
Abstract
Usher syndrome is a progressive form of deafblindness, which can have significant psychological consequences. This study aimed to get insight in the perceived impact of Usher syndrome type 2 (USH2) on families with a parent affected by this syndrome, and in the experiences of these families with social, professional, and peer support. Participants were 10 parents with USH2 living in the Netherlands, 10 of their co-parents, and 10 of their children. The parents filled in questionnaires and participated in a semi-structured interview. A photo-elicitation interview and a semi-structured interview were administered to the children. Interviews were transcribed and systematically coded, using thematic and open coding. Parents rated the family’s quality of life in general as satisfactory. Both negative and positive consequences were described of USH2 for the family. Parents without USH2 and their children stated to provide support to the parent with USH2, which was often described as self-evident. Some parents without USH2, however, described their family tasks as a burden. Some parents also reported that psychological problems of the parent with USH2 affected the well-being of other family members. Several parents and some children expressed that the syndrome was hardly discussed within the family. Unfulfilled family support needs were mentioned, a lack of involvement of family members in the professional support, as well as a lack of professional and peer support for children and partners. This study revealed that USH2 in a parent has impact on the entire family. Family-centred approaches are recommended for professionals who support parents with Usher syndrome.
Usher syndrome is a common cause of ‘acquired deafblindness’, defined as combined loss of hearing and vision that occurs after language development has started (see Ask Larsen & Damen, 2014; Dammeyer, 2012). Usher syndrome is a hereditary, progressive condition with three clinical types: Type 1, Type 2, and Type 3. The type of Usher determines the severity of the hearing loss, the extent in which vestibular problems are present and the age of onset of sensory loss (Bonnet & El-Amraoui, 2012).
In the Netherlands, Usher type 2 (USH2) is the most common type of Usher syndrome. USH2 causes hearing loss from birth, varying between mild to profound hearing loss, and retinitis pigmentosa (RP), a progressive disease of the retina. RP in individuals with USH2 usually manifests itself during puberty, starting with night blindness and leading to an increased reduction of the visual field and a gradual loss of visual acuity (Pennings et al., 2002).
Progressive vision loss in USH2 has a huge personal impact and demands that adjustments are needed repeatedly (Högner, 2015). Several studies found that people with USH2 experience high levels of stress (see Högner, 2015; Miner, 1997). Other studies showed that the self-image and self-confidence of people with USH2 are often affected, which can make people feel unhappy and depressed (Högner, 2015; Wahlqvist et al., 2013). Participants with USH2 also indicated that the syndrome had a negative social impact. As a result of their progressive condition, they experienced loss of friendships, changes in family roles, divorces, and concerns about their abilities as a parent (Miner, 2008).
Although the psychological and social impact of Usher syndrome has been shown in several studies, only one recently published study so far investigated the consequences of Usher syndrome for the family (see Wahlqvist et al., 2020). Wahlqvist et al. (2020) used questionnaires to assess health-related quality of life of 11 parents with Usher syndrome and 3 parents with other causes of deafblindness, and their family members. In addition, questionnaires on family climate and sense of coherence were administered. The survey revealed problems in health-related quality of life, especially in the parent with deafblindness, some negative aspects in the family climate, and a low to moderate sense of coherence between family members (see Wahlqvist et al., 2020).
Research on the impact of a disability on the family is in line with the increased focus on the social network of persons with a disability in health care research. According to Bailey et al. (1998), it is worthwhile to assess the impact a disability has on the quality of family life, because it can provide important information for policy, innovation, and ethical issues in health care (Bailey et al., 1998). The concepts ‘Quality of Life’ and ‘Quality of Family life’ are, however, difficult to define because they are situation-specific. According to Calman, quality of life is a multidimensional concept related to hope for the future, past experiences, and the present state of being (Calman, 1984). To enable assessment of quality of life, Schalock developed a model in which eight domains are divided into three areas: independence, social participation, and well-being (Schalock et al., 2007). Zuna and colleagues defined family quality of life as ‘a dynamic sense of well-being of the family, collectively and subjectively defined and informed by its members, in which individual and family-level needs interact’ (Zuna et al., 2010, p. 262). Zuna et al. (2009) point out that family quality of life is influenced by the support and services a family receives.
Whereas the study of Wahlqvist et al. investigated health-related quality of life of individual members of families with a parent with Usher syndrome (see Wahlqvist et al., 2020), no research has been carried out on these families perceived family quality of life, and on the support given to these families.
This study was carried out to get insight in the perceived impact of USH2 on the quality of family life in families with a parent affected by this syndrome, and in the experiences of these families with social, professional, and peer support. The following research questions were formulated: (1) How do parents with USH2 and their co-parents rate their family’s quality of life? (2) How do these parents rate the amount of social support? (3) Is there an association between the rated quality of family life and the rated amount of social support? (3) How do the parents and children experience the consequences of USH2 on their family? (4) What are the experiences of the parents with professional support of the family? and (5) What are the experiences of the parents with peer support of the family?
Methods
Ethics
The study adhered to the ethical principles for the involvement of human subjects in medical research that are formulated in the World Medical Association Declaration of Helsinki (Williams, 2008) and was approved by the scientific committee of an expertise and development program of the collaborating expertise organizations in the field of auditory and communication disabilities in the Netherlands. Informed written consent was given by the participants or, for participants below 16, by legal representatives.
Participants
Ten parents with USH2 formed a purposeful sample, recruited by email, social media messages, or face-to-face contact via service providing organizations for people with sensory disabilities within the Netherlands, organizations of self-advocates with Usher syndrome, social media platforms, conferences, or via people with Usher syndrome who were known to the researchers or were already recruited. The inclusion criteria they needed to meet for inclusion were (1) being diagnosed with USH2, (2) living with a partner, and (3) living with one or more children. In addition, 10 partners and 10 children of the participants with Usher syndrome were included in the study together with 10 of their partners and 10 of their children. Parents with USH2 were between 28 and 67 years old (M = 48.9) and parents without USH2 between 29 and 67 years (M = 49.4). The couples were of mixed gender. Eight parents with USH2 were female. Most parents (N = 14) had received higher education. Children were between 6 and 19 years old (M = 11; see Table 1).
Characteristics of the participating children.
Procedure
The ‘Family Quality of Life Scale’ (FQoLS; Beach Center on Disabilities, 2006) was translated into Dutch with permission of the authors. The FQoLS and the ‘Social Support List – Interactions’ (SSL-I; Van Sonderen, 2012) were adapted for the target group after applying the ‘Three-Step Test Interview’ (TTI) method (Hak et al., 2008) to a participant with USH2: the forms were made easier to read, statements of the FQoLS were more clearly formulated, and less relevant and unclearly formulated questions of the SSL-I were omitted.
After the administration of the questionnaires to the parents, they were interviewed separately. The parents were also asked to discuss with their child if he or she wanted to participate in a conversation about the family with the interviewer and if so, to make or select pictures or images about the family (see interview Children). If the child was willing to participate, the interview with the child was scheduled. Before the interview with the children was carried out the researchers had asked the parents what the child knew about the disabilities of the parent and it appeared that all children knew about this.
Questionnaires
The Beach Center FQoLS (Herafter FQoLS; Beach Center on Disability, 2003) measures family members’ satisfaction with five aspects: (1) family interaction, (2) parenthood, (3) emotional well-being, (4) physical well-being, and (5) disability-related support. Each item is rated on a 5-point scale ranging from totally untrue to totally true.
The SSL-I (Van Sonderen, 2012) measures experienced social support. The 5-point scale answering options range from seldom or never to very often.
Interviews
Parent interviews were conducted by the first author (PhD in educational psychology; senior researcher) or second author (MSc in educational psychology; junior researcher) at their home. The interviews lasted 45 min to 2 h. Before the interview started, the interviewer explained that the study aimed to investigate experiences of families with a parent with USH2. Most of the participants had never met the interviewer. None of the parents needed a sign language interpreter.
The interviewers used an interview guide with a semi-structured and a structured part. The structured part existed of four pre-formulated questions concerning advice for peers and other families, and experience with the interview. For the semi-structured part, the interviewers followed an interview guide that contained four statements, that were presented to the participants to respond to. In addition to each statement, the interviewers also used a list of possible topics that could be addressed if the interviewee did not address these spontaneously. Both the statements and questions (see Appendix 1) were based on the aims of the study and formulated by the first and second author in collaboration with a sounding board that consisted of a person with USH2, a partner of a person with USH2, and a senior researcher with expertise in semi-structured interviews.
The interviewer made sure there were breaks during the interview, to prevent fatigue. The conversations were recorded with a voice recorder and were then fully transcribed by a professional transcription bureau. The transcripts were then send for feedback to the participants and were adjusted, based on their comments.
Children were interviewed by a psychologist experienced in assessing children (MSc in psychology, clinical assessor) at their home. The psychologist met the child in the presence of one parent and checked whether the child agreed to talk with the psychologist about their family. Subsequently, an ‘auto photo-elicitation interview’ (Copes et al., 2018) and a semi-structured interview were held without the parent. During the pho-elicitation part, the child was asked to comment on family pictures the child had made or selected. During the semi-structured part, the psychologists introduced specific topics (see Appendix 2).
Quantitative data analysis
The scores on the SSL-I and FQoLS questionnaires were analysed using descriptive statistics. For all participants and for the parent with and without USH2 separately, means and standard deviations were calculated for the overall average score on Social Support and Family Quality of Life and for the average score on each of the five subscales of the FQoLS. For all participants, the means for subscales were analysed with the Wilcoxon signed ranks to test whether there were significant differences in the ratings of subscales. The means of the partners with USH2 were compared with those of the other parent, to see whether there were significant differences, using the Wilcoxon signed rank test. To calculate the association between family quality of life and social support, the Spearman correlation was calculated.
Qualitative data analysis
The transcripts of the interviews of both parents and children were coded with MAXQDA, a software programme for qualitative analysis (VERBI Software, 2014), using a combination of thematic and open coding (Flick, 2018). The thematic categories were based on the conceptualization of quality of life by Schalock et al., (2007), theory on coping strategies (Carver & Scheier, 1994), and on previous studies involving adults with Usher syndrome (Högner, 2015; Miner, 1997). New codes were added during the coding process when relevant statements were made by the interviewee that could not be related to one of the thematic codes. The coding results were achieved on the basis of consensus between the first and second author. The first two transcripts were coded by both researchers independently and then compared. On the basis of this comparison, the coding system was fine-tuned. The remaining transcripts were divided among the first and second author for coding. Subsequently, the coding results were discussed until the coders reached consensus with each other about the selection of codes, the labels of new categories, and the clustering of categories. The final codebook consisted of 9 main categories and 49 subcategories (see Table 2).
Codebook.
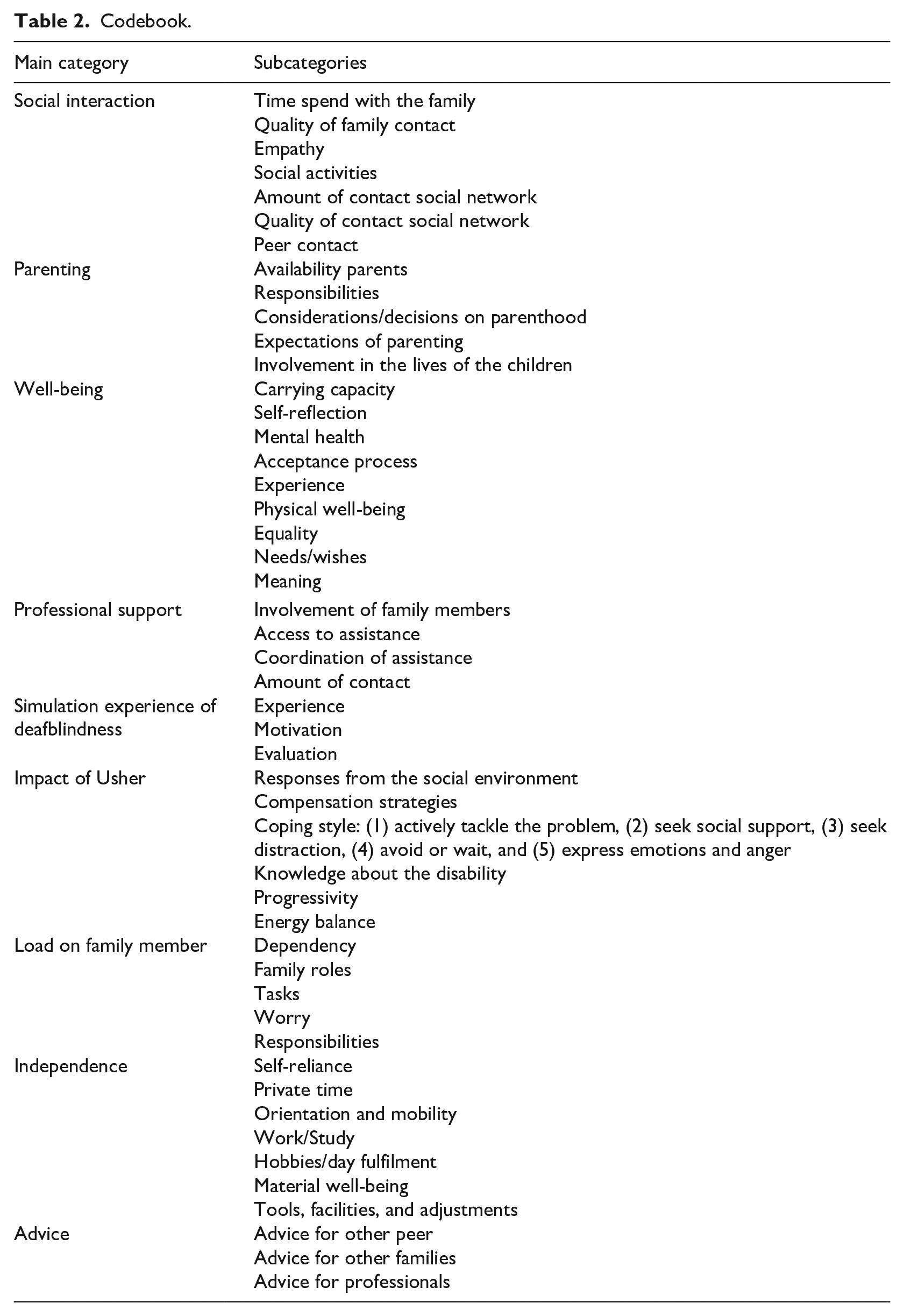
After the final coding of the material was performed, the first and second author analysed the coded interview material on how the participants experienced the influence of USH2 on the family and how the parents felt the family was supported. This led to the following nine themes guiding our results section of the parents: (1) quality of family life, (2) division of tasks and roles between parents, (3) coping, (4) psychological consequences, (5) parenting, (6) impact on children, (7) communicating about Usher in the family, (8) professional support, (9) peer support. The analysis of the final coded material also led to the following three themes guiding our results section of the children: (1) knowledge of the condition of the parent, (2) impact on the child and the family, (3) communication about Usher in the family. During the last phase, the analysis was refined by the selection of quotes illustrating the various perspectives of the interviewed parents and children.
The quotes are presented in the article with a participant code with a letter U, P, and C indicating whether the participant was a person with Usher, Partner, or Child. In addition, the gender of the participants is provided, in line with the COREQ checklist for describing qualitative research (Tong et al., 2007).
Results
Quantitative data analysis
The mean scores of overall Family Quality of Life (see Table 3) ranged between 3.5 and 4.77 (M = 4.03, SD = 0.37). This implies that the parents were generally satisfied with their family’s quality of life. Subscale ‘Emotional well-being’ had a significant lower average then three of the four other subscales: Family interaction, Z(19) = −3.24, p = .001, ES = −0.72; Parenting, Z(19) = −2.70, p = .005, ES = −0.60; and Physical well-being, Z(19) = −2.02, p = .044, ES = −0.45. The effect sizes indicate that there was a big difference between the rated quality of family life for ‘Emotional well-being’ versus the rated quality of family life for subscales ‘Family interaction’ and ‘Parenting’. However, the difference between the rated ‘Emotional well-being’ and the rated ‘Physical well-being’ was average. The subscale ‘Disability-related support’ had a significant lower average then all the other subscales except ‘Physical well-being, with Z(19) = −3.79, Z(19) = −3.55, and Z(19) = −2.01, respectively, for the comparison with the subscales ‘Family interaction’, ‘Parenting’, and ‘Emotional well-being’, and accompanying p values of .00, .00, and .44. The effect sizes of −0.85, −0.79, and −0.45 show that there was a big difference between ‘Disability-related support’ and the subscales ‘Family interaction’ and ‘Parenting’, but an average difference with the subscale ‘Emotional well-being’. The average overall social support score was 2.59 for all participants, which implies that on average the parents rated receiving regular social support (see Table 4). Parents with USH2 rated significantly more support than the parents without USH2, Z(19) = −2.04, p = .041, ES = 0.44. No correlation was found between the rated amount of social support and the rated quality of family life, r(20), −0.166, p = .485.
Ratings of the Family Quality of Life Scale.
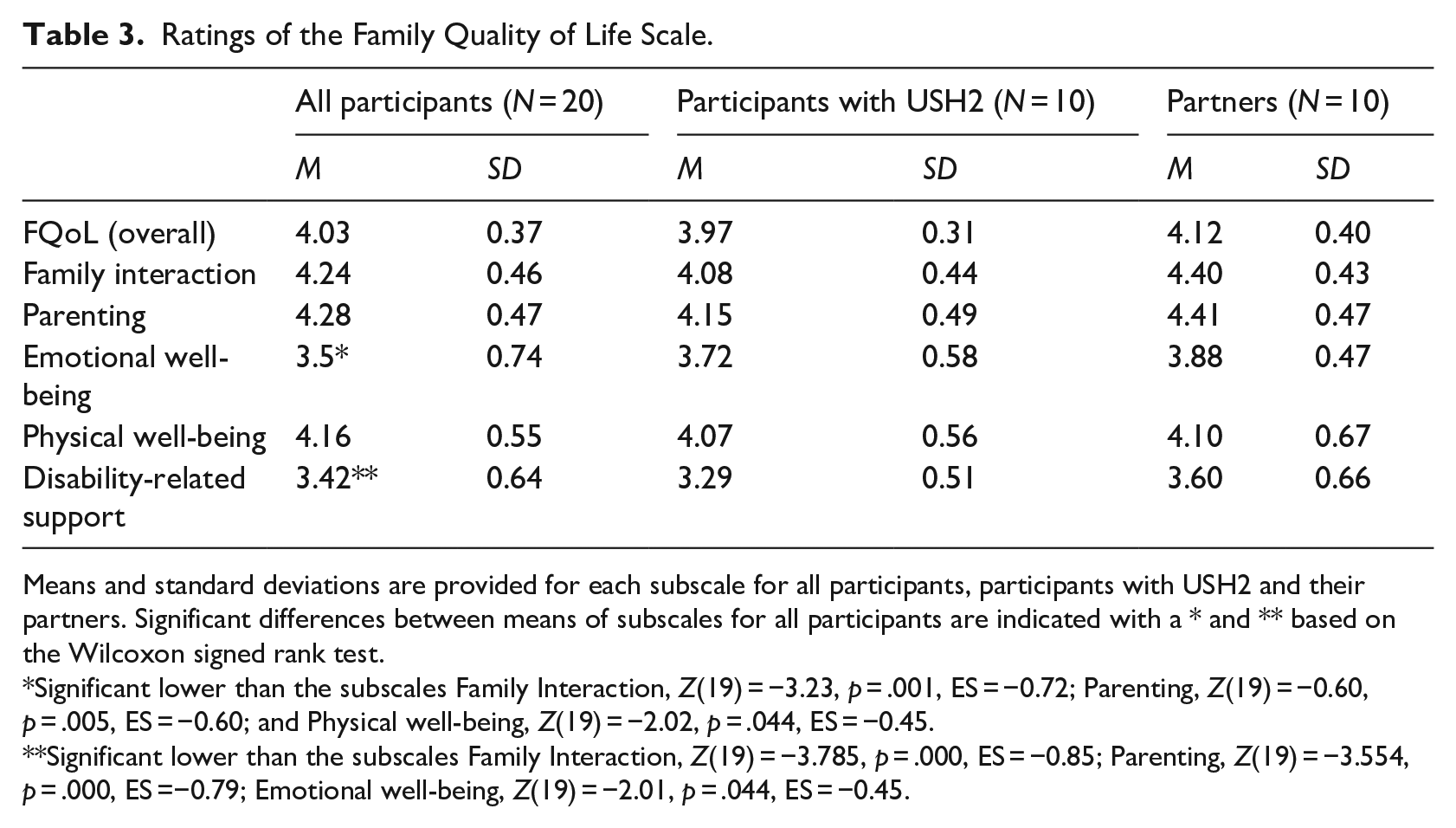
Means and standard deviations are provided for each subscale for all participants, participants with USH2 and their partners. Significant differences between means of subscales for all participants are indicated with a * and ** based on the Wilcoxon signed rank test.
Significant lower than the subscales Family Interaction, Z(19) = −3.23, p = .001, ES = −0.72; Parenting, Z(19) = −0.60, p = .005, ES = −0.60; and Physical well-being, Z(19) = −2.02, p = .044, ES = −0.45.
Significant lower than the subscales Family Interaction, Z(19) = −3.785, p = .000, ES = −0.85; Parenting, Z(19) = −3.554, p = .000, ES =−0.79; Emotional well-being, Z(19) = −2.01, p = .044, ES = −0.45.
Ratings of the Social Support List – Interaction.
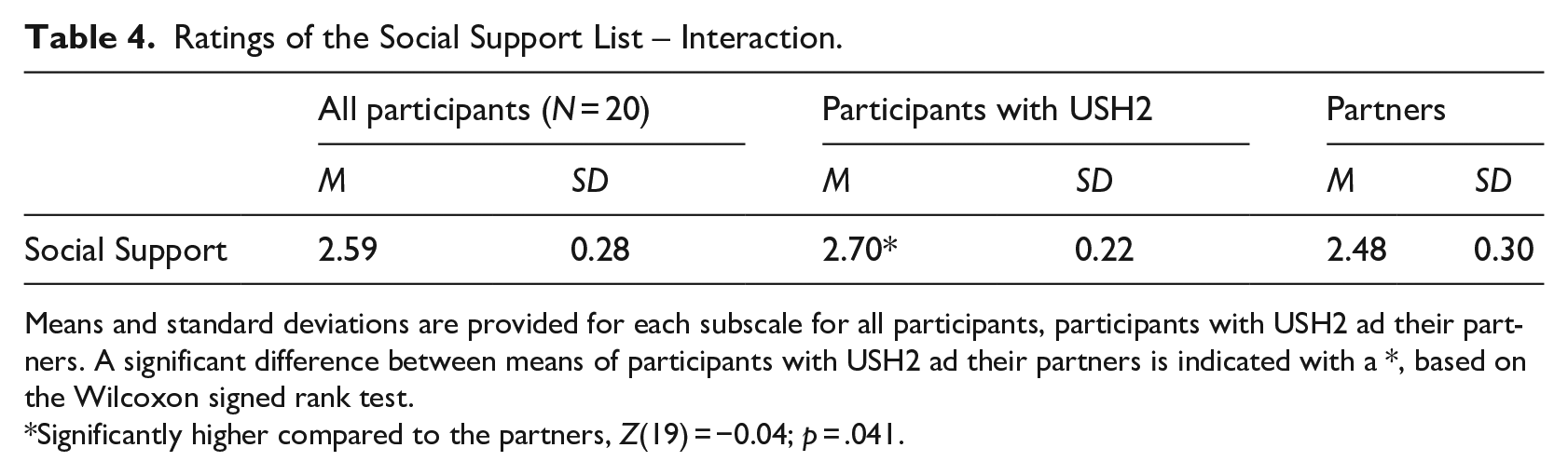
Means and standard deviations are provided for each subscale for all participants, participants with USH2 ad their partners. A significant difference between means of participants with USH2 ad their partners is indicated with a *, based on the Wilcoxon signed rank test.
Significantly higher compared to the partners, Z(19) = −0.04; p = .041.
Qualitative data analysis
During the analysis of the interviews with the parents, nine topics were identified: Family quality of life, Division of tasks and roles between parents, Coping, Psychological consequences, Parenting, Impact on children according to the parents, Communicating about Usher in the family, Experiences with professional support, and Experiences with peer support. During the analysis of the interviews with the children, the three topics were identified: Knowledge of the condition of the parent, Impact on the child and the family, and Communication about Usher in the family.
Family quality of life
Ten parents described their family’s quality of life as average or above average. One parent with USH2 stated that the quality of the family’s life was low because of relationship problems between the parents.
Some parents stated that Usher syndrome had little or no influence on the family’s quality life, some parents expressed having no idea about the influence, and six parents stated that the quality of their family’s life would have been higher if there was no Usher within the family.
[P3, Male] ‘Yes, if you look pure, really to the family, the four of us, yes, I think a 6.5. We have four very beautiful people, but Usher pushes that figure down heavily’.
One of the parents explained the reduced quality as the result of inequality between the parents. Two parents indicated that the family’s quality of life was probably higher because the challenges made the relationship between the family members stronger and was educational for the children.
[P5, Female] ‘Yeah, I also think, I’ve been talking to my husband about that, that Usher is also something that may deepen your relationship a little and what may be good for your children. To learn to take into account the needs of others. That not everything is the same everywhere in a family’.
Division of tasks and roles between parents
Several parents indicated that Usher has an impact on the division of tasks. It was often mentioned that the parent without USH2 was responsible for income, because the parent with USH2 had no or part-time work, and that this made the parent with USH2 do most of the parenting.
[P8, Male] ‘She is the linchpin of the family, actually. She has, I think, formed 90% of the family. And the other 10% I was allowed to do. But anyway, I still have my health [. . .] and the mouths have to be filled as well’.
Several parents explained that parents without USH2 had extra tasks in the household. Two parents without USH2 described to defend the parent with USH2 when the children did not want to do the tasks this parent had asked them to do. Some parents without USH2 indicated that they had a role in explaining to the outside world what is going on.
[P1, Male] ‘I found it awkward, because I always had the feeling that I am like a kind of walking information pole, I had to explain things to people’.
Many parents with and without USH2 described the division of tasks and roles as self-evident or as something that happened automatically.
[U4, female] ‘Walking to the car, walking in the dark, that’s just a real automatism. That’s just in there. A kind of oiled couple. Without the need for words that just goes like that’.
Other parents without USH2 described that they experienced extra tasks or roles as a burden.
[P3, Male] ‘I also know that I have a life of my own, and have to work, and do things for the children. So you can’t only support the other. And I’m telling you, Usher is quite prominent. So on a given moment you don’t feel like it either, in Usher’.
Coping
Parents with and without USH2 reported that coping with the progressive condition is a continuous process.
[U9, Female] ‘It’s so erratic that you can’t find some kind of grip in it either. And you both need to know that it’s erratic. And that it is a continuous process of tuning and that is just complicated. Because that is not natural. And then it is progressive too’.
Several parents with and without USH2 reported to actively tackle the problems they face. Examples given were explaining to a communication partner to speak slower and louder and orienting on computer programmes that can be used when the vision gets worse.
[U4, Female] ‘What I also find increasingly difficult now is access to information. So, say, working on the computer. I know there are solutions for that, so I’m like, ‘Okay, what I can see now, I’m doing’, but I know when my vision gets even worse that I can go to voice-over, special computer programs. So, I’ve got that in a drawer now, so to speak. Like, I don’t need it now, but I know it’s there.
Several examples were also given of an avoiding coping style. One of the parents with USH2 explained to avoid seeking professional help, because the person looks up to the intake. Another parent with USH2 described avoiding potential difficult situations.
[U9, Female] ‘I also notice that my comfort zone is getting smaller and smaller. Because I don’t want bruises anymore. I don’t want to be tired anymore. I want it to be easy. I don’t want to explain it anymore’.
Another way of coping with Usher that was described is to express anger and frustration. This was mentioned as a coping style of the parent with USH2 by six parents with and one parent without USH2.
[P3, Male] ‘. . . and also frustration, (name partner with USH2) is now and then literally frustrated, physically, that from time to time she hits something, and a hole in the door, and bumps her head. That is also partly due to her character, but that is also the complete frustration caused by poor eyesight and hearing’.
One parent with USH2 explained formulating reassuring thoughts. Two parents with and one without USH2 described seeking support to cope with difficult situations.
[U5, Male] ‘We have to ask for help now and then, it’s just as simple as that’.
Psychological consequences
Eight parents with USH2 reported psychological consequences now or in the past, such as stress, a burn-out, or depression.
[U10, Female] ‘I can still regularly fall into such a depression. That has to do with Usher, the fact that it’s dark, the fact that it’s cold, the fact that I can go outside less, the fact that I can do even less than in summer’.
Feelings of loneliness were mentioned by four parents without USH2 and eight parents with USH2. One parent without USH2 reported having less energy due to the communication challenges of the partner. Some parents with and without USH2 described that psychological problems of the parent with USH2 effected the other parent and one parent without USH2 explained that it effected the children.
[P3, Male] ‘. . . And the children got that too, because they actually feel her restlessness and her sadness’.
Some parents also indicated to worry about the future. Parents without USH2 mentioned worries about practical problems. Parents with USH2 also mentioned worries about psychological consequences.
[U5, Male] ‘Imagine that I have to stop my work. Well, I hope not, but I’m afraid it’s likely that I end up hitting rock bottom’.
Parenting
Most parents indicated that they were satisfied with how they were raising or had raised their children.
[U10, Female] ‘At the time I didn’t think so, but when I look back, I have to look back, well, I think we did a good job’.
One parent with USH2 indicated to be dissatisfied as a parent because of the relationship problems of the parents. Three parents (one parent with USH2 and two parents without USH2) indicated that the parent with USH2 was struggling with or had doubts about parenting.
[P2, Male] ‘My partner says: yes, I’m falling short, actually. For herself she feels that way, as if she is missing out. Because yes, you are not a real mother. You can’t go anywhere with your daughter, you can’t go shopping. You can’t play in the garden with your granddaughters’.
Impact on children according to the parents
Several parents stated that they found it important that their children were not hindered by having a parent with USH2. Several parents indicated that the family needs to take USH2 into account, for example, that it needs to be structured and tidy in the house so the parent is able to find things or does not fall over objects on the floor.
[U9, Female] ‘I think it is very important that the children can develop themselves as well as possible. And that Usher does not harm their own development. I am not saying that they should not take it into account. Or that Usher should not be there. From the beginning, that they were really just still on my arm, I have been aware of that. They must get the opportunities to develop themselves into who they are. But I am their mother. And so they will have to take Usher into account’.
Three parents gave examples showing that Usher syndrome had an influence on the way the children were raised. Two parents with USH2 indicated that their children had become independent relatively soon, probably because of having a parent with USH2.
[U7, Female] ‘Our youngest said something like this: “Well, I’ll cycle to school myself”. Then I thought: oh, I don’t know if that’s possible. But he was independent at a very young age, perhaps because of that (Usher of the parent)’.
Parents also described that children explained to their friends that they needed to take the disabilities of the parent into account, when visiting their home. Some parents described that their child took over tasks of the parent with USH2. One parent with USH2 described how she explained to the child not to feel responsible for the parent: [U3, Female] ‘But darling, I think it’s really sweet of you to help me, but I’m responsible for . . .’. That’s what I’m trying to do, make it really clear to him, that he doesn’t need to have a huge sense of responsibility to keep his mother safe, to help her cross the road.
According to one parent without USH2, Usher’s progressive character negatively influenced the involvement of the parent with USH2 in the lives of the children. According to another parent without USH2, the parent with USH2 was more strict to the children in order to maintain control over the situation.
[P2, Female] ‘My partner is quite strict. That’s because he doesn’t see it, so he has to hold the reins and that’s only possible if he keeps them on a short leash, that he knows what’s going on’.
Communicating about Usher in the family
Several parents explained that little is communicated about USH2 within the family. Various reasons were given: the situation is already difficult enough, the disability is stable, things are going well now so there is little need to talk about it.
[U3, Female] ‘Well, we don’t really pay much attention to that. That may sound a bit crazy, but . . . You can’t prepare for it anyway or you don’t know how it goes, so it’s just learning to deal with the situation as it presents itself every time’.
Experiences with professional support
Six parents without USH2 and four partners with USH2 mentioned negative experiences with professional support. Some of these experiences were related to the family: a lack of involvement of family in the support of the person with USH2 and a lack of considerateness of inequality in the relationship of the parents. Other explanations were not having a personal click with the professional, the professional has a single focus on the visual disability, too much professionals involved, the support was not attuned to the severity of the problems, or the professional had a lack of knowledge.
Several participants also reported positive aspects: the support provided insight, understanding and tools, supported the acceptation process, the professional provided a listening ear, the professional provided home-visits, the professional was involved.
Two participants with USH2 indicated that service provides should take the progressivity into account and prevent that an intake has to be done over and over again.
[U4, Female] ‘You actually need all your energy to just stand your ground. Not such a conversation with yet another professional asking: How was that? And how is it? And how much can you still see? And how much do you still hear?’
A type of support given to family members of USH2 that parents had mixed feelings about is the provision of exercises in which deafblindness is simulated. Twelve parents indicated that simulation was experienced as intense and did not correspond with the reality.
[U1, Female] ‘I’ve tried so many times to let people experience Usher through simulation glasses and headphones and the like. And then people think it’s very intense for a while, but it’s just so different when you can’t take them off’.
Ten parents with and without USH2 mentioned the importance of involvement of the other parent in professional support. One parent with USH2 choose not to involve the partner because it may cause a burden. Three parents without USH2 indicated to have missed being involved and four parents with USH2 indicated to have missed the involvement of their partner or children. One of these parents suggested that such involvement would have prevented the separation with a previous partner.
[U2, Male] ‘But when I look back at my ex, well then it [involvement in professional support] would have helped. Would that have saved the relationship?, yes, if we would have done so in time, we would still have stayed together’.
Two parents with USH2 expressed that there is a lack of professional support for the partner and children. Two parents with USH2 indicated that their children did not have any need for support. Several parents mentioned unfulfilled support needs of the family, especially the need for support in transportation and the need for domestic help.
[U1, Female] ‘Yes, we really need practical support (laughs). We really need someone who does the housework actually. That’s really just a crime right now’.
In addition, the following unfulfilled support needs were mentioned: psychological counselling for the parent without USH2, support in communicating about USH2 with the children, support for the family and social network in dealing with the impact and the progressivity of the disability, and parenting support.
[U3, Female] ‘. . . there is no attention for the family situation at the moment. Yes, of course you can do an experience tour. Or you can talk to a social worker about . . . But those are things that you really have to initiate yourself’.
Experiences with peer support
All parents with USH2 stated that they felt supported by contacts with peers with USH2. Parents without USH2 confirmed the importance of peer support for the parent with USH2.
[U3, Female] ‘Yes, then, then you just feel more understood by a fellow Usher, when he says, I know exactly how you feel. Then I think, yes, I believe you’.
Five participants with USH2 indicated that they also had negative experiences with peer contact. One of the participants explained that meeting someone who is much more seriously affected was confronting.
[U10, Female] ‘There is a lot of recognition, but sometimes it’s also a bit . . . Yes, I have . . . Then I tend to compare that with each other’s Usher situation. And that is sometimes confronting, actually’.
Three parents with and one without USH2 mentioned that they regretted the fact that there are no specific peer groups for partners and children of people with USH2.
[P1, Male] ‘For example, suppose you have a session where several partners are present to share experiences, I would like that. Yes, absolutely. I would be open to it’.
Perceived impact of USH2 on the family by the children
Knowledge of the condition of the parent
During the photo-elicitation interviews, one of the children spontaneously mentioned the disabilities of the parent with USH2. The child belonged to the oldest age group. The chosen pictures by the children were often of their room or objects to which they were attached. When the interviewer asked the children whether they knew that mom or dad can’t see well and hear well, all children confirmed that. Children gave examples of the consequences of disabilities, such as the parent is not able to ride a bike or a car, the parent is not able to run, the parent bumps on things or trips over clutter, the parent does not hear everything or uses aids.
[C4, Female] ‘Just that she quickly bumps into things. For example, if the cover of the dishwasher is open then she doesn’t see that, she bumps into it’.
During the interview, only a few children mentioned the term ‘Usher syndrome’. The statements of the children in the oldest age group showed that they knew or had experienced that the condition is progressive.
[C9, Male] ‘And that it’s getting worse and worse. And that she can’t do everything she wants anymore’.
Impact on the child and the family
Several children explained that they were used to help the parent or take the needs of the parents into account. A number of children mentioned that the other parent supported the parent with USH2. Older children explicitly stated that they did not know otherwise and that it was natural for them to support the parent.
[C9, Male] ‘Sometimes she says hey, what are you saying? I can’t hear you. If you want to say something to her, you can’t shout from upstairs. I used to do that wrong. But now I just come down’.
Some children also indicated that Usher has an emotional impact on the parent with USH2. When asked how they felt about this, they indicated that they found it sad for the parent with USH2.
[C6, Male] ‘You can see how hard it is for her. And I can imagine that too’.
Several children mentioned positive consequences of the condition of the parent, such as having a (guide) dog, not having to stand in line at an amusement park, being at home a lot with the parent, having a nice family help, or having a good relationship with the parent.
[C1, Female] ‘That’s a guide dog and he’s helping daddy. And she can run very fast and she often runs very good. And she’s very cute when she has her ears down’.
One of the older children stated to be worried that the parent will not be able to see future grandchildren. A number of older children mentioned that the social environment did not always understand the situation.
[C6, Male] ‘Yeah, I think it’s normal now. But yes, it’s always different when you compare it to other mothers. Because yes, she sees, say . . . It’s always . . . Because, when other people see my mother, it’s always a bit crazy actually. Because then she runs into things and stuff. Or she hears nothing’.
When children were asked whether there is a difference with other families, two children indicated that it is easier for other families to go somewhere. One child stated that their family situation was different because the parent with USH2 was always at home. An older child said, looking back, to have not missed anything at home.
[C5, Female] ‘I haven’t missed anything in my youth. I mean, she was always in the schoolyard anyway and we always had a babysitter and someone to help with cleaning’.
Communication about Usher in the family
One child explains having asked his parent about having Usher syndrome, because he held a lecture about Usher syndrome at school. Several older children mentioned that Usher syndrome is not something that is regularly spoken about in the family.
[C5, Female] ‘just because it’s . . . it’s always been there, so there’s not that much to talk about. Because . . . we know just a little bit how it is’.
Discussion
The study revealed that in general, parents with USH2 and their partners rated their overall family’s quality of life as satisfactory and also indicated to receive regular social support. The parents had different opinions concerning the impact USH2 has on their family’s quality of life. Some parents said to believe that USH2 had no or only a small effect, six parents stated that USH2 had a negative effect, and two parents stated that they believed it had a positive effect.
When comparing the average rated family quality of life on the FQoLS in our study with the ratings found in a study involving 566 families without disabilities (Zuna et al., 2009), the ratings in our study appeared to be lower. The mean ratings of ‘disability related quality of family life’ were the lowest rated aspect of family quality of life. This finding seems to correspond with negative aspects that several parents mentioned of the provided professional support and with unfulfilled support needs.
In our study we found that the rated ‘emotional well-being’ was also significantly lower than other aspects of family quality of life. This finding may be explained by psychological problems of parents with USH2, also found in previous studies (see Högner, 2015; Miner, 1997; Wahlqvist et al., 2020). Our study added to these studies the finding that both parents with and without USH2 experienced feelings of loneliness and that some parents described negative consequences of psychological problems of the parent with USH2 on the well-being of other family members. This is also in line with a study that found distress in partners of adults with sensory loss (Lehane et al., 2018). The relatively low emotional well-being of the parents without USH2 in our study may also be related to their extra tasks in the family, which were sometimes described as a burden.
Regular support tasks were also mentioned for and by the children, which corresponds with findings in previous studies of children of parents with disabilities (see Chen & Panebianco, 2020; Jurkovic et al., 1991). In our study, these tasks were often described as ‘self-evident’. But some parents without USH2 described having to defend the parent with USH2’s request for support of the children.
Another interesting finding in our study is that several parents and some children stated that USH2 is hardly discussed within the family. A possible interpretation is that this is a form of an avoiding coping style (see Carver & Scheier, 1994). Not discussing USH2 may have contributed to the feelings of loneliness that some parents described.
In contrast with not discussing USH2 in the family, several parents with USH2 reported discussing their feelings with peers with USH2. The fact that the parents without USH2 did not receive peer support may have contributed to the significantly less reported social support of parents without USH2 compared to the parents with USH2.
More research is needed to get insight in the specific factors that influence the quality of family life of families of which one of the parents is affected by USH2. The limitation of this study is that there was hardly no diversity in the participants with USH2: they were predominantly female and highly educated. Other limitations are that we did not validate the translated FQoLS questionnaire.
A strength of this study is that it used a mixed methods approach and investigated the perspectives of different family members: parents with and without USH2, and their children. Because childhood memories are vulnerable to reconstruction and errors (Wang & Gülgöz, 2019), studying the experiences of the children during their childhood can be seen as a strength. However, the abilities of children to reflect on their own situation are limited (Solberg, 2014), which needs to be taken into account when interpreting their statements.
The reported impact that USH2 can have on equality between and well-being of family members, and on the quality of family life, suggests that a family-centred approach is needed in the support of people with USH2 and likely also of people with other types of Usher syndrome. Since several participants mentioned that given support only focused on the individual with USH2 and a family-centred approach was missing, we recommend service providing organizations in the Netherlands to adopt such an approach, learning from the experiences with family-centred support in the care for people with other types of severe and chronic conditions, such as cancer (see Rait, 2015).
In our study, all participants with USH2 received or had received some type of professional support. Nevertheless, unfulfilled support needs were mentioned. Several participants also described the intake procedure of service providing organizations as a barrier to ask for support. In addition to positive experiences, negative experiences with professional support were described in cases where there was insufficient knowledge and skills of professionals. A recommendation for service providing organizations in the Netherlands is to attune services to the specific and changing needs of people with USH2 and their families, to make services easily accessible and to train professionals in supporting people with Usher syndrome. An example of specialized services for people with Usher syndrome and other causes of deafblindness can be found in the United States and Canada, where intervener services are offered in the community with the aim of enhancing participation and independence in daily life (see Wiley et al., 2014).
A type of support that was mentioned as helpful by many participants with UHS2 in our study is peer support. However, peer support was missed by some participants for partners and children. Facilitating peer support for all family members is another recommendation for the service providing organizations in the Netherlands, and to consider involving experts by experience in the care for people with USH2 and other types of Usher. For this, we advise the service providers to collaborate with self-advocate organizations for people with Usher syndrome and to learn from experiences with using experts by experience in nursing care (see Happell et al., 2019).
We conclude that our study revealed that USH2 in a parent has impact on the entire family. The consequences of USH2 are experienced daily, by both the person with USH2 and the family members. How the impact of USH2 is perceived can, however, differ between families, but also between individuals within the family. Longitudinal studies of families with a parent with USH2 and other types of Usher syndrome may reveal how these families cope with their family tasks and give more insight in facilitating and restricting factors for family quality of life over time and are therefore recommended. In addition, it is recommended to carry out such research involving diverse families with a parent with various types of Usher syndrome.
Footnotes
Appendix
Guide for the interviews with children.
| Topics | Examples of how this topic was discussed with the children |
|---|---|
| The condition of the parent | If the child did not mention dual sensory loss or Usher syndrome spontaneously, the interviewer would try to find out if the child knew about the condition. For example, by asking: Did you know that your mother/father has difficulties with seeing and hearing? When children confirmed this or had mentioned the disabilities or Usher syndrome earlier, the interviewer asked follow-up questions to find out what the child knew, for example, whether the problems in seeing and hearing were severe or not, whether the child thought the condition would improve, stay the same, or would get worse in the future. |
| The impact of the condition of the parent | The interviewer asked children whether there were activities or situations that were easy or difficult for the parent. The interviewer also tried to find out whether difficulties in activities or situations effected the family and the child personally, for example, by asking whether the child helped the parent. |
| Differences compared to other families | The interviewer asked whether the child thought that his family was similar or different from other families. |
| Professional support | The interviewer asked children if they knew whether professional support (‘help by someone’) was given to the parent, the family, or other family members. To older children the interviewer asked whether they thought sufficient support was provided. |
| Relationship with the parents | The interviewer asked the children to who the child would go to for help (when worrying about something, to ask for practical help or advice) |
| Talking about the condition of the parent | If the child mentioned the disabilities of the parent of Usher, a follow-up question could be formulated if the child talked about this with the parents and siblings. |
Acknowledgements
We thank the participating parents and children for taking part in our study. We thank Machteld Cossee for taking part in the Three-Step Interview method. We thank Annemarie Jongbloed and Machteld Cossee for their contributions in the sounding board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to thank ‘Verbindend Vernieuwen’ [United Innovations] in the Netherlands for funding our research.