
Abstract
Mindful of the assertion that children with vision impairment (VI) are three times more likely than their peers to develop a mental health problem, this study aimed to identify practitioner-perceived priorities in supporting the emotional well-being of visually impaired children, via eliciting self-reported explorations of professional practice and experiences of Qualified Teacher of Children and Young People with Vision Impairment (QTVI). Using a focus group-based interviewing technique with QTVIs from a single peripatetic VI advisory service in England, the study found that despite evident good practice, the QTVIs could feel inhibited by a lack of confidence in their ability to deliver adequate and appropriate intervention. This stems from a perceived lack of knowledge of resources available, a feeling of ‘reinventing the wheel’ and ‘bolting on’ to existing generic materials to try to improve their relevance to VI, and also an uncertainty regarding ownership of delivery of such interventions. QTVIs demonstrated clear willingness to support the emotional well-being of pupils on their caseload, but expressed a desire for more professional training, a clearer understanding of the breadth of the QTVI role, and a centralisation of knowledge and resources pertaining to emotional well-being. Therefore, this article recommends the development of resources for sharing good practice, as well as encouraging the VI educational sector to provide additional continuing professional development opportunities, and also potentially a review of the course specification of the Mandatory Qualification for Vision Impairment Teaching in England.
Keywords
Introduction
Promoting good mental health and emotional well-being in young people has become a key facet of the children’s rights agenda, both on national and global stages (e.g., Public Health England, 2016; World Health Organization, 2016). Yet the UK Government has been accused of ‘failing a generation’ (p. 1) by a joint report by the House of Commons Education and Health and Social Care Committees (2018) on children and young people’s mental health provision. The report identifies evidence of young people ‘falling through the gaps’ (paragraph 49) due to a lack of preventive input and also inadequate and inequitable access to care and treatment. In the sphere of vision impairment (VI), there is currently no specialised mental health provision for visually impaired children and their families (Petch & Mukhopadhyay, 2016). This is despite Harris and Lord’s (2016) comparative study into the risk of psychiatric disorders between visually impaired children and their sighted peers finding that ‘vision impairment among children as young as 11 years of age is associated with an increased risk of psychiatric disorder’ (p. 775) and that this risk is exacerbated in children wherein other Special Educational Needs and Disability was present.
Augestad’s (2017) systematic review into the frequency of occurrence of mood disorders in visually impaired children found several empirical examples to support Harris and Lord’s assertion (e.g., Brunes et al., 2015; Huurre & Aro, 1998, 2000; Pinquart & Pfeiffer, 2012, 2014) and therefore recommended that teachers and other educational practitioners be vigilant in trying to ‘detect whether some students show signs of behaviour that could increase their risk of developing mental health disorders’ (Augestad, 2017, p. 422). It therefore seems imperative that a consideration of the role of Qualified Teachers of Children and Young People with Vision Impairment (QTVIs) in this capacity is undertaken, especially given that Harris and Lord (2016, p. 776) estimate that ‘20% to 30% of children with sight impairment may be in need of professional advice and support’. The QTVI, as a ‘frontline’ professional (House of Commons Education and Health and Social Care Committees, 2018, p. 3) in managing, coordinating, and shaping a ‘range of proximal and distal influences’ (McLinden et al., 2017, p. 576) on a child’s life, may well constitute a key support mechanism.
QTVIs possess a unique and critical positionality in relation to the support of the children they work with, in terms of their potentially ‘transformative’ role (Ravenscroft, 2018) in supporting them to ‘achieve both academic outcomes and to make a successful transition to independent adulthood’ (VIEW, 2019, p. 19). A QTVI is a vital cog in the machinations supporting the delivery to visually impaired children of an additional, or expanded, curriculum (Hatlen, 1996; Sapp & Hatlen, 2010), which aims to ensure they develop a skillset that allows them to engage with both the ‘standard core curriculum . . . [and] the activities that are basic to their well-being’ (Opie, 2018, p. 76). If a child is unable to achieve these outcomes, then they are more likely to feel a sense of marginalisation (Augestad, 2017, p. 420), which could in turn negatively impact their mental health and emotional well-being (Huurre et al., 2001). The consequences of poor mental health as a child are both immediate, thus requiring significant educational and medical support, and potentially long-lasting, with childhood mental health issues often persisting into adult life (Scott et al., 2016, p. 146).
Context
Rationale
The rationale for this study thus also arose from a desire to respond to the findings of McLinden and McCracken (2016) in their review of the role of QTVI in facilitating inclusive education. It aimed to meet one of their key recommendations, that of using qualitative interviewing to produce rich data to enhance the findings of their study, which examined firsthand the professional experiences of specialist VI teachers via creation of a large-scale dataset stemming from questionnaire responses. While several studies have also provided an overview of the role of the QTVI (e.g., Keil, 2012; Mason & McCall, 1997; Ravenscroft, 2015), there is a dearth of research that actively incorporates the viewpoints of QTVIs in a knowledge-generation capacity. Therefore, this study aimed initially to identify practitioner-perceived priorities in supporting the emotional well-being of visually impaired children, via eliciting self-reported explorations of professional practice and experiences of QTVIs.
The study was also influenced by McLinden et al.’s (2017) mapping of the role of the QTVI onto the ecological systems theory model expounded by Bronfenbrenner (1979, 2005). Their research positioned the QTVI as a bridge to curriculum access, noting the array of direct and indirect functions undertaken by the QTVI to ensure that a visually impaired child receives a holistic and appropriately tailored curriculum. The 1978 Warnock Report heralded a move towards greater inclusive educational practice, which has been translated over the past four decades as an increased incidence of mainstream educational placement for children who have a VI and no further additional needs (McLinden & Douglas, 2013). Resultantly, many QTVIs now play an itinerant role in supporting children on their caseload. They are likely to plan and/or deliver an additional curriculum for visually impaired children, outside of but feeding into, the core curriculum of their peers, based on the supposition that they may require more formally structured learning experiences to develop certain skillsets to fill in any ‘gaps’ in learning caused by the absence or reduction of vision as an integrating sense.
Douglas et al.’s (2009) literature review of additional curricula found that among the key elements covered, supporting children to develop social and self-advocacy skills has a critical place. This is recognised by Mandatory Qualification outcome 6 (National College for Teaching and Leadership, 2015) of the VI teacher training standards, which asserts that a key tenet of the QTVI role is to support the development of the emotional well-being of pupils with VI (McLinden et al., 2017, p. 575).
Emotional well-being
Emotional well-being is recognised as a key enabler to educational and wider societal inclusion. Public Health England (2014, p. 4), for example, asserts that effective social and emotional competencies are associated with greater health and well-being, and better achievement. Despite this, while there has been a drive by educational settings to implement strategies to support the academic attainment visually impaired children, until recently, the commitment to developing their social and emotional well-being has not benefitted from the same impetus (Bearfield, Douglas & Myko, 2005, p. 6). Despite the 2014 Children and Families Act marking a statutory recognition that children’s emotional well-being must be supported on a parity with their physical health (Department for Education [DfE], 2014a, Part 3, section 25, 2, a), the recent House of Commons Education Committee (2019) found that 5 years on, ‘this generation is being let down – the reforms have not done enough to join the dots, to bring people together and to create opportunities for all young people to thrive in adulthood’ (p. 4). It therefore seems a prescient, and pressing, point to re-examine the role of the QTVI in relation to supporting emotional well-being.
Methodology
This project explored the views and experiences of practitioners from a peripatetic advisory VI teaching Service in England regarding supporting emotional well-being in children on their caseload. To do so, it utilised an ascending methodology (van Meter, 1990), in that it hoped to generate data and ideas, and accepts that while outcomes may proffer maximum theoretical understanding for the participants, outcomes may be non-generalisable (Faugier & Sargeant, 1997, p. 791). It cannot be said that this research could ever be completely inductive, as although it attempts to capture the experiences and perspectives of participants, the discussion was based around a topic of the researcher’s choice (Rubin & Rubin, 1995), which stemmed from professional and theoretical knowledge. Thus, it can be said to ascribe to an abductive theoretical approach, in terms of aiming to discover the social constructions of those experiencing a phenomenon and how it conceptualises their reality (Blaikie, 2007). It may potentially offer an innovative addition to the field of VI-educational research in that the application of the boundary of a single ‘case’ to a team of QTVIs could be considered revelatory (Yin, 2003), as there is a dearth of research that delineates the boundaries and complexity of the role of the QTVI. Therefore, a study of this nature has the potential to provide strong insight and generate emergent theory (Robinson & Seale, 2018).
Focus groups
The drivers behind the methodological design were both theoretical and logistical. Given the constraints of the teaching timetable and the disparate geographical nature of caseloads of the teachers involved, it is only on a monthly basis that dedicated time is arranged for staff to formally meet. One of said staff training sessions had been allocated to the researcher by the ‘gatekeeper’ (Homan, 2002, p. 23), in this case, the Head of Service, who gave permission for the research to take place. Therefore, a focus group format was utilised, rather than individual interviews.
Focus groups may be considered a dynamic format, in terms of rapidity of data generation when there are time and logistical constraints related to its collection. Because of the interaction between participants, they possess ‘a “synergy” that makes them more productive than an equivalent number of individual interviews’ (Morgan, 1996, p. 138). They can provide naturalistic, less artificial (Wilkinson, 1999) opportunities for collective sense-making (Frith, 2000; Wilkinson, 1998), but perhaps most importantly in the context of this study, they constitute a ‘useful exploratory tool for looking at under-researched areas’ (Braun & Clarke, 2013, p. 110).
Focus groups require the researcher to play a more active role than in other interview formats, in terms of creating and directing the discussion (Frey & Fontana, 1991; Morgan, 1996). Thus, a topic guide was created to provide stimulus to discussion, with related leading questions to allow the discussion to emerge inductively to an extent, but also be managed where necessary (Figure 1). This approach was also adopted due to the time and logistical constraints of the data collection. Because a single, 90-min slot had been allocated, it was necessary that the facilitator take a more structured, directive approach. However, this was done to funnel the discussion and elicit meaningful dialogue, rather than to disrupt the flow or control the participants (Krueger, 1994; Merton et al., 1990; Morgan, 1996).
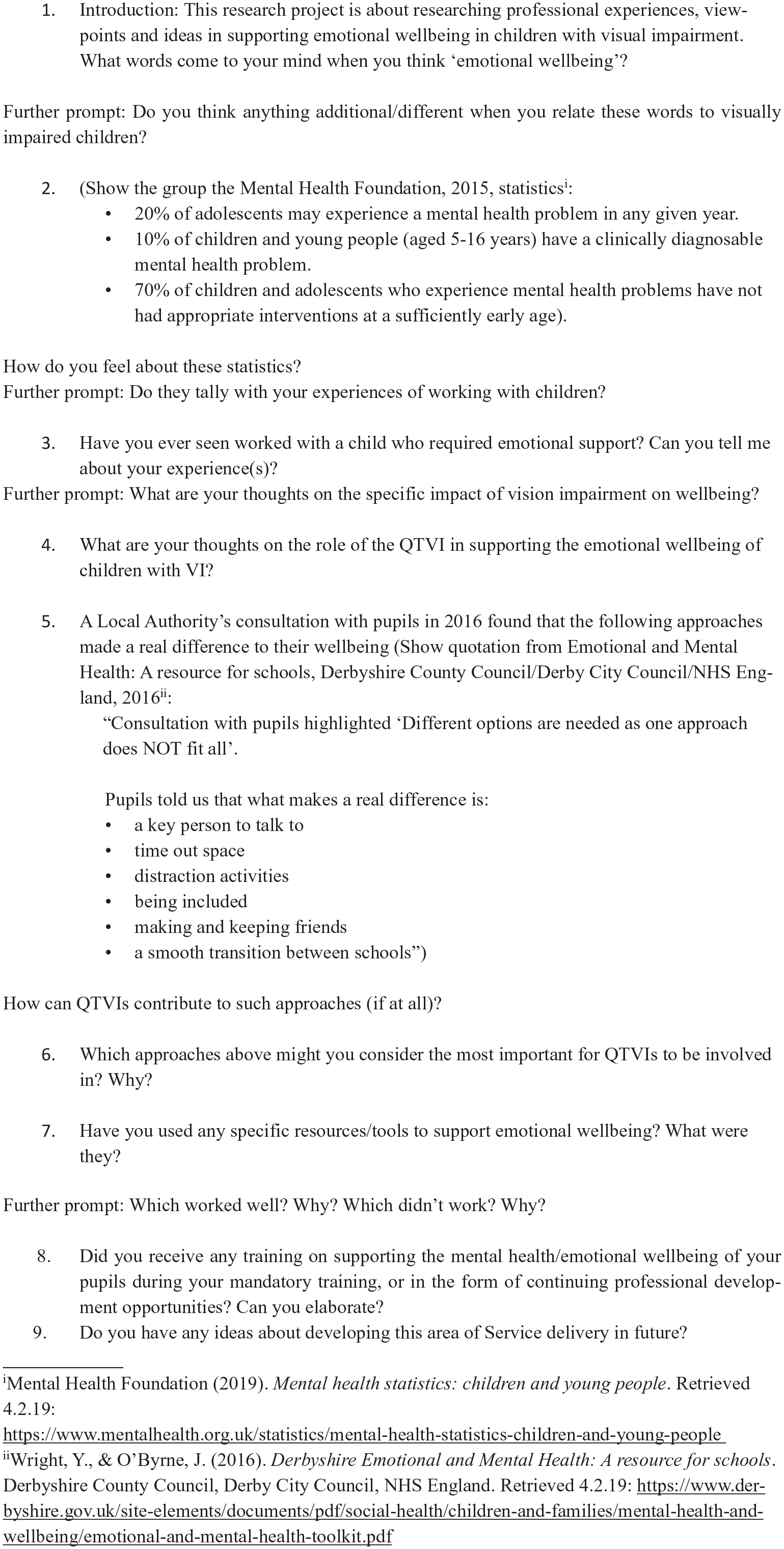
Focus group topic guide.
Focus group moderation ‘involves being finely attuned to the dynamics of groups, and the unstated processes that can go on in groups (such as power and silencing)’ (Braun & Clarke, 2013, p. 127). Therefore, conversational continuers were applied at relevant junctures and included employing silence, indicating concurrence, repetition, or recycling part of an answer or formulating and vocalising an inference pertaining to the participants’ contributions, which also offered the function of validating theory (Bischoping & Gazso, 2016, pp. 113–114). This approach was fairly successful, but reflection on the process has identified room for improvement. When re-listening to the focus group audio recordings, it was clear that at times the facilitator was too quick to fill conversational gaps when carefully employed silence may have induced another member of the group to respond.
Sampling
Pragmatic considerations informed sampling decisions. Because the research objective was to garner professional experiences, it followed that a purposive (Abrams, 2010), homogeneous sample was selected. All eight participants were QTVIs who had the shared goal of generating key information that may inform their own practice (Moutsakas, 1994) and who were likely to possess key insights into the topic studied (Padgett, 1998). However, given that all worked for the same Service and were available and prepared to participate in the study, it could also be considered a convenience sample. The benefit in one sense is that because the interviews took place in a work environment during official working hours, there may have been a sense of formality about proceedings, allowing participants to remain focused and ‘on task’, leading to the generation of a quite large data corpus.
However, equally, the familiarity level of the participants undoubtedly had some impact on the discourse, although not as Braun and Clarke (2013, p. 114) suggest – ‘being part of the same social network (e.g . . . as work colleagues) can inhibit disclosure and open discussion’. Conversely, participants felt comfortable enough to share related personal anecdotes pertaining to their own emotional well-being and that of their families, perhaps on occasion leading them into territory defined as ‘too settled’ by David and Sutton (2011, p. 136), thus leading to danger of conversational tangents and requiring the aforementioned moderator intervention. In addition, the personal nature of this emergent data heightened both the level of data sensitivity and the emotive nature of the discussion. This resulted in further checks with participants after the event to ascertain whether permission was still granted to use all information, or whether any should be redacted from the transcripts, due to its highly personal nature. It transpired that all participants were, however, happy to include all existent data in the study.
Ethical considerations
This strategy was grounded in an acknowledgement that ‘research is not a value-neutral activity’ (Braun & Clarke, 2013, p. 65). Hence, this deontological ethical approach informed the research design from its inception and influenced the methodology continuously, rather than simply being considered during reflection after the event (Brinkmann & Kvale, 2008). Participants’ names were anonymised and coded as single letters and all were contacted after the interview in a process of member-checking (McMillan & Wergin, 2002, p. 122) to confirm consistency of meaning and interpretation. In addition, participants were asked to give formal written consent to the recording and use of data, as ‘the principal of informed consent is a standard feature of ethical procedure in social research’ (Homan, 2002, p. 24), and were reminded that this consent could be withdrawn by them at any point without repercussion.
Transcription and coding
Following data collection, an orthographic transcription of data was produced using ‘experiential analytic methods’ (Braun & Clarke, 2013, pp. 168–169), focusing on words spoken, rather than non-verbal cues or verbal emphasis. This decision stems simply from the scope confines of this study, as it may have been useful to invoke a more in-depth narrative or discourse analytical approach to elicit more fine-grained analyses of meaning (Bischoping & Gazso, 2016). NVIVO was then used to analyse the transcription of the focus group data. It must be noted that despite the application of ‘in vivo’ coding, the process cannot be said to be truly emergent and inductive, as there has undoubtedly been a thematising of meanings (Holloway & Todres, 2003, p. 347), based in prior knowledge of the existing research field, actively applied by the researcher, whether purposefully or not (Taylor & Ussher, 2001). Therefore, the coding employed herein can be considered an abductive process, as it has not, as Braun and Clarke (2006, p. 84) assert, taken place within an ‘epistemological vacuum’.
A process of ‘subsumption’ (Smith, Flowers & Larkin, 2009) was then undertaken to promote and refine codes into themes (see Figure 2). This demonstrates a recursive approach to analysis (Braun & Clarke, 2006, p. 86), in that data was returned to and re-examined continuously throughout the analytical process. It is hoped that by incorporating the expressed views of participants and relating them to the wider body of research to the point of theoretical saturation, the themes identified or developed herein will be robust and linked to wider implications. A latent thematic analytical was undertaken, with interpretations of data meanings going beyond superficial, semantic level analysis (Boyatzis, 1998). It must also be noted that the themes discussed herein have been included as they are considered to possess ‘‘keyness’’ (Braun & Clarke, 2006, p. 82) relating to the analytical focus of the research question, rather than due to their prevalence within the dataset.
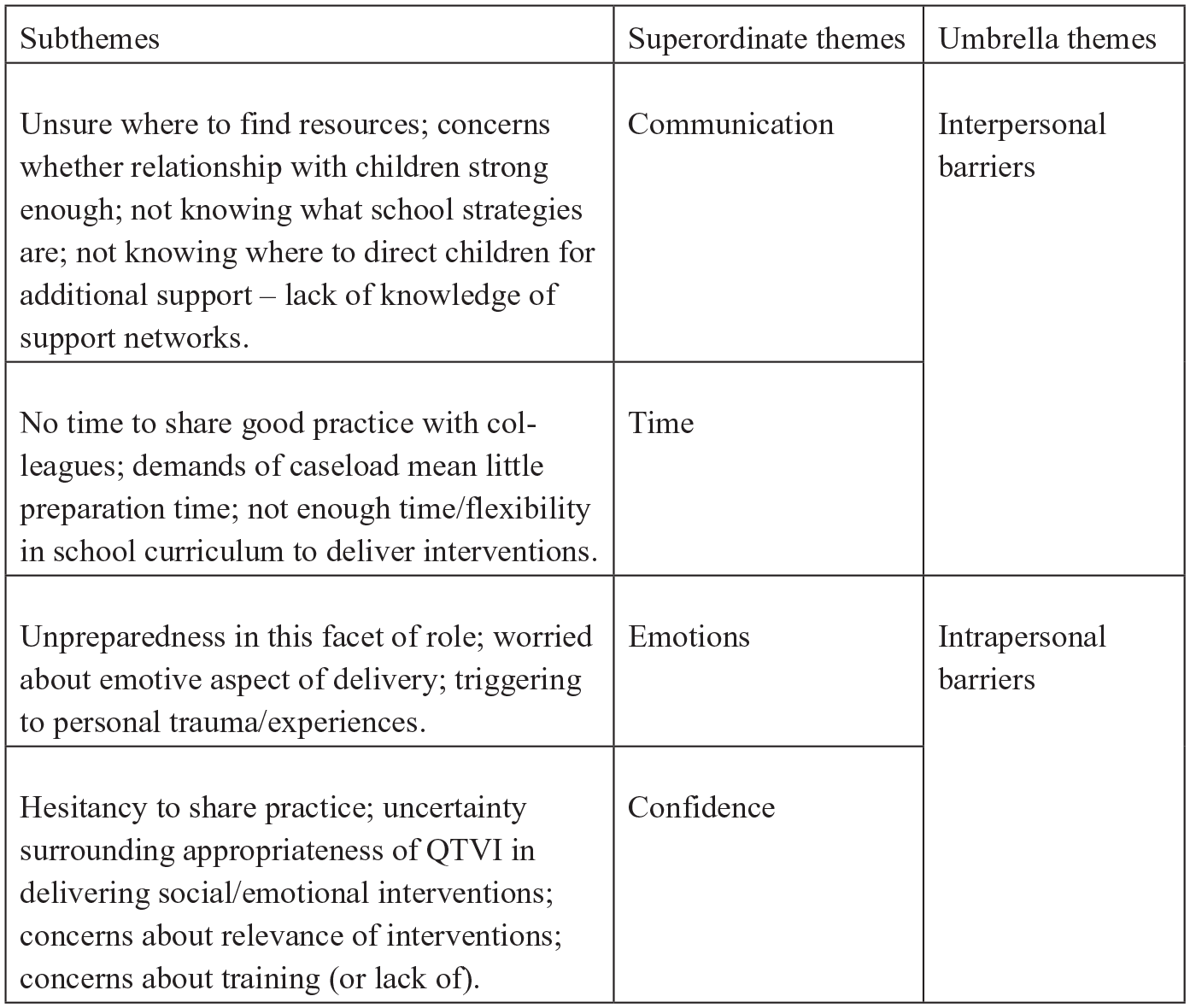
Table of coded themes emerging from focus group data.
Findings and discussion
While the group was exploratory in its aim, it was hoped that the experience would provide a collective forum that would go beyond sharing teaching tips and offer an opportunity for critical reflection (Cornwall, 2012, p. 136). It was hoped that the professionals would be able to share a wealth of experience and expertise, which would generate identification of best practice and priorities in supporting the emotional well-being and mental health of the pupils on their caseloads, in terms of strategies, resources, and approaches. However, it soon became clear that the participants all felt strongly about the importance of supporting emotional well-being in their pupils, but that they felt constrained in their ability to do so, thereby viewing inclusion through a lens of exclusion (Paliokosta & Blandford, 2010, p. 179) and focusing largely on the difficulties and barriers faced. Thus, the sub-themes applied during the coding process reflect this, and two overarching ‘umbrella’ themes were identified and are discussed below.
Interpersonal barriers
The participants outlined their perspectives on what the role of the QTVI in supporting emotional well-being entails. However, they felt that it was difficult to achieve an overarching definition of boundaries and baseline expectations of the role due to several (potentially constraining) variables, including caseload numbers, personalised levels of input required by each student, strength of existing support networks, and the reaction of the visually impaired child himself or herself:
I’d certainly say it’s difficult for us to be consistent . . . we’re sort of, responding individually, you know, depending on how much capacity we’ve got, and so on, and depending on how involved we are with that student. (H) I think our role is to ask questions, to not ignore it and to ask questions, but I think it depends on the pupil and what the level of your involvement is. Some people we don’t see that often, we don’t know that well. (C)
There was initially an underlying hesitancy and uncertainty as to how effective the QTVI could be in this role, or even whether the QTVI is the right professional to take it on:
Unless it’s with a pupil you are seeing very regularly . . . it’s quite difficult, ‘cause from a social and mental health point of view, would a teenager, would somebody relate to someone who comes in very infrequently? I don’t know. They need somebody who they can build a relationship with and that’s not necessarily us. (C)
However, after a participant shared a powerful story about how a QTVI, who visited a child monthly, had been the person a child had opened up to about her fears of dying due to her medical condition, rather than a ‘closer’ adult, the team began to acknowledge their impact:
You can’t underestimate the relationship you have, even if you’re only going once a month . . . (D) You are consistent. (C) That’s right. (D) That’s useful to know, yeah. (H) And I think if they’ve got that confidence in us . . . that we will advocate for them and try and put things in place, perhaps people will, from time-to-time, share their emotions with us . . . (D) (Several people) Yeah . . . I suppose ’cause we’re on their side aren’t we? (A)
(Lots of concurrence)
. . . ’Cause when we see them, they know that we come to see them . . . (B) . . . And I think it’s easy [for us] to dismiss our impact. (D)
This sense of collective buoyancy continued; there was an acknowledgement of existing good practice embedded by some schools, but tempered with warning that visually impaired children may miss out on incidental learning, such as posters on walls advertising services, or they may miss an announcement in assembly due to not attending to study Braille. This therefore reiterates the QTVI’s vital role in supporting children in ‘learning to access’ (McLinden et al., 2016, p. 177), and to develop the awareness and self-advocacy skills to be comfortable in asking for any help they might need:
It has to be quite clear to the children where their support network is and how to access it . . . I mean I feel like it does for, for every child, but it’s that wider world learning that our children quite often miss. (E) I think when you’ve got any difficulties, that self-awareness and that support network, knowing you’ve got people who help you and understand you is even more important. (C)
This demonstrates the importance of the QTVI in contribution to the meso-systemic level of support of the children (McLinden et al., 2017; McLinden & McCracken, 2016). Their ability to act as a conduit for information can have a key contribution to facilitating ‘“systemic optimism” to reflect the child’s need to be supported by adults and peers who can help them direct their efforts towards positive change for the future’ (Bailey, 2012, p. xvi).
Intrapersonal barriers
As demonstrated above, a striking outcome was the apparent self-perceived lack of confidence among professionally trained and highly experienced QTVIs in identifying and delivering appropriate resources and interventions. One participant had brought along an exemplar resource to share with the group but seemed reluctant to do so, which suggested insecurity:
I don’t know if other people want to say first what they use? (G)
This inference was strengthened by her apparently relieved response to positive group reactions to the resource she had brought to share:
I’ve done ‘Strengths With Children’ [the resource]. (F) Yeah I have. (D) So that makes me feel a bit more confident in sharing it then, because we’ve . . . all kind of had a go at using these! (G)
Upon member-checking with this participant during the data analysis, she confirmed that she had, in line with Paliokosta and Blandford’s (2010, p. 179) findings, felt a sense of inadequacy in sharing her use of the tool, which she ascribed to her perceived lack of certainty surrounding the teaching of emotional well-being strategies.
However, as the discussion progressed, it became clear that many team members were already employing impactful strategies and confidence grew:
It’s been fascinating doing this work [on emotional wellbeing], and one of the youngsters I’ve worked with in a particular secondary school, you know, I was just amazed, ’cause one of the things in this book is a whole load of descriptions of an emotion, and then you have to say ‘what is that emotion? And they’re very subtle – and this young person at that time was in Year 8, and was able to identify, you know, words like ‘disconnected’, and you know, he was so literate in the emotional stuff, and I think one of the values of it was that it, it, it brought to his attention, how emotionally literate he was . . . (G) (Interjecting) ‘Brilliant’. (E)
This could suggest that having a forum to share good practice may be useful for QTVIs to enhance expertise. Additionally, despite outlining several successful applications of a range of tools and resources pertaining to supporting emotional wellbeing within the discussion, participants expressed uncertainty regarding their effectiveness in this context. This may imply that a lack of explicit training in supporting emotional well-being could be a key inhibitor of QTVI confidencempetence in this facet of their role. This therefore indicates that on a national scale, additional Continuing Professional Development opportunities in supporting emotional well-being should be developed and that perhaps an evaluation of the content of the Mandatory Qualification for VI Teacher Training Course is necessary. As Sapp and Hatlen (2010, p. 343) state,
It is not good enough for teachers to know that students with [vision] impairments may have deficits in social skills: they must know how to assess their students’ social skills and provide targeted instruction for the areas of deficit.
An expected minimum standard that QTVIs undertaking the UK’s DfE (2016) Mandatory Qualification for Teaching Children with a Vision Impairment (MQVI) must evidence is their knowledge and understanding of ‘how to help learners with VI to develop effective social and emotional skills’ (Standard 6.7, DfE, 2016, p. 22), yet there are very few (if any) formal and nationally recognised continuing professional development opportunities for QTVIs to refresh or build knowledge in this area following completion of the qualification, which is a clear issue for the sector to address. A lack of availability of such resources might make it tempting to lower the priority of mental health/well-being in Service planning and delivery, given time and budgetary constraints. However, it also is vital that Services are proactive in searching out relevant courses outside of the sector and applying the knowledge gleaned to a VI context, and sharing good practice to other VI educational providers, stakeholders, families, schools and most importantly, with visually impaired children themselves.
In addition, there must be better dialogue between VI-related academia and professional contexts. The DfE (2016) requires that MQVI course providers must ensure that ‘there are sufficient, up to date, specialist teaching resources available that are relevant to training teachers of children and young people with VI’ (point 5.5, p. 14). Therefore, providers must take an osmotic approach to course content development. They must endeavour to look ‘to the field’ to accumulate contemporary knowledge of resources and good practice, while simultaneously undertaking and sharing new research to effectively equip the next generation of QTVIs and allow current QTVIs the opportunity to hone or develop their skillset. Thus, a national cohesive movement, involving all facets of the VI education sector, towards both the creation and sharing of resources to support emotional well-being of visually impaired children is not only useful but also necessary.
Reflections
Future studies
It is clear from the data generated that there is a need for further research on both: (1) supporting the development of emotional well-being among visually impaired children (as also asserted by Royal National Institute for the Blind, 2013) and (2) how to maximise the effectiveness of the ‘social dimension’ (McLinden & McCracken, 2016, p. 485) of the QTVI’s role in cohesively facilitating inclusive education across systems to support a child’s emotional well-being. To meet the former recommendation, individual semi-structured interviews could be undertaken with the focus group participants. Beyond using interviews to triangulate data, they can also be used to explore specific emergent details in more depth (Crabtree et al., 1993). This could lead to opportunities for a more micro-analytical form of data analysis, such as interpretative phenomenological analysis (IPA).
Adopting an IPA approach may offer a more ‘detailed and nuanced analysis of the lived experience of a small number of participants with an emphasis on convergence and divergence between participants’ (Smith et al., 2009, p. 202), thereby potentially identifying more detailed (or at least a wider array of) strategies for supporting emotional well-being stemming from experiential learning. Such a study would be an extremely useful addition to the field, given Douglas et al.’s (2009) findings that the heterogeneity of the population with VI, combined with the subjectivity of interpretations of outcomes, means it has thus far been difficult to ascertain exactly which interventions in supporting emotional well-being make the biggest impact at grassroots educational level. The richness of data generated by interviews could also explore further a key thematic outcome of this study via establishing intrapersonal confidence levels in QTVIs in delivering this facet of their role.
To enhance knowledge of the socio-ecological role of the QTVI in supporting emotional well-being, a case study approach could be taken to examine in-depth the role of the QTVI at the meso-systemic level (McLinden et al., 2017) surrounding the child. To achieve this, repeating the focus group activities with participants including the different stakeholders involved in the support of the visually impaired child could help to contextualise the role of the QTVI within the wider multi-agency support picture and identify opportunities for further collaboration. Segmentation could be used in sampling to vary the composition of these future groups to build in a ‘comparative dimension’ (Morgan, 1996, p. 143) to the data. Indeed, the focus group format would be a suitable means of involving the pupils themselves in this exploratory process, given the appropriateness of the methodology for pursing objectives that are empowering and participatory (Morgan, 1996, p. 149). This appears to be a particularly pressing need, as giving visually impaired children the opportunity to actively participate in knowledge-generation pertaining to their support is not only an expectation of the disability studies paradigm (Davis & Watson, 2000; Oliver, 1992), but is also now their legal right (DfE, 2014a).
Limitations
A limitation of this study is its small sample size, which inhibits generalisability. To overcome this, the study could be repeated with different cohorts of QTVIs. Data could be comparatively analysed in a number of ways: for example, between those QTVIs working in peripatetic capacity and those who are based at a single site, such as at a specialist school or integrated resource. It must also be acknowledged that there may be clear differences in outcomes if QTVIs were interviewed from different peripatetic services and data compared. We may infer that geographic location (i.e., rural or urban area, small county or large), nature of local offer (i.e., whether service provides a teaching or advisory role), and balance of caseload (whether QTVIs work with specific age groups only, or across Key Stages) may be influencing factors in experiential disparities. Another option could be to examine data from experienced QTVIs (>5 years’ professional experience) against that from relatively newly qualified QTVIs. Sample grouping would be organised around those who undertook the qualification prior to the 2016 new specification for the mandatory qualification, which occurred following the National College for Teaching and Leadership 2014 consultation into mandatory qualifications, and those who qualified since.
Criterion 1 of the specification that arose from this consultation stated the main objective of the specialist VI teachers should be to support the achievement of their pupils, defining ‘achievement’ to encompass both academic attainment and ‘in relation to, for example, physical, mental and emotional well-being’ (DfE, 2016, p. 6), thereby reinforcing the positioning of supporting mental health and well-being as a critical function of the QTVI. This study may have twofold utility – first, it may establish whether length of service enhances knowledge of interventions and practice to support emotional well-being /mental health of visually impaired children. Or it may suggest that those who have undertaken the MQVI in more recent times have clearer understandings around this facet of the QTVI role due to the increased importance of focus on mental health in the course content. This data may help to identify whether generic national or specific in-service training opportunities (or both) may be beneficial within the VI education sector.
Conclusion
The unique challenges to learning and participation in education associated with VI are well documented (Mason & McCall, 1997; McLinden & Douglas, 2013; McLinden et al., 2016) – as is the importance of equipping practitioners with the knowledge and skills to overcome them (McLinden et al., 2017, p. 569). This study has found supporting emotional well-being to be a particularly crucial yet complicated facet of the QTVI role. Participants identified lack of clarity of role boundaries and lack of practitioner confidence as key confounding issues. However, they also identified good practice as being embedded within the team and felt buoyed by opportunities to share experiences and ideas. This suggests that more networking within teams and across the VI Educational professional community is needed to ensure cohesion of the distal influences in the child’s macro-system (McLinden & McCracken, 2016, pp. 483–484). As Participant E succinctly put it, at the heart of the QTVI’s role is ‘giving our children the tools to move forward into adulthood, to be more emotionally literate and self-aware, and have that skillset there and ready’.