
Abstract
Impaired vision often results in restrictions across diverse key indicators of successful aging. However, little is known about how impaired vision affects the long-term trajectories of these outcomes, whether effects are moderated by age, and whether psychosocial resources beyond well-being such as subjective age views are also affected by vision loss. We analyzed how self-reported vision problems as a time-varying predictor are related to long-term changes in health and cognitive ability (functional health, number of chronic diseases, self-rated health, information processing speed), well-being (life satisfaction, positive and negative affect, depressive symptoms, loneliness), and subjective age views (subjective age; aging-related cognitions: social loss, physical decline, continuous growth). Our sample was derived from the German Ageing Survey, comprising 6,378 individuals (40–89 years) who provided up to four observations over a 9-year period. Controlling for gender, age, education, and functional as well as self-rated health, we observed that both on a between- and a within-person level, indicators of successful aging were consistently less favorable among individuals with more vision problems. Associations between vision problems and functional health became stronger with advancing age. In contrast, with increasing age, vision problems were less closely associated with change in several indicators of psychosocial functioning. Our findings suggest that self-reported visual impairment is associated with restrictions across a broad range of developmental domains. Some detrimental effects of vision problems are augmented in later life, whereas several effects on well-being and subjective age views were attenuated with advancing age, which might indicate processes of late-life adaptation to vision loss.
Keywords
In this study, we will investigate the role of self-reported vision problems as a predictor of a broad set of developmental outcomes across a long-term 9-year observational interval. We focus on the outcome dimensions of health and cognitive ability, well-being, and subjective age views. This comprehensive set of potential outcomes of visual impairment has, to our knowledge, not yet been included in one single longitudinal study. Vision problems will be specified as a time-varying predictor, so that their between-person as well as within-person, time-varying associations with all outcomes can be investigated and compared. That is, beyond examining the overall effect of vision problems on trajectories of successful aging outcomes, we will be able to investigate the role of measurement occasion–specific changes in vision problems for these outcomes, thus taking a more dynamic and process-related perspective. Moreover, we will examine the potentially moderating role of age for the predictive effects of self-reported vision problems on the various outcomes based on a large age-heterogeneous sample comprising middle-aged and older adults.
Consequences of impaired vision
The consequences of visual impairments affect different developmental domains (Heyl & Wahl, 2014; Swenor, Lee, et al., 2019; Wahl, 2013; Zimdars et al., 2012). Regarding health and cognitive ability, individuals with impaired vision reveal a steeper functional health decline compared to individuals with intact vision (Lin et al., 2004), and this decline results in increasing difficulties with everyday tasks such as stair climbing or use of public transportation. Moreover, among those with self-reported poor vision or with age-related eye diseases, certain chronic diseases such as heart disease or stroke seem to be more common than among individuals with intact vision (Crews et al., 2017; Y. Li et al., 2011; Yu & Liljas, 2019). Impaired vision is also a prospective predictor of poorer subsequent self-rated health (Yu & Liljas, 2019). In addition, impaired visual ability is related to steeper decline in cognitive ability (Swenor, Wang, et al., 2019; Zheng et al., 2018).
Well-being is another domain that is, via multiple pathways (Brown & Barrett, 2011), negatively affected by the experience of vision loss (Pinquart & Pfeiffer, 2011). Individuals with impaired vision or age-related eye diseases are less satisfied with their lives, report lower positive and higher negative affect, greater loneliness as well as less social participation and poorer quality of their social relationships (e.g., Brunes et al., 2019; Hajek et al., 2020; La Grow et al., 2015; Mick et al., 2018). Poorer objective and subjective vision is also a prospective predictor of subsequent well-being (Xiang et al., 2019), particularly of higher depressive symptoms (Frank et al., 2019; Schilling et al., 2013; Yu & Liljas, 2019).
Finally, only four studies (Jang et al., 2004; Kim et al., 2012; Nakagawa et al., 2018; Schroyen et al., 2020) have so far investigated the association between vision and subjective age views, which describe “expectations, experiences or feelings about the process of aging” (Faudzi et al., 2019, p. 550). All four studies were based on cross-sectional data, and they have produced mixed findings. It is thus unclear how vision and subjective age views are interrelated when considered longitudinally.
Vision impairment and successful aging: the role of chronological age
Whether vision loss has more or less severe consequences with advancing age may depend on the specific outcome domain in question. First, health and cognitive abilities usually decline with advancing age (Baltes & Smith, 2003; Schaie, 2013), so that the occurrence of vision loss in later life might be an additional burden that increases this age-related vulnerability. In contrast, younger adults might have more resources available to compensate for the detrimental impact of vision loss on health-related outcomes. Several studies indeed found that with increasing age, the association between sensory and cognitive functions becomes stronger (e.g., Baltes & Lindenberger, 1997; Tay et al., 2006). In contrast, the moderating role of age in the relationship between vision and health has been less extensively investigated so far.
Second, with regard to well-being, vision loss gets more common with age (Correia et al., 2016; Keeffe, 2019), thus corresponding to an “on-time” experience at older ages. Individuals who are older might thus have already anticipated the worsening of their visual acuity to some extent. This anticipation might in turn facilitate adaptation to such an impairment and prevent or at least buffer declines in well-being. Several studies indeed reported that the negative association between vision and well-being is smaller among older compared to younger individuals (Boerner, 2004; Brunes et al., 2019; Good et al., 2008). However, these studies all relied on a cross-sectional study design so that it is still unclear if such a moderating role of chronological age can also be observed from a dynamic perspective, when changes in both vision and well-being are considered.
Third, according to stereotype embodiment theory (Levy, 2009), subjective age views grow more important and more salient when individuals enter old age and thus become targets of their own stereotypes about older adults. This seems to result in closer associations between subjective age views and health with advancing age (Bergland et al., 2014; Brothers et al., 2015; Levy et al., 2016; Miche et al., 2014). However, to our knowledge, potential age moderation effects on the association between vision loss and subjective age views have not been investigated so far.
Finally, these age moderation effects may vary in size and direction according to the temporal dynamics of visual impairment. The theory of strength and vulnerability integration (SAVI) predicts that
When older adults avoid or reduce exposure to emotional distress, they often respond better than younger adults; when they experience high levels of sustained emotional arousal, however, age-related advantages in emotional well-being are attenuated, and older adults are hypothesized to have greater difficulties returning to homeostasis. (Charles, 2010, p. 1068)
With regard to vision loss, this could mean that older adults, that is, individuals who are 60 years old or older, might be better able than adults in midlife (40–60 years) to adjust to a condition of constant vision loss and to prevent decline in well-being and other outcomes. In contrast, temporary deteriorations in vision that cause high emotional distress and fears (e.g., of going blind) and that require rapid short-term adjustments might affect older adults’ well-being to a larger extent compared to middle-aged adults.
Hypotheses
Our expectations are as follows:
More severe self-reported vision problems are associated with poorer health and cognitive ability, lower well-being, and less favorable subjective age views, as well as with less favorable 9-year trajectories in these outcomes. Additionally, on a within-person, time-varying level, we expect that on measurement occasions when individuals encounter more severe problems with vision, they score lower on health and well-being and report less favorable subjective age views.
Between- and within-person associations between self-reported vision problems and developmental outcomes might vary by chronological age. Given that evidence to date is scarce – particularly with regard to the role of age for longitudinal, time-varying associations between vision problems and these outcomes – we will address this research question in an exploratory way without stating specific a-priori expectations.
Method
Study population and sample description
Data of the German Ageing Survey, a cohort-sequential study comprising German community-dwelling adults aged 40 years and older at the time of their first study participation (Vogel et al., 2020), were used. Six measurement occasions (T1: 1996, T2: 2002, T3: 2008, T4: 2011, T5: 2014, T6: 2017) have been completed so far. At each measurement occasion (with the exception of 2011 and 2017), a new sample was drawn based on national probability sampling. Samples were systematically stratified by age, gender, and region of residence (West or East Germany). If they gave their consent, study participants were re-interviewed at the subsequent measurement occasions.
For the present analyses, four measurement occasions (2008, 2011, 2014, 2017) were included. Measurement occasions prior to 2008 were not included because the format to assess vision problems was different at these earlier measurement occasions.
Our study sample consists of n = 6,378 individuals who were aged between 40 and 89 years in 2008 and who provided at least one valid observation on all included outcomes and predictors 1 (mean number of observations per individual = 2.58, SD = 1.26). The number of individuals providing data at the measurement occasions 2011, 2014, and 2017 was 3,799, 3,440, and 2,859, respectively. A sample description is provided in Table 1.
Sample description (baseline, N = 6,378).
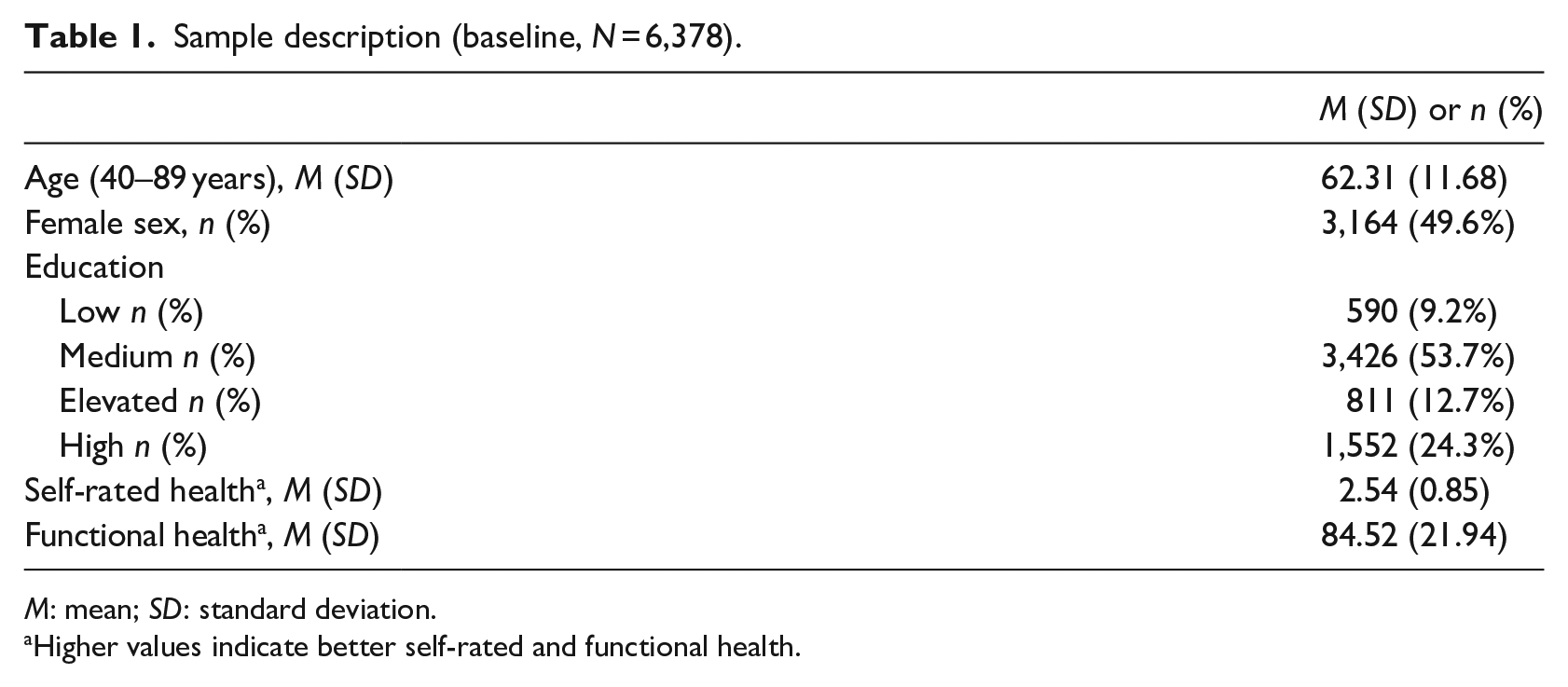
M: mean; SD: standard deviation.
Higher values indicate better self-rated and functional health.
There was a relatively large proportion (31.2%) of individuals who had only one study participation and thus provided only one observation, but whose data are nevertheless important for the estimation of effects at baseline. To investigate the extent of sample selectivity due to selective dropout, we compared the subsample of individuals with only one observation with those who had at least two study participations. Notably, the effect sizes of all differences were in a range between d = 0.04 (number of chronic diseases) and d = 0.34 (education), thus corresponding – according to common classifications (e.g., Cohen, 1992) – to small effects. The distribution of gender was also comparable for both subsamples: 47.9% of participants were female in the sample with two and more observations and 50.4% of individuals were female in the sample of individuals with only one observation, χ2 (1) = 3.49, p = .06, Φ = .03.
Measures
Self-reported problems with vision
Study participants rated their difficulties with vision based on two items covering near and distance vision (“Do you have problems reading the newspaper [even when using a vision aid]?” and “Do you have problems recognizing familiar persons on the street [even when using a vision aid]?”). The response format was a 4-point Likert-type scale ranging from 1 (“no difficulties”) to 4 (“impossible”).
To obtain a composite measure of overall vision problems, comprising both near and distance vision, and to achieve a higher reliability of the measure as well as better model parsimony for the analyses, we aggregated both vision items into one measure by averaging them. We also transformed the original scale range (1–4) to 0–3.
Health and cognitive ability
Four indicators of health and cognitive ability were included. Functional health was measured by the physical functioning subscale of the 36-Item Short Form Survey (SF-36) assessment instrument (Bullinger & Kirchberger, 1998). Participants indicated the extent to which they were limited (“limited a lot,” “limited a little,” or “not limited at all”) with regard to 10 typical everyday activities (e.g., walking several blocks). Answers were summed and transformed according to the manual, resulting in a sum score with a range from 0 to 100. Higher values indicate better functional health.
Number of chronic diseases was based on a list comprising 11 chronic conditions (e.g., diabetes, cancer, cardiovascular diseases). For each participant, a sum score of self-reported chronic diseases was computed.
A single-item question (“How would you rate your current health?”) was used to assess self-rated health. The response format ranged from 1 (“very good”) to 5 (“very poor”). Responses were recoded so that higher scores indicate better self-rated health.
The assessment of information processing speed, which is a key marker of cognitive functioning (Finkel et al., 2007; Lindenberger et al., 1993; Salthouse, 1996), was based on the digit symbol substitution test, a subtest of the Wechsler Adult Intelligence Scale (WAIS-R; Tewes, 1991). Higher test scores indicate higher information processing speed.
Well-being
Given the multidimensionality of well-being (Diener et al., 1999; Headey et al., 1985; Ryff et al., 2006), multiple indicators were included. Life satisfaction was measured based on the Satisfaction with Life Scale (SWLS; Diener et al., 1985) comprising five items. Higher scores indicate a higher life satisfaction (Cronbach’s α 2008–2017: .85, .84, .85, .84).
Positive and negative affect were assessed by the Positive and Negative Affect Schedule (PANAS; Watson et al., 1988). The positive affect and negative affect subscales each contain 10 adjectives describing positive (e.g., excited, inspired) versus negative (e.g., upset, hostile, nervous) emotions. Respondents indicated how often they had experienced each of these emotions within the past months. Individuals’ mean scores on both subscales were computed, with higher mean scores indicating more positive/negative affect (Cronbach’s α 2008–2017 for positive affect: .87, .86, .87, .86; Cronbach’s α 2008–2017 for negative affect: .87, .86, .86, .85).
Depressive symptoms were assessed based on a 15-item German adaptation (Hautzinger & Bailer, 1993) of the Center for Epidemiological Studies Depression Scale (Radloff, 1977). Participants were asked how often they had experienced 15 different depressive symptoms during the last week (e.g., “I felt sad,” “My sleep was restless”). Higher sum scores indicate more or more frequent depressive symptoms (Cronbach’s α 2008–2017: .86, .86, .85, .85).
Finally, loneliness was assessed by a modified version of the De Jong Gierveld Loneliness Scale (Gierveld & Tilburg, 2006). The six items of the scale (e.g., “There are enough people I feel close to.”) were summed up, with a higher sum score indicating greater loneliness (Cronbach’s α 2008–2017: .84, .81, .84, .84).
Subjective age views
Two indicators of subjective age views were included. Subjective age was assessed based on a single-item question, by asking individuals “How old do you feel?.” To facilitate the interpretation of subjective age, we computed a proportional discrepancy score between felt age and chronological age (subjective age = [felt age − chronological age] / chronological age; Rubin & Berntsen, 2006). 2
Multidimensional aging-related cognitions (Steverink et al., 2001; Wurm et al., 2007) were assessed based on three subscales, namely, social loss (e.g., “Aging means to me that I am less needed”; Cronbach’s α 2008–2017: .75, .73, .73, .72), physical decline (e.g., “Aging means to me that I am less energetic and fit”; Cronbach’s α 2008–2017: .77, .79, .78, .79), and continuous growth (e.g., “Aging means to me that I can still learn new things”; Cronbach’s α 2008–2017: .82, .79, .79, .81). For each subscale, a sum score was computed and transformed so that higher values indicate higher endorsements of social loss, physical decline, and continuous growth, respectively.
Covariates
We controlled for age, gender, education, self-rated health (except in the model with self-rated health as outcome), and functional health (except in the model with functional health as outcome). The assessment of education was derived from the International Standard Classification of Education (ISCED) coding of the United Nations Educational, Scientific and Cultural Organization (2012). Four groups of school and professional education were differentiated (i.e., low, medium, elevated, and high education).
Statistical analyses
Longitudinal multilevel regression models 3 (Hox & Kreft, 1994; Ram & Grimm, 2015) were computed using Stata 15.0 (StataCorp LLC, 2017) to investigate the predictive role of self-reported problems with vision for trajectories of health and cognitive ability, well-being, and subjective age views. The time unit specified in the model was “years since baseline (2008).” Self-reported problems with vision were specified as a time-varying predictor. 4
Linear trajectories were modeled in this study because not all individuals provided four observations so that the amount of repeated observations may not be sufficient for a reliable estimation of nonlinear trajectories.
Results
Vision problems as predictors of health and cognitive ability
Between-person effects of vision problems
Regarding the outcomes of health and cognitive ability (Table 2), the between-person component indicating overall more self-reported problems with vision was consistently associated with all health outcomes at baseline, that is, with poorer functional and self-rated health, with a higher number of chronic diseases, and with lower information processing speed. Longitudinally, overall more problems with vision also predicted a steeper decline in functional health as well as a steeper increase in the number of chronic diseases.
Predictors of health and cognitive ability.
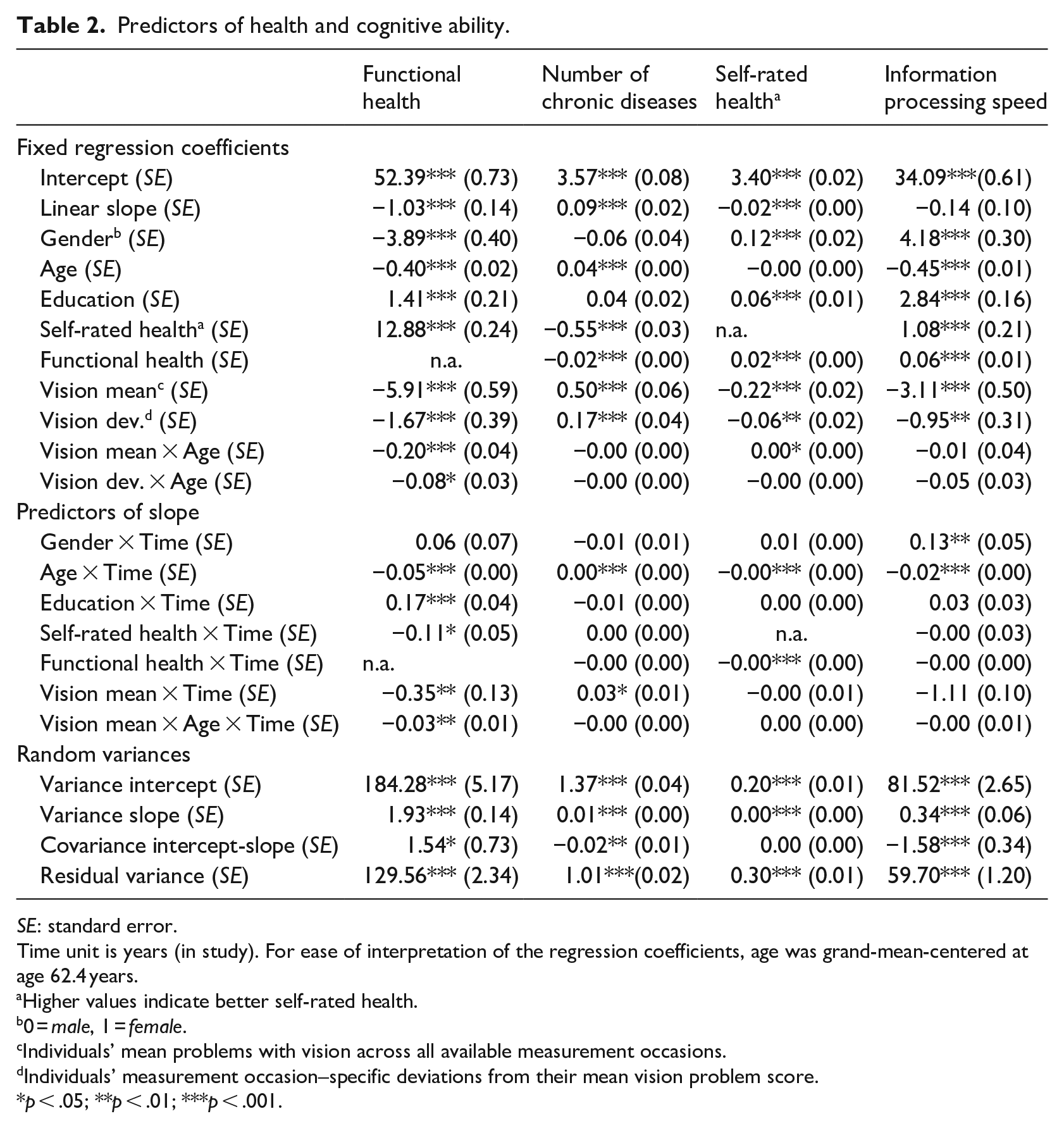
SE: standard error.
Time unit is years (in study). For ease of interpretation of the regression coefficients, age was grand-mean-centered at age 62.4 years.
Higher values indicate better self-rated health.
0 = male, 1 = female.
Individuals’ mean problems with vision across all available measurement occasions.
Individuals’ measurement occasion–specific deviations from their mean vision problem score.
p < .05; **p < .01; ***p < .001.
Within-person effects of vision problems
Similarly, the within-person component of vision problems was significantly related to all health outcomes. On measurement occasions when individuals had more problems with vision, they also revealed poorer functional and self-rated health, more diseases, and they scored lower on information processing speed.
The role of baseline age
With regard to the potentially moderating role of age in the associations between problems with vision and health outcomes, all described between- and within-person associations of vision problems with functional health increased with advancing baseline age: That is, in individuals who were older at baseline, the association of overall more vision problems with poorer baseline functional health and with a steeper decrease in functional health was stronger than that among individuals with a younger age at baseline. Furthermore, the within-person association linking measurement occasion–specific, increased vision problems with poorer functional health on that specific measurement occasion was also closer among individuals who were older at baseline (Figure 1).
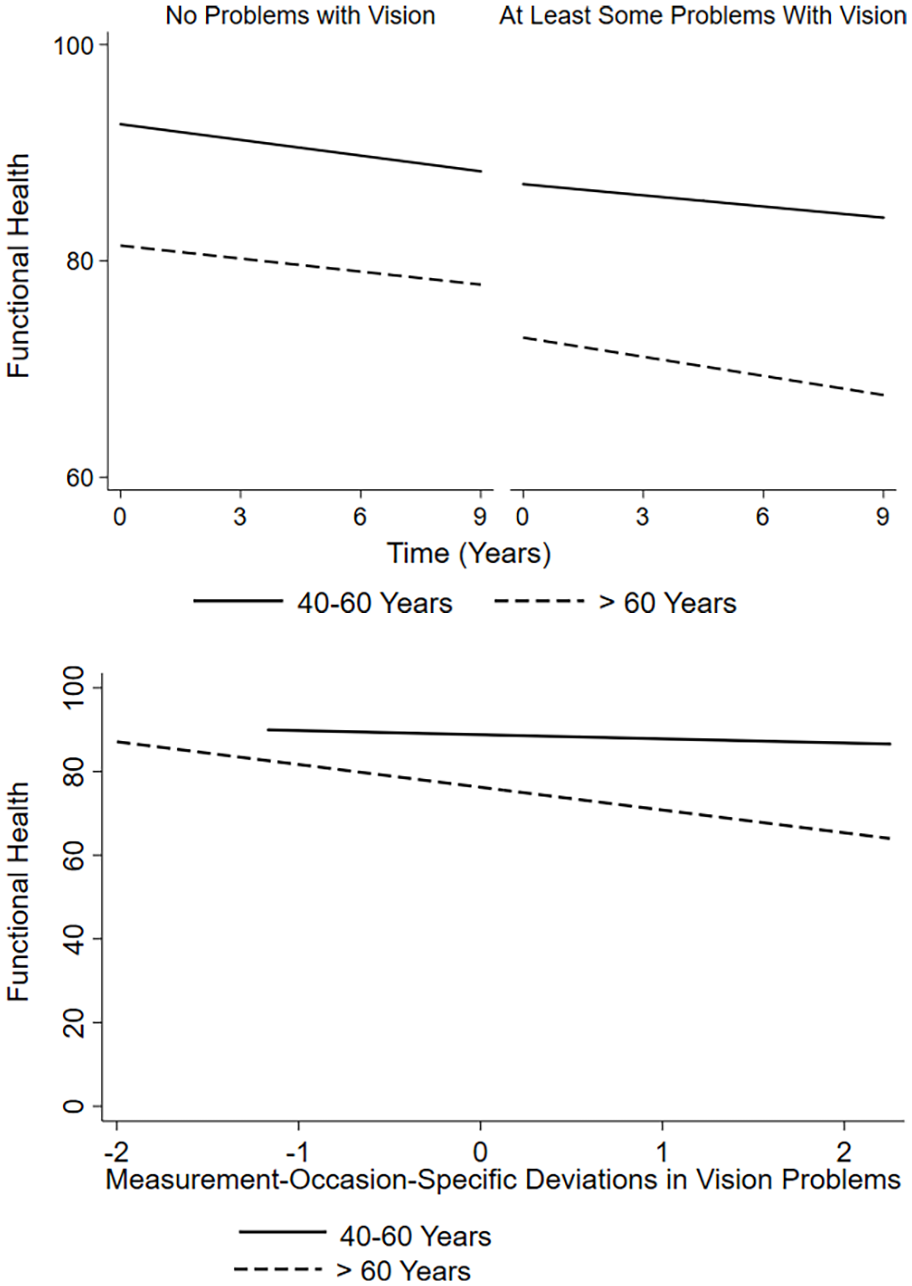
The association of self-reported vision problems with functional health.
In contrast, the described association between overall more problems with vision and poorer baseline self-rated health decreased with advancing baseline age.
Vision problems as predictors of well-being
Between-person effects of vision problems
All outcomes of well-being (Table 3) were, at baseline, significantly related to the vision between-person component indicating overall mean vision problems. Those reporting overall more vision problems had a lower life satisfaction, lower positive and higher negative affect, more depressive symptoms, and higher levels of loneliness at baseline. In addition, these person-specific vision problem mean scores were significantly negatively related to change in life satisfaction and positive affect and significantly positively related to change in negative affect and depressive symptoms, indicating less favorable changes over time across all well-being outcomes except loneliness among those with more vision problems.
Predictors of well-being.
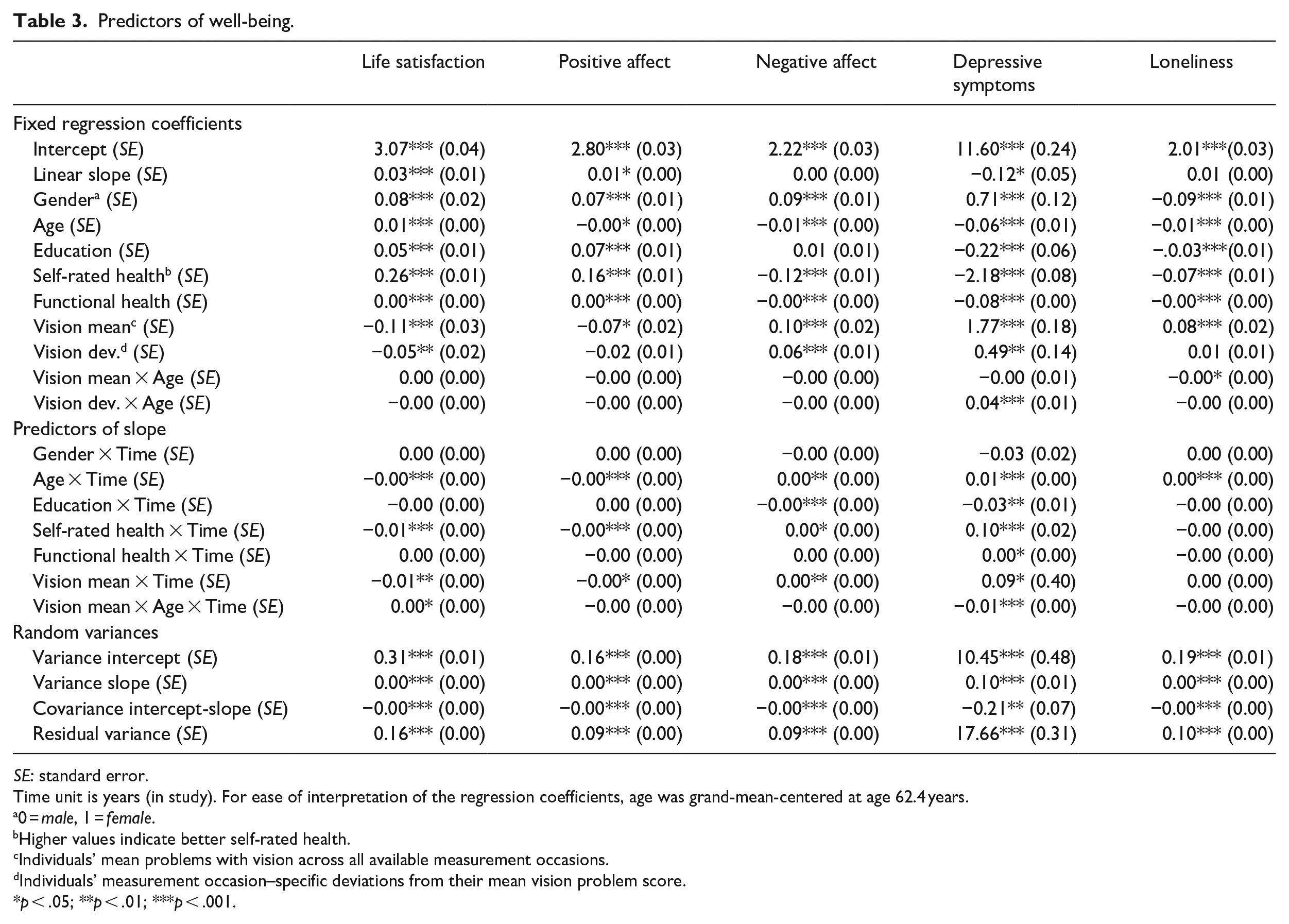
SE: standard error.
Time unit is years (in study). For ease of interpretation of the regression coefficients, age was grand-mean-centered at age 62.4 years.
0 = male, 1 = female.
Higher values indicate better self-rated health.
Individuals’ mean problems with vision across all available measurement occasions.
Individuals’ measurement occasion–specific deviations from their mean vision problem score.
p < .05; **p < .01; ***p < .001.
Within-person effects of vision problems
The within-person effects of vision problems were also significant for several well-being outcomes. On measurement occasions when individuals encountered more problems with vision, they reported a lower life satisfaction, higher negative affect, and more depressive symptoms.
The role of baseline age
With regard to age moderation effects on vision-well-being associations, overall more vision problems were related to less favorable trajectories of life satisfaction (i.e., less increase in life satisfaction over time), but this association was attenuated among those who were older at baseline.
For depressive symptoms, an older baseline age augmented the within-person association between more vision problems on a certain measurement occasion and more depressive symptoms (Figure 2). At the same time, the association of overall more vision problems with less favorable change in depressive symptoms became weaker with an increasing baseline age.
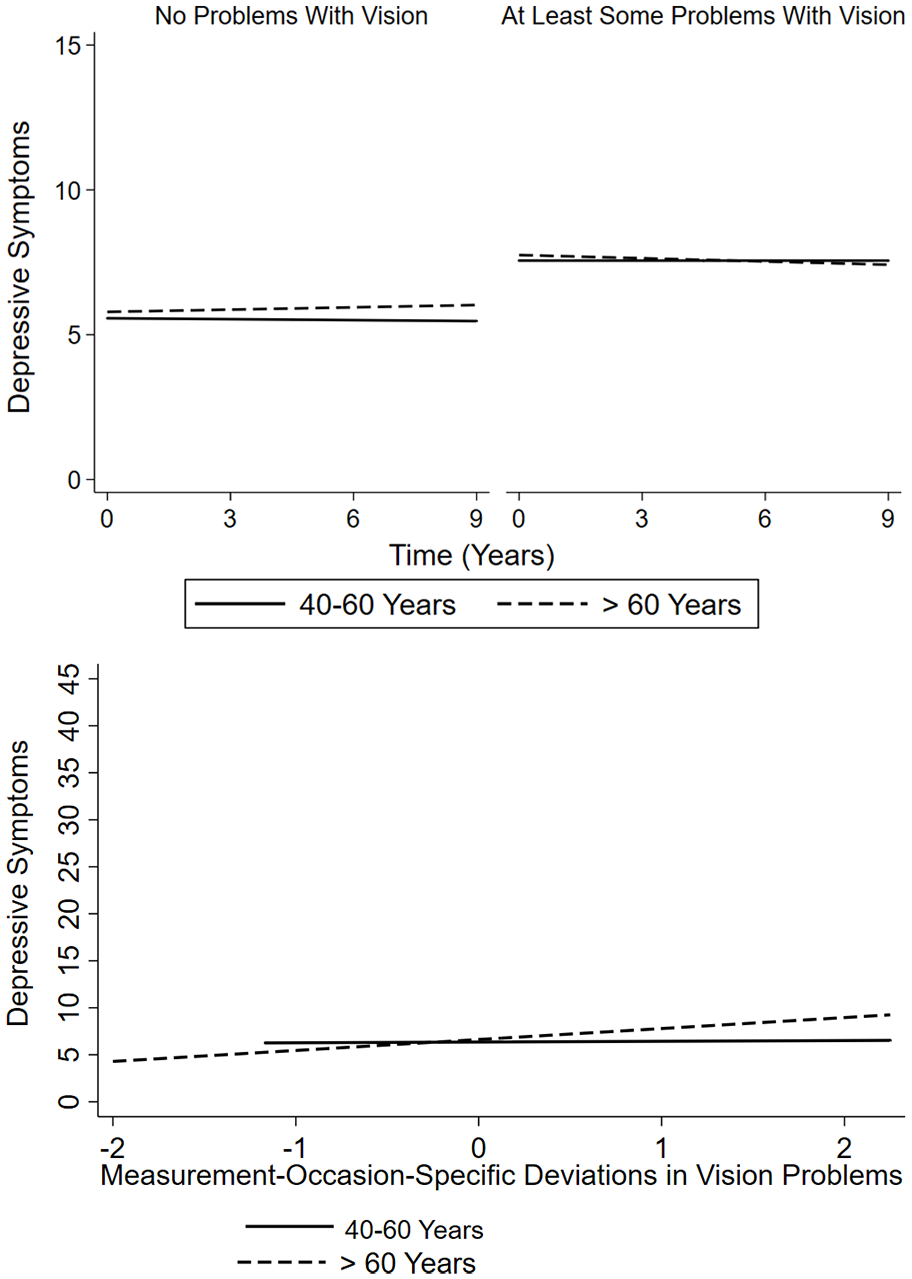
The association of self-reported vision problems with depressive symptoms.
Overall more vision problems were related to greater loneliness at baseline, but less so among those who were older at baseline.
Vision problems as predictors of subjective age views
Between-person effects of vision problems
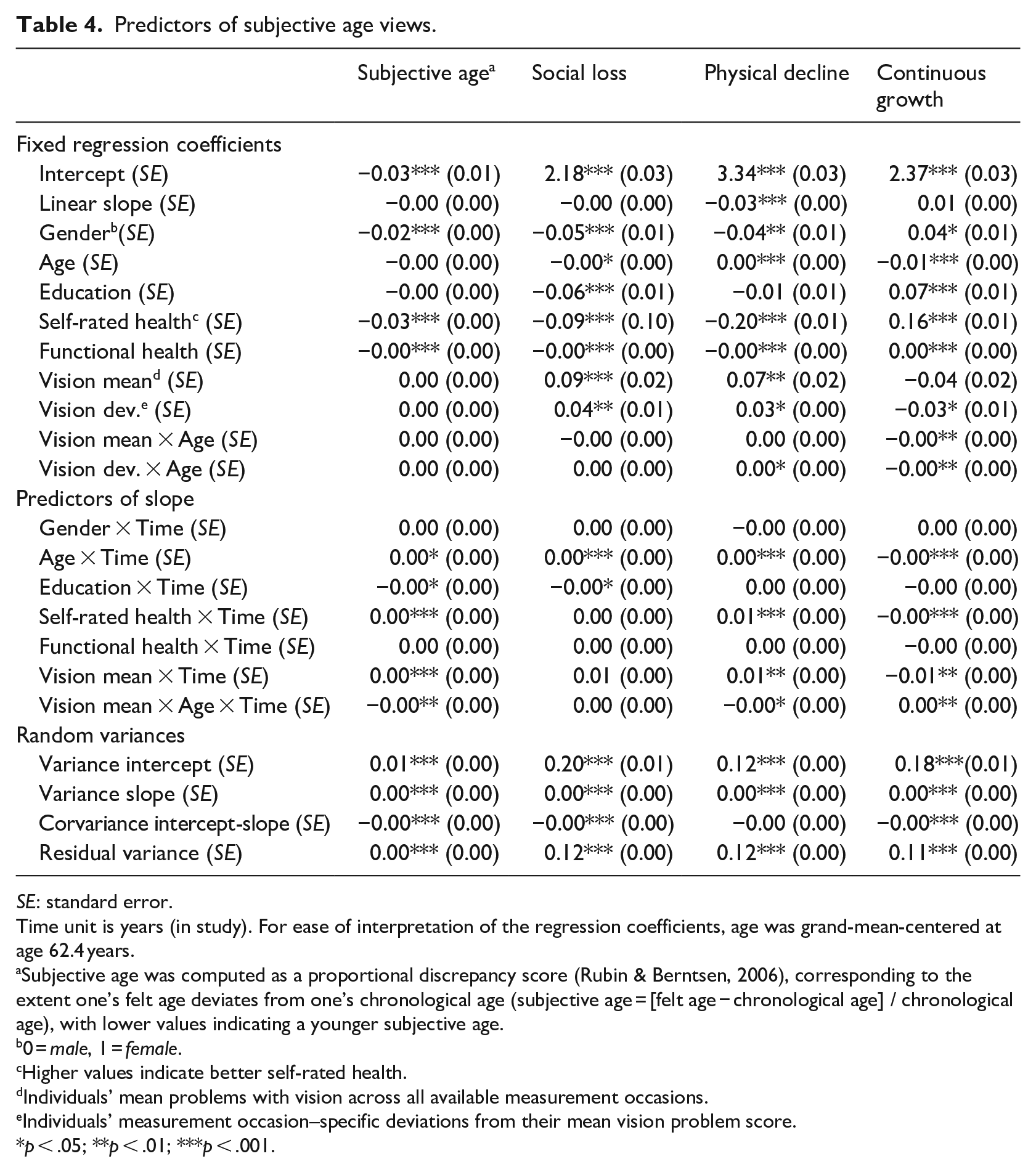
Finally, several associations between vision problems and subjective age views reached statistical significance (Table 4). Those with overall more vision problems had higher self-perceptions of social loss and physical decline at baseline. Moreover, overall mean vision problems were significantly positively associated with change in subjective age and self-perceptions of physical decline, and negatively with change in continuous growth. These associations indicate that more problems with vision were associated with an older subjective age, higher self-perceptions of physical decline, and lower self-perceptions of continuous growth over time.
Predictors of subjective age views.
SE: standard error.
Time unit is years (in study). For ease of interpretation of the regression coefficients, age was grand-mean-centered at age 62.4 years.
Subjective age was computed as a proportional discrepancy score (Rubin & Berntsen, 2006), corresponding to the extent one’s felt age deviates from one’s chronological age (subjective age = [felt age − chronological age] / chronological age), with lower values indicating a younger subjective age.
0 = male, 1 = female.
Higher values indicate better self-rated health.
Individuals’ mean problems with vision across all available measurement occasions.
Individuals’ measurement occasion–specific deviations from their mean vision problem score.
p < .05; **p < .01; ***p < .001.
Within-person effects of vision problems
Also several within-person effects of vision problems were significant. On measurement occasions when individuals faced more severe problems with vision, they reported higher self-perceptions of social loss and physical decline as well as lower self-perceptions of continuous growth.
The role of baseline age
There were several significant age moderation effects on the associations between vision problems and subjective age views. Overall more vision problems were associated with lower perceptions of continuous growth at baseline. This association was stronger among individuals who were older at baseline (see Figure 3). In contrast, the association between overall more vision problems and less favorable change in subjective age and in self-perceptions of physical decline and continuous growth was weaker among individuals who were older at baseline.
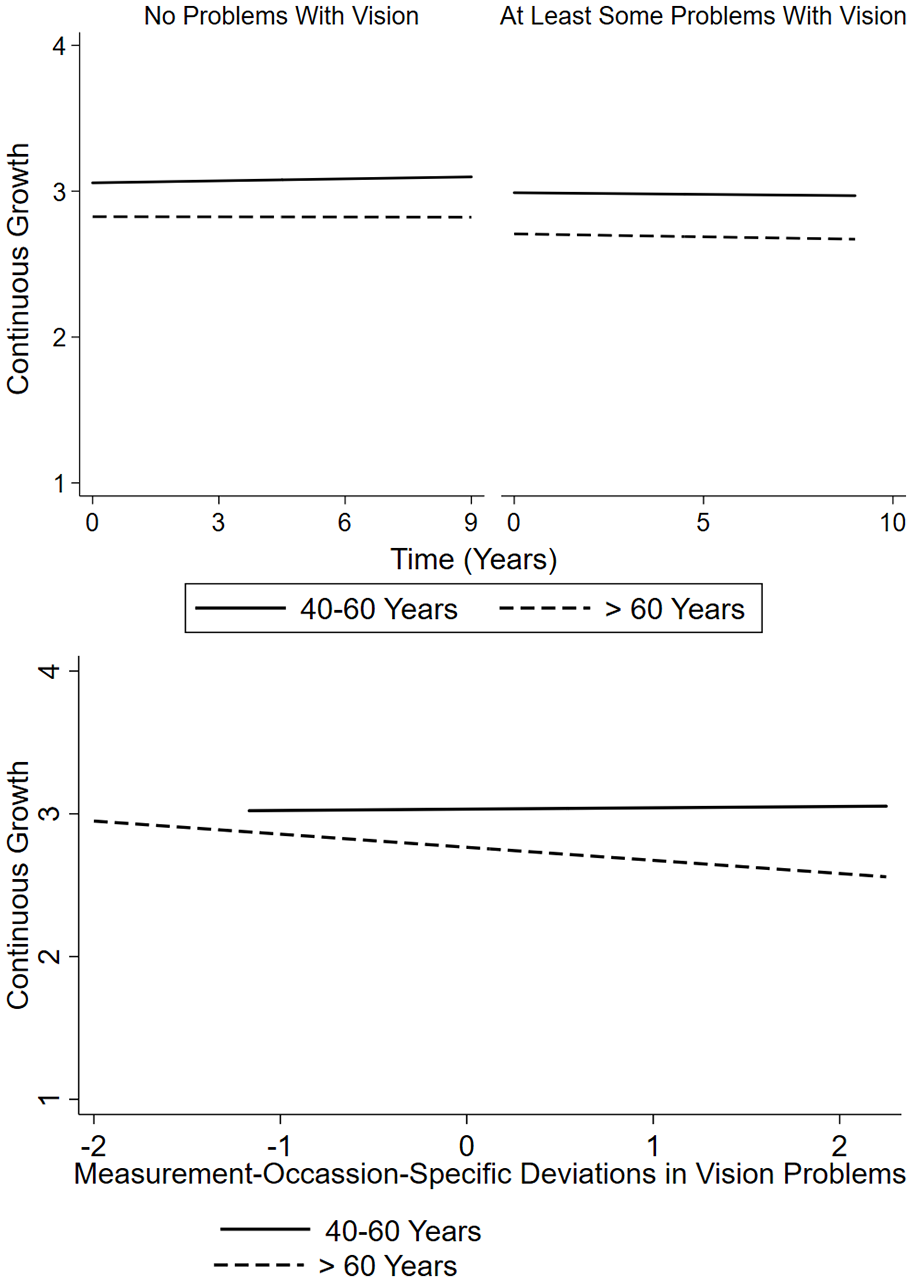
The association of self-reported vision problems with self-perceptions of continuous growth.
At the same time, time-varying associations between more vision problems at a specific measurement occasion and higher self-perceptions of physical decline as well as lower self-perceptions of continuous growth at that measurement occasion grew stronger with an older baseline age. These effects are illustrated for self-perceptions of continuous growth in Figure 3. 5
Discussion
Vision problems and trajectories of successful aging outcomes
We were able to demonstrate meaningful and robust associations of vision problems with long-term changes in successful aging indicators. Specifically, individuals who reported more problems with vision experienced a steeper 9-year decline in functional health, a steeper increase in the number of chronic diseases and less favorable long-term changes in indicators of well-being (life satisfaction, positive and negative affect, depressive symptoms) as well as in subjective age views (subjective age, self-perceptions of physical decline and continuous growth).
Adults who report more problems with vision are thus at a higher risk of long-term decline in health and psychosocial functioning. These decline dynamics might be prevented or buffered if visually impaired individuals receive the optimal medical treatment (e.g., cataract surgery) or assistive devices to minimize the everyday consequences of vision loss. Also, supporting visually impaired individuals in making use of compensatory resources such as cognitive abilities, which seem to gain in importance for independent functioning and well-being when sensory impairment sets in (Heyl & Wahl, 2012; Wettstein et al., 2015), is a promising approach. In addition, coping strategies that promote maintenance of health and well-being, particularly accommodative strategies of flexible goal adjustment and goal disengagement (Brandtstädter, 2015), but also the combined use of several strategies, have been found to reduce the negative consequences of impaired vision (Boerner & Wang, 2012; Heyl et al., 2007; Wettstein et al., 2019), and should therefore be promoted among individuals with vision loss.
The role of chronological age
The role of baseline age as a potentially moderating factor turned out to be complex and domain specific. For functional health, all between- and within-person effects of vision problems revealed an age-related increase. Also, when specifying vision problems, assessed at baseline, as a time-invariant predictor, vision problems were associated with a steeper decline in functional health among individuals who were older. This means that older adults in particular experience compromised health and restrictions in everyday activities when vision problems set in and progress, whereas middle-aged adults may have more compensatory resources available to counteract the negative effect of visual impairment on functional health. In addition, sources of vision loss might be different at different ages. Among older adults, a common cause, such as changes in the central nervous system (Baltes & Lindenberger, 1997), might operate and cause both impaired vision and reduced cognitive functioning (Kiely & Anstey, 2015; K. Z. H. Li et al., 2015; Roberts & Allen, 2016; Wahl & Heyl, 2003). This co-occurrence of two impairments might be particularly detrimental for late-life functional health (Heyl & Wahl, 2010, 2012; Wettstein et al., 2015).
In contrast, self-rated health at baseline was less closely related to vision problems among adults who were older at baseline. This seemingly contradictory pattern of findings can be seen in analogy with the “disability paradox” (Albrecht & Devlieger, 1999) or “well-being paradox” (Schilling, 2006) that postulates that disability and impaired health are not necessarily reflected in subjective ratings of health and quality of life. The specific group of older adults with vision loss might regard their impaired vision as to some extent normative and therefore perceive their own health as less restricted compared to individuals in middle adulthood who have to deal with the rather unexpected, “off-time experience” of vision loss.
Chronological age also moderated several of the associations between vision problems and well-being. With increasing baseline age, overall more problems with vision had a weaker detrimental impact on changes in life satisfaction and depressive symptoms. Also, the baseline loneliness levels of older adults were less closely related to vision problems than the loneliness levels of individuals with a younger age. It thus seems that older adults adapt to vision loss more successfully than younger adults, at least when specific well-being outcomes are focused and when temporal dynamics of vision loss are not considered. Adaptation and “well-being restoration” processes after the onset of vision loss in late life, such as age-related macular degeneration, have been reported before (e.g., Schilling & Wahl, 2006). Also, our finding that individuals well-being might be less affected by vision loss with advancing age is in line with other studies (Boerner, 2004; Brunes et al., 2019; Good et al., 2008), and such an age pattern was also found in this study when specifying vision problems assessed at baseline as a time-invariant predictor in additional analyses.
However, within-person associations revealed a different pattern: on measurement occasions when individuals encountered more problems with vision, they reported more depressive symptoms, and this within-person association was particularly close among older adults. This finding illustrates the importance of taking the temporal dynamic of vision loss, such as temporary vision improvements or deteriorations, into account when investigating its consequences for well-being. With regard to adaptation to vision loss, it seems that with increasing age, individuals are better able to adjust to overall vision loss and minimize long-term detrimental effects on depressive symptoms. However, a more short-term increase in problems with vision seems to be challenging particularly for older individuals, resulting in a parallel increase in depressive symptoms that is larger than for middle-aged adults. The SAVI model might provide an explanation for this finding by claiming that when older adults experience high emotional arousal, they might reveal a steeper well-being decline than younger adults and need more time for processes of adjustment (Charles, 2010). A recent increase in vision problems might be such a source of “sustained emotional arousal” that challenges and compromises older adults’ adjustment to a stronger extent compared to younger individuals, for example, by arousing fears of going blind or losing autonomy in everyday life.
Finally, associations between vision problems and subjective age views are also age dependent. The baseline self-perception of continuous growth, that is, experiencing aging as an opportunity for ongoing personal development and for broadening one’s skills, was particularly low among older adults with overall more vision problems compared to younger adults with more vision problems. Moreover, a measurement occasion–specific increase in vision problems was associated with self-perceptions of higher physical decline and less continuous growth, and these associations grew stronger with advancing baseline age. This finding can be seen as additional evidence for a higher vulnerability to recent vision deterioration with advancing baseline age on a within-person level, that is, when intraindividual changes in vision problems are considered. According to our findings, this higher vulnerability seems to affect all successful aging domains included. With regard to subjective age views, this finding is also in line with other studies reporting stronger associations between health and subjective age views with advancing age (Bergland et al., 2014; Brothers et al., 2015; Levy et al., 2002, 2016; Stephan et al., 2012).
At the same time, however, and in line with the findings on some of the well-being outcomes, other associations of vision problems with subjective age views, namely those reflecting between-person effects of and interindividual differences in vision problems, rather indicate a lower vulnerability with advancing age: Longitudinally, overall more vision problems predicted an older subjective age, a higher self-perception of physical decline, and a lower self-perception of continuous growth over time, but these effects were weaker among older adults. This age moderation effect remained significant for the associations between vision problems and changes in self-perceptions of physical decline and continuous growth when we specified vision problems at baseline as a time-invariant predictor.
Our findings thus imply that the assumption that “successful aging may be more challenging for visually impaired older adults” (Swenor, Lee, et al., 2019) needs refinement: Whether an older age represents an additional challenge to successful aging among individuals with vision loss depends on various factors, including the specific outcome domains as well as the time frame and dynamics of vision loss.
Age and consequences of vision problems: practical implications
With regard to practical implications of our findings, the often stated argument that particularly older adults with vision loss should be the target group for interventions might need some refinement, and a more differentiated perspective within the research domain of psycho-ophthalmology (Heyl & Wahl, 2014; Méndez-Ulrich & Sanz, 2017; Wahl, 2013) is needed. For several well-being and subjective age views outcomes, our findings rather suggest a higher long-term adaptational potential with advancing age, supporting that “visually impaired elderly can effectively compensate for or otherwise adapt to declines in competence domains” (Burmedi et al., 2002, p. 15). Interventions to counteract long-term detrimental consequences of vision loss for psychosocial functioning, for example, by promoting helpful coping strategies (Boerner, 2004; Boerner & Wang, 2012; Brennan-Ing et al., 2013; Heyl et al., 2007; Wettstein et al., 2019), might therefore be particularly beneficial for adults in midlife, rather than in late life.
However, short-term decreases in vision seem to affect individuals’ well-being and subjective age views to a greater extent when they are older, so that they may need more support than middle-aged adults in such “shock” times of a recent vision deterioration. Also, independent of whether the vision loss set in recently or long time ago, its effects on functional health are consistently stronger and more detrimental for individuals who are older. Therefore, for this particular health domain, interventions should indeed primarily focus on older adults to help them to reduce restrictions in the execution of everyday tasks, for example, by investing in compensatory resources such as cognitive abilities (Heyl & Wahl, 2012).
Limitations
This study has several limitations. All outcomes included as well as our key predictor, vision problems, were self-reported. Reported problems with vision do not necessarily reflect the objective extent of visual acuity. One reason for the discrepancy between subjective and objective vision could be that items such as “problems recognizing people” might measure not only vision-related but also cognitive problems for some individuals (although the vast majority of individuals in our study sample did not have scores on the digit symbol substitution test that indicate a probable cognitive impairment). On the other hand, items with similar formulations as the ones used in this study have been used before to assess self-reported problems with vision (Frank et al., 2019; Xiang et al., 2019; Yip et al., 2014), and they reveal a considerable overlap with objective vision measures (Eekhof et al., 2000). For instance, Whillans and Nazroo (2014) reported that 97% of those with self-reported normal vision also exhibited a normal vision score when objectively tested.
Furthermore, about one third of the study sample had only one study participation and thus provided only one observation. These individuals might actually be those who experienced the most pronounced vision deteriorations and the steepest declines in health and psychosocial functioning over time. However, our selectivity analyses with regard to the study variables at baseline revealed that the baseline differences in all study variables were of small effect size, so that the bias in the effect estimates should be minor only.
Caution is needed with regard to causal interpretation. The between-person predictor effects of vision problems are based on the information aggregated across all measurement occasions, which is a necessary computation step to disentangle between- and within-person effects of time-varying predictors (Hoffman & Stawski, 2009; Schwartz & Stone, 1998). Within-person effects indicate the extent to which the respective outcome at a specific measurement occasion is associated with a measurement occasion–specific increase or decrease in vision problems. Consequently, it could for instance be that a measurement occasion–specific increase in depressive symptoms causes negative self-evaluations, including the subjective perception of deteriorated vision. Alternatively, specific life events which were not studied here might have affected change in both vision problems and the outcome variables between adjacent measurement occasions, thereby causing a spurious association between vision problems and successful aging outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The German Ageing Survey (DEAS) was funded under Grant 301–1720–2/2 by the German Federal Ministry for Family, Senior Citizens, Women, and Youth. The content is the sole responsibility of the authors. This contribution is part of the project “Health Trajectories into Old Age – Ways into Need for Long-Term Care” that is funded by the National Association of Statutory Health Insurance Funds (GKV-Spitzenverband).