
Abstract
Research has shown that visual impairment may impact daily functioning, health, and well-being negatively for adults of all ages. Ex-service personnel (‘veterans’) too may be at risk of poor health and well-being outcomes associated with post-military life, and this may be exacerbated by the presence of visual impairment. Despite this, research considering the experience of blind veterans has been limited and has not yet assessed well-being for these individuals across a broad spectrum of life domains. Rather, it has highlighted poor mental health and psychological well-being in working-age visually impaired veterans. However, the experiences of older visually impaired veterans (who make up the majority of visually impaired veterans in the United Kingdom) have been poorly represented in the literature. This pilot study aimed to provide a preliminary assessment of holistic well-being in an adult sample of 97 UK blind veterans, predominantly composed of older age veterans (majority over 80 years). Cross-sectional well-being data were collected using a validated measure of well-being (the Well-Being Inventory [WBI]). Results suggest that members of Blind Veterans UK are functioning well and are satisfied across four life domains (vocation, finances, health, and social relationships). Lower health satisfaction was identified, particularly in blind veterans with comorbid mental health conditions. Results are discussed in relation to the older age of the sample, the limitations of face-to-face survey administration, and the applicability of the WBI finance domain in this age cohort. Recommendations are made for future research in this population.
Introduction
In the United Kingdom, it is estimated that around 2 million people are currently living with sight loss or blindness, a figure that is estimated to rise to around 4 million by 2050 as a result of an aging population (Pezzullo et al., 2018). The risk of visual impairment (VI) increases with age: the prevalence of sight loss in UK adults is shown to increase significantly from 11% to 53% between the ages of 75 and 90 years (Evans et al., 2002). Research has shown that VI may impact various aspects of daily life and psychological and psychosocial functioning (Garcia et al., 2017; Pinquart & Pfeiffer, 2011). For those who experience age-related VI, there is evidence of poorer quality of life, functional impairment in daily life, and high rates of depression and anxiety, compared to those who do not have sight loss (Han et al., 2019; Kempen et al., 2012; van der Aa et al., 2015; Zheng et al., 2017).
In the United Kingdom, nearly half of all ex-service personnel (‘veterans’) are over the age of 75 (Ministry of Defence, 2019). As such, age-related VI is likely to be prevalent in this population, as well as the adverse effects that are often associated with the experience of sight loss. Furthermore, veteran status may also be associated with negative psychological outcomes, with factors surrounding discharge, particularly early or unexpected discharge, identified as one risk factor for mental health difficulties among veterans (Holliday & Pedersen, 2017). UK veterans are significantly more likely to report self-harm and mental health conditions than non-veterans (Bergman et al., 2016, 2019; Jones et al., 2019). Research also suggests that loneliness and social isolation may occur following military service, reflecting factors such as losing touch with comrades, not feeling understood by the civilian community, and experiences of post-traumatic stress disorder (PTSD) and related symptomology (Solomon et al., 2015; SSAFA, 2016). Difficulties transferring skills to civilian employment and adapting one’s identity from the military to civilian context may further contribute to the challenges experienced by individuals following military service (Gordon et al., 2020).
While both VI and veteran status have been found to impact individuals in various aspects of life, particularly with regards to negative psychological outcomes, few studies have explored the experiences of blind veterans in the United Kingdom or internationally. A systematic review of the mental health of veterans with a physical impairment found a paucity of research looking specifically at mental health in relation to VI (Stevelink, Malcolm, Mason, et al., 2015). Subsequently, three papers have been published investigating psychological well-being in blind veterans (Stevelink & Fear, 2016; Stevelink, Malcolm, & Fear, 2015; Stevelink, Malcolm, Gill, & Fear, 2015). One of these papers reported relatively high rates of mental health problems and hazardous drinking in blind veterans (Stevelink, Malcolm, Gill, et al., 2015). An adverse impact on a number of daily life domains was also reported in relation to sight loss, resulting in financial hardship and strain on family relationships, loss of confidence, and a negative impact on identity (Stevelink, Malcolm, & Fear, 2015). Blind veterans have reported using a number of strategies to cope with sight loss, including both adaptive (e.g., using low visions aids or downwards social comparison, whereby individuals compare themselves to others who are worse off than themselves) and maladaptive behaviours (e.g., substance misuse, social withdrawal) (Stevelink & Fear, 2016; Stevelink, Malcolm, & Fear, 2015). Some of the results reported in studies of veterans with a VI reflect findings relating to the wider UK veteran population. For example, the military ethos of ‘cracking on’ has been reported by veterans who have VI (Stevelink & Fear, 2016; Stevelink, Malcolm, & Fear, 2015), which reflects attitudes held by the wider UK veteran population (Iversen et al., 2011). Similarly, increased hazardous drinking has been reported among younger compared to older UK service personnel and veterans, and in comparison with the general population (Fear et al., 2007; Murphy & Turgoose, 2019), which may reflect a broader military-wide drinking culture (Jones & Fear, 2011), rather than the impact of VI.
The abovementioned studies offer an indication of the psychological impact of VI on veterans, in addition to the potential challenges of being a veteran, the coping strategies these veterans might adopt, and the potential impact of challenges experienced across the wider veteran population. However, existing research relating to the experience of veterans with VI has a number of limitations. In particular, samples have been small (samples between 9 and 77) and have tended to exclude blind veterans over the age of 55. This exclusion may partly reflect the broader practical challenges of including older adults who have VI in research (Knechel, 2013; Trujillo Tanner et al., 2018). As such, research has excluded a large majority of the UK blind (and sighted) veteran population, most of whom are over the age of 75 years (Ministry of Defence, 2019). Representation of both working-age and older visually impaired veterans is important, given the different support needs that these groups may require. While vocational and interpersonal goals may be important to the rehabilitative services provided to working-age adults with a VI (Bell & Mino, 2013; Lindsay, 2011), strategies to maintain mobility to optimise social participation and health may be an important focus of rehabilitation for older adults with a VI (Rudman & Durdle, 2008).
This study
This article reports findings from a collaborative pilot study conducted by Anglia Ruskin University’s Veterans and Families Institute for Military Social Research (VFI) and Blind Veterans UK (BVUK), which gathered cross-sectional well-being data within a sample of BVUK members. The aim of this study was to provide an assessment of the holistic well-being of UK blind veterans, utilising a sample of BVUK members, which consisted of primarily older adults.
The concept of ‘well-being’ has historically been poorly defined in research (Dodge et al., 2012). A review of literature found 42 instruments designed to measure some aspect of well-being (Cooke et al., 2016), with huge variation in their length, their conceptualisation of well-being, and the constructs measured. The majority of the instruments measured constructs such as life satisfaction, positive affect, and positive relations, but did not consider broader life circumstances that are reflective of, and impact, well-being (Cooke et al., 2016). In response to the lack of a standardised measure of holistic well-being that can be used with military veterans, Vogt et al. (2019) developed the Well-Being Inventory (WBI), which has been rigorously validated in six phases with multiple cohorts of US military veterans (Vogt et al., 2019). This set of measures assesses individuals’ status, functioning, and satisfaction with regard to key aspects of their life (referred to as ‘domains’), including their health, vocation, finances, and social relationships. ‘Status’, as conceptualised in that framework, reflects objective circumstances within different life domains, including whether an individual has a health condition, is employed, has the financial resources necessary to meet their needs, and has social connections within their communities. ‘Functioning’ reflects one’s performance of key role functions within each life domain. For example, in the health domain, one’s engagement in health risk and protective behaviours is assessed. ‘Satisfaction’ reflects one’s subjective perception of how well things are going in each aspect of life, including one’s health, vocation, finances, and social relationships. Each component of well-being is assessed independently of the other components, thereby allowing for the possibility that individuals may simultaneously experience both high and low well-being in different aspects of their lives (e.g., positive social well-being despite poor health).
The WBI was chosen for use in this study for its ability to assess well-being across key life domains that contribute to an individual’s overall well-being. Through its consideration of status, functioning, and satisfaction across these key life domains, the WBI provides a comprehensive assessment of factors that set the stage for well-being, which facilitates the ability to pinpoint areas of both strength and vulnerability within the overall concept of well-being. In addition, the WBI was validated for use with military veterans, albeit in a US working-age cohort (average age 34.5 years) (Vogt et al., 2019). As such, this is the first study to employ the WBI in an older UK veteran sample. Particular attention was paid to the impact of modifying the survey administration mode to incorporate researcher-administration (rather than self-administration) to more effectively recruit participants from this older sample population.
Method
Participants
A total of 105 BVUK members were recruited to take part in this pilot study. The only inclusion criterion for participation was membership of BVUK, a charitable organisation that supports ex-service men and women who have sight loss. BVUK provide rehabilitation to its members through re-education, training, settlement, and welfare support. People are eligible to become members of BVUK if they have served in the UK Armed Forces as a regular or reservist, or served during World War II in the Merchant Navy, or Polish or Indian Forces under British Command. Individuals are eligible to become a member regardless of whether or not their sight loss is connected with their service in the Armed Forces, but they must meet specific sight loss criteria, based on Snellen visual acuity and assessment of visual fields. All members of BVUK have sight loss equivalent to a certification of ‘severe sight impairment’ (blindness).
Participants were recruited by the BVUK research team in person, via email, and via an advert in the BVUK monthly magazine (The Review). Assistance was provided by a member of BVUK operational staff in the recruitment of working-age members (under 65 years) via email. Members were provided with an information sheet explaining the study and were required to provide informed consent prior to taking part. Four participants chose not to share their data with the external research partner (Anglia Ruskin University’s VFI) for analysis, two requested for their data to be deleted, and two participants completed only a small number of WBI questions (the data were also deleted). As such, 97 cases were included in this analysis.
Data collection
While Vogt et al. (2018) suggest the use of the WBI as a self-report measure, the WBI was offered as both a self-administered and researcher-administered survey. This was viewed as an essential means of increasing accessibility of the research to older BVUK members (the average age of BVUK members is 85 years) and those members who did not feel comfortable accessing the survey online. There is a tendency for lower levels of internet use by older adults compared to younger adults (ONS, 2019), and recruitment of older adults is more likely through non-web-based methods than web-based methods (Corey et al., 2018). Furthermore, older adults with VI are less likely to engage with technology and the internet than those who do not have a VI (Gell et al., 2015). Research suggests that both younger and older adults with a VI may have insufficient online skills to use common internet applications (Van der Geest et al., 2014), as well as facing challenges relating to online navigation, the use of screen readers, and difficulty processing visual cues and large amounts of information (Okonji et al., 2015; Şimşek et al., 2010). Engagement with online survey research may, therefore, be limited by these factors.
Participants who chose to complete the survey online were sent an email link by a member of the BVUK research team. An accessible online survey format was developed for users with a VI, informed by feedback from a working group of BVUK members (n = 6) during a workshop conducted prior to this pilot project. This included adaptations to the colour scheme, font size and style, and layout of the questions. Participants who were unable to, or chose not to, complete the survey online were able to complete the survey over the telephone or face-to-face with a member of the BVUK research team. The majority (n = 72) completed the survey face-to-face, 16 participants completed the survey over the phone, and nine completed the survey online. The survey (which consisted of a registration/consent section, demographic questions, and the WBI) took around 1 hr to complete. As a result of face-to-face data collection and phone surveys, time of completion was higher than is normally expected with the WBI (15–20 min) (Vogt et al., 2018). The incidence of sight loss in the sample population may also have increased time of completion for those who self-administered the survey online; use of screen reading equipment, or low levels of vision, may mean that an individual requires additional time to access and navigate through online surveys and other online materials (Kaczmirek & Wolff, 2007; Sahib et al., 2012).
Measures
Demographic information was collected for each participant, including age, gender, ethnicity, nationality, marital status, and number of dependents. Military service information included type of service (full-time regular or reservist), service branch (Army, Royal Navy, Royal Marines, Royal Air Force, or Merchant Navy), and rank on discharge (commissioned or other ranks). Participants were also asked about the reason for their sight loss (e.g., during service, post-service combat or non-combat related, age-related or non-age-related), time since sight loss diagnosis, and length of their BVUK membership.
Well-being was measured using an anglicised version of the WBI (Vogt et al., 2019) to assess status, functioning, and satisfaction in four key life domains. It consists of four domain scales, including a combination of multi-code and single-code categorical questions and Likert-type scale questions to address well-being in relation to the following areas:
Vocation – includes labour force participation, paid employment, full vs. part-time employment, and full-time involvement in unpaid vocations, including volunteer work, and care-giving/ homemaking, and education.
Finances – includes current financial stability and financial preparedness.
Health – includes ongoing physical or mental health illnesses and/or disabilities.
Social relationships – includes the three subdomains of intimate relationships, parenting, and broader social relationships with friends, relatives, and the wider community.
Within each domain status, functioning and satisfaction measures can be derived. Status measures address objective life circumstances within each life domain, such as employment status and level of social engagement. Functioning measures assess the extent to which individuals are able to perform well within each of the above life domains. The satisfaction measure addresses individuals’ subjective experiences of satisfaction with regard to each of the above life domains. Throughout the inventory, respondents are instructed to select a single response to statements using a 5-point Likert-type type response format (e.g., 1 = Never to 5 = Most or all of the time; 1 = Very dissatisfied to 5 = Very satisfied). Functioning and satisfaction scores are calculated by averaging item scores to provide a score out of 5, with 5 being the highest level of functioning and satisfaction.
Data analysis
Data were inputted into SPSS for analysis. Descriptive statistics, including frequencies and percentages, were used to analyse demographic and military service information, and the WBI status responses. Mean scores are reported for the functioning and satisfaction measures of the WBI. Given the need to report findings with real-life application (to increase understanding of BVUK member well-being to tailor services and support to meet the well-being needs of members) additional interpretation of results was provided by grouping responses into two categories, in accordance with Vogt et al. (2020): those in the highest third of the response continuum, corresponding to average responses of ‘often or always’ functioning well or being ‘somewhat or very satisfied’ (scores ranging from 3.668 to 5), and those in the bottom two thirds of the response continuum, reflecting average responses of ‘rarely to sometimes’ functioning well or ‘not satisfied’ on average (scores ranging from 1 to 3.667). These categories are useful in providing a meaningful interpretation of results to practitioners, with an indication of how well an individual is functioning, or how satisfied they are, with respect to different life domains.
Results
Participant characteristics
Table 1 provides the participant characteristics in full (n = 97). The majority of the sample were male (93.8%), white British (95.9%), and over 80 years of age (55.7%). A quarter (25.8%) of the sample were of working-age (all of whom were between 40 and 64 years). The most common Service Branch was the Army (55.7%). The majority of participants had been full-time regular personnel (87.6%, including Conscription/National Service) and were non-commissioned on discharge (89.7%). The most common length of time that members had been registered with BVUK was between 6 months and 5 years (40.2%). The most common reason reported for sight loss was an age-related condition which occurred post-service (50.5%). The average time since VI diagnosis was 12.3 years (ranging from 0.8 to 71.7 years).
Participant characteristics for the sample (n = 97).
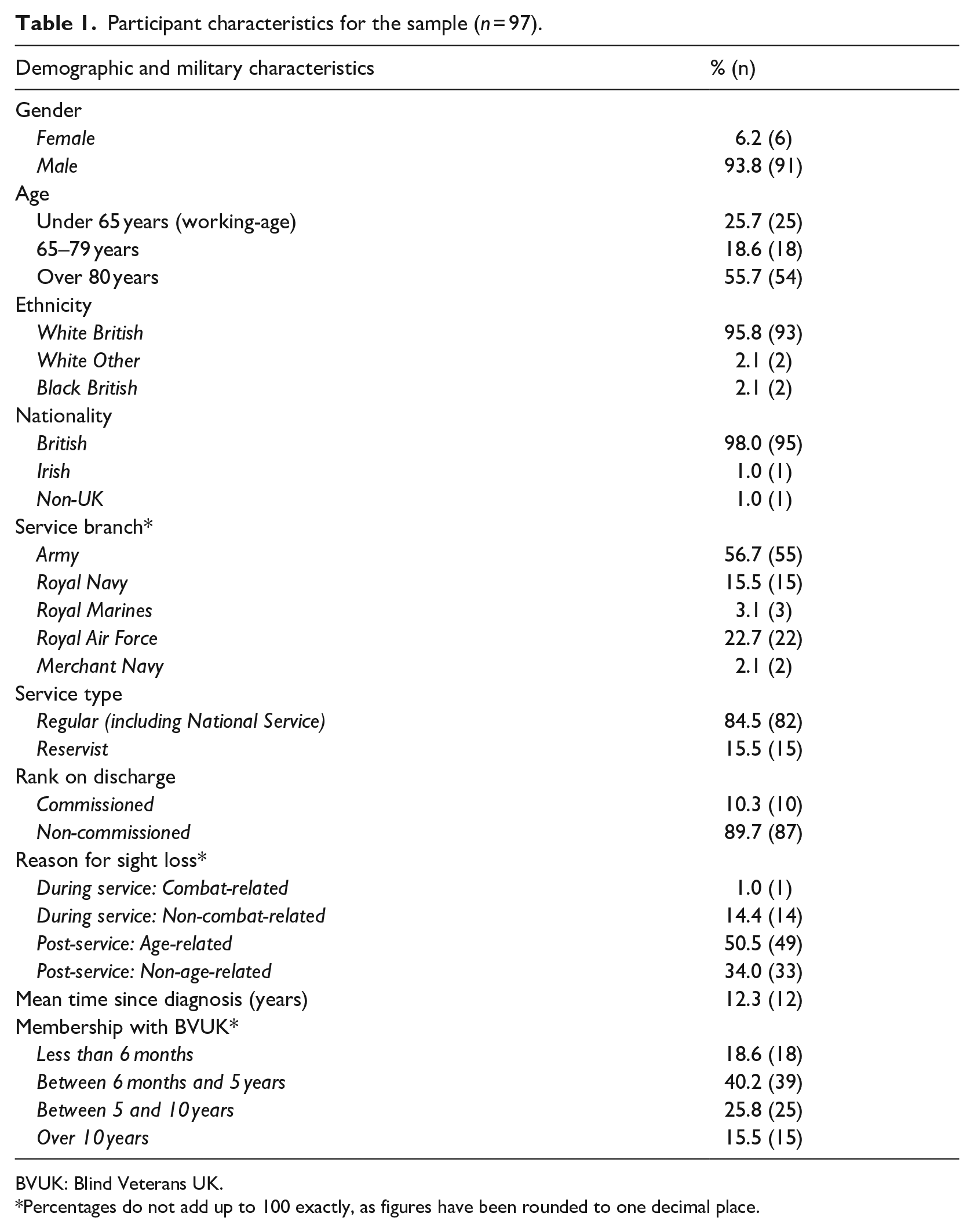
BVUK: Blind Veterans UK.*Percentages do not add up to 100 exactly, as figures have been rounded to one decimal place.
Participant well-being
Mean scores for the WBI functioning and satisfaction measures were above 3.668 for the majority of the domains (see Figure 1). This suggests that overall, participants in the sample reported that they were functioning well in the majority of domains and were satisfied with most areas of their lives. Table 2 shows the categorical results for WBI status, functioning, and satisfaction.
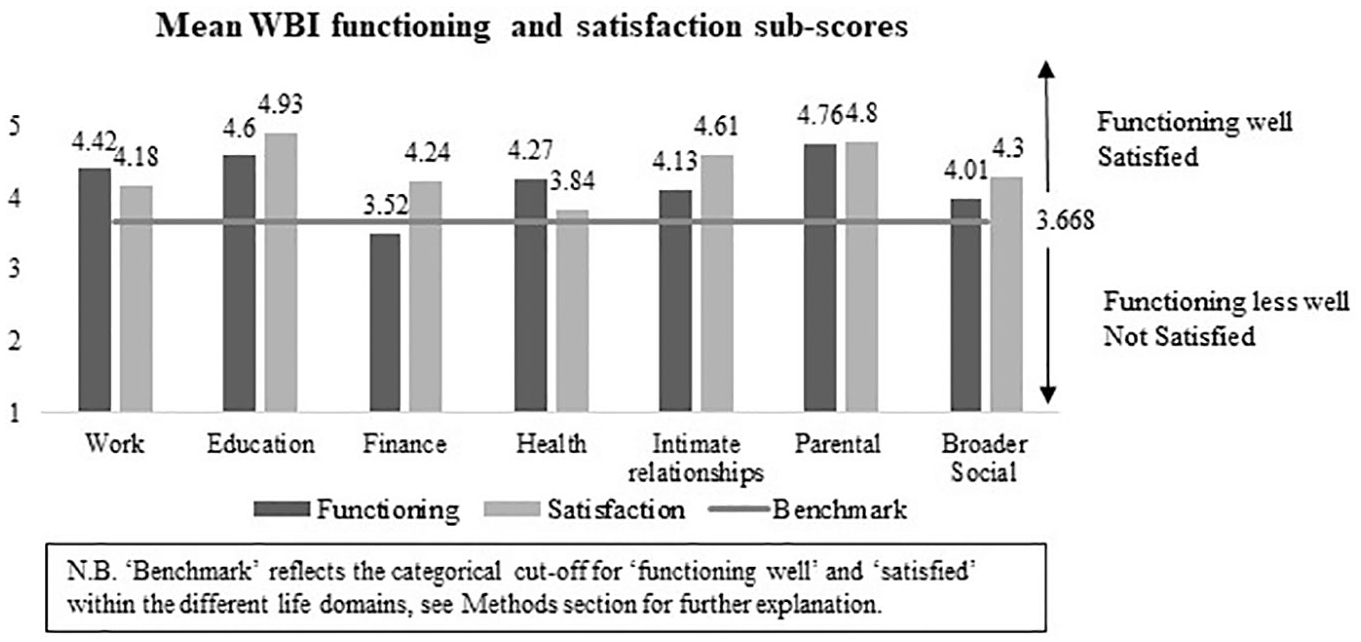
Mean Well-Being Inventory functioning and satisfaction sub-scores across the sample (n = 97).
Proportional results for WBI domain status, functioning, and satisfaction.
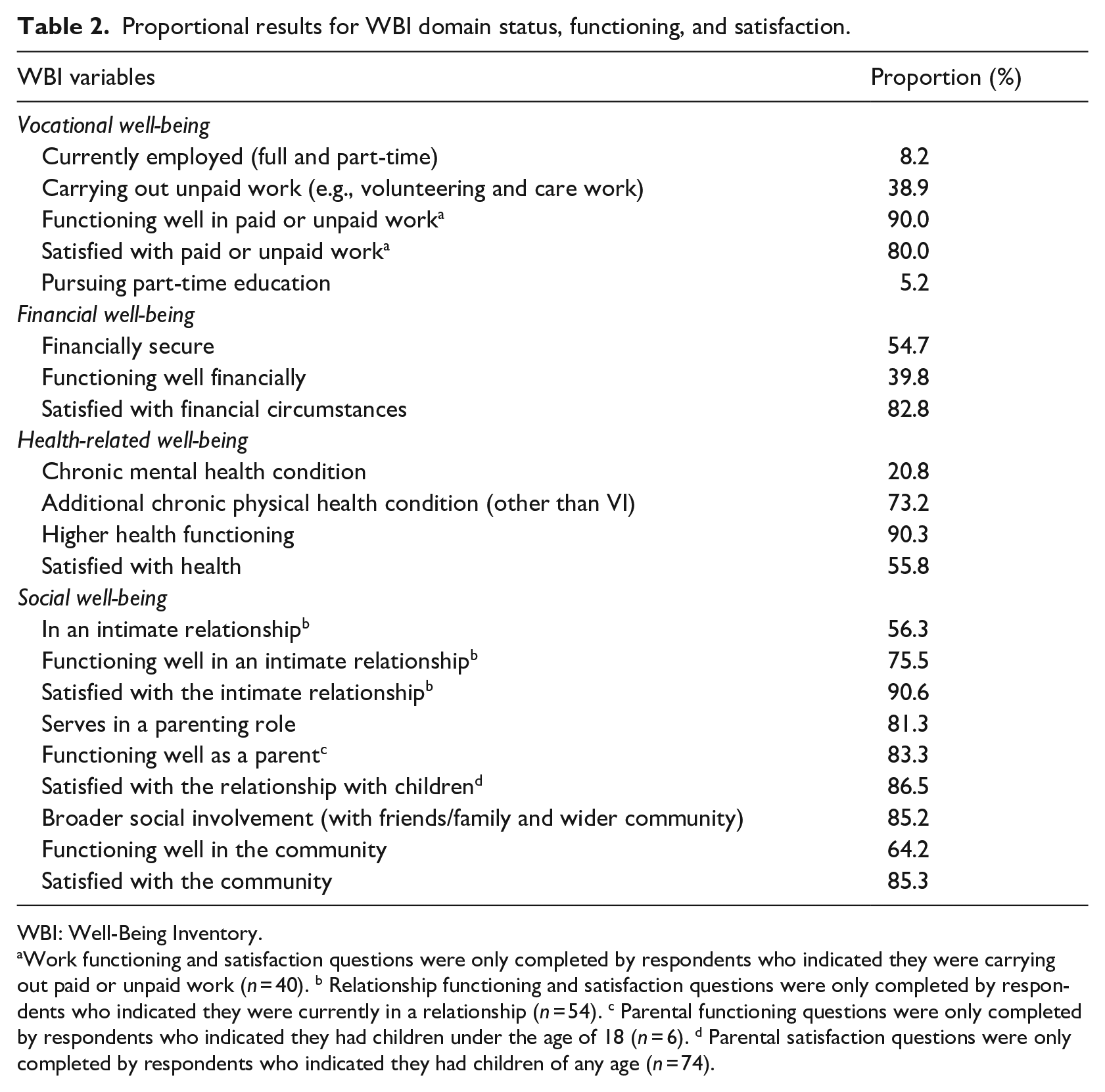
WBI: Well-Being Inventory.
Work functioning and satisfaction questions were only completed by respondents who indicated they were carrying out paid or unpaid work (n = 40). b Relationship functioning and satisfaction questions were only completed by respondents who indicated they were currently in a relationship (n = 54). c Parental functioning questions were only completed by respondents who indicated they had children under the age of 18 (n = 6). d Parental satisfaction questions were only completed by respondents who indicated they had children of any age (n = 74).
Vocation (work and education)
Mean scores for work functioning and satisfaction are shown in Figure 1. The large majority of respondents reported functioning well (90%) and being satisfied (80%) with their paid or unpaid work (see Table 2). The majority of participants were unemployed and not looking for work (87.7%), with just a small proportion in paid employment (8.2%), or unemployed but looking for work (4.1%). Within working-age participants (i.e., under the age of 65 years; n = 25), 24% were in paid employment. The predominant reason why participants were unemployed and not looking for work was retirement from the workforce (81.2%), followed by an ongoing physical or mental illness (14.1%). Thirty-nine percent of the sample were carrying out unpaid work, the majority of which was volunteer work (97.3%). A small proportion of respondents were pursuing part-time education (5.2%; educational functioning and satisfaction sub-scores were not included due to the small proportion pursuing education).
Finances
Mean scores for financial functioning and satisfaction are shown in Figure 1. Less than half (39.8%) of respondents reported functioning well financially, but the majority (82.8%) were satisfied with their financial circumstances, and over half were financially ‘secure’ (54.7%). Financial security was calculated by assessing responses to the WBI questions that ask about ability to meet immediate financial needs (i.e., ability to cover necessary expenses, current debt, and housing stability) and financial preparedness for the future (i.e., current savings, insurance, and pension fund; for full scoring instructions, see Vogt el at., 2018). A third of participants were considered financially ‘at risk’ (33.7%), meaning they indicated that they were not financially prepared for the future, while 11.6% of the sample were considered financially ‘problematic’, meaning they indicated that they were unable to meet all immediate financial needs.
During data collection, it became clear that some of the questions in the financial domain were of limited relevance to older (non-working-age) veterans. Questions which asked respondents about the extent to which they were saving for retirement were not relevant for 71% of the sample, who were already retired and drawing their pension. Retired participants skipped these questions or gave the most appropriate answer (e.g., ‘Yes’, if they had saved for retirement in the past, or ‘No’, if they had never saved, or if they were no longer saving for retirement). Answering the financial functioning questions in this way may have had implications for survey scoring. Retired respondents who answered ‘Never’ when asked how often they had paid money into a pension fund, would have a reduced financial functioning score.
An additional challenge in the financial domain was that many of the questions were difficult to answer for those whose finances were managed by a spouse or another person (i.e., with power of attorney). Several participants were unable to provide an answer on items relating to household income, savings, and spending behaviours, while others reported that they were only able to offer an approximate response or selected ‘No’ if the question was not of relevance to them. As highlighted above, providing a negative answer impacted a participant’s financial functioning score. For these reasons, we present the findings for the finance domain separately for working-age and non-working-age veterans in Table 3.
Proportional results for financial status, functioning, and satisfaction stratified by age group.
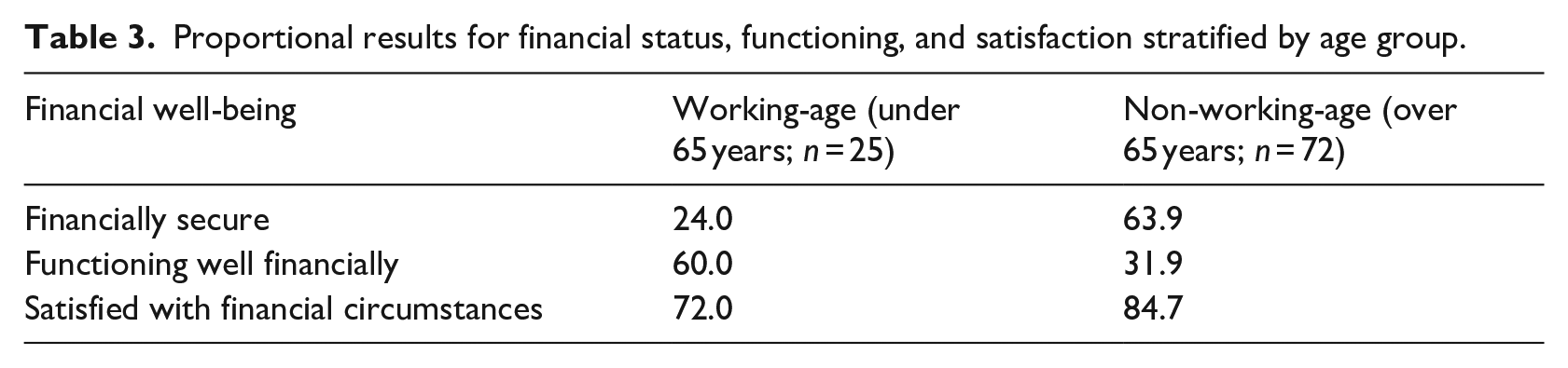
Table 3 indicates a disparity between the financial status, functioning, and satisfaction scores for each of these two groups: only 31.9% of non-working-age veterans appear to be functioning well, despite the large majority reporting they were satisfied with their finances (84.7%) and financially secure (63.9%). This may reflect the impact of the difficulties experienced in answering the questions related to managing finances and saving for retirement in the financial functioning section. Indeed, the majority of non-working-age veterans reported that they ‘Never’ followed a budget (64.3%) or kept a record of their finances (54.3%), and almost all respondents in this group (95.7%) reported that they ‘Never’ contributed part of their salary to a pension fund.
The results for working-age veterans suggest that despite the fact that the majority reported functioning well (60%) and being satisfied with their finances (72%), only 24% were financially secure. The majority of this group were considered financially ‘at risk’ (60%), and 16% were considered financially ‘problematic’. As shown in Table 3, responses from this group appeared to reduce the overall proportion of participants considered financially ‘secure’ (54.7%), with many working-age respondents reporting being financially unprepared for the future: a higher proportion of working-age veterans, compared to non-working-age veterans, reported that they do not have insurance (working-age: 28%; non-working-age: 8.5%) or 3 months of income set aside (working age: 44%; non-working age: 9.9%) to cover an unexpected financial event, and 60% of working-age veterans were not putting aside money for retirement.
Health
Mean scores for health functioning and satisfaction are shown in Figure 1. The large majority of respondents reported high health functioning (90.3%), indicating that respondents were looking after their health by avoiding risky health behaviours such as excess drinking or smoking and by eating well and exercising as much as their health status and age permitted. However, 44.2% of the sample reported that they were not satisfied with their overall health. Responses to individual questions within this domain indicated that a third (33.7%) reported being dissatisfied with their physical health and a fifth (22.3%) were dissatisfied with their mental health. A small number (8.4%) reported dissatisfaction with their health care. Comorbidity was high in the sample, with the majority (78.4%) of participants reporting a chronic mental or physical health condition in addition to their VI. On average, participants reported two additional chronic health conditions (ranging from 0 to 9). Lower levels of health satisfaction were particularly apparent in the 20.8% of participants who reported having a mental health condition; just 25% of these individuals were satisfied with their health, compared to 64% of those with a physical health condition only. No health conditions associated with substance misuse were reported in this sample.
Social relationships
Mean scores for social relationship functioning and satisfaction are shown in Figure 1. Over half of participants reported that they were currently in an intimate relationship (56.3%), and most of these individuals reported that they were functioning well (75.5%) and satisfied with their relationship (90.6%). A small proportion of respondents had children below the age of 18 (6.2%), and the majority of these individuals were functioning well in their parenting role (83.3%). Of those that reported having children of any age (81.3%), 86.5% were satisfied with their relationship with their children. The majority of participants reported involvement with both the community and family/friends in the past 3 months (85.2%), 13.7% reported involvement with either their community or family/friends, and just 1.1% reported no social involvement at all. This high level of community involvement was reflected in community functioning and satisfaction sub-scores, with the majority of respondents functioning well and satisfied with their broader community involvement (64.2% and 85.3%, respectively).
Discussion
This pilot study investigated well-being in a sample of 97 BVUK members. The age profile of the sample broadly reflected that of the BVUK membership (Blind Veterans UK, 2019), and the UK veteran population as a whole (Ministry of Defence, 2019), with the majority of participants being over the age of 75 years. The majority of the sample were white British males and had previously served in the Army. Similarly, the sample offers a good representation of the wider community of individuals who have a VI, with the most commonly reported reason for sight loss being an age-related condition; in the United Kingdom, age-related macular degeneration (AMD) is the leading of cause of sight loss (Quartilho et al., 2016).
The WBI results indicated that members of BVUK report functioning well and being satisfied across four life domains (vocation, finances, health, and social relationships). Average scores of at least 3.668 (i.e., scoring in the top third of the 1-5 continuum) indicated a high level of functioning and satisfaction, with the exception of financial functioning and health satisfaction. Scores for these two measures were lower; the majority of participants functioned less well financially (60.2%), and just under half were not satisfied with their health (45.4%).
Financial hardship has previously been associated with VI in blind veterans (Stevelink, Malcolm, & Fear, 2015). Experiences of financial hardship, which may reflect the low household income and the additional costs of living often associated with having a VI, are typical among both older and working-age adults with a VI (Hill et al., 2017). However, lower financial functioning in this sample appears to have been impacted by the older age of the sample (over half of participants were >80 years). Some participants, who were surveyed face-to-face, reported that they no longer managed their own finances. Some of these individuals indicated that they ‘Never compared prices’ or ‘Never put money into a savings account’ because such activities are carried out by someone else on their behalf. Similarly, a small number indicated that they did not have to monitor their spending or follow a budget because they were financially comfortable. Furthermore, a number of participants were retired, creating difficulties when responding to questions that asked if they were putting money aside for retirement. Difficulties in responding to these questions lowered overall scores for this domain, which may partly explain why financial functioning appears to be higher in those of working-age; 60.0% of those under 65 years of age were functioning well financially, compared to just 31.9% in those over the age of 65. Conversely, it is respondents of working-age who appear to be driving down the proportion of participants who report being financially ‘secure’ (working age: 24%; non-working age: 63.9%). The majority of this group were considered financially ‘at risk’ (60%), suggesting that they were able to meet their immediate financial needs, but were not financially prepared for the future. This appears to be driven largely by the fact that 60% of this group were not currently putting money aside for retirement. This finding warrants further investigation; however, results from this group should be interpreted with caution because of the small sample size (n = 25).
Lower health satisfaction may be expected in this population, all of whom had a VI. VI and other chronic physical health conditions have been associated with poor health-related well-being and quality of life in older adults with a VI (Chia et al., 2004; Langelaan et al., 2007; Siira et al., 2019). In addition, many participants had a comorbid physical or mental health condition. The presence of multiple health conditions has been reported as a particular challenge to health management in older adults with sight loss (Burton et al., 2016) and appears to have contributed to lower health satisfaction in this sample. A fifth of this sample reported that they had a comorbid mental health condition. This is considerably higher than that reported for older adults (75 +) in the general population, in which 9% report a common mental health disorder (McManus et al., 2016). However, there was some anecdotal evidence from the face-to-face and phone interviews that mental health conditions may have been underreported, with some participants mentioning conditions later in the survey that had not been identified in the health section of the survey. Just 25% of those who had a comorbid mental health condition were satisfied with their health, compared to 64% of those with a comorbid physical health condition alone. This suggests that those who have a comorbid mental health condition may be at greater risk of poor health-related well-being than those with a comorbid physical health condition alone. Encouragingly, the health functioning score indicated that despite lower satisfaction than in other domains, and high proportions of comorbidity, BVUK members were generally looking after their health by regularly engaging in behaviours that support good health and avoiding risky health behaviours. Unlike the high levels of hazardous drinking reported in previous work with members of BVUK (Stevelink, Malcolm, Gill, & Fear, 2015), no problems with drugs or alcohol were reported in this study. This may be due to the older age of the veterans in this sample, as hazardous drinking tends to be associated with younger veterans and service personnel (Fear et al., 2007).
Limitations
Some limitations of this study must be acknowledged. First, this was a pilot study with a small sample size and no comparator group, meaning that comparisons of well-being with ex-service personnel without VI, or civilians with VI, were not possible on this occasion. Furthermore, due to the nature of the sample (i.e., older adults), the sample sizes for particular domains of the WBI, particularly parental functioning (relating to children under the age of 18) and work, were very small.
Second, it should be noted that during data collection, some limitations were identified in relation to the applicability of the WBI to the older members of the sample population, particularly with regards to questions addressing participants’ financial outcomes (i.e., saving for retirement and managing finances). Third, there were some challenges associated with the way that data were collected. It should be noted that the WBI was designed as a self-report measure, and self-administration is preferred to ensure privacy and confidentiality when responding to sensitive items (Vogt et al., 2018). However, due to the nature of the sample (i.e., older veterans with a VI), the majority of the data were collected face-to-face and measures were administered by a member of the BVUK research team. This may have increased the likelihood of a desirability bias in the answers given and an inflation of well-being scores. In light of this, it will be important for any future research to validate the researcher-administrated version of the WBI in this population.
Finally, the nature of the sample itself should be considered in the context of the wider population of blind veterans in the United Kingdom. A majority of the sample were currently in receipt of significant support from BVUK, but because data were not collected regarding the level of support received by each participant, the impact of engagement with BVUK support services and activities cannot be explored.
Conclusion and future directions
Overall, results from this pilot study indicate that BVUK members report a good level of functioning and satisfaction across the life domains explored by the WBI (vocation, finance, health, and social relationships). VI may typically be associated with negative psychological impacts and a restriction on daily living and social activities (Han et al., 2019; Kempen et al., 2012; van der Aa et al., 2015; Zheng et al., 2017), but results suggest that BVUK members involved in this study may maintain a high level of well-being in these domains. Lower health satisfaction was identified, particularly in blind veterans with comorbid mental health conditions. This finding is of importance and suggests that additional mental health conditions, or difficulties associated with mental health, may impact overall health-related well-being to a higher degree than additional physical health conditions. Given the impact that mental health has been found to have on general health and well-being in non-veteran populations (Chaudhury et al., 2018; Connell et al., 2012; World Health Organization, 2004), this finding warrants further investigation in this cohort. Furthermore, this study identified issues with the applicability of the WBI finance questions for older veterans, and a possible need to support working-age blind veterans in preparing financially for the future. While this study provides a preliminary assessment of well-being in UK blind veterans, future research would benefit from a larger sample size, comparison groups of both non-VI ex-service personnel and VI civilians, and confirmation of researcher-administered survey results based on self-administration of the survey (e.g., interactive accessible computer survey). These efforts would enable a more in-depth exploration of the strengths and vulnerabilities in these populations and provide opportunities to identify how support services for VI veterans, and the wider veteran community, might best be targeted to meet their well-being needs.