
Abstract
Educational support for children with visual impairments (VIs) at school relies on effective information-sharing between hospital eye services and schools. There may be delays in this process which impede school staff’s efforts to help affected children. As part of a programme of work aiming to improve outcomes for children with cerebral visual impairments (CVIs), this study carried out qualitative interviews to understand the views of primary school staff about receiving and using external specialist advice in general. These data can be used to inform and improve information-sharing aimed at supporting children in primary school who have VI.
Views of primary school teachers and staff with responsibility for supporting children with additional needs were elicited in nine interviews, across three mainstream primary school settings in Gloucestershire, UK. Interviews were carried out in October 2017. Participants were asked about their experiences of working with children with additional needs and engaging with outside specialist providers. Thematic analysis was used to look for patterns in the data.
Interviews revealed four major themes: understanding the condition (including training, individual differences, and understanding the aim of the strategy); translating reports into action (including adaptations to recommendations, team working, and communication formats); follow-up (including feedback and measuring progress); and barriers and opportunities for accessing support (including systematic barriers, going private, and ideal scenarios).
This small study provides insights into how teachers and school staff perceive the relationship with external specialists. Services for children with VI in primary schools may be enhanced if they provide information about the impact of VI; about the underlying conditions if known, training and awareness activities for staff and offer a route for follow-up or enquiries. These insights can be used to inform service design and policy.
Background
In the United Kingdom, the Children and Families Act 2014 changed how support for children with special educational needs or disabilities (SEND) should be assessed and provided for, emphasising their functional needs as well as their medical diagnoses (Castro & Palikara, 2016). Children with SEND are allocated extra help either from within-school resources, from external agencies who may support schools or using extra resource applied for by the school as part of a Local Authority (LA; local government department for that city or geographic area) funded Education, Health and Care plan (EHCP). Some LAs will provide additional ‘top-up’ funding for specific pupils without an EHCP. School budgets include a proportion intended for this in-house support for SEND pupils; however, this is not ring-fenced. If schools apply for top-up funding or for an EHCP for a child with vision problems, the LA requests reports from relevant professionals, including paediatric specialists such as ophthalmologists, optometrists, and orthoptists, who are required to contribute details of a child’s visual impairments (VIs) and the practical implications of these impairments. Once assessed, the level of support to be provided for a child is specified and the provision of that support is dependent on the activities of teachers and learning support assistants (LSAs) in school and/or qualified teachers of the visually impaired (QTVIs). To help the children being supported by within-school resources, the schools may themselves request assessments from specialists such as educational psychologists, speech and language therapists, or QTVIs, as needed. These may be funded by the LA or be private practitioners.
It is important therefore that vision care specialists provide information about each child’s VI to the QTVI service and/or to the school, so they can allocate appropriate support. However, lack of timely input from ophthalmologists or hospital vision care teams to schools has been reported (Boyce et al., 2015; Youngerson-Reilly et al., 1994). This causes distress to families and a delay in support for the child. The lack of information held by special schools about their children’s visual needs has been well documented (Little & Saunders, 2015; Woodhouse et al., 2014). Furthermore, a recent study has shown benefits in behaviour and attention to lessons, for children in a special school after their visual needs were communicated to their school (Black et al., 2019). It is likely lack of school-held information is particularly a problem for children with cerebral visual impairments (CVIs), as many have near-normal acuity (van Genderen et al., 2012) and so their vision problem is not easily apparent and their VIs may be undetected.
The CVI Project is a 5-year programme of work involving several interlinked studies which aim to increase understanding about CVI and how best to help affected children (www.thecviproject.co.uk). As part of a study estimating the prevalence of CVIs in primary schools, we opportunistically elicited the thoughts of staff in the participating schools about what information regarding a child’s medical or sensory problems they find helpful, and how they tried to use it in practice. Qualitative interviews with school staff who work with children with additional needs were carried out to provide insight into their experiences when engaging with external specialists in general, so that we could use their perspectives to help refine a model of information-sharing about CVIs for use in a future study. We report the results here as they may be useful more widely to help inform communications between vision specialists and schools.
Methods
Qualitative research methodology is useful for elucidating a deeper understanding of experiences, decision-making, and behaviour, to inform intervention design (Corrrigan et al., 2006). The Socioecological Model provides a useful framework from which to investigate our research question by identifying influences on the child’s development at both the microsystem and mesosystem levels (Kilanowski, 2017). Individual members of staff work one-to-one with children using strategies that have been transmitted via communication between school and external service providers. We sought, therefore, to identify the barriers and facilitators to this communication to influence the design of a future intervention for children with CVI. Purposive sampling was used to identify eligible participants (staff) from primary schools who had taken part in our study on the prevalence of CVIs in primary schools (results under review).
All participating schools in Gloucestershire from the prevalence study (n = 9) were contacted by telephone and invited to take part. Initial contact was made with the named contact person on record from the previous study, usually the Head Teacher or the teacher with primary responsibility for SEND pupils (Special Educational Needs Co-ordinator, SENCO). Contacts were informed that anyone working with children with special needs was eligible to participate. The topic guide (Table 1) was developed after consideration of the existing literature, the study aims, and discussion with a group of parents and professional study advisors. Interviews were held either face-to-face or by telephone by one researcher, a member of the study team with expertise in qualitative research methods. Interviews were continued until the researcher felt that no new topics were emerging. Interviews were audio recorded and transcribed with consent. NVivo 11 was used to code the interviews and thematic analysis was carried out to look for patterns in the data. A grounded theory approach was taken (Strauss & Corbin, 1994), coding each transcript iteratively so that themes emerged without a pre-existing framework. Themes were discussed with other members of the study team to reach a consensus on the final major and subthemes. Ethical approval for the study was granted by the University of Bristol’s Faculty Research Ethics Committee (Ref: 39801).
Topics discussed during the interviews.
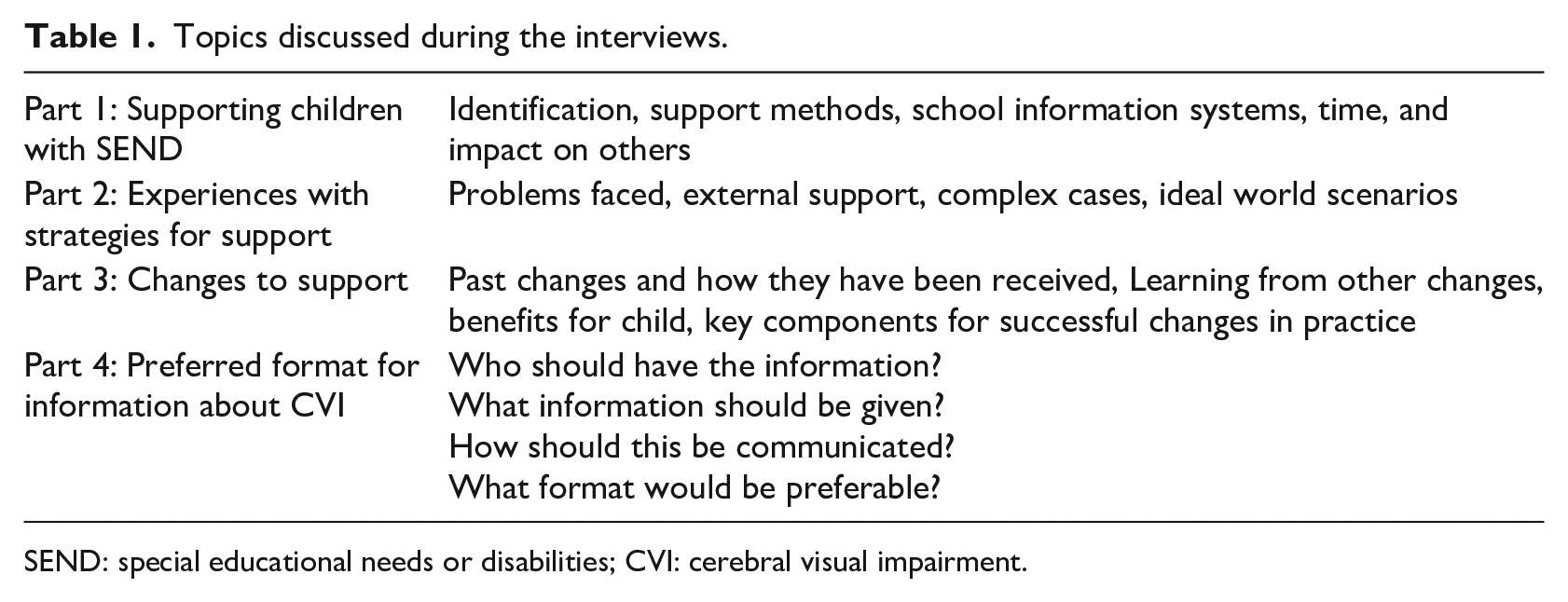
SEND: special educational needs or disabilities; CVI: cerebral visual impairment.
Results
Three schools volunteered to take part and nine members of school staff volunteered to be interviewed. All nine interviews were carried out, three face-to-face and six by telephone. Three roles were represented: two head teachers, three teachers who were SENCOs, and four teaching assistants with responsibility for working with children with special educational needs. Length of service varied from 5 to 25 years, as seen in Table 2.
Role and length of service for each interview participant.
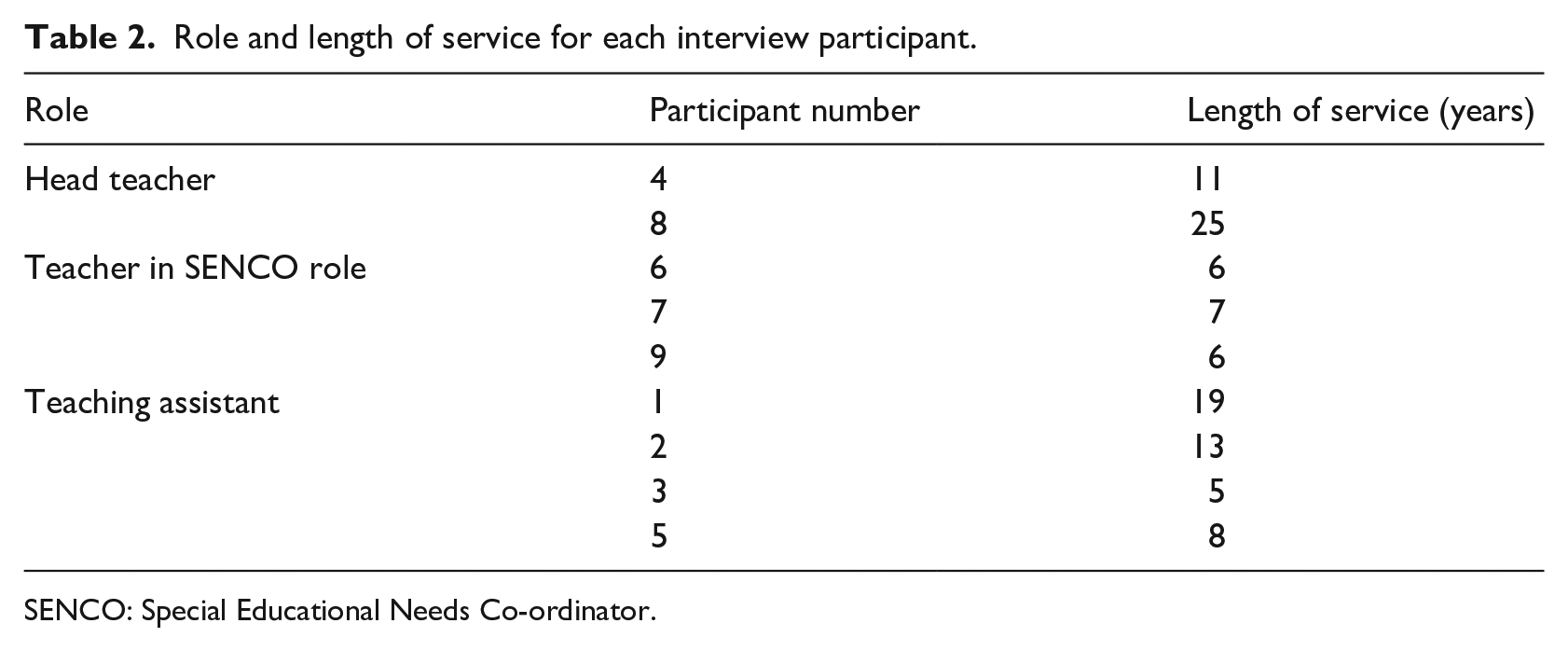
SENCO: Special Educational Needs Co-ordinator.
Interviews ranged from 20 to 56 min (average of 32 min) in length. Analysis of the interviews led to the emergence of four major themes including understanding the condition, translating reports into action, follow-up and barriers, and opportunities for accessing support for children. The major themes and subthemes are summarised in Figure 1 and discussed in the following sections. Table 3 shows a selection of illustrative quotes for each subtheme.
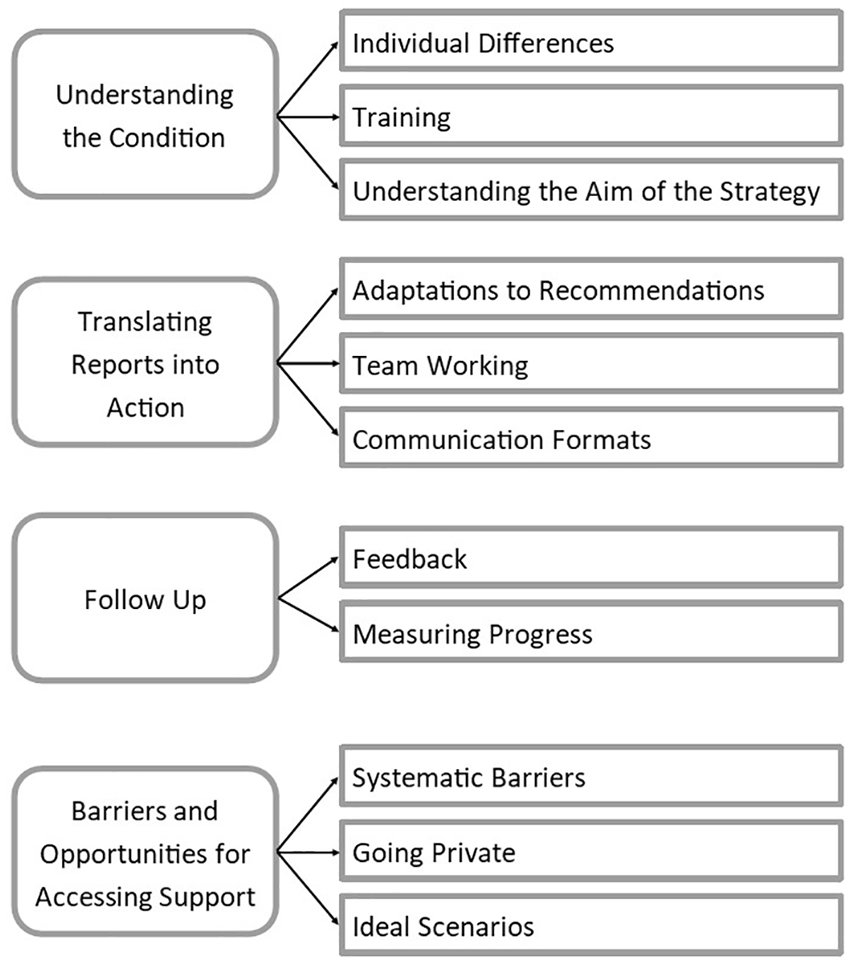
Themes from interviews.
Illustrative quotes for each subtheme.
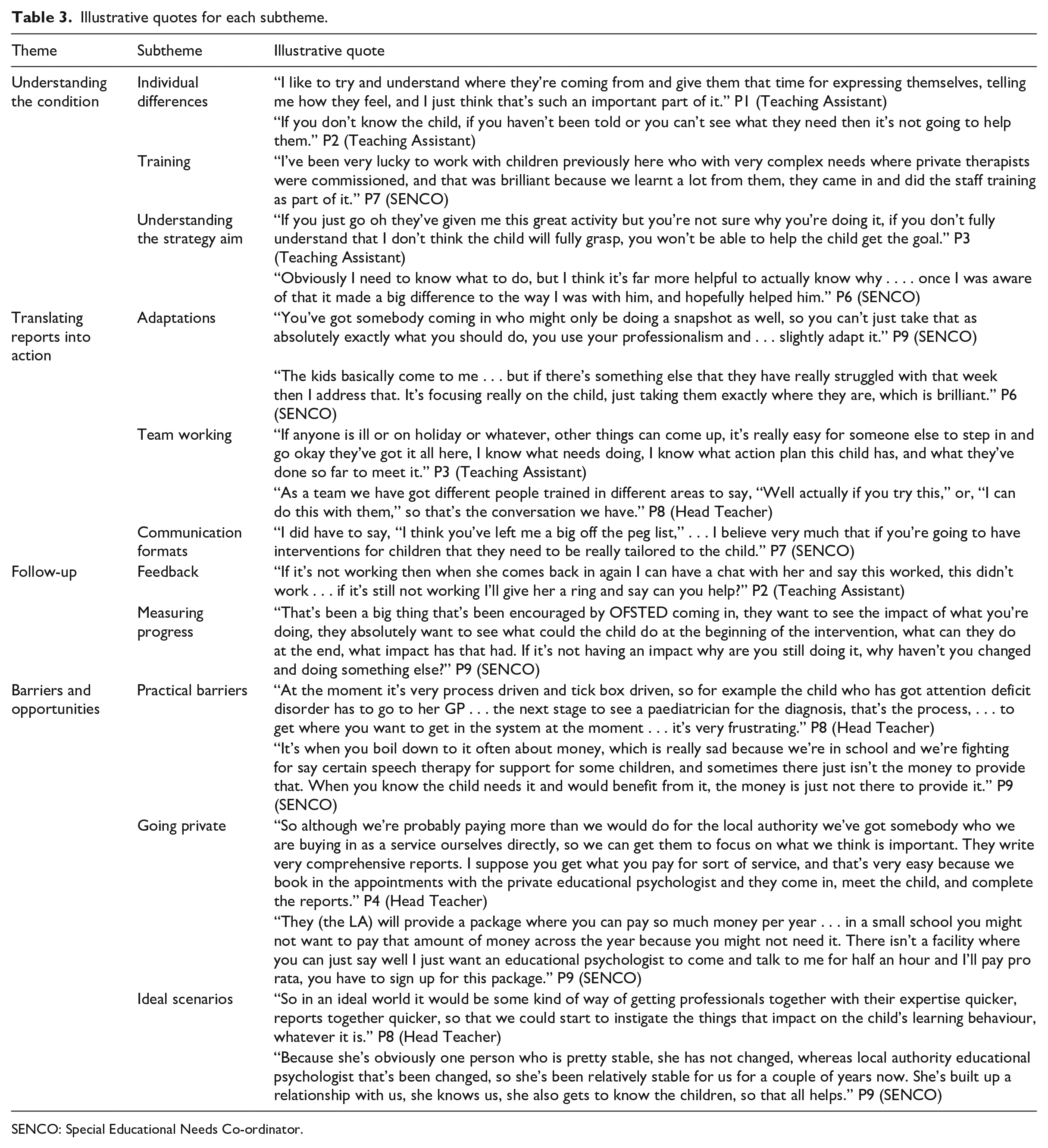
SENCO: Special Educational Needs Co-ordinator.
First theme: understanding the condition
Every participant contributed to this theme, which broadly emphasises the need for people working with children with additional needs to ensure they are aware of the impact of the condition for each specific child. They valued expert input in widening their knowledge of each condition and how it might affect the child. Finally, they wanted to know why and how a strategy was supposed to help so they could tailor its implementation to the school environment and the interests of the child.
Individual differences
Participants described the importance of understanding the specific needs of each child when it came to support. They used empathy and tried to understand the perspectives of the child given their specific challenges and used this to tailor their day-to-day support at school, for example, ‘rather than saying no you need to do this, well you can go okay you need a quiet room, you need a darkish space, you need this, and then they can see that they’re starting to make progress’ (P8, Head Teacher). This approach contributed to how school staff could tailor any recommendations to the individual child, as described in the second theme.
Training
Where possible, participants were keen to undertake training to widen their knowledge and understanding of children’s needs. They described situations where training from external specialists was particularly useful, for example, ‘the OT that we had for the first child I had was very good . . . she gave me personal training, and she actually did staff training on all sorts of things, so that was really useful’ (P6, SENCO).
Understanding the strategy aim
Where participants discussed specific strategies for supporting children, most emphasised the importance of understanding the aim of the strategy, not just how it was implemented, as ‘it’s far more helpful to actually know why’ (P6, SENCO). This meant that participants could be confident to individualise the strategies, changing them to make them more meaningful for the child without losing sight of the purpose behind them.
Second theme: translating reports into action
This theme arose from descriptions of action that might be taken following the input of specialist support. Participants expressed the need to adapt the content of the reports to the setting and the needs of the child. They highlighted the value of good team dynamics to both implementation of strategies and monitoring of progress.
Adaptations to recommendations
Adapting the strategy to improve effectiveness was seen as an essential part of implementing support. Participants gave examples of strategies that they had used in one context that could be adapted and prove useful in another. One participant described how they had been using Lego to support communication and this was useful when the child was upset:
He built in Lego the dinner hall, he built all the tables, the characters on it, and from that, it absolutely broke the ice, because he was able to then talk about the incident that had happened, I could understand him, so rather him going off in his fit of rage and bottling it all, suddenly he started talking about his emotions. (P1, Teaching Assistant)
Participants also observed instances where strategies were clearly not working and spoke of the need to move on to try something else. Participants used their knowledge of the aim of the strategy combined with their understanding of the child’s condition and individual differences to decide how strategies might work best for them.
Team working
Participants spoke about the importance of appropriate and timely communication within both school-based teams and external agencies, describing how different team members’ expertise could be useful, and how willing they were to adopt perspectives and ideas from others. Working effectively as a team ensured consistency of support could be maintained, and specific needs communicated to all those who needed to know. Participants found challenges getting the right people to communicate, especially when various agencies were involved, but where this was successful the value was seen as addressing the needs of the child in a comprehensive way:
Professionals talking to each other is crucial, so it’s called TAC, Team Around the Child meeting, and . . . they are a very useful meeting because you get a different insight into the child according to different experts’ knowledge and expertise. (P8, Head Teacher)
Overall, staff understood the benefit of seeing the child’s needs holistically and as interlinked, rather than as separate conditions that each depended on a different strategy for support. Team working was therefore a crucial part of being able to meet the child’s needs for effective support.
Communication formats
One of the aims of this study was to gain insight into the most helpful format for communicating with external agencies both before, and for feedback following an assessment, which would influence the design of a proposed future intervention for children with CVI. In this subtheme, participants gave their opinions on what works well for communicating with agencies, the findings of assessment, and recommendations for support. The overall consensus was that reports should be individually tailored to the child and that lists of generic strategies where staff were responsible for choosing which to implement were not helpful. A variety of formats was also useful, including conversations and written reports. Finally, one participant detailed the ‘analysis of assessment’ format where
you identify a child’s needs then you identify a child’s possible outcome, and then you identify how you think that can be done, and then obviously there’s space to review. The idea is that the outside agencies do their reports in a similar way . . . and put it all together in one plan. (P9, SENCO)
Third theme: follow-up
Participants discussed the benefits of feedback and highlighted their preference for verbal feedback as well as written. They also described how ‘follow-up’ enables them to monitor and measure progress using recommended strategies.
Feedback
Feeling engaged with specialists helped participants to feel supported in their efforts to help the children in their care. Being able to easily contact individuals who provided advice was a way of refining the strategies. Some participants expressed that they would also value an informal initial consultation to check that formal assessment was appropriate, as well as a simple referral process. There was a consensus among participants that feedback should include formal and informal methods to be successful:
If it was something that you recommended that we do, you’ve written a report and sent it out to us, and then . . . come back in the following term, how are you finding it, has anything changed? And then I think that would be wonderful, . . . and I think that would make it effective. (P1, Teaching Assistant)
Measuring progress
Measuring progress was important for assessing how well strategies were working and to aid refining either the support or the target to match the child’s needs. It also gave the participants confidence that something they were doing was working and helped keep the targets within reasonable expectations. Individual needs of the child were considered important and thus having child-appropriate measures to monitor progress was discussed. One participant gave an example of using an alternative assessment tool for a child with Down’s syndrome that better indicated her progress in several key areas, ‘it’s so important for us to have something that we can assess her on and go actually, she’s doing brilliantly’ (P3, Teaching Assistant). Participants also saw the benefits of measuring progress for OFSTED inspections, and as evidence for escalating support through the SEN pathway.
Fourth theme: barriers and opportunities for accessing support
This final theme explored staff perspectives on accessing external support, describing the barriers to the current systems, ways that schools cope with access problems (including using private providers), and finally ideal world scenarios that would improve access to external support.
Practical barriers
Finances were the most commonly cited barrier to accessing external support with seven of nine participants raising this as a problem. This led to frustration that children were missing out on essential specialist support. Participants also expressed frustration at the time involved, requirements for various stages to go through prior to a diagnosis, with some parts of this process seen as unnecessary or irrelevant. Participants also described situations were progress has been reliant on parent involvement, ‘When you’ve got parents who are on board and they’re quite dogged in their approach then it could be quite successful . . . if the parent will push it forward and be persistent then they will probably make more headway than we will’ (P4, Head Teacher).
Going private
All three schools described how they engage private educational psychologist services, rather than use a package offered by the LA. The reasons given were mainly quality of service and cost-effectiveness. One school described how the LA package involved more money for a larger service provision than was needed by a small school. Value for money was described in terms of how easy it is to access the service, speed from requesting a visit to assessment and reporting, and the comprehensive nature of the reports. Other benefits to sourcing private external provision included the opportunity to benefit from increased follow-up support, for example, ‘if we go to the boss and we feel that we’ve done everything EP (educational psychologist) said then she would be back in contact and we won’t give up on it’ (P1, Teaching Assistant).
Ideal scenarios
In this final subtheme, participants commented on approaches that they felt work best. Participants felt strongly that getting to know and understand both the school staff and the child made for a better intervention, and where external providers spent time with the school and the child, this was seen as positively influencing the outcomes for that child. This was echoed by the benefits of being able to have one named person to work with, providing continuity.
The team for visual impairment . . . came in from reception to see the little boy that had CVI, and at the time he hadn’t been diagnosed with it . . . and they could easily have just discharged him, but they didn’t . . . and I think that’s good having that continuity as well. (P7, SENCO)
Finally, an intervention that can bring multidisciplinary groups of professionals together relatively quickly was seen to benefit children, as strategies for support can then be promptly worked up and implemented.
Discussion
The participants in this small study provided wide-ranging insights about working with external agencies to provide support for children with additional needs. They emphasised how understanding the condition and the underlying aims of any strategy were vital and focussed on the translational work needed from receiving an assessment report to implementing and adapting effective support strategies. They also described how maintaining communication and measuring progress via follow-up was key to the success of strategies, offered examples of barriers for engaging with external support, and were vocal in their criticism of how funding cuts in recent years have impeded their ability to provide support. Using private providers for some assessments has become the norm for these schools.
These insights related to specialised reports from a range of professionals and may be useful in efforts to improve communications specifically between hospital eye clinics and schools. Increased understanding about the nature and implications of visual problems might be achieved by signposting school staff to established resources or by providing schools with patient information leaflets (PILs) relevant to the child’s condition, as well as giving them to families. Helping the teachers translate the reports into action may be carried out by the QTVIs if involved. Their input could be supplemented or reinforced by the inclusion in PILs of the need for enlarged font size, or positioning within a classroom, as appropriate to the condition. Even when a diagnosis has not yet been established, including details of the child’s functional problems, for example, reduced contrast sensitivity or visual field, routinely in letters and reports could help school staff and QTVIs address the child’s day-to-day needs. If resources allow, clear jargon-free reports to schools about specific children’s needs are known to be effective (Black et al., 2019).
The request for follow-up is less easy to address as hospital services do not have the time or infrastructure to communicate regularly with schools. Possible solutions might be for units to offer a telephone helpline with answerphone, or an email address, that schools could use if they have a query regarding child with VI. Alternatively, the local QTVI team could offer this and then ask questions of the local eye clinicians as needed, on behalf of the schools. Either option would need resource from the QTVI or eye clinic team, but this input could save unnecessary clinic appointments if families and teachers had this way of having their queries or worries addressed (Anari et al., 2006).
Participants reported use of private providers for educational psychology and some therapy services. While this may not be commonplace for services for VI children, there are increasing numbers of private providers of vision screening services for healthy children including optometric organisations. Better lines of communication between schools and the hospital eye service would allow schools to ask about the merits of any private services that they may be considering. Some eye units have successful shared-care arrangements with private providers such as optometrists and this can reduce the load on busy eye units, as is already a model used for glaucoma (Gray et al., 2000). There is, however, a need for close working between professional groups to maintain quality and confidence (Townsend et al., 2015).
This was a small study which only reports the views of professionals working in three primary schools, all in the same local authority area. We had a range of roles of those working directly with children with additional educational needs take part; however, while our findings may ‘ring true’ for some other schools, they are not generalisable to other schools or locations. With a larger sample it would be useful to interview more staff with experience of working with children who have been diagnosed as having CVI; however, it was not possible in this study to limit eligibility using this criterion as CVI is currently only diagnosed in specialist clinics in the United Kingdom. Future studies may be able to investigate the communication between external support services specific to CVI and schools as this condition becomes more widely recognised. Despite these limitations, the interviews have demonstrated the value that school staff place on good communication with external support services, including being given the rationale behind strategies to try and follow-up support.
In conclusion, these interviews illustrate the value of eliciting opinions from the intended recipients of any professional advisory reports or guidance leaflets. The interviewees were clear that they wanted to understand the reasoning behind the advice they were given, so they could use their own professional skills to best effect in delivering the advice. This suggests that extra effort to share information with schools, both in general and about specific diagnoses, is likely to improve the quality of in-school support for children. As resources for children with additional needs are often scarce, these insights may be helpful for professionals who provide specialist advice to schools, including vision care specialists, in making sure they provide what is needed in the time available. They may also be useful for schools themselves, to help articulate their needs and preferences from advisory specialists, with benefits for the teachers and the children they support.
Footnotes
Acknowledgements
The study team are very grateful to all participating schools, their staff and children, and in particular the interviewees who contributed to this report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study/project presents independent research funded by the National Institute for Health Research (NIHR) Senior Fellowship award SRF_2015_08_005. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.