. The parents’ answers about the habits were almost the same, showing their involvement in their children’s daily caretaking of oral health. The parents, as well as sighted children, showed a vaster knowledge about oral health.
Regarding oral health, sighted children revealed better values, mostly because children with visual impairment had more tooth decay in both dentitions, and in classifications of GI and OHI-S indexes, sighted children obtained better scores.
The present study obtained similar results to previous ones. However, more studies should be conducted about this theme to allow a continuous verification of current oral health. It would be interesting to focus more on the oral hygiene habits of these children, to understand what their greatest difficulties are, to identify the most suitable utensils, and also to create more preventive measures that can aid these individuals.
Footnotes
Acknowledgements
The authors would like to thank the participants of all involved schools.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical committee
This study has been authorized by the ethics committee of the Faculty of Dental Medicine of the University of Lisbon and Governmental Department of Education of Lisbon.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: